Yang Su, Dongmei Zou, Yi Liu, Chaoqun Wen, Xialing Zhang
{"title":"与溶栓疗法相比,抗凝剂对肺栓塞临床疗效的影响;Meta 分析","authors":"Yang Su, Dongmei Zou, Yi Liu, Chaoqun Wen, Xialing Zhang","doi":"10.1002/clc.70016","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Pulmonary embolism (PE) is a critical condition requiring effective management strategies. Several options are available, including thrombolytic therapy and anticoagulants.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>To assess the impact of thrombolytic therapy either combined with anticoagulant (AC) or alone versus AC alone on mortality, recurrence, clinical deterioration, bleeding, and hospital stay.</p>\n </section>\n \n <section>\n \n <h3> Method</h3>\n \n <p>This study included 25 previously published studies from 1990 to 2023, with a total of 12 836 participants. Dichotomous and continuous analysis models were used to evaluate outcomes, with heterogeneity and publication bias tests applied. A random model was used for data analysis. Several databases were searched for the identification and inclusion of studies, such as Ovid, PubMed, Cochrane Library, Google Scholar, and Embase.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>For sub-massive PE, CDT plus AC significantly reduced in-hospital, 30-day, and 12-month mortality compared to AC alone, odds ratio (OR) of −0.99 (95% CI [−1.32 to −0.66]), with increased major bleeding risk but no difference in minor bleeding or hospital stay, OR = 0.46, 95% CI [−0.03 to 0.96]). For acute intermediate PE, systemic thrombolytic therapy did not affect all-cause or in-hospital mortality but increased minor bleeding, reduced recurrent PE, and prevented clinical deterioration. The heterogeneity of different models in the current study varied from 0% to 37.9%.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The addition of CDT to AC improves mortality outcomes for sub-massive PE but raises the risk of major bleeding. Systemic thrombolytic therapy reduces recurrence and clinical decline in acute intermediate PE despite increasing minor bleeding. Individualized patient assessment is essential for optimizing PE management strategies.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 9","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70016","citationCount":"0","resultStr":"{\"title\":\"Anticoagulant Impact on Clinical Outcomes of Pulmonary Embolism Compared With Thrombolytic Therapy; Meta-Analysis\",\"authors\":\"Yang Su, Dongmei Zou, Yi Liu, Chaoqun Wen, Xialing Zhang\",\"doi\":\"10.1002/clc.70016\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Pulmonary embolism (PE) is a critical condition requiring effective management strategies. Several options are available, including thrombolytic therapy and anticoagulants.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>To assess the impact of thrombolytic therapy either combined with anticoagulant (AC) or alone versus AC alone on mortality, recurrence, clinical deterioration, bleeding, and hospital stay.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Method</h3>\\n \\n <p>This study included 25 previously published studies from 1990 to 2023, with a total of 12 836 participants. Dichotomous and continuous analysis models were used to evaluate outcomes, with heterogeneity and publication bias tests applied. A random model was used for data analysis. Several databases were searched for the identification and inclusion of studies, such as Ovid, PubMed, Cochrane Library, Google Scholar, and Embase.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>For sub-massive PE, CDT plus AC significantly reduced in-hospital, 30-day, and 12-month mortality compared to AC alone, odds ratio (OR) of −0.99 (95% CI [−1.32 to −0.66]), with increased major bleeding risk but no difference in minor bleeding or hospital stay, OR = 0.46, 95% CI [−0.03 to 0.96]). For acute intermediate PE, systemic thrombolytic therapy did not affect all-cause or in-hospital mortality but increased minor bleeding, reduced recurrent PE, and prevented clinical deterioration. The heterogeneity of different models in the current study varied from 0% to 37.9%.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>The addition of CDT to AC improves mortality outcomes for sub-massive PE but raises the risk of major bleeding. Systemic thrombolytic therapy reduces recurrence and clinical decline in acute intermediate PE despite increasing minor bleeding. Individualized patient assessment is essential for optimizing PE management strategies.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"47 9\",\"pages\":\"\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-09-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70016\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.70016\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.70016","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
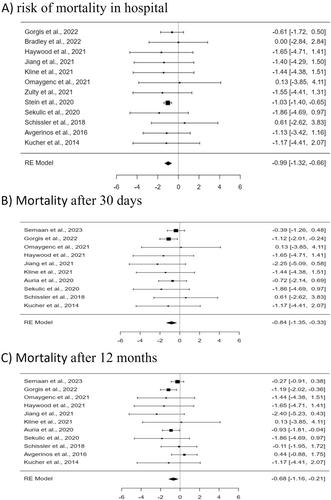
背景 肺栓塞(PE)是一种危重病,需要有效的治疗策略。目前有多种方法可供选择,包括溶栓疗法和抗凝剂。 目的 评估溶栓疗法与抗凝剂(AC)联合或单独使用对死亡率、复发、临床恶化、出血和住院时间的影响。 方法 本研究纳入了 25 项先前发表的研究,时间跨度从 1990 年到 2023 年,共有 12 836 名参与者。采用二分法和连续分析模型评估结果,并进行了异质性和发表偏倚检验。数据分析采用随机模型。为了识别和纳入研究,研究人员检索了多个数据库,如 Ovid、PubMed、Cochrane Library、Google Scholar 和 Embase。 结果 对于亚重度 PE,与单用 AC 相比,CDT 加 AC 能显著降低院内、30 天和 12 个月的死亡率,几率比(OR)为-0.99(95% CI [-1.32 to -0.66]),大出血风险增加,但小出血或住院时间无差异,OR = 0.46,95% CI [-0.03 to 0.96])。对于急性中型 PE,全身溶栓治疗不会影响全因死亡率或院内死亡率,但会增加轻微出血、减少复发性 PE 并防止临床恶化。本研究中不同模型的异质性从 0% 到 37.9% 不等。 结论 在 AC 基础上加用 CDT 可改善亚严重 PE 的死亡率,但会增加大出血的风险。全身溶栓治疗可减少急性中型 PE 的复发和临床衰退,尽管会增加轻微出血。对患者进行个体化评估对于优化 PE 管理策略至关重要。
Anticoagulant Impact on Clinical Outcomes of Pulmonary Embolism Compared With Thrombolytic Therapy; Meta-Analysis
Background
Pulmonary embolism (PE) is a critical condition requiring effective management strategies. Several options are available, including thrombolytic therapy and anticoagulants.
Objectives
To assess the impact of thrombolytic therapy either combined with anticoagulant (AC) or alone versus AC alone on mortality, recurrence, clinical deterioration, bleeding, and hospital stay.
Method
This study included 25 previously published studies from 1990 to 2023, with a total of 12 836 participants. Dichotomous and continuous analysis models were used to evaluate outcomes, with heterogeneity and publication bias tests applied. A random model was used for data analysis. Several databases were searched for the identification and inclusion of studies, such as Ovid, PubMed, Cochrane Library, Google Scholar, and Embase.
Results
For sub-massive PE, CDT plus AC significantly reduced in-hospital, 30-day, and 12-month mortality compared to AC alone, odds ratio (OR) of −0.99 (95% CI [−1.32 to −0.66]), with increased major bleeding risk but no difference in minor bleeding or hospital stay, OR = 0.46, 95% CI [−0.03 to 0.96]). For acute intermediate PE, systemic thrombolytic therapy did not affect all-cause or in-hospital mortality but increased minor bleeding, reduced recurrent PE, and prevented clinical deterioration. The heterogeneity of different models in the current study varied from 0% to 37.9%.
Conclusion
The addition of CDT to AC improves mortality outcomes for sub-massive PE but raises the risk of major bleeding. Systemic thrombolytic therapy reduces recurrence and clinical decline in acute intermediate PE despite increasing minor bleeding. Individualized patient assessment is essential for optimizing PE management strategies.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


