{"title":"流明临床","authors":"","doi":"10.1111/jgh.16704","DOIUrl":null,"url":null,"abstract":"<p><b>7</b></p><p><b>Safety, efficacy and tolerability of an ultra-low volume bowel preparation (NER1006) – a real world experience</b></p><p><b>Anthony Sakiris</b>, Arvinf Rajandran, Jane Lynch, Myles Rivlin and Sneha John</p><p><i>Gold Coast University Hospital, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic assessment with colonoscopy allows for the detection of polyps and adenomas which are precursors to colorectal adenocarcinoma. The quality of bowel preparation is of significant importance to the outcome of a colonoscopy as poor bowel preparation results in prolonged procedure times, the need for repeat procedures and missed lesions. A split-dose regimen of 3-4L Polyethylene Glycol (PEG) has historically been the recommended form of bowel preparation. NER1006 is a 1L split-dose PEG bowel preparation that is comparatively novel to Australia and has been adopted within our service since 2020. NER1006 provides enhanced osmotic activity from the high-dose ascorbate that is present in the second dose. Given its ultra-low volume, the aim of this study was to assess the safety, efficacy and tolerability of NER1006 in a real-world setting within our hospital network.</p><p><i><b>Methods:</b></i> This study was a retrospective analysis of prospectively collected data for colonoscopy procedures at two centres within our hospital health service. Patients who underwent a colonoscopy between July 2020 and February 2024 and received NER1006 as bowel preparation with a split-dose regime were analysed. The study population consisted of patients who returned a positive faecal occult blood test from the Australian National Bowel Cancer Screening Program (NBCSP) as well as symptomatic patients referred through our nurse-led Direct Access Colonoscopy clinic. The quality of the bowel preparation was quantified through the Boston Bowel Preparation Scale (BBPS). The Polyp Detection Rate (PDR), Adenoma Detection Rate (ADR), Sessile Serrated Lesion Detection Rate (SSLDR) and Advanced Adenoma Rate (AADR) were also calculated as quality indicators of colonoscopy. Adverse events related to NER1006 were classified as either minor or major. Major adverse events were defined as those requiring hospitalisation or those that prevented the patient from adequately completing their bowel preparation.</p><p><b><i>Results:</i></b> A total of 2920 colonoscopies were performed on 2874 patients. There were 1571 males, 1301 females and 2 indeterminate with a mean age of 57 years. 2827/2920 (97%) of the colonoscopies performed produced a BPPS score equal to or greater than 6 (good or excellent), with an average score of 7.90. Analysis revealed a 72% PDR, 55% ADR, 16% SSLDR and 25% AADR. There were 2 cases (0.07%) of major adverse events. One patient was unable to complete their bowel preparation due to vomiting and one patient presented with an acute kidney injury. There 98 cases (3.36%) of minor adverse events. Tachycardia (>100 bpm) was the most common minor adverse event and involved 48 patients (2%). Nausea was the second most reported minor adverse event and occurred in 29 patients (1%) with only 10 cases (0.3%) associated with vomiting. 17 patients (0.6%) noted mild to moderate abdominal pain. Other non-specific minor adverse events involving 4 patients (0.14%) included headache and dizziness.</p><p><b><i>Conclusion:</i></b> This study highlights that a split-dose regime of NER1006 is a safe, effective and tolerable bowel preparation. Our utilisation of NER1006 surpasses the 90% standard for adequate bowel preparation suggested by the Quality Committee of the European Society of Gastrointestinal Endoscopy. Established targets of a 40% PDR and a 25% ADR were also exceeded in our population. In our real-world experience, only a small minority of patients who were administered NER1006 exhibited adverse effects. Clinical dehydration due to NER1006 has been demonstrated in previous studies and may have been a contributor for our patients with tachycardia. However, other factors such as anxiety should also be considered. The implementation of multimodal education regarding the process of bowel preparation has assisted in enhancing the overall safety and tolerability of NER1006 within our network. Instructions for our patients to sip the bowel preparation slowly through a straw to minimise taste, drinking clear savoury fluids to offset the sweetness of NER1006 and ensuring adequate clear fluid intake have all been suggested strategies. This is the largest study regarding ultra-low volume bowel preparation reported within the Australian context, however it is limited by its retrospective model. Larger multi-centre prospective studies are recommended to further identify the factors that contribute towards the potential adverse effects of ultra-low volume bowel preparation in order to better prevent or manage them.</p><p><b>9</b></p><p><b>The presence of hiatal hernia is a significant predictor for symptomatic recurrence after cessation of vonoprazan therapy for gastroesophageal reflux disease: A long-term observational study</b></p><p><b>Satoshi Shinozaki</b><sup>1</sup>, Hiroyuki Osawa<sup>2</sup>, Yoshimasa Miura<sup>3</sup>, Hirotsugu Sakamoto<sup>2</sup>, Yoshikazu Hayashi<sup>2</sup>, Tomonori Yano<sup>2</sup>, Edward Despott<sup>4</sup> and Hironori Yamamoto<sup>2</sup></p><p><sup>1</sup><i>Shinozaki Medical Clinic, Utsunomiya, Japan;</i> <sup>2</sup><i>Jichi Medical University, Shimotsuke, Japan;</i> <sup>3</sup><i>Nihon University, Chiyoda, Japan;</i> <sup>4</sup><i>Royal Free Hospital, London, UK</i></p><p><b><i>Background and Aim:</i></b> Gastroesophageal reflux disease (GERD) symptoms frequently recur after cessation of acid blockers. The presence of a hiatal hernia may worsen GERD symptoms and increase the risk of esophageal malignancy. The aim of this study is to clarify the timing and predictors for recurrence of GERD symptoms after cessation of vonoprazan (VPZ) therapy.</p><p><b><i>Methods:</i></b> A retrospective observational study involved 86 patients who underwent cessation of VPZ therapy for symptomatic GERD. Collated data from medical record review included the endoscopic findings and Izumo scale score.</p><p><b><i>Results:</i></b> The mean duration of continuous VPZ therapy before cessation was 7.9 months. GERD symptoms requiring the resumption of VPZ therapy recurred in 66 of 86 patients (77%). Kaplan-Meier analysis showed that overall recurrence-free rates at 6 months, one and two years after VPZ cessation were 44%, 32% and 23%, respectively. Alcohol use, the presence of a hiatal hernia and long-term therapy for more than six months were identified as significant positive predictors for symptomatic recurrence. Notably, hiatal hernia had the highest hazard ratio in both univariate and multivariate analyses. The recurrence-free rate in patients with a hiatal hernia was much lower at 6 months than in patients without a hiatal hernia (15% and 51%, respectively p=0.002). After the symptomatic recurrence, GERD symptoms improved significantly after one-month VPZ therapy.</p><p><b>11</b></p><p><b>Establishment of a tertiary faecal microbiota transplant service and 24 month outcomes</b></p><p><b>Emma Buckner</b><sup>1,2</sup> and Thomas Goodsall<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology, John Hunter Hospital, Newcastle, Australia;</i> <sup>2</sup><i>School of Medicine and Public Health, The University of Newcastle, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> <i>Clostridium difficile</i> infection (CDI) is the most common cause of nosocomial diarrhoea in Australia and results in morbidity, risk of mortality, increased length of admission and resource utilisation. Recurrent CDI risk after antibiotic treatment is 20% and morbidity and mortality risk increase to 26-36% after first recurrence. Faecal Microbiota Transplant (FMT) is recommended in Australia as the preferred management for second and subsequent recurrences of CDI and is effective in 90% of cases after one FMT and 98% after a second FMT. We report our experience introducing an FMT service to a tertiary hospital and report the 24-month patient outcomes.</p><p><b><i>Methods:</i></b> A business case was prepared and submitted to the New Interventional Procedures and Quality use of Medicines committee at our hospital for introduction of an FMT service using TGA approved stool sourced from a third-party Australian provider (BiomeBank, Adelaide, South Australia). Successful approval was granted based on supporting evidence for efficacy and safety, proposed use of TGA approved stool product, limited scope of practice to recurrent or refractory CDI, structured supervision and accreditation program with audit and governance oversight, a cost analysis demonstrated cost benefit of FMT compared with antibiotic therapy, and supply of a -80 degree freezer for local storage of donor stool product.</p><p><b><i>Results:</i></b> 21 FMT procedures were performed in 17 patients. Demographics and outcomes are presented in Table 1. Complete remission was achieved in 14/17 patients (82%) after the first FMT and of the three patients requiring repeat FMT, one achieved remission after the second FMT, one required colectomy for persistent <i>C. difficile</i> colitis and megacolon, and one experienced ongoing recurrence in the setting of prophylactic antibiotics for lung transplant. Another patient was diagnosed with intercurrent Crohn’s colitis at the time of FMT and required colectomy for refractory Crohn’s colitis despite steroids and infliximab 4 weeks after FMT; the stool was <i>C. difficile</i> PCR negative and there was no histological evidence of persistent <i>C. difficile</i> infection. One other patient had deep ileocolonic skip ulcers consistent with Crohn’s disease and responded to FMT and induction steroids, while another had endoscopic and histological evidence of ulcerative proctitis which clinically responded to FMT and was in clinical and biomarker remission at 6 months. One patient experienced persistent diarrhoea after FMT despite clearance characterised by negative stool PCR and was subsequently diagnosed with a duodenal neuroendocrine tumour requiring Whipple’s resection.</p><p><b><i>Conclusion:</i></b> A funded FMT model was successfully introduced at our hospital with Clinical Governance approval. Primary response and cure was achieved in 88% of patients consistent with published outcomes. IBD was diagnosed in 3/17 patients at the point of FMT and cured in one case. Risk factors for requiring subsequent FMT were severe CDI with colitis and ongoing antibiotic use. No significant adverse events or deaths were directly attributable to FMT. This model could be reproduced to support other centres wanting to introduce an FMT service to provide quality evidence-based care.</p><p><b>18</b></p><p><b>Haemosuccus pancreaticus: an interesting and rare presentation of upper gastrointestinal bleeding</b></p><p><b>Annabelle Faint</b><sup>1</sup>, <b>Laurence Vaitiekunas</b><sup>1,4</sup>, Muddassir Rashid<sup>2</sup>, Arjuna Somasundaram<sup>2</sup> and Alexander Huelsen<sup>1,3</sup></p><p><sup>1</sup><i>Digestive Health, Gold Coast University Hospital, Gold Coast, Australia;</i> <sup>2</sup><i>Department of Radiology, Gold Coast University Hospital, Gold Coast, Australia;</i> <sup>3</sup><i>School of Medicine, University of Queensland, Gold Coast, Australia;</i> <sup>4</sup><i>School of Medicine and Dentistry, Griffith University, Gold Coast, Australia</i></p><p><b><i>Introduction:</i></b> Haemosuccus pancreaticus (HP) is a rare and life-threatening cause of upper gastrointestinal bleeding and is characterised by haemorrhage into the main pancreatic duct.<sup>1,2</sup> HP has a mortality rate of up to 9.6%.<sup>3</sup> Typically associated with chronic pancreatitis, HP arises from prolonged enzymatic exposure of peripancreatic arterial walls, precipitating a bleeding event that fistulsed into the pancreatic ductal system.<sup>4</sup> Clinical manifestations include haematemesis, melaena, abdominal pain, and in severe cases, haemodynamic instability. Diagnostic challenges can often arise due to the failure of initial endoscopic evaluation to identify a source of bleeding, compounded by a general lack of familiarity and awareness of this entity.<sup>1,2</sup> Computed tomography angiography (CTA) remains the gold standard for diagnosis and can guide management which includes angiographic embolisation and surgery. Surgical treatment is typically reserved for uncontrolled haemorrhage or when embolisation fails.<sup>2</sup> We describe a case of a 29-year-old male with a background of chronic pancreatitis and pancreatic pseudocyst (PC), exhibiting clinical manifestations indicative of haemosuccus pancreaticus, wherein a distal splenic artery pseudoaneurysm had bled into a pancreatic pseudocyst and the pancreatic ductal system. This was treated successfully by angiographic embolisation of the splenic artery.</p><p><b><i>Case Report:</i></b> A 29-year-old male with a history of alcohol-related chronic pancreatitis and an 8cm pancreatic tail pseudocyst presented with a two-day history of hematemesis, melaena, and epigastric pain. He reported abstinence from alcohol for several months and he denied smoking and the use of anti-inflammatory medications. His last gastroscopy in 2022 showed chronic gastritis only. On examination, he was pale with a soft abdomen demonstrating severe epigastric tenderness. There was no melaena on rectal examination. He was tachycardic to 116bpm and his blood pressure was 124/64 mmHg. Biochemistry revealed a hemoglobin of 37g/L, ferritin 2ug/L, urea of 1mmol/L, total bilirubin 5umol/L, ALP 92U/L, GGT 257U/L, ALT 16U/L, AST 25U/L. Resuscitation with four units of packed red blood cells and intravenous fluids stabilised his condition. His haemoglobin incrementally increased to 71g/L without evidence of ongoing gastrointestinal bleeding during his admission. Urgent gastroscopy demonstrated gastric erythema and small erosions in the antrum, without stigmata of recent bleeding. A subsequent abdominal CTA showed a 7 x 6mm distal splenic artery pseudoaneurysm projecting inferiorly into a large, longstanding pseudocyst posterior to the pancreatic tail, not identifiable on initial contrast CT abdomen. On comparison with prior imaging, the PC had developed intracystic high density material, in keeping with interval haemorrhage (Image 2). Angiographic embolisation with three 5mm microcoils to the lower pole branch of the splenic artery was successful (Image 4). He remained clinically stable following the procedure and was discharged after a period of inpatient observation.</p><p><b>References</b></p><p>\n 1. <span>Alshaikhli, A</span>, <span>Al-Hillan, A</span>. (<span>2023</span>). <span>Haemosuccus Pancreaticus. StatPearls. Treasure Island (FL)</span>. StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK570570/</p><p>\n 2. <span>Yashavanth, H. S.</span>, <span>Jagtap, N.</span>, <span>Singh, J. R.</span>, <span>Ramchandani, M.</span>, <span>Lakhtakia, S.</span>, <span>Tandan, M.</span>, <span>Gupta, R.</span>, <span>Vamsi, M.</span>, <span>Bhaware, B.</span>, <span>Rao, G. V.</span>, and <span>Reddy, D. N.</span> (<span>2021</span>) <span>Hemosuccus Pancreaticus: A systematic approach</span>. <i>Journal of Gastroenterology and Hepatology</i>, <span>36</span>: <span>2101</span>–<span>2106</span>. https://doi.org/10.1111/jgh.15404.</p><p>\n 3. <span>Yu, P</span>, <span>Gong, J</span>. <span>Hemosuccus pancreaticus: A mini-review</span>. <i>Ann Med Surg (Lond)</i>. <span>2018</span>; <span>28</span>: <span>45</span>-<span>48</span>. Published 2018 Mar 9. https://doi.org/10.1016/j.amsu.2018.03.002</p><p>\n 4. <span>Mekheal, N.</span>, <span>Roman, S.</span>, <span>Alkomos, M. F.</span>, <span>Mekheal, E.</span>, <span>Farokhian, A.</span>, <span>Millet, C.</span>, <span>Shah, H.</span>, <span>Melki, G.</span>, & <span>Baddoura, W.</span> (<span>2022</span>). <span>Hemosuccus Pancreaticus: Challenging Diagnosis and Treatment</span>. <i>European Journal of Case Reports in Internal Medicine</i>, <span>9</span>(<span>5</span>), 003337. https://doi.org/10.12890/2022_003337</p><p><b>39</b></p><p><b>Comparative evaluation of Atmo Gas Capsule System and SmartPill GI Monitoring System for transit time assessment in motility disorders</b></p><p><b>Jerry Zhou</b><sup>1</sup>, Allen Lee<sup>2</sup>, Thomas Abell<sup>3</sup>, Ashok Attaluri<sup>4</sup>, Michael Cline<sup>5</sup>, William Hasler<sup>6</sup>, Vincent Ho<sup>1</sup>, Anthony Lembo<sup>5</sup>, Amir Masoud<sup>7</sup>, Richard McCallum<sup>8</sup>, Baharak Moshiree<sup>9</sup>, Eamonn Quigley<sup>10</sup>, Satish Rao<sup>11</sup>, Mayra Sanchez<sup>7</sup>, Irene Sarosiek<sup>8</sup>, Abigail Stocker<sup>3</sup>, Brian Surjanhata<sup>12</sup>, William Chey<sup>2</sup> and Braden Kuo<sup>11</sup></p><p><sup>1</sup><i>Western Sydney University, Sydney, Australia;</i> <sup>2</sup><i>University of Michigan, Ann Arbor, USA;</i> <sup>3</sup><i>University of Louisville, Louisville, USA;</i> <sup>4</sup><i>Alliance for Multispecialty Research, Kansas City, USA;</i> <sup>5</sup><i>Cleveland Clinic, Cleveland, USA;</i> <sup>6</sup><i>Mayo Clinic, Scottsdale, USA;</i> <sup>7</sup><i>Hartford Health, Fairfield, USA;</i> <sup>8</sup><i>Texas Tech University, El Paso, USA;</i> <sup>9</sup><i>Atrium Health Wake Forest Medical University, Charlotte, USA;</i> <sup>10</sup><i>Houston Methodist Research Institute, Houston, USA;</i> <sup>11</sup><i>Augusta University, Augusta, USA;</i> <sup>12</sup><i>Massachusetts General Hospital, Boston, USA</i></p><p><b><i>Background and Aim:</i></b> Motility disorders, such as gastroparesis and slow transit constipation (STC), are common gastrointestinal (GI) conditions affecting up to 5% of individuals worldwide. The symptoms of motility disorders can be debilitating, affecting quality of life and driving utilisation of healthcare systems. Diagnosis relies on evaluation of regional transit times, with delayed gastric and colonic transit indicated for gastroparesis and STC, respectively. The SmartPill GI Monitoring System (SmartPill), an FDA-cleared wireless motility capsule (WMC), has been used in the assessment of gastroparesis and STC since 2008 but has recently been discontinued, leaving a need for a like replacement. This study aimed to assess a new WMC, the Atmo Gas Capsule System (Atmo Capsule), against SmartPill for the assessment of regional transit time in these conditions.</p><p><b><i>Methods:</i></b> Individuals with upper, lower, or combined GI symptoms were recruited in a prospective multi-centre study. Participants concomitantly ingested the Atmo Capsule and SmartPill in a randomized order. Regional transit times including Gastric Emptying Time (GET) and Colonic Transit Time (CTT) were measured and compared between the devices, where paired data were available. GET >5 hours and CTT >59 hours were defined as delayed.</p><p><b><i>Results:</i></b> 213 participants were recruited across 12 sites: 177 yielded paired GET results, and 147 for CTT. Pearson correlation coefficients for GET and CTT comparisons between Atmo Capsule and SmartPill were 0.86 (0.81-0.89) and 0.74 (0.66 – 0.81) respectively. GET demonstrated a positive predicted value (PPV) of 78.00% (SE: 5.86%), negative predictive value (NPV) of 85.83% (SE: 3.09%), and overall agreement (OA) of 83.62% (SE: 2.78%). For CTT, PPV was 67.35% (SE: 6.70%), NPV was 92.89% (SE: 2.60%), and OA was 84.35% (SE: 3.00%). No serious adverse device effects were reported. 32.2% of the total GET evaluable cohort had delayed GET, 27.2% of the CTT evaluable cohort had delayed CTT. For the cohort that had measurement for all transit regions, 20% had delayed CTT only, 11% had delayed GET only and 18% had a delay in multiple GI regions as measured by Atmo.</p><p><b><i>Conclusion:</i></b> The Atmo Capsule exhibited substantial agreement with SmartPill in measuring both GET and CTT, highlighting its utility as a potential replacement for the discontinued SmartPill for assessment of motility disorders. Observations of multi-regional dysmotility further highlight the value of measuring multiple regional of the GI tract with a single test.\n\n </p><p><b>46</b></p><p><b>The efficacy of EndoClot® in the prevention of delayed bleeding following advanced endoscopic resection</b></p><p><b>Anthony Sakiris</b>, Christopher Graddon, Arvinf Rajandran and Sneha John</p><p><i>Gold Coast University Hospital, Gold Coast, Australia</i></p><p><b><i>Background and Aims:</i></b> Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD) are advanced endoscopic techniques that have been increasingly employed for the resection of large precancerous polyps or early gastrointestinal neoplasia. Delayed bleeding is a common adverse event related to endoscopic resection. Modalities such as thermocoagulation with haemostatic forceps and clipping are available options to control bleeding. Recently, topical haemostatic agents have been utilised as an alternative therapy and are applied over the bleeding resection site. EndoClot® is a novel topical haemostatic agent that consists of biocompatible, non-pyrogenic and starched derived polysaccharides. EndoClot® is able to effectively control bleeding by creating a gelled matrix that accelerates the clotting process by concentrating platelets, red blood cells and coagulation proteins at the resection site. The matrix lasts temporarily and can dissipate over a few hours to days. EndoClot® has recently been incorporated within our health network. The aim of our study was to assess the efficacy of EndoClot® in preventing delayed bleeding following the advanced endoscopic resection of high-risk lesions.</p><p><b><i>Methods:</i></b> This study was a retrospective analysis of prospectively collected data of advanced endoscopic resections at one centre within our hospital health service. Patients who underwent advanced endoscopic resection between March and April 2024 and received EndoClot® adhesive were analysed. EMR was performed as per standard technique with submucosal injection with gelofusin and methylene blue +\\- adrenaline at the endoscopist’s discretion. Indications for EndoClot® use within the colon and rectum included polyps proximal to the splenic flexure greater than 20mm resected with hot-snare EMR and polyps distal to the splenic flexure resected with hot-snare EMR or ESD in high-risk patients (i.e. use of antiplatelets or anticoagulation). Indications for EndoClot® use within the duodenum included polyps greater than 10mm resected with hot-snare EMR and any ampullectomy. Indications for EndoClot® in the oesophagus and stomach included any lesions resected with EMR or ESD in high-risk patients. We recorded basic patient demographics and the use of antiplatelets or anticoagulation. Lesion characteristics such as size, location and histology were documented. Delayed bleeding was defined as clinically evident gastrointestinal bleeding that occurred up to 14 days following the procedure which resulted in an emergency department presentation, required a blood transfusion or a repeat intervention.</p><p><b><i>Results:</i></b> EndoClot® was administered following the endoscopic resection of 11 lesions for a total of 10 patients. 90% were male with mean age 67 years (SD 8.62 years). 2 patients (20%) were taking either antiplatelets or anticoagulation. 64% of resections were in the colon or rectum, 27% in the duodenum and 9% in the oesophagus. EMR was the most utilised resection technique (91%). The most common lesion was a tubular adenoma (36%) and 27mm was the mean lesion size resected (SD 11.34mm). There was one delayed post-polypectomy bleed in a patient on Clopidogrel and Warfarin (re-commenced 48 hours post procedure with Enoxaparin bridging), who presented 10 days following a descending colon hot-snare EMR of a 25mm tubular adenoma. This patient underwent a total of 3 subsequent inpatient colonoscopies to definitively control the bleeding over 3 admissions, with evidence of a visible vessel requiring thermal therapy at the second colonoscopy and re-application of EndoClot® during one of the procedures.</p><p><b><i>Conclusion:</i></b> Our study demonstrates that EndoClot® is an effective haemostatic agent for the advanced endoscopic resection of high-risk lesions given no evidence of delayed bleeding for patients not on antiplatelet or anticoagulant therapy. Our single delayed bleeding case required 3 subsequent colonoscopy procedures with ongoing bleeding despite thermal therapy, and hence the rebleeding risk would unlikely have been mitigated by use of a topical hemostatic agent. EndoClot® appears to be safe with no noted adverse effects related to its administration. Our study is limited due to its retrospective nature with small sample size. Obtaining data from a larger cohort will enable higher-quality evidence regarding the use of EndoClot®.</p><p><b>54</b></p><p><b>Delayed autonomic ganglionopathy following nivolumab therapy in a patient with metastatic melanoma</b></p><p><b>Kai Dong Choong</b><sup>1,2</sup>, <b>Aung Du</b><sup>2</sup>, Milly Wong<sup>1</sup> and Digby Cullen<sup>1</sup></p><p><sup>1</sup><i>St John of God, Perth, Australia;</i> <sup>2</sup><i>Sir Charles Gairdner Hospital, Perth, Australia</i></p><p><b><i>Introduction:</i></b> Immune checkpoint inhibitors (ICI) have shown improved clinical outcomes in several malignancies; however, they have also been associated with immune-related adverse effects (irAE). Neurological irAE, in comparison to other systems are reported to be rare. Alongside clinical scarcity, the mechanisms contributing to neurotoxicity remain poorly understood, rendering diagnosis challenging and requiring a high degree of suspicion. Here, we report a case of delayed autonomic ganglionopathy, likely precipitated by use of ICI, nivolumab.</p><p><b><i>Case Report:</i></b> A 76-year-old man presented with diarrhoea, abdominal pain, anorexia, post-prandial fullness, dizziness and 24kg weight loss over 6 months. Significant medical history includes metastatic melanoma treated with nivolumab for one year, completed three months before onset of symptoms. On examination, he appeared cachectic. He was hypertensive (150/94 mmHg), had a regular heart rate (74 bpm) and postural drops of up to 70mmHg. Other examination findings were unremarkable. General haematology and biochemistry revealed hyponatraemia (129mmol/L). Thyroid function tests and screening for endocrine causes were unremarkable. Normal chromogranin-A levels excluded neuroendocrine tumours. Coeliac serology was negative. Stool microbiology was negative for pathogens. Metronidazole challenge did not alleviate gastrointestinal symptoms. Normal faecal calprotectin and C-reactive protein excluded enteral inflammation. Antinuclear antibodies were normal and paraneoplastic screen was also unremarkable. Protein electrophoresis, serum light chains were normal and intestinal biopsy excluded amyloidosis. PET-CT did not detect metastasis. Bedside and stress echocardiography were unremarkable. Gastroscopy unveiled large residual food boluses, suggestive of decreased gastric motility. After exclusion of infective, neoplastic, autoimmune and metabolic causes, we concluded that this was a case of delayed autonomic ganglionopathy secondary to nivolumab. Management focused on symptomatic relief and improving quality of life. Diarrhoea was partially managed by cholestyramine, pancreatic enzymes, loperamide, and domperidone. Abdominal pain was managed with mebeverine in combination with both sublingual and transdermal buprenorphine. Anorexia and post-prandial fullness were managed with nizatidine. Postural hypotension was partially alleviated with midodrine, fludrocortisone and sodium chloride supplements. Recent follow-up included dose adjustments to fludrocortisone and midodrine. Postural hypotension remained but did not precipitate falls or syncope. Diarrhoeal episodes decreased to 4-5 times daily. Our patient regained some independence and was able to engage in social activities.</p><p><b><i>Conclusion:</i></b> We report a case of delayed autonomic ganglionopathy caused by use of nivolumab monotherapy. As acute and subacute presentations of neurological irAE are rare, and delayed presentations are exceedingly rare, clinicians ought to maintain a high level of suspicion on patients receiving treatment with ICI.</p><p><b>73</b></p><p><b>Living with faecal incontinence: A qualitative investigation of patient experiences and preferred outcomes through semi-structured interviews</b></p><p><b>Sadé Assmann</b><sup>1,2,3</sup>, Daniel Keszthelyi<sup>2,3</sup>, Stephanie Breukink<sup>1,3,4</sup> and Merel Kimman<sup>5</sup></p><p><sup>1</sup><i>Department of Surgery and Colorectal Surgery, Maastricht University Medical Centre +, Maastricht, The Netherlands;</i> <sup>2</sup><i>Department of Gastroenterology-Hepatology, Maastricht University Medical Centre, Maastricht, The Netherlands;</i> <sup>3</sup><i>Research Institute of Nutrition and Translational Research in Metabolism (NUTRIM), Maastricht University, Maastricht, The Netherlands;</i> <sup>4</sup><i>Research Institute for Oncology and Reproduction (GROW), Maastricht University, Maastricht, The Netherlands;</i> <sup>5</sup><i>Department of Clinical Epidemiology and Medical Technology Assessment, Care and Public Health, Research Institute (CAPHRI), Maastricht University Medical Centre +, Maastricht, The Netherlands</i></p><p><b><i>Background and Aim:</i></b> Faecal incontinence (FI) is a prevalent and debilitating anorectal problem which can cause embarrassment, anxiety, social isolation and diminishes quality of life (QoL). Currently, there is no optimal treatment option for FI, consequently, treatments primarily focus on symptom reduction and improving QoL. In order to gain a clearer understanding of the challenge’s patients encounter, it is essential to actively listen to patients’ perspectives and experiences, as well as the specific outcomes they aim to achieve from treatment. This study aims to explore how FI impacts patients’ lives and identify important treatment outcomes as part of the development of a Core Outcome Set (COS).</p><p><b><i>Methods:</i></b> Patients with FI were recruited from surgery and gastroenterology outpatient clinics in the Netherlands. Semi-structured interviews were performed, audio recorded, transcribed per verbatim and coded. Thematic analysis using the framework method with an inductive open coding approach was performed to identify (sub)themes and categories relevant to the patients.</p><p><b><i>Results:</i></b> Twelve interviews were conducted before saturation was reached (75% female, 25% male, mean age 63, range 39-83 year). Four main themes emerged ‘Physical symptoms’, ‘Impact on daily life’, ‘Emotional impact’ and ‘Coping’. Patients expressed how FI severely limits daily activities and emotional wellbeing. Treatment priorities centred on resuming normal activities rather than solely on symptom reduction (table 1).</p><p><b><i>Conclusion:</i></b> The impact of FI extends far beyond uncontrolled loss of faeces, affecting psychological, emotional, and social wellbeing. Patients prioritise outcomes focussed on reclaiming normalcy and independence rather than focusing on physical symptoms alone. Integrating these patient-centered outcomes in future studies could enhance treatment satisfaction and patient-perceived treatment success. Furthermore, outcomes identified through this study will be combined with other outcomes identified through literature review, forming a comprehensive list for a Delphi survey with relevant stakeholders to establish a consensus on a final list of outcomes for a COS for FI.</p><p><b>100</b></p><p><b>Digitally-delivered gut-directed hypnotherapy is superior to an active control program in patients with irritable bowel syndrome: a randomised controlled trial</b></p><p><b>Ellen Anderson</b>, Simone Peters, Peter Gibson and Emma Halmos</p><p><i>Monash University and Alfred Health, Melbourne, Australia</i></p><p><b><i>Background:</i></b> Face-to-face gut-directed hypnotherapy (GDH) is an effective therapy for irritable bowel syndrome (IBS), but is currently considered third line due to limited accessibility. Nerva is a digitally-delivered GDH program, comprising of psychoeducation (that includes diaphragmatic breathing) and GDH, with the intention to improve access to the IBS population. Efficacy data are limited to a retrospective study, in which gastrointestinal and psychological outcomes improved.</p><p><b><i>Aim:</i></b> To perform a single-blinded randomised controlled trial to determine the efficacy of the app-delivered GDH program compared with an active control of psychoeducation alone on gastrointestinal symptoms and psychological outcomes in patients with IBS.</p><p><b><i>Results:</i></b> Of 244 enrolled participants, 45 withdrew prior to completing the first 14 sessions. Hence, 199 (96 GDH and 103 Control; median age 37 (IQR 30-46) years and 91% were female) were included in a modified intention to treat analysis. Baseline demographics, gastrointestinal symptoms, psychological indices and QoL were similar between the groups and there was an even distribution of participants from Australia and USA. At the conclusion of the intervention, GDH induced clinical response in 71% compared to 53% with Control (p=0.011; chi-squared). IBS-SSS was a median (IQR) of 200 (131-304) with GDH, which was lower than 246 (165-308) with Control (p=0.032; Mann-Whitney; Figure). This was a reduction of 97 (41-166) for GDH and 57 (0-123) for Control (p=0.008) from baseline. There was a divergence in symptom improvement from 28 sessions (see Figure). Improvement in IBS-VAS pain >30% was reported by 59% with GDH compared to 41% with Control (p=0.009). IBS-QOL improved by 9 (0-27) with GDH compared to 3 (0-15) with Control (p=0.017). Both interventions improved DASS-21and SCL-90 scores similarly. Six months following intervention, 138 (84% GDH and 75% Control) completed symptom measures. The improved IBS-SSS and IBS-VAS pain scores compared with baseline were maintained in those participants (p<0.0001 for both groups), but there were no longer differences between the groups.</p><p><b><i>Conclusion:</i></b> The digitally-delivered GDH intervention is superior to psychoeducation alone in alleviating IBS symptoms and in a greater proportion of participants and in improving participant QoL. Benefits appear to be durable. These results support the use of app-delivered GDH (with psychoeducation) that is cheaper and more accessible than in-person therapy for IBS sufferers.</p><p><b>103</b></p><p><b>Endoscopic intermuscular dissection: blurring the line between endoscopy and surgery</b></p><p><b>Niroshan Muwanwella</b><sup>1</sup> and Dilini Gunawardena<sup>2</sup></p><p><sup>1</sup><i>Royal Perth Hospital, Perth, Australia;</i> <sup>2</sup><i>PathWest Laboratory Medicine, Perth, Australia</i></p><p><b><i>Introduction:</i></b> Endoscopic Intermuscular Dissection (EID) is a novel endoscopic resection method where a lesion is resected including the inner circular muscle layer of the gastrointestinal tract. Published literature is limited, however shows promising results both as a means of obtaining accurate local staging as well as a curative, organ sparing, endoscopic resection method for T1 rectal malignancies suspicious for deep submucosal invasion (SMI). We present the first Australian report of EID utilised to resect a pT1 malignant rectal polyp with superficial SMI.</p><p><b><i>Case report:</i></b> A 70-year-old man was referred for resection of a large rectal polyp. Assessment revealed a 3cm Paris IIa+Is polyp. Kudo pit pattern was type III<sub>L</sub> in the periphery, type III<sub>S</sub> in the centre and a small area with type V<sub>I</sub> and V<sub>N</sub>. Imaging classification was malignant polyp suspicious for SMI. Therefore, decision was made to undertake EID to ensure complete (R0) resection. Circumference of the polyp was marked with diathermy. Standard lifting agent consisting of colloid, Indigo Carmine and dilute Adrenaline was injected submucosally into the periphery of the polyp. Using a Dual Knife J (Olympus endoscopy, Tokyo, Japan), mucosa was incised and the submucosa exposed. After applying traction, circular muscle layer was incised to expose intermuscular space. Dissection was performed in this plane and the polyp removed ensuring R0 resection leaving the outer longitudinal muscle layer intact. The defect was left open, intravenous antibiotic administered intra-procedure. Patient made an uneventful recovery and was discharged home the next day on oral antibiotics. Histopathology revealed a 13mm well differentiated invasive adenocarcinoma, pT1, SM1. Deep and circumferential margins were clear and there was no perineural or lymphatic invasion. However, venous invasion and tumour budding was identified. Therefore, patient was referred to colorectal surgical team for a discussion of completion surgery.</p><p>Selecting the optimal treatment modality for T1 rectal malignancies suspicious for deep SMI is important to be able to offer patients with organ sparing resections. Available imaging modalities are poor at differentiation between T1 and >T2 cancers. EID bridges a gap in this area. It can offer curative endoscopic resection for a considerable proportion of these patients while providing accurate staging for the remainder, justifying major abdominal surgery.</p><p><b>119</b></p><p><b>Faecal microbiota transplant in advanced Parkinson's disease, microbial changes and effects on motor and gastrointestinal function: A randomised placebo controlled crossover study</b></p><p>Lucy Bracken<sup>1,2</sup>, Fiona Tudehope<sup>1</sup>, William J Ryan<sup>3</sup>, Scott Read<sup>1,4</sup>, Duncan Wilson<sup>5</sup>, Tanya Golubchik<sup>6</sup>, Brian Gloss<sup>7</sup>, Sarah Bray<sup>5</sup>, Laura Williams<sup>5</sup>, Sophie Waller<sup>5</sup>, Jessica Qiu<sup>5</sup>, David Tsui<sup>5</sup>, Donna Galea<sup>5</sup>, Neil Mahant<sup>5</sup>, Hugo Morales Briceno<sup>5</sup>, Florence CF Chang<sup>5,2</sup>, Jane Griffith<sup>5</sup>, Sushil Bandodkar<sup>5</sup>, Xi Chen<sup>5</sup>, Victor Fung<sup>5,2</sup> and <b>David Van Der Poorten</b><sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology Department, Westmead, Australia;</i> <sup>2</sup><i>Faculty of Medicine, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>John Curtin School of Medical Research, Australian National University, Canberra, Australia;</i> <sup>4</sup><i>School of Medicine, Western Sydney University, Blacktown, Australia;</i> <sup>5</sup><i>Neurology Department, Westmead Hospital, Westmead, Australia;</i> <sup>6</sup><i>School of Medical Sciences, University of Sydney, Sydney, Australia;</i> <sup>7</sup><i>Westmead Institute for Medical Research, Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Preliminary findings from case reports and small human studies suggest that faecal microbiota transplant (FMT) has therapeutic potential in Parkinson’s disease (PD) with effects on both motor and gastrointestinal symptoms. We aimed to determine whether FMT improves motor function, constipation and quality of life in patients with advanced PD and the specific microbiome changes associated with this.</p><p><b><i>Methods:</i></b> We conducted a randomised, blinded, placebo-controlled, crossover trial of FMT in patients with PD already on treatment with levodopa/carbidopa via a PEG-J tube. Patients had to be on a stable dose for 6 months and have ≥ 3 hours of OFF time. Patients were randomized 1:1 to FMT or Placebo and received infusions via PEG-J tube on week 0 and 2 and then had crossover therapy on weeks 6 and 8 after a four-week washout. Biomictra FMT (BiomeBank SA) was used with two different donors. The primary outcomes were safety/tolerability of FMT and change in daily OFF time. Secondary outcomes were change in constipation and quality of life (QOL) scores. Microbial composition was assessed at baseline, post FMT/Placebo and end of study and compared to clinical endpoints. Microbiome sequencing was performed on extracted DNA via the Illumina NextSeq 2000 platform. Species classification and analysis was performed using MetaPhlan.</p><p><b><i>Results:</i></b> We undertook preliminary analysis after recruiting nine patients who each had completed FMT and placebo infusions. The median age of the patients was 64 with the majority male (78%). There were no serious adverse events recorded. There were three (9%) infusion related blood pressure fluctuations that did not require treatment and six (17%) infusion related episodes of mild abdominal discomfort and bloating split equally between placebo and FMT. Compared to baseline, there was an increase in microbiome richness by Chao1 index post FMT (273 vs 311, p=0.04) and alpha diversity measured by Shannon index (3.89 vs 4.07, p=0.11). The five most common genera at baseline in study patients were <i>Bacteroides</i>, <i>Phocaeicola</i>, <i>Escherichia, Alistipes</i> and <i>Blautia</i>, while in donors it was <i>Bifidobacterium, Phocaeicola, Faecalibacterium, Lachnospiraceae</i> and <i>Bacteroides</i>. Post FMT patients had substantially more <i>Faecalibacterium</i> and <i>Bifidobacterium</i> in keeping with engraftment. Compared to baseline, six patients had improved OFF time, ON time and QOL scores after FMT, but only two had an improvement in constipation. When compared with Placebo, FMT was associated with an absolute reduction in 1.04 OFF hours (p=0.193) and an absolute increase in ON hours by 1.53 (p=0.113). In those with less OFF time and better QOL scores post FMT, baseline microbiome alpha diversity was increased (4.1 vs 3.61, p=0.11), as was post FMT richness (278 v 337, p=0.13). There was no difference in clinical or microbiome outcomes when comparing the two FMT donors.</p><p><b><i>Conclusions:</i></b> This preliminary analysis shows FMT in Parkinson’s disease patients via PEG-J tube is a safe and potentially effective treatment. Microbial changes related to richness and diversity appear to be associated with response to therapy. Specific changes at a genera and species level require further characterization.</p><p><b>138</b></p><p><b>A novel blood-based cytokine release assay shows high sensitivity and specificity for coeliac disease diagnosis even in people following a strict gluten-free diet</b></p><p><b>Olivia Moscatelli</b><sup>1</sup>, Amy Russell<sup>1</sup>, Lee Henneken<sup>2</sup>, Linda Fothergill<sup>1</sup>, Hugh Reid<sup>3</sup>, Jamie Rossjohn<sup>3</sup>, Melinda Hardy<sup>1</sup>, Vanessa Bryant<sup>1</sup> and Jason Tye-Din<sup>1</sup></p><p><sup>1</sup><i>Walter and Eliza Hall Institute, Melbourne, Australia;</i> <sup>2</sup><i>The Royal Melbourne Hospital, Melbourne, Australia;</i> <sup>3</sup><i>Monash University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> T-cell diagnostics in clinical practice are limited to tuberculosis but could eventually be used to replace histology in antigen-driven immune diseases, such as coeliac disease (CD), if they were more sensitive. Current diagnosis of CD is suboptimal. For patients already following a gluten-free diet (GFD), prolonged gluten challenge to establish a diagnosis is often poorly tolerated. Detection of gluten-specific CD4+ T cells is attractive for CD diagnosis but sophisticated techniques like HLA-DQ-gluten tetramers are impractical. We recently showed serum interleukin (IL)-2 release to gluten is a marker of gluten-specific T cells. We aimed to assess the diagnostic performance of an IL-2 whole blood assay (WBA) employing an “in-tube gluten challenge” and compared this to serum IL-2 levels after oral gluten and tetramer analysis.</p><p><b><i>Methods:</i></b> The IL-2 WBA was assessed in 79 adults with CD (71 on a GFD with negative CD serology and 8 consuming gluten; 75 HLA-DQ2.5) and 92 without CD (34 on GFD with self-reported non-celiac gluten sensitivity, NCGS, and 58 healthy controls consuming gluten; 35 HLA-DQ2.5). Fresh blood was incubated for 24 hours with gluten peptides and IL-2 assessed (MesoScale Discovery). Serum IL-2 levels at 0 and 4 h after single-bolus 10 g gluten challenge and tetramer frequency was also assessed in the treated CD and NCGS cohorts.</p><p><b><i>Results:</i></b> IL-2 WBA showed high accuracy to detect CD: sensitivity 85% (67/79), specificity 97% (89/92), AUC=0.93. Sensitivity increased to 88% (67/76) when CD patients with the atypical HLA-DQ8 genotype were excluded (AUC 0.95). The IL-2 WBA response correlates with both gluten-induced serum IL-2 (n=50, r=0.65, p < 0.0001) and the frequency of gluten-tetramer+ gut-homing T cells per million CD4+ T cells (n = 10, r=0.9, p < 0.0001). The IL-2 WBA was positive at tetramer frequencies as low as 1 per million CD4+ T cells. Higher baseline IL-2 WBA was associated with vomiting after gluten challenge.</p><p><b><i>Conclusion:</i></b> The IL-2 WBA demonstrates exceptional sensitivity equivalent to detecting a single gluten-specific T cell in a 4 ml blood vial. It is a simple, tube-based assay requiring < 10 mL whole blood and can predict the severity of gluten-induced symptoms. It shows high diagnostic accuracy for CD with the important advantage of detecting CD in patients following a GFD with negative transglutaminase-IgA. Ongoing refinements aim to improve diagnostic sensitivity. The IL-2 WBA has the potential to revolutionise CD diagnosis and overcome the current limitations of CD serology and histology.</p><p><b>159</b></p><p><b>Thionamide-induced neutropenic enterocolitis in a patient in thyroid storm: a rare clinical entity</b></p><p><b>Ibrahim Mian</b>, Aisling Hand and Katherine Griffin</p><p><i>Gold Coast University Hospital, Gold Coast, Australia</i></p><p><b><i>Introduction:</i></b> Neutropenic enterocolitis (NEC) is a severe, life-threatening condition characterized by inflammatory necrosis of the bowel wall, seen in neutropenic patients. Bowel wall inflammation in NEC progresses to ulceration and necrosis, which if not addressed promptly can cause bowel perforation. There have been no reported cases of NEC secondary to thionamide use and for a patient in thyroid storm.</p><p><b><i>Case Report:</i></b> A young woman in her thirties with a recent diagnosis of Graves' disease for which she took methimazole, presented to hospital with fevers, abdominal pain, and diarrhoea after recently returning from Thailand. She was febrile to 38.8°C, tachycardic to 140 bpm, and a blood pressure of 105/56 mmHg. Her exam was remarkable for exophthalmos, a large palpable goitre, and swollen exudative tonsils. She had an absolute neutrophil count of 0.00x 10^9/L (2.5-7x 10^9/L), free T4 63.5 pmol/L (10-20 pmol/L), free T3 28.9 pmol/L (2.8-6.8 pmol/L), and a TSH 0.00 mU/L (0.50-4.00 mU/L). Her presentation was in keeping with agranulocytosis secondary to thionamide use for her Graves’ disease complicated by thyroid storm from a bacterial tonsillitis. Her management was complicated as she was unable to use alternative antithyroid drugs for her thyroid storm. As such, she was managed with intravenous fluids, broad spectrum antibiotics, and granulocyte-colony stimulating factor (G-CSF) for her bacterial tonsillitis and neutropenic sepsis. Lugol’s iodine, glucocorticoids, and propranolol were used to manage her thyroid storm, whilst awaiting a thyroidectomy. On day 10 of her admission, she developed severe abdominal pain with associated haematochezia. She examined as peritonitic. Her CT abdominal imaging demonstrated features consistent with NEC. She was abruptly taken to theatre for an emergency laparotomy. Histology from her diseased bowel remained consistent with NEC. By day 31 of her admission, she underwent a total thyroidectomy without complications and was discharged in the following days.</p><p><b><i>Conclusion:</i></b> This case highlights the clinical challenges in managing a patient with NE in concomitant thyroid storm and neutropenic sepsis from thionamide-induced agranulocytosis. The patient's management was complicated by overlapping symptoms of thyrotoxicosis and NEC, underscoring the need for high clinical suspicion and early imaging in febrile neutropenic patients with gastrointestinal symptoms. Lugol's iodine served as a critical bridging therapy in managing thyrotoxicosis until surgical intervention was feasible. The case also raises considerations for the selective use of G-CSF in high-risk patients with NEC. Ultimately, thionamide-induced NEC, though rare, requires prompt recognition and management due to its high mortality risk.</p><p><b>172</b></p><p><b>Nasogastric delivery of fecal microbiota transplantation for treatment of <i>Clostridioides difficile</i> infection: a case report</b></p><p><b>Amitjeet Singh</b>, Edward Young and Arvind Rajagopalan</p><p><i>Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> <i>Clostridioides difficile</i> is a significant healthcare challenge due to its association with antibiotic-associated diarrhea, increasing incidence, and the emergence of highly virulent strains. Traditional treatments like metronidazole and oral vancomycin are becoming less effective due to rising resistance, while faecal microbiota transplantation (FMT) has shown promise, particularly via direct caecal delivery. This case report describes the successful use of nasogastric FMT to avoid colectomy in a patient with severe <i>C. difficile</i> infection (CDI) complicated by toxic megacolon.</p><p><b><i>Case Report:</i></b> A 46-year-old female with cirrhosis presented to the emergency department with haematemesis and haemodynamic instability. An emergency endoscopy demonstrated large oesophageal varices with high-risk stigmata, managed with band ligation. She was commenced on intravenous pantoprazole and ceftriaxone according to routine variceal bleeding protocols. Unfortunately, one week into her admission (after completing 5 days of ceftriaxone) she developed abdominal pain, diarrhoea and fevers to 38.1°C. Laboratory investigations showed a white cell count of 19x10<sup>9</sup>/L, C-reactive protein of 143mg/L and albumin of 21 g/dL. Computed tomography (CT) scan of her abdomen showed colitis involving the ascending colon and splenic flexure but no colonic dilation. A stool PCR was positive for <i>C. difficile</i> toxin. Treatment was initiated with oral vancomycin 250mg four times daily and intravenous metronidazole 500mg three times daily. Despite escalation of vancomycin to 500mg four times daily, the patient symptoms worsened, with increasing abdominal pain, diarrhea, and new onset hepatic encephalopathy. Repeat abdominal X-rays demonstrated significant colonic dilation, with a transverse colon diameter of up to 12cm. The decision was made to proceed with FMT, however colonoscopic delivery was not safe due to the toxic megacolon. Push enteroscopy was also deemed to be high-risk given the recent oesophageal banding, decompensated cirrhosis with ascites and encephalopathy, and ileus with resultant risk of aspiration. We administered the first 50ml syringe of FMT solution via enema without complication. Four hours after the enema, three syringes of FMT solution were administered at two-hour intervals via the nasogastric tube, with concurrent intravenous metoclopramide 10mg three times a day as an anti-emetic and prokinetic. The syringes were each delivered slowly over 10 minutes, ensuring no nausea or vomiting occurred. The following day the patient had a significant improvement in abdominal pain, diarrhea, and encephalopathy. A repeat abdominal X-ray showed the resolution of toxic megacolon with a normal amount of gas throughout the large bowel. There was significant improvement in her C-reactive protein and white cell count. The patient was discharged home with 14-days of oral vancomycin.</p><p><b><i>Discussion:</i></b> In this case, we have demonstrated successful salvage of a <i>C. difficile</i>-related toxic megacolon following administration of FMT via a nasogastric tube, where push enteroscopy was relatively contraindicated. Comparative studies on the efficacy of fecal transplantation based on the administration method have yielded mixed results. A systematic review found that the success rates of fecal transplantation were lower when administered via enteroscopy or nasoenteric tube (88%) compared to colonoscopy and enema (95%). Another review analysing colonoscopic versus nasogastric methods across 12 studies revealed a higher success rate for the colonoscopic approach (93%) over nasogastric (85%), though the difference was not statistically significant. Nevertheless, in severe cases there are often contraindications to traditional methods for FMT delivery, as was the case in our patient. There are few published articles on the use of FMT for patients with toxic megacolon. Evidence has shown that FMT is effective in patients with recurrent CDI while evidence and experience in the context of severe and fulminant <i>C. difficile</i> continues to grow. To our knowledge this is the first reported case where nasogastric delivery of FMT solution has led to resolution of a <i>C. difficile</i>-related toxic megacolon. There are inherent risks of aspiration with this method, however a colectomy would have resulted in extremely high morbidity and mortality given the patient’s decompensated cirrhosis. This highlights the importance of the awareness of various routes of FMT delivery in order to tailor delivery to specific patient circumstances.</p><p><b>173</b></p><p><b>Endoscopic submucosal dissection of complicated giant gastrointestinal lipomas - a tertiary care center experience</b></p><p><b>Wei Ling Teh</b>, Sherman Picardo, Niroshan Muwanwella and Marcus Chin</p><p><i>Royal Perth Hospital, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal (GI) lipomas are benign subepithelial lesions (SELs) composed of mature adipose tissue. While often asymptomatic, GI lipomas can cause complications such as bleeding, luminal obstruction, or intussusception, necessitating intervention. Currently, there is no standardized approach for the treatment of symptomatic GI lipomas. Most cases reported in the literature were resected surgically. Recently, endoscopic resection techniques have evolved, with endoscopic submucosal dissection (ESD) emerging as a promising approach for the management of GI lipomas. We aim to analyse the success and safety of ESD in resecting GI lipomas.</p><p><b><i>Methods:</i></b> This was a retrospective, observational case series study. We reviewed gastrointestinal lipomas resected by ESD at our hospital between March 2017 and October 2023<b>.</b> All upper ESDs were performed using either EG760Z (Fujifilm, Tokyo, Japan) or GIF-HQ190 (Olympus Medical, Tokyo, Japan) Gastroscope. Colonic ESD was performed with EC760ZVL Colonoscope (Fujifilm, Tokyo, Japan). Utilizing either Dual Knife J and/or IT-2 knife (Olympus Medical, Tokyo, Japan), we directly dissected the submucosal connective tissue beneath the lesion, achieving en-bloc resection.</p><p><b><i>Results:</i></b> Here, we present seven instances wherein giant GI lipomas were effectively excised using ESD. All patients included in our study exhibited sizable GI lipomas and were experiencing associated symptoms. The mean age of patients was 59 years (41-68). The average lipoma size was 79 mm (50-100mm). Histopathology examination confirmed the diagnosis of lipomas in six cases and one case of angiolipoma. All patients were followed up either in clinic to ensure resolution of symptoms or with surveillance endoscopies. We demonstrated the successful removal of three bleeding and three obstructive large GI lipomas, all without complications, including bleeding and perforation.</p><p><b>175</b></p><p><b>Effectiveness and long-term durability of cricopharyngeal peroral endoscopic myotomy for treating dysphagia with upper oesophageal sphincter dysfunction: a mixed aetiology study</b></p><p><b>Alvin Cheah</b><sup>1,2</sup>, Michal Szczesniak<sup>1,2</sup>, Dheeraj Pandey<sup>1,2</sup>, Julia Maclean<sup>1,2</sup> and Peter Wu<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, St George Hospital, Sydney, Australia;</i> <sup>2</sup><i>St George and Sutherland Clinical School, University of New South Wales, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Encouraging preliminary data shows that cricopharyngeal peroral endoscopic myotomy (C-POEM) improves oropharyngeal dysphagia (OPD) in Parkinson’s disease (PD) patients with upper oesophageal sphincter (UOS) dysfunction on pharyngeal high-resolution impedance manometry (PHRIM). UOS dysfunction can manifest in a spectrum of neuromyogenic disorders, including PD, cerebrovascular accidents (CVA), inflammatory myopathies and post head and neck cancer (HNC) treatment. The aim of this study is to assess the efficacy and the long-term durability of C-POEM as a treatment for dysphagia with mixed aetiologies with proven underlying UOS dysfunction.</p><p><b><i>Methods:</i></b> Consecutive patients with OPD underwent PHRIM and were offered C-POEM if failed UOS relaxation was observed. Analysis was carried out on Swallow Gateway and failed UOS relaxation was defined as increased integrated relaxation pressure (IRP<sub>0.25</sub>) above upper limit of normal for a liquid bolus (either thin IDDSI 0 or thick IDDSI 4) of highest volume tolerated without piecemeal swallowing. Sydney Swallow Questionnaire (SSQ) was obtained at baseline, 1 month and yearly up to 3 years after C-POEM to measure symptoms of swallow dysfunction. The mean change in total SSQ scores from pre-treatment to 1 month post were assessed using paired t-test. Long term trend in total SSQ score post-treatment was assessed using repeated measures mixed model.</p><p><b><i>Results:</i></b> Between September 2020 and Sept 2023 consecutive patients (n = 15) underwent C-POEM for OPD and UOS dysfunction demonstrated on PHRIM. Patients with OPD were of various aetiologies such as CVA (n=4), inflammatory myopathies (n=4), Parkinson’s disease (n=2) and HNC (n=5). In one HNC patient included in the analysis, C-POEM could not be completed due to extensive submucosal fibrosis. There was an improvement in mean SSQ scores 1-month post C-POEM (714, 95%CI [542-885]) from baseline (1133, 95% CI [951-1314]). The mean change was statistically significant (∆ 419, 95% CI [253-585], p=0.0001). We observed no deterioration in swallow function on SSQ post C-POEM on repeated measures mixed model. Mean follow-up period was 8 months and the SSQ score remained stable with minimal non-significant change of -0.69 per month, 95% CI [-9.02-2.29] (p=0.87). There were no complications identified in the study group.</p><p><b><i>Conclusion:</i></b> C-POEM is an effective and safe novel endoscopic technique that improves dysphagia symptoms in patients with neuromyogenic disorders and HNC by targeting spastic UOS, thus improving bolus flow during swallowing. Importantly, dysphagia symptoms remained stable post C-POEM. However, considering the small sample size, larger and longer prospective trials looking at the merits of C-POEM is warranted.</p><p><b>176</b></p><p><b>Evaluating hypopharyngeal post-swallow and contractile admittance as non-radiological markers of pharyngeal residue and clearance in dysphagia</b></p><p><b>Alvin Cheah</b><sup>1,2</sup>, Dheeraj Pandey<sup>1,2</sup>, Julia Maclean<sup>1,2</sup>, Peter Wu<sup>1,2</sup> and Michal Szczesniak<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, St George Hospital, Sydney, Australia;</i> <sup>2</sup><i>St George and Sutherland Clinical School, University of New South Wales, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Post-swallow residue and presence of pharyngeal space during pharyngeal constriction are swallowing impairment signs and pose aspiration risk. Analysis of admittance during pharyngeal high-resolution impedance manometry (PHRIM) offers a potential non-radiological marker of pharyngeal residue post-swallow and during pharyngeal contraction, providing quantitative interpretation at bedside. Additionally, absence of radiation exposure makes it appropriate for follow up studies with repeat progress measurements. The aim of this study was to compare estimates obtained with admittance against radiographic equivalents.</p><p><b><i>Methods:</i></b> We identified 98 patients with oropharyngeal dysphagia of various aetiologies who underwent concurrent videofluoroscopy and PHRIM. Using SwallowGateway (5ml liquid (IDDSI 0) swallows), hypopharyngeal post-swallow admittance (HpPostAdm) was calculated as mean admittance spanning the hypopharyngeal segment within 0.5s after the stripping wave. Hypopharyngeal contractile admittance (HpContAdm) was calculated as mean admittance during the period of hypopharyngeal contraction. In the same cohort, fluoroscopic videos of 5ml liquid (IDDSI 0) swallows in lateral projection were independently analysed after spatial calibration referenced to radio opaque PHRIM sensors. Areas (cm<sup>2</sup>) of post-swallow reside were calculated for vallecula (VR), pyriform sinuses (PR) and other pharyngeal areas (OR). These were summed to derive total pharyngeal residue (TR). Intraluminal area at maximum pharyngeal constriction (AMPC) was measured in the frame showing maximum obliteration of the space in the pharynx before the pharynx begins to relax. Sydney Swallow Questionnaire (SSQ) was routinely obtained prior to PHRIM assessment to measure baseline swallow dysfunction.</p><p><b><i>Results:</i></b> Patient backgrounds included Parkinson’s disease (12), head and neck cancer (55), inclusion body myositis (8), cerebrovascular accident (2), muscular dystrophy (3), MOGAD (1), multiple sclerosis (1), motor neuron disease (1) and idiopathic (15). Majority were male (70%) and mean SSQ was (588.92 ±SD 409.15). We observed significant correlation between HpPostAdm and residue area observed radiographically post-swallow in the lateral plane. Correlation was highest with PR (Spearman’s ρ=0.64, p<0.0001) followed by TR (ρ=0.59, p<0.0001) and VR (ρ=0.34, p=0.001). Correlation between HpContAdm and AMPC was also significant with ρ=0.341, p=0.0006.</p><p><b>177</b></p><p><b>Beyond metrics: esophageal hypervigilance better predicts esophageal symptom severity compared with pH study and HRM metrics</b></p><p><b>Lyman LIN</b><sup>1</sup>, Tamara Debreceni<sup>1</sup>, Ruby Han<sup>1</sup>, Dhivya Pandiaraja<sup>1</sup>, Melissa Braudigom<sup>1</sup>, Jacinta McMahon<sup>1</sup>, Shahreedhan Shahrani<sup>1</sup>, Santosh Sanagapalli<sup>2</sup> and Chamara Basnayake<sup>1,3</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>St Vincent's Hospital Sydney, Sydney, Australia;</i> <sup>3</sup><i>The University of Melbourne, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> In clinical practice, the results from manometry and pH studies are often insufficient to explain the symptom severity of dysphagia and gastroesophageal reflux disease symptoms (GORD) perceived by patients. Oesophageal hypervigilance is thought to be a contributor to symptom severity of dysphagia and GORD. The 7-item questionnaire Oesophageal Hypervigilance and Anxiety Scale (EHAS-7) was developed to assess oesophageal hypervigilance. Our study aims to investigate whether manometry/pH study metrics or EHAS-7 have a greater correlation with the symptom severity of GORD and dysphagia. We hypothesise oesophageal hypervigilance can better predict symptom severity for symptoms than physiological study metrics.</p><p><b><i>Methods:</i></b> Consecutive patients attending for high resolution manometry (HRM) with or without a 24-hour pH study at a tertiary referral centre, from March 2022 to October 2023, were prospectively included. Patients completed the following questionnaires: EHAS-7, Brief Esophageal Dysphagia Questionnaire (BEDQ) and Gastroesophageal Reflux Disease Questionnaire (GERDQ). Pearson’s correlation was used to determine the interrelationships between questionnaire results, HRM and pH study metrics.</p><p><b><i>Results:</i></b> 286 patients were included with 170 completing pH studies. The median age was 55 (IQR 42 – 66) and 181 (63.3%) were female. Chicago 4 diagnoses included 189 (66.1%) patients with a normal study, 40 (14.0%) with achalasia, 15 (5.2%) esophagogastric junction outflow obstruction (EGJOO), 25 (8.74%) ineffective oesophageal motility (IEM), 8 (2.80%) absent contractility, 3 (1.05%) diffuse oesophageal spasm (DES) and 6 (2.10%) Jackhammer oesophagus. In the whole cohort, symptom severity (BEDQ) was significantly correlated with EHAS-7 (r = 0.362, p < 0.001) and several HRM metrics: including median integrated relaxation pressure (IRP) for supine 5ml swallows (r = 0.320, p < 0.001), median IRP for upright 5ml swallows (r = 0.358, p < 0.001) and median IRP for 2cm bread swallows (r = 0.360, p = 0.001). Among patients with normal manometry findings, BEDQ had a significant correlation with EHAS-7 (r = 0.245, p = 0.002) and median DCI for upright swallows (r = 0.230, p = 0.046). In patients with achalasia, BEDQ was significantly associated with EHAS-7 (r = 0.414, p = 0.017) but not HRM metrics. For those with IEM, BEDQ was correlated with EHAS-7 (r = 0.594, p < 0.002) and median DCI for supine swallows (r = 0.542, p = 0.025). Regarding patients with absent contractility, symptoms were only correlated with EHAS-7 (r = 0.823, p = 0.023). BEDQ was not associated with either EHAS-7 or any manometry metrics for patients with DES or Jackhammer oesophagus. For patients presenting with GERD symptoms including heartburn and regurgitation, symptoms (GERDQ) were significantly associated with EHAS-7 (r = 0.148, p = 0.028) but not pH metrics. Age, sex, and BMI did not correlate with symptom severity for dysphagia or GORD.</p><p><b><i>Conclusion:</i></b> In this cohort, we observed a stronger correlation between dysphagia and GORD symptom severity with Oesophageal hypervigilance scores compared to physiological metrics. These findings suggest a potential utility of Oesophageal hypervigilance as a predictor for patient-reported Oesophageal symptom severity. Subsequent studies should be conducted to investigate whether treating oesophageal hypervigilance improves symptom severity.</p><p><b>211</b></p><p><b>Evaluating the use of faecal occult blood tests for bowel cancer screening in persons with established spinal cord injury aged 50 – 74 years</b></p><p><b>Michael Yulong Wu</b><sup>1,2,3</sup>, Carmen Tung<sup>1</sup>, Mccawley Clark-Dickson<sup>4</sup>, Samuel Arthurs<sup>1</sup> and Ian Norton<sup>1,2</sup></p><p><sup>1</sup><i>Royal North Shore Hospital, Gold Coast, Australia;</i> <sup>2</sup><i>Northern Clinical School, University of Sydney, Gold Coast, Australia;</i> <sup>3</sup><i>Faculty of Health Science and Medicine, Bond University, Gold Coast, Australia;</i> <sup>4</sup><i>Sydney Adventist Hospital, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> In 2006 the Australian Government established the National Bowel Cancer Screening Program (NBCSP) with an aim to reduce the morbidity and mortality of colorectal cancer by early detection of malignancy. The program involves sending a biennial faecal occult blood test (FOBT) kit to all Australians aged 50 – 74 years old and those who test positive are recommended to proceed with colonoscopy if appropriate. The role and accuracy of FOBT in the spinal cord injury (SCI) population is yet to be established in the literature. We have postulated that the frequent use of rectal enemas, digital stimulation, chronic constipation and associated anorectal disorders in SCI patients can lead to colonic microtrauma with higher rates of positive FOBT. Therefore, the purpose of this study is to investigate the proportion of positive FOBT among patients with established SCI compared to the general population as measured by the NBCSP. We hypothesised that patients with SCI have a higher false positive rate.</p><p><b><i>Methods:</i></b> A prospective study was conducted at a tertiary hospital with one of the two inpatient spinal injury units in New South Wales. All established SCI patients aged 50 – 74 years old were included. Patients outside of the age criteria, those with active per-rectal bleeding, haemorrhoids, per-vaginal bleeding, hematuria, SCI within 12 months, colonoscopy within 4 years, or had already completed FOBT as part of the NBCSP were excluded. Recruited patients had two separate faecal samples sent for FOBT. Those with at least one positive FOBT were offered either an inpatient colonoscopy or outpatient follow-up at their local hospital.</p><p><b><i>Results:</i></b> A total of 18 patients were included in the study with a mean age of 61.1 years. In total 44.4% of patients tested positive on at least one FOBT. Of those who tested positive, two patients agreed to proceed with colonoscopy. In both cases the colonoscopy was normal. The majority of patients declined follow-up colonoscopy due to perceived difficulty with bowel preparation and procedural risks. Most patients reported rectal enema use, digital simulation and manual evacuation as part of their routine bowel care (Table 1). Out of those who used enemas, digital stimulation or manual evacuation, 41.1% returned a positive FOBT.</p><p><b><i>Conclusion:</i></b> To date, there is a lack of prospective studies that have investigated the accuracy of FOBT in patients with SCI. In this study, patients with SCI have higher rates of positive FOBT compared to the general Australian population at 6.2%. Follow-up colonoscopy rates were poor and patient compliance can be improved by more streamlined inpatient bowel preparation protocols. Higher rates of positive FOBT may be attributed to colonic and anorectal microtrauma. Our results suggests that the FOBT may not be an accurate screening tool in this population and a primary screening colonoscopy strategy may be more appropriate.</p><p><b>212</b></p><p><b>Upadacitinib real-world efficacy and safety in treatment of inflammatory bowel disease: an Australian single-centre experience</b></p><p><b>Gordon Chen</b>, <b>Vikram Rao</b>, Sheng Wei Lo, Elaine Koh, Abha Kaul and Richard La Nauze</p><p><i>Peninsula Health, Frankston, Australia</i></p><p><b><i>Background and Aim:</i></b> Upadacitinib, a recently approved small molecule inhibitor of Janus kinase 1 (JAK1), has been subject to much excitement as a new effective therapy in the management of moderate to severe ulcerative colitis (UC) and moderate to severe Crohn’s disease (CD). There has been rapidly increasing evidence of efficacy in both forms of inflammatory bowel disease (IBD) in literature but still a relative paucity of safety data. This retrospective, single centre, observational study aimed to assess the clinical efficacy and audit the safety of this novel medication in the biologic-experienced IBD cohort.</p><p><b><i>Methods:</i></b> Retrospective review was undertaken for all IBD patients prescribed Upadacitinib between January 2023 and May 2024 at a single-centre IBD service in Melbourne, Australia. Patients that have had at least 6 months of follow-up were included. Clinical and biochemical parameters were assessed at baseline, end of induction and at 6-months. Datapoints included previous exposure to biologics/JAK inhibitors, bowel motion frequency, clinical score indices (SCCAI/HBI), C-reactive protein (CRP), faecal calprotectin (FCP), and any adverse events.</p><p><b><i>Results:</i></b> Four patients were identified for inclusion, three patients with UC and one patient with CD, with median follow-up time of 41.1 weeks (IQR 35.8-50.9). All were anti-tumour necrosis factor (TNF)-experienced. 75% (3/4) achieved the primary outcome of clinical remission at 6-months, all achieved the secondary outcomes of drug persistence at 6-months, corticosteroid-free remission and normalization of biomarkers (CRP, FCP) by end of induction, and maintained this through to 6-months. Adverse events occurred in 75% (3/4), 50% (2/4) of which were serious (requiring hospitalisation) within the 6-month follow up period. Patient 2 (Table 1), a 25-year-old female vaccinated with no comorbidities, was hospitalised for moderate-severity COVID. Patient 4 (Table 1), a 41 year-old female without significant comorbidities, was hospitalised for complicated cystourethritis. Two patients developed acne.</p><p><b><i>Conclusion:</i></b> This real-world data in Australia supports the efficacy of upadacitinib as another therapeutic option in the biologic-experienced IBD cohort. It is noted that the serious adverse event rate is higher than previously reported in safety trials which highlights the importance of ongoing real-world monitoring of this medication.</p><p><b>230</b></p><p><b>Machine learning with natural language processing to identify cases of Barrett’s oesophagus from electronic endoscopy reports</b></p><p><b>Madoka Inoue</b><sup>1,3</sup>, Hideo Tohira<sup>2,4,5</sup>, James Chen<sup>3</sup>, Shiv Meka<sup>6</sup>, Spiro Raftopoulos<sup>1,5,7</sup> and Krish Ragunath<sup>1,3</sup></p><p><sup>1</sup><i>Curtin Medical School, Curtin University, Perth, Australia;</i> <sup>2</sup><i>Curtin School of Nursing, Curtin University, Perth, Australia;</i> <sup>3</sup><i>Department of Gastroenterology, Royal Perth Hospital, Perth, Australia;</i> <sup>4</sup><i>Department of Emergency Medicine, Chibanishi General Hospital, Japan;</i> <sup>5</sup><i>UWA Medical School, University of Western Australia, Perth, Australia;</i> <sup>6</sup><i>Health in a Virtual Environment, East Metropolitan Health Service, Perth, Australia;</i> <sup>7</sup><i>Department of Gastroenterology, Sir Charles Gairdner Hospital, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Accurately identifying Barrett's oesophagus (BO) cases from electronic endoscopy reports is crucial for epidemiological studies but is often complicated by limitations in diagnostic coding systems and reporting structures. Few studies have applied natural language processing (NLP), a machine learning application for text classification, for this purpose. Thus, this study aimed to 1) develop machine learning models to identify BO cases using NLP to generate features from free-text descriptions in electronic endoscopy reports, and 2) evaluate the predictive performance of these models.</p><p><b><i>Methods:</i></b> This retrospective observational study utilised data from electronic endoscopy reports of patients (age ≥18 years) who underwent upper gastrointestinal endoscopy between January 1999 and December 2023, at four teaching hospitals in Perth, Western Australia. Endoscopists usually complete these reports post-procedure, including two free-textual sections: endoscopic findings (Findings) and a summary (Conclusion). BO cases were manually identified from a 20% random sample of these reports through free-text review. Three corpora were then created: 1) \"Findings\" only, 2) \"Conclusion\" only, and 3) \"Findings & Conclusion\". The sampled reports were divided into 70% for training and 30% for testing. NLP was used to compute the term frequency-inverse document frequency of each word, ranking their relevance. Three machine learning models—Random Forest (RF), Support Vector Machine (SVM), and XGBoost (XGB)—were developed based on each corpus. Optimal parameters were determined through 5-fold cross-validation, and model performance was evaluated using F1-measure (harmonic mean of recall and precision), recall (sensitivity), and precision (positive predictive value).</p><p><b><i>Results:</i></b> Among 186,896 electronic endoscopy reports, 37,396 were randomly sampled. Of the sampled reports, 42 and 90 were missing in the “Findings” and “Conclusion” sections, respectively. These reports were excluded when deriving models. A total of 26,177 reports were used for training and 11,219 for testing. We found that XGB performed best with an F1measure of 0.940, recall of 0.940, and precision of 0.939, derived using the combined corpus \"Findings & Conclusion\" as features. This was followed by RF with the combined corpus, achieving an F1-measure of 0.937, recall of 0.947, and precision of 0.928. SVM with the combined corpus attained an F1-measure of 0.922, recall of 0.895, and precision of 0.950.</p><p><b><i>Conclusion:</i></b> The machine learning model, using free-text findings and a summary in the endoscopy report as inputs, could identify BO cases with high recall and precision. Further improvement might involve including additional information like patient demographics and leveraging large language models for word embedding.</p><p>\n \n </p><p><b>238</b></p><p><b>Increased risk of future advanced neoplasia in individuals that have synchronous adenomas and clinically significant serrated polyps</b></p><p><b>Geraldine Laven-law</b><sup>1</sup>, Erin Symonds<sup>1,2</sup>, Kalindra Simpson<sup>1,2</sup>, Michelle Coats<sup>2</sup>, Mahinda De Silva<sup>2</sup>, Paul Hollington<sup>3</sup>, Charles Cock<sup>1,2</sup> and Molla M Wassie<sup>1</sup></p><p><sup>1</sup><i>Flinders University, College of Medicine and Public Health, Flinders Health and Medical Research Institute, Adelaide, Australia;</i> <sup>2</sup><i>Department of Gastroenterology and Hepatology, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia;</i> <sup>3</sup><i>Department of Colorectal Surgery, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Colorectal cancer (CRC) commonly develops from pre-cancerous neoplasia through the adenoma-carcinoma and serrated pathways. Individuals with prior history of adenoma and/or clinically significant serrated polyp (CSSP) are considered at above-average risk for CRC and undergo colonoscopy surveillance at intervals recommended by national guidelines. While individuals with synchronous adenoma and CSSP are recommended the same surveillance colonoscopy interval as those with only CSSP, there is limited evidence to support this recommendation. This study determined whether synchronous adenomas and CSSP increase the risk of future advanced neoplasia compared to no neoplasia, prior adenoma, or prior CSSP.</p><p><b><i>Methods:</i></b> This was a retrospective analysis of data from patients enrolled within a South Australian CRC surveillance program, and undergoing colonoscopies between 2010 – 2023 inclusive. Included patients were those that had a finding of no neoplasia or pre-cancerous neoplasia (adenoma and/or CSSP), who received a recommended surveillance interval and underwent another complete colonoscopy. Patients with inflammatory bowel disease, organ transplants, or CRC syndromes were excluded. Demographics and colonoscopy findings were extracted from clinical databases. Advanced neoplasia was defined as adenocarcinoma, advanced adenoma (adenoma ≥ 10 mm, high-grade dysplasia, and/or villous change), and/or advanced CSSP (sessile serrated lesions or hyperplastic polyps ≥ 10 mm, with dysplasia, and/or any traditional serrated adenoma). Multivariable Cox regression determined the effect of prior neoplasia on risk for developing future advanced neoplasia, controlling for age, sex, and colonoscopy interval. P < 0.05 was considered statistically significant.</p><p><b><i>Results:</i></b> A total of 11,134 colonoscopy pairs were included; 3,680 (33%) patients had no neoplasia, 5,884 (53%) had adenoma, 773 (7%) had CSSP, and 797 (7%) had synchronous adenoma and CSSP resected at the first colonoscopy of the pair. Patients were aged a median 65 (interquartile range 57 – 72) years, and 53% were male. Advanced neoplasia was found in 12% (1,336/11,134) of subsequent colonoscopies, but in 26% (140/536) of those with initial synchronous adenoma and CSSP when at least one lesion was advanced. Patients with synchronous advanced adenoma and non-advanced CSSP developed advanced neoplasia earlier than their advanced adenoma-only and non-advanced CSSP-only counterparts (Figure, p < 0.05).</p><p><b>239</b></p><p><b>Small bowel metastatic melanoma – a case report</b></p><p><b>Keith Brick</b> and Montri Gururatsakul</p><p><i>Queensland Health, Cairns, Australia</i></p><p><b><i>Introduction:</i></b> Melanoma is known to metastasize widely. The most frequent sites for metastatic melanoma are lymph nodes, lungs, liver, brain, bone and adrenal glands (1), but rarely gastrointestinal tract. The most common site of melanoma metastases to the gastrointestinal (GI) tract is the small intestine (1, 2). This case study reports a patient with small bowel metastatic melanoma who presented with recurrent iron deficiency anaemia.</p><p><b><i>Case Report:</i></b> A 73 year old male presented with iron deficiency anaemia. He initially had upper endoscopy and colonoscopy which were unremarkable, and subsequently had video capsule endoscopy which found a non bleeding ulcerated mass lesion at the proximal jejunum. He has a background of previous cholecystectomy, diverticular disease, multiple SCC and BCCs excisions, and in 2021 he had a melanoma in situ excised from his upper lip with at least 3 mm margins. A CT Enteroclysis identified a short segment (49mm) of abnormal mural thickening of the small bowel with a nodular appearance with some dilatation of the proximal bowel loop (figure 1). The lesion was not seen on a push enteroscopy. He underwent antegrade double balloon enteroscopy and a suspicious medium-sized ulcerated mass with no bleeding was found in the mid-jejunum, which was biopsied and tattooed (figure 2). The histopathology was non diagnostic. His case was discussed at both at radiology and histology MDT, and referred for surgical resection. He underwent successful robotic small bowel resection which has confirmed a diagnosis of metastatic melanoma. Subsequent somatic mutation testing for BRAF, KIT and NRAS were negative. He is now being considered for immunotherapy.</p><p><b>References</b></p><p>\n 1. <span>Liang, KV</span>, <span>Sanderson, SO</span>, <span>Nowakowski, GS</span>, <span>Arora, AS</span>. <span>Metastatic Malignant Melanoma of the Gastrointestinal Tract</span>. <i>Mayo Clinic Proceedings.</i> <span>2006</span> <span>81</span>(<span>4</span>) <span>511</span>-<span>16</span>. https://doi.org/10.4065/81.4.511</p><p>\n 2. <span>Lens, M</span>, <span>Bataille, V</span>, <span>Krivokapic, Z</span>. <span>Melanoma of the small intestine</span>. <i>Lancet Oncol.</i> <span>2009</span>; <span>10</span> (<span>5</span>): <span>516</span>–<span>521</span>. doi: https://doi.org/10.1016/S1470-2045(09)70036-1</p><p><b>240</b></p><p><b>A large choledochoduodenal fistula – a case report</b></p><p><b>Keith Brick</b>, Montri Gururatsakul and Shihaz Hussain</p><p><i>Queensland Health, Cairns, Australia</i></p><p><i><b>Introduction</b>:</i> A choledochoduodenal fistula is an abnormal communication between the common bile duct & the duodenum. It is often secondary to PUD, cholelithiasis, malignancy or iatrogenic (1). Presenting symptoms of cholangitis (fever, jaundice & abdominal pain) are common. This is a case report of an asymptomatic large choledochoduodenal fistula.</p><p><i><b>Case Report</b>:</i> A 65 year old female presented to hospital with hepatic encephalopathy & haematemesis. She has a background of Child-Pugh B cirrhosis secondary to Hepatitis C & alcohol on regular variceal screening, recently diagnosed metastatic rectal adenocarcinoma for palliative treatment, previous laparotomy for cholecystectomy & H. pylori infection. Of relevance she did not have a history of peptic ulcer disease (PUD), no recent biliary tract stones & was asymptomatic with no signs of cholangitis.</p><p>An upper endoscopy for bleeding was performed & identified a large 11mm choledochoduodenal fistula in the first part of the duodenum (fig 1), confirmed by bile draining through the fistula. The major papilla appeared normal without evidence of previous sphincterotomy. Previous staging CT abdomen for rectal cancer showed pneumobilia although no fistula apparent. Blood tests at presentation revealed a raised total bilirubin of 43. Liver enzymes ALP 87U/L, GGT 15U/L, ALT 24U/L & mildly raised AST 42U/L consistent with known decompensated cirrhosis. A cholestatic picture was not expected given the large size of the choledochoduodenal fistula. Due to her co-morbidities, dedicated imaging was not undertaken to further investigate, however a CT abdomen for a separate indication did identify the fistula (fig 2). Four previous surveillance UGIEs reported duodenal diverticulum, however no fistula documented. Her metastatic malignancy was diagnosed 6 weeks prior to the UGIE that identified the fistula.</p><p><b>Reference</b></p><p>\n 1. <span>Wu, MB</span>, <span>Zhang, WF</span>, <span>Zhang, YL</span>, <span>Mu, D</span>, <span>Gong, JP</span>. <span>Choledochoduodenal fistula in Mainland China: a review of epidemiology, etiology, diagnosis and management</span>. <i>Ann Surg Treat Res.</i> <span>2015 Nov</span>; <span>89</span> (<span>5</span>) <span>240</span>-<span>6</span>. https://doi.org/10.4174/astr.2015.89.5.240</p><p><b>245</b></p><p><b>An unusual cause of dysphagia</b></p><p><b>Eliza Flanagan</b><sup>1,2</sup>, Carl Cosgrave<sup>1,2</sup>, Irene Lu<sup>1,2</sup> and Alvin Ting<sup>1,2</sup></p><p><sup>1</sup><i>Barwon Health, , Australia;</i> <sup>2</sup><i>Monash University, Australia</i></p><p><b><i>Introduction:</i></b> The most common causes of dysphagia include intrinsic oesophageal pathology, such as motor disorders and obstructive lesions. Extrinsic conditions are rarer and usually occur secondary to mediastinal masses or vascular compression. Mediastinal masses comprise a wide variety of benign and malignant lesions and are typically identified incidentally or due to investigations performed for symptoms arising from mass effect. The differential diagnoses for mediastinal masses include thymoma, neurogenic tumours, lymphomas, cysts and germ cell tumours. Symptoms secondary to mass effect may include dyspnoea, cough, chest discomfort, dysphagia, or neurologic issues such as Horner’s syndrome. Imaging via CT chest provides detailed information regarding location and assists with differential diagnosis. Patient management relies on tissue diagnosis obtained via biopsy or during planned resection. Inflammatory myofibroblastic tumours (IMTs) are a rare intermediate-grade neoplasm, considered to be a subtype of sarcoma. They have high recurrence rates following resection and low metastatic potential [1]. They are most often found in children, and occur predominantly in the abdomen (up to 75%), lung, pelvis and retroperitoneum; however, any site can be involved [1, 2]. Most cases have a benign course and depending on the location, are often asymptomatic. Diagnosis is made by histologic findings characterized by spindle cell proliferation and an inflammatory infiltrate [1]. The anaplastic lymphoma kinase (ALK) gene has a critical role in the biology of many IMTs, and approximately 50% of IMTs contain a translocation in the ALK gene, resulting in tyrosine kinase activation. Complete surgical resection is the standard of care [1, 2] and if recurrence occurs, re-resection would be offered plus consideration of chemotherapy [3].</p><p><b><i>Case Report:</i></b> A 41-year-old lady with no significant past medical history was referred to hospital with chest discomfort and mildly elevated troponin 42ng/L [0-40]. She described a history of four months of progressive dysphagia to both solids and liquids, with worsening dyspnoea and orthopnea. Her electrocardiogram was normal and repeat troponin was stable. A computed-tomography (CT) scan of her chest was performed which demonstrated a large posterior mediastinal mass measuring 60x50x70mm in size, with compression of the oesophagus and trachea. She underwent an endoscopic ultrasound which was unable to pass the extrinsic compression but core lesional biopsies (fine needle biopsy) were able to be taken to expedite diagnosis. She subsequently underwent a thoracotomy and complete resection of the mass, with histopathology confirming an inflammatory myofibroblastic tumour with ALK gene rearrangement. Following tumour resection, her dysphagia resolved; and she is being followed up with regular surveillance CT imaging.</p><p><b>References</b></p><p>\n 1. <span>Siemion, K.</span>, et al., <span>What do we know about inflammatory myofibroblastic tumors? - A systematic review</span>. <i>Adv Med Sci</i>, <span>2022</span>. <span>67</span>(<span>1</span>): p. <span>129</span>-<span>138</span>.</p><p>\n 2. <span>Kovach, S.J.</span>, et al., <span>Inflammatory myofibroblastic tumors</span>. <i>J Surg Oncol</i>, <span>2006</span>. <span>94</span>(<span>5</span>): p. <span>385</span>-<span>91</span>.</p><p>\n 3. <span>Wang, Q.A.</span>, et al., <span>Update of Diagnosis and Targeted Therapy for ALK(+) Inflammation Myofibroblastic Tumor</span>. <i>Curr Treat Options Oncol</i>, <span>2023</span>. <span>24</span>(<span>12</span>): p. <span>1683</span>-<span>1702</span>.</p><p><b>246</b></p><p><b>Prolonged wireless ambulatory reflux testing - technical success and clinical findings</b></p><p><b>Ash Rankine</b> and Emily Stimson and <b>Magnus Halland</b></p><p><i>Newcastle Gastroenterology, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastro-oesophageal reflux disease (GORD) is common, but symptoms overlap with many other upper gastrointestinal conditions and objective evidence of GORD on endoscopy is uncommon. Thus, an objective diagnosis of GORD is often sought with ambulatory 24-hour catheter-based pH test. However, the test is limited by tolerability and false negative diagnoses due to the relatively short duration of monitoring. Endoscopically placed, wireless prolonged pH testing is another alternative. We aimed to determine; (i) Technical success of introducing a wireless pH testing service, (ii) Indications and outcomes of wireless pH testing and (iii) Compare outcomes among patients who underwent both standard 24-hour pH impedance testing AND subsequent prolonged ambulatory wireless testing.</p><p><b><i>Methods:</i></b> Chart review of patients who underwent wireless pH testing at a single gastroenterology practice between April 2022 and April 2024. Descriptive analysis of clinical characteristics and pH variables was performed.</p><p><b><i>Results:</i></b> 40 wireless pH studies were conducted, all were initially technically successful, however two studies had premature dislodgement (<24h). LA Grade B esophagitis was observed in 5 patients. All tests were performed off PPI therapy and gastric pH was confirmed to be <4 in all patients prior to device placement. The mean age was 47.5 years (range 21-74) and 60% were female. The mean duration of pH data collection was 75.2 hours (SD 11.2). The indication for the test was “Reflux “in 78%, “Atypical GORD” in 15% and “globus or vomiting” in 7%. A positive study, defined as at least one 24-hour period with >6.5% esophageal acid exposure (AET), occurred in 18 patients (45%). Graph 1 shows the proportion of abnormal days of acid exposure among all patients. 3 of the 40 patients had completed an ambulatory pH testing prior to the prolonged wire-less test. In one of these 3 patients severe GORD was present on prolonged wireless testing whereas a concordant result was present in 2. There were no anesthetic or significant endoscopic complications. Mild and moderate chest discomfort was reported in 5 patients and 3 patients respectively.</p><p><b>271</b></p><p><b>The prevalence and predictors of oesophago-pharyngeal reflux in lung transplant recipients</b></p><p><b>Alyce Lonsdale</b>, Mary Eid, David Darley, Mark Danta, Nick Olsen and Santosh Sanagapalli</p><p><i>St Vincent's Clinical School, University of New South Wales Medicine, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Lung transplantation is an important therapeutic option for patients with end-stage lung disease, however, outcomes are poorer than other types of solid organ transplantation. While gastro-oesophageal reflux disease has been linked to lung allograft rejection, existing evidence is of poor quality. This study hypothesised that microaspiration of gastric contents via the pharynx into the lungs contributes to lung allograft injury. Accordingly, it aims to (1) identify the incidence of proximal oesophageal reflux events among lung transplant recipients; and (2) assess the effect of sex, age, body mass index (BMI), oesophageal dysmotility, and the type of pretransplant end-stage lung disease as risk factors for oesophago-pharyngeal reflux.</p><p><b><i>Methods:</i></b> This cross-sectional study assessed lung transplant recipients at three to six months post-transplant, who underwent oesophageal multichannel intraluminal manometry and 24-hour pH testing between March and August 2023. Proximal and distal reflux episodes, and total acid exposure time (AET) were measured using a catheter with one distal pH-probe and eight impedance rings, spanning from 6cm above the manometrically determined lower oesophageal sphincter (LOS).</p><p><b><i>Results:</i></b> Among the fourteen lung transplant recipients included in the study (8 [57.1%] female; median age, 56.5 years [IQR, 46-62]; median BMI, 22.7 kg/m<sup>2</sup> [IQR, 20.2-27.9]), six patients (42.9%) experienced an abnormal number of total impedance-detected reflux episodes, and eight patients (57.1%) had an abnormal total AET. Five patients (35.7%) experienced an abnormal number of impedance-detected proximal oesophageal reflux episodes, with three (21.4%) and seven (50.0%) experiencing an abnormal number of acidic and weakly acidic events, respectively. Univariate Poisson regression with bootstrapped confidence intervals (CI) identified that male sex (IRR=2.08, 95%CI [1.01,5.17], p=0.04), and a reduction in oesophageal motility parameters such as LOS basal pressure respiratory mean (IRR=0.96, 95%CI [0.94,0.98], p<0.001), LOS residual pressure median (IRR=0.93, 95%CI [0.88, 0.98], p=0.004) and distal contractile integral (IRR=0.63, 95%CI [0.48, 0.77], p=0.001), in addition to the presence of cystic fibrosis (IRR=1.77, 95%CI [1.23, 3.00], p=0.04) and the absence of pretransplant chronic obstructive pulmonary disease (IRR=0.48, 95%CI [0.16, 0.96], p<0.05), were predictors of increased proximal oesophageal reflux episodes (p<0.05). BMI (IRR=0.982, 95%CI [-0.168,0.079], p=0.737) and age (IRR=0.975, 95%CI [-0.085,0.018], p=0.124) were not statistically significant predictors.</p><p><b><i>Conclusion:</i></b> This study concludes that lung transplant recipients have greater episodes of proximal oesophageal reflux, compared to a healthy population, which may have implications for patient outcomes post-transplantation. Further research should explore the relationship between proximal oesophageal reflux episodes and lung function in lung transplant recipients.</p><p><b>273</b></p><p><b>Clinical characteristics and current clinical practice in patients with acute pancreatitis at a large tertiary centre</b></p><p><b>Cindy Ho</b>, Hardesh Dhillon, Kyle Williams, Eliza Flanagan, Faris Gondal, Sally Bell and Simon Hew</p><p><i>Monash Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Acute pancreatitis (AP) is a prevalent and potentially serious gastrointestinal illness. Contemporary studies evaluating the characteristics and management of patients with AP in large Australian tertiary centres are limited. Our study aims to detail the clinical characteristics of patients with AP and evaluate current clinical practices.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort study including all inpatients with AP at a large tertiary health service in Melbourne, Australia, from May 2022 to 2023. Data on demographics, fluid resuscitation, interventions, and nutrition were collected. Serious complications were defined as necrotising pancreatitis (NP), intensive care unit (ICU) admission, or death. For gallstone-related AP, time to laparoscopic cholecystectomy and readmission rates were calculated.</p><p><b><i>Results:</i></b> 553 patients with 639 admissions had AP. Most were male (51.4%) with a median age of 54 years (IQR 38-70) and BISAP of 1 (IQR 0-1). Gallstones (35.8%) were the commonest cause, followed by alcohol (26.6%) and idiopathic or unclear aetiology (16.6%). The mean intravenous fluid, mostly Hartmann’s (87.3%), administered within 24 hours of AP diagnosis was 4.5 litres (SD 0.4). NP, observed in 32 patients (5.0%), was associated with increased length of stay (LOS) (p<0.0001) and higher intervention rates for peri-pancreatic collections (OR 5.9, 95% CI 2.0-17.5) (Figure 1). Interventions included endoscopic (56.3%), percutaneous (18.8%), surgical (18.8%), or combined approaches (6.3%). The median time to drainage was 23.5 days (IQR 22.0-32.0). Nutritional support was required in 39 patients (6.1%), particularly those with NP (OR 4.6, 95% CI 1.8-11.5). The median time to light diet was 2 days (IQR 1-3). 36 patients needed ICU admission (5.6%), with a median ICU stay of 4.2 days (IQR 1.9-9.7) and a total hospital stay of 18.0 days (IQR 9.5-43.0). Higher BISAP scores correlated with increased ICU admissions (OR 10.9, 95% CI 5.2-22.2). Overall median LOS was 4 days (IQR 2-6), with a 2.2% mortality rate. 154 patients with gallstone-associated AP underwent laparoscopic cholecystectomy (80.7%), primarily as inpatients (76.0%), with a median time to surgery of 3 days (IQR 2-4) and 39 days (IQR 19-61) for outpatients. 37 patients (19.3%) did not undergo surgery due to comorbidities, patient wishes, or death. Nine readmissions occurred, three preventable by timely surgery.</p><p><b>274</b></p><p><b>Autoimmune enteropathy associated with COVID-19 infection - a case report</b></p><p><b>Wei Ling Teh</b>, Siaw Chai, Dilini Gunawardena and Jesica Makanyanga</p><p><i>Fiona Stanley Hospital, Perth, Australia</i></p><p><b><i>Introduction:</i></b> Autoimmune enteropathy (AIE) is a rare cause of chronic diarrhea that can occur as a primary condition or secondary to another immune-mediated process. Autoantibodies are not necessary for diagnosis, making AIE challenging to diagnose due to its overlap with other diseases characterized by villous atrophy. There is no standard treatment. Typically, patients are treated with glucocorticoids, sometimes combined with other immunosuppressive agents. This case highlights an AIE case whose symptoms began following COVID-19 infection, successfully managed with prednisolone and vedolizumab.</p><p><b><i>Case report:</i></b> A previously well 31-year-old woman was referred in March 2023 for months of severe watery diarrhea and vomiting, leading to electrolyte disturbances and weight loss. The diarrhea began after a mild COVID-19 infection in December 2022 and worsened after taking amoxicillin for an ear infection. She was not on regular medications. Her aunt had Crohn’s disease. ANA, ANCA, and coeliac antibodies were negative. Immunoglobulin levels were normal. HLA-B27 was negative, but HLA-DQ 2.5 indicated susceptibility to coeliac disease. Faecal tests were negative for infective causes. A secretory diarrhea screen (calcitonin, chromogranin A, gastrin, VIP) was negative. Endoscopy revealed mild gastritis and atrophic mucosa in the duodenum and terminal ileum, with normal colonic mucosa. Duodenal and ileal samples showed marked villous atrophy, active neutrophilic inflammation, absence of goblet cells, and a paucity of plasma cells and intraepithelial lymphocytes. Colonic biopsies showed focal active colitis without ulceration or CMV inclusion bodies. Anti-enterocyte and anti-goblet cell immunofluorescent staining were negative. She did not experience sustained benefit from corticosteroids or infliximab. Azathioprine was discontinued due to pancreatitis. Empirical trials of gluten free diet, octreotide and rifaximin were ineffective. In August 2023, vedolizumab, slow corticosteroid taper and partial parenteral nutrition (PN) were started. She showed gradual clinical improvement and reduced dependence on PN, eventually stopping it in April 2024. Repeat endoscopy in February 2024 showed epithelial cell regeneration and improved cryptitis, though goblet cells were still absent. She is currently on vedolizumab and 15mg of prednisolone daily, and in symptomatic remission.</p><p><b>275</b></p><p><b>The role of drug and alcohol services for patients with alcohol-associated acute pancreatitis at a large tertiary centre</b></p><p><b>Cindy Ho</b>, Hardesh Dhillon, Alex Mitropoulos, Eliza Flanagan, David Jacka, Sally Bell and Simon Hew</p><p><i>Monash Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Alcohol is a common cause of acute pancreatitis (AP), and ongoing consumption increases the risk of recurrent episodes. No specific guidelines exist for behavioural or pharmacological interventions to reduce recurrence of alcohol-associated AP. Studies exploring the role of addiction medicine for patients with alcohol-induced pancreatitis are limited. Our study aims to describe the utilization of the addiction medicine unit (AMU), a drug and alcohol physician-led inpatient consultation service, for patients admitted to a tertiary hospital with alcohol-associated AP.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort study including all inpatients diagnosed with alcohol-associated AP at a tertiary health service in Melbourne, Australia between May 2022 to 2023. Data on AMU referrals and assessment, recommended interventions, and outpatient follow-ups were collected. Re-admission rates for AP within this timeframe were calculated. Serious complications of AP were defined as those with necrotising pancreatitis, requiring intensive care unit (ICU) admission, or death.</p><p><b><i>Results:</i></b> 141 patients with 170 admissions were admitted with alcohol-associated AP. Most were males (76.6%), with a median age of 47 years (IQR 35-57) and median BISAP score of 0 (IQR 0-1). Fourteen patients (8.2%) had necrotizing pancreatitis, 13 (7.6%) required ICU admission, and 2 (1.4%) patients died. Fifty-seven patients (33.5%) were referred to the AMU. Of those referred, 98.2% were reviewed, either in person (73.2%) or via phone advice to clinicians (26.8%). Multi-disciplinary interventions including medications for addiction and outpatient services were recommended most (53.0%), followed by outpatient services alone (30.3%), and medications alone (16.7%). Outpatient services included follow-up in the AMU outpatient clinic, or more commonly, self-referrals to SECADA, a consortium for drug and alcohol addiction services including counselling and detox programs<b>.</b> 44 patients were recommended to commence or up-titrate medications for addiction by the AMU, which included naltrexone (61.4%), topiramate (38.6%), baclofen (6.8%), disulfiram (2.3%), either as single agents or in combination. Eighteen patients were re-admitted with alcohol-associated AP, with 11 (61.1%) not seen by the AMU during their initial admission. Of the 113 patients (66.5%) not referred to the AMU, contributing factors included patient refusal and weekend admissions.</p><p><b><i>Conclusion:</i></b> Within the limits of a single centre cohort with a short follow-up interval, our study demonstrated that approximately one-third of patients with alcohol-associated AP were referred to the AMU. Combination pharmacological and outpatient follow up were the most common interventions recommended. Efforts to improve referral patterns during index admissions may be helpful to reduce readmissions for alcohol-associated AP.</p><p><b>293</b></p><p><b>Enterocolitis with rectal and ileal stenosis: A rare presentation of metastatic urothelial carcinoma</b></p><p><b>Nicholas Smith</b>, Andrew Taylor and Jennifer Borowsky</p><p><i>Princess Alexandra Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Urothelial carcinoma is the most common histologic subtype accounting for approximately 90% of bladder cancers [1]. The most common sites of distant metastasis include liver, lung, and lymph nodes. Gastrointestinal tract involvement is rare [1].</p><p><b><i>Case Report:</i></b> An 81-year-old man presented with 3-months of vomiting, diarrhoea and abdominal pain. His background included; hypertension, benign prostatic hypertrophy and stage 3 chronic kidney disease. He was a non-smoker and lacked a family history of colorectal or urological malignancy. His medications included; perindopril, atenolol, aspirin and dutaasteride-tamsulosin. There was no non-steroidal anti-inflammatory exposure. Computer tomography revealed extensive mural thickening of both his small and large bowel suggestive of enterocolitis with pneumatosis intestinalis and a thickened bladder wall. Blood investigations were unremarkable apart from his known renal dysfunction and a mild leukocytosis of 11.5x10<sup>9</sup>/L and eosinophilia of 0.40x10<sup>9</sup>/L. C-reactive protein was 11mg/L. Colonoscopy showed congested and nodular mucosa throughout the entire colon with rectal and terminal ileal steosis, only traversable with a paediatric gastroscope (Figure 1.A). There was mucosal friability and loss of the normal haustral folds and vascular pattern. Histology revealed malignant cells present within lymphatics of the terminal ileum and colonic specimens. Immunohistochemistry showed positive staining of these cells with CK7, GATA3, and 34βE12 (Figure 1.B). There was no significant staining with CK20, PAX8, p53, TTF1 or CDX2. Urine cytology found atypical urothelial cells suggestive of a high-grade urothelial cell carcinoma. Cystoscopy revealed widespread erythema and cystitis with bullous areas with histology confirming the diagnosis of urothelial carcinoma, plasmacytoid subtype. Fludeoxyglucose positron emission tomography showed the expected uptake in the bladder and small and large bowel with small volume avid ascites. With the diagnosis of metastatic urothelial carcinoma, the patient was referred for palliative chemotherapy.</p><p><b><i>Discussion:</i></b> The mechanism of urothelial carcinoma related stenosis remains unclear. With rectal invasion, it has been hypothesized that a locally aggressive cancer of the bladder can penetrate Denonvilliers’ fascia and encircle the rectum [2]. It has also been thought that the cancer cells may spread along the lateral bladder pedicles to reach the posterior rectal wall [2]. Several case reports have detailed gastrointestinal tract metastases of urothelial carcinoma [2,3,4,5]. Wasfie [5] presents a case with stenotic small bowel disease. Liu [3] and Takeuchi [2] report cases with stenotic rectal disease. Ours is the only report with extensive entero-colitis with both rectal and ileal stenosis. This highlights the important but rare differential of metastatic disease in presentation of enterocolitis.</p><p><b>References</b></p><p>\n 1 <span>Shinagare, AB</span>, <span>Ramaiya, NH</span>, <span>Jagannathan, JP</span>, <span>Fennessy, FM</span>, <span>Taplin, ME</span>, <span>Van den Abbeele, AD</span>. <span>Metastatic pattern of bladder cancer: correlation with the characteristics of the primary tumor</span>. <i>AJR Am J Roentgenol.</i> <span>2011 Jan</span>; <span>196</span>(<span>1</span>): <span>117</span>-<span>22</span>.</p><p>\n 2 <span>Takeuchi, H</span>, <span>Tokuyama, N</span>, <span>Kuroda, I</span>, <span>Aoyagi, T</span>. <span>Annular rectal constriction caused by infiltrating bladder cancer: A case report</span>. <i>Mol Clin Oncol.</i> <span>2016 Dec</span>; <span>5</span>(<span>6</span>): <span>842</span>-<span>844</span>.</p><p>\n 3 <span>Liu, YH</span>, <span>Pu, TW</span>, <span>Yu, HW</span>, <span>Kang, JC</span>, <span>Yen, CH</span>, <span>Chen, CY</span>. <span>Invasive urothelial carcinoma of urinary bladder presenting with annular constriction and mimicking proctitis observed by colonoscopy: A case report</span>. <i>Int J Surg Case Rep.</i> <span>2021 May</span>; <span>82</span>: <span>105785</span>.</p><p>\n 4 <span>Tse, CS</span>, <span>Elfanagely, Y</span>, <span>Fine, S</span>. <span>Metastatic urothelial bladder cancer involving the rectum/Practical Gastro</span>. <span>2020</span> Nov; Vol XLIV, Issue 11.</p><p><b>296</b></p><p><b>Gastro-oesophageal reflux, determined with 24-hour pH-impedance monitoring, is highly prevalent in patients with chronic respiratory conditions, with many being asymptomatic or having extra-oesophageal symptoms</b></p><p><b>Michael Yulong Wu</b><sup>1,2,3</sup>, Ross Hansen<sup>1</sup>, Julia Mathers<sup>2</sup>, Vincent Liu<sup>2</sup>, David Joffe<sup>1,2</sup> and May YW Wong<sup>1,2</sup></p><p><sup>1</sup><i>Royal North Shore Hospital, Sydney, Australia;</i> <sup>2</sup><i>Northern Clinical School, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Faculty of Health Science and Medicine, Bond University, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> It is theorised that gastro-oesophageal reflux disease (GORD) can precipitate respiratory conditions due to aspiration of gastric contents into the respiratory tract provoking inflammation and neural reflexes which may trigger tracheobronchial constriction and hyperresponsiveness. However reflux symptoms can be unreliable indicators of the presence or absence of reflux. The primary aim of this study is to examine the prevalence of GORD using objective 24-hour pH-impedance monitoring in patients with chronic respiratory diseases (chronic obstructive pulmonary disease, bronchiectasis, asthma, interstitial lung disease). Secondary aims were to determine whether oesophageal symptoms and extra-oesophageal symptoms could predict presence of GORD, and whether respiratory function testing reflected severity of GORD.</p><p><b><i>Methods:</i></b> This is a retrospective cohort study using data collected between 2003 – 2023 in a quaternary referral centre. Patients over 18 years, referred for 24-hour pH-impedance monitoring for investigations into respiratory disease were included. An AET >4.2% was positive for GORD. A patient reported symptom questionnaire was used to categorise patients into those with oesophageal symptoms and extra-oesophageal symptoms. Oesophageal symptoms included chest pain and heartburn, and extra-oesophageal symptoms included cough, recurrent airway infections, vocal changes and throat symptoms such as irritation, constant clearing and laryngopharyngitis.</p><p><b><i>Results:</i></b> A total of 438 patients were included. The mean age was 60 years. Concurrent asthma and COPD (72.1%, n=316) were the most common respiratory diagnoses. Almost half of all patients had GORD (49%, n=217). GORD was present in a large proportion of asymptomatic patients (38.0%, n=82) and those with extra-oesophageal symptoms (32.9%, n=71) (Figure 1). Chronic cough and throat symptoms were the most common extra-oesophageal manifestations of reflux (61.4%, n=269 and 29.8%, n=71). Those with recurrent airway infection had the highest proportion of patients with GORD (59%, n=27). There were no significant differences in FEV<sub>1</sub> (p=0.55) , FVC (p=0.42) or FEV<sub>1</sub>/FVC (p=0.99) between those with and without diagnosis of GORD.</p><p><b>310</b></p><p><b>Case report: ocrelizumab induced colitis</b></p><p><b>Karly Potts</b> and David Scott</p><p><i>Hunter New England Health, Newcastle, Australia</i></p><p><b><i>Introduction:</i></b> Ocrelizumab is a humanised anti CD20 monoclonal antibody that is the sole disease modifying therapy for primary progressive multiple sclerosis. Fourteen case reports describing ocrelizumab associated colitis have been published. The majority describe disease onset within a few weeks therapy initiation. We herein report a case of severe ocrelizumab induced colitis following five years of therapy.</p><p><b><i>Case report:</i></b> A 68-year-old male presented with a four-week history of non-bloody diarrhoea and associated generalised abdominal pain. Pertinent medical history consisted of primary progressive multiple sclerosis, managed with 6 monthly ocrelizumab for the proceeding five years. Abdominal CT revealed mild mural thickening from the caecum to the descending colon. Stool testing for was positive for Blastocystic species, but otherwise negative for bacterial, viral, and parasitic pathogens. Colonoscopy demonstrated multiple deep ulcers in the left colon and normal intervening mucosa. There was near complete denudation of the right colon. Biopsy showed extensive ulceration with focal ischaemic changes and an inflammatory infiltrate characterised by an absence of B cells (figure 1). CMV was excluded by serology and biopsy. The patient failed to improve following 48 hours of empirical intravenous ceftriaxone and metronidazole. Oral budesonide and 100mg intravenous methylprednisone were commenced for severe drug induced colitis. A surgical opinion was sought for consideration of colectomy, but symptoms improved following steroid initiation, and no intervention was required. Prednisone was commenced at 60mg daily, to be gradually tapered. On day 17 of prednisone therapy the patient experienced worsening abdominal pain. Inflammatory markers, previously down trending, had increased. Repeat CT abdomen demonstrated overall improved appearances, and stool culture was negative. Treatment was escalated to a three-day course of methylprednisone and tofacitinib added to ongoing budesonide. This resulted in clinical and biochemical improvement and was followed by prednisone taper. Three months later, the patient remained well, with normalisation of biochemical parameters. Budesonide and prednisone were weaned, and he continued tofacitinib.</p><p><b>325</b></p><p><b>Expect the unexpected: A rare case of duodenal-type follicular lymphoma</b></p><p><b>Joel Thio</b></p><p><i>Department of Gastroenterology and Hepatology, Logan Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Duodenal-type follicular lymphoma is a rare entity that usually follows an indolent course. Most cases usually present asymptomatic and are found incidentally on endoscopic examination of the small bowel. The most common finding on endoscopic examination is that of white polypoid nodules. We present a case of an incidental finding of duodenal-type follicular lymphoma in a 61-year-old male.</p><p><b><i>Case report:</i></b> A 61-year-old Indian male presented to our service for further investigation of his iron deficiency anaemia with symptoms of generalised fatigue without obvious bleeding. He had a background of hypertension, ischemic heart disease, and benign prostate hypertrophy. Regular medications included perindopril, clopidogrel, rosuvastatin, and tamsulosin with dutasteride. Laboratory investigations revealed a haemoglobin of 127 g/L and a ferritin of 29 micrograms/L. He had a recent colonoscopy which was normal.</p><p><b><i>Discussion:</i></b> Follicular lymphoma typically follows an indolent course, and management mainly involves close monitoring and commencing treatment once symptoms manifest. This case highlights the importance of increased vigilance of this condition with the potential for subtle appearances on endoscopy.</p><p><b>327</b></p><p><b>Does a restrictive blood transfusion strategy have better outcomes in upper gastrointestinal bleeding? Six years of real world data</b></p><p><b>Hirannya Karunadasa</b>, Daniel Clayton-chubb, Stuart Roberts, Gregor Brown and <b>Shara Ket</b></p><p><i>Alfred Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Transfusion of blood products is an important component of resuscitation in the management of upper gastrointestinal bleeding (UGIB). Randomised studies have suggested that use of a restrictive transfusion strategy is associated with reduced all-cause mortality and rebleeding rates. The applicability and generalisability of a restrictive transfusion strategy in clinical practice remains unclear. The aim of this study was to evaluate and compare outcomes of restrictive versus liberal transfusion strategies in patients with UGIB over a six-year period in a real-world setting.</p><p><b><i>Methods:</i></b> A retrospective audit of patients presenting with or developing UGIB during admission in a quaternary referral hospital between 2018 to 2023 was conducted. Participants were excluded if they had lower gastrointestinal bleeding, had exsanguinating bleeding, were managed with outpatient gastroscopy or refused transfusion of blood products. Data collected included demographics, pathology results, transfusions, interventions and outcome data. Patients with a 24-hour nadir haemoglobin between 70g/L and 90g/L were stratified into a liberal transfusion group if packed red blood cells (PRBC) were transfused in that 24-hour period or into a restrictive transfusion group if they did not receive PRBC. The primary outcomes were mortality and rebleeding within 30 days of UGIB.</p><p><b><i>Results:</i></b> Of the 1089 patients included, 413 (37.9%) patients had a 24-hour nadir haemoglobin between 70g/L and 90g/L qualifying for evaluation of restrictive versus liberal transfusion strategies. The male gender accounted for 64.4% (n=266/413) of patients. The median age was 72 years (IQR 57-82 years), and the median Charlson Comorbidity Index was 6 (IQR 4-8). The median 24-hour nadir Hb was 78g/L (IQR 74-84 g/L). The leading cause of bleeding was peptic ulcers at 35.1% (n=145/413), while 10.2% (n=42/413) of patients had variceal bleeding. Most patients were stratified into the liberal transfusion group with 298 (72.2%) patients being transfused PRBC within the first 24 hours, with a median of 2 units (IQR 1-3 units) transfused within 24 hours. Regarding primary interventions, 40.9% (n=169/413) of patients required endoscopic intervention, with 4 (1.0%) requiring angiographic intervention and 2 (0.5%) requiring surgical intervention. A significantly greater proportion of patients in the liberal transfusion group experienced rebleeding within 30 days (n=43/298, 14.4% vs n=8/115, 7.0%; p=0.04). Although a numerically higher occurrence of all-cause mortality within 30 days was noted in the liberal transfusion group, this difference did not reach statistical significance (n=27/298, 9.1% vs n=6/115, 5.2%; p=0.23). In terms of secondary outcomes, the liberal transfusion group had poorer outcomes with significantly higher proportions of cardiac and pulmonary complications, acute kidney injury and bacterial infection (see Table 1, p<0.05).</p><p><b><i>Conclusion:</i></b> In the management of UGIB, a restrictive transfusion strategy appears to be associated with a significantly lower proportion of rebleeding and complications within 30 days of UGIB. This lends strength to current guidelines recommending restrictive transfusion strategy in the management of non-exsanguinating UGIB.</p><p><b>328</b></p><p><b>The effectiveness of budesonide orodispersible tablets in the real-world is lower than in clinical trials: a multicentre cohort study</b></p><p><b>Sarah Taylor</b><sup>1</sup>, Emily Barwick<sup>2</sup>, Varan Perananthan<sup>3</sup>, Sarah Lucas<sup>1</sup>, Ayushi Chauhan<sup>1</sup>, Catherine Yu<sup>1</sup>, Katrina Tan<sup>1</sup>, Diana Lewis<sup>1</sup>, Chamara Basnayake<sup>4</sup>, Hamish Philpott<sup>5</sup>, Sanjay Nandurkar<sup>6</sup>, Rebecca Burgell<sup>3</sup> and Mayur Garg<sup>1,2</sup></p><p><sup>1</sup><i>Northern Health, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia;</i> <sup>3</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>4</sup><i>St Vincents Hospital, Melbourne, Australia;</i> <sup>5</sup><i>Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>6</sup><i>Eastern Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Eosinophilic oesophagitis (EoE) is a chronic immune-mediated disorder that causes oesophageal dysfunction secondary to eosinophil-predominant inflammation. A budesonide orodispersible tablet (BOT) formulation has been shown to induce clincohistological remission in 57% of patients after 6 weeks of treatment, with histological remission in 93%. Real-world data for this medication however is currently limited. Previous Pharmaceutical Benefits Scheme (PBS) prescribing criteria mandated evidence of histological remission as defined by a peak eosinophil count of fewer than 5 eosinophils per high power field (hpf) within 12 weeks, but this has now been changed to allow treatment for up to 48 weeks. This study aimed to evaluate the real-world efficacy and adherence of patients with EoE treated with BOT at five tertiary centres in Victoria and South Australia.</p><p><b><i>Methods:</i></b> A retrospective medical record review of patients aged 18 years and over with a confirmed histological diagnosis of EoE (>15 eosinophils per hpf) and that were treated with BOT between July 2019 until February 2024 at five tertiary centers was performed. Data collected included patient demographics, endoscopy reports, histopathology, clinical symptoms, and previous medical treatments. Outcomes were reported using descriptive statistics.</p><p><b><i>Results:</i></b> 83 patients (69 [83%] male, median age 37 [range 19-79] years) on 1mg BD BOT were identified, with follow-up data for median 11 (IQR 10-16) months following commencement of BOT. The peak median eosinophil count prior to commencement on BOTs was 40 (IQR 30-50) per hpf. Patients had a median duration of disease prior to BOT therapy of 3 (IQR 2-6) years. 65% of patients had an allergic diathesis (asthma, hay fever, eczema, allergic rhinitis, or an allergy). Other therapies had been trialed prior to BOT commencement in 92 % of patients, with the majority (81%) having had proton pump inhibitor therapy. 14 patients (17%) had required previous oesophageal dilatation. Prior to BOT therapy, 40% of patients had experienced a food bolus obstruction with none occurring post commencement of BOT. Fewer than half (47%) had a repeat gastroscopy performed within 12 weeks of BOT commencement (median 80 days, IQR 67-112). The median peak eosinophil count on repeat gastroscopy post induction with BOT was 2 (IQR 0-30). Histological remission was noted in 48 (58%), clinical remission (defined as absence of symptoms) in 35 (42%) and endoscopic remission (no endoscopic features of EoE) in 26 (32%). 14 (17%) of patients were noted on clinic review to be using the medication incorrectly, with none of these patients achieving histological remission. Adverse events were reported by 15% of patients, with the most common being altered taste and oesophageal candidiasis (6% and 4.76 %, respectively).</p><p><b>353</b></p><p><b>Intrusive endometriosis involving the small bowel: a case report</b></p><p><b>Thant Zaw</b><sup>1</sup>, Peter Boyd<sup>1,2</sup> and Montri Gururatsakul<sup>1,2</sup></p><p><sup>1</sup><i>Cairns Hospital, Cairns, Australia;</i> <sup>2</sup><i>James Cook University, Cairns, Australia</i></p><p><b><i>Introduction:</i></b> Endometriosis, a condition characterized by the presence of endometrial tissue outside the uterine cavity, is a well-known affliction affecting approximately 10% of women of reproductive age. However, the occurrence of endometriosis in the small bowel remains a rare and intriguing phenomenon. This is a case report of a patient with small bowel endometriosis.</p><p><b><i>Case report:</i></b> A 40-year-old woman with a history of severe endometriosis presented at the Emergency Department with severe, recurring abdominal pain localized around the peri-umbilical area. She reported minimal relief from analgesics and had one episode of vomiting along with a single occurrence of loose stool, without any signs of blood in the stool or diarrhea. Notably, she had undergone a lower segment Caesarean section in 2017. A CT scan of the abdomen and pelvis revealed multiple segments of thickened, inflamed small bowel near the terminal ileum, raising concerns of Crohn's disease (Picture 1). Subsequent colonoscopy revealed luminal narrowing at the terminal ileum without any obvious mucosal abnormalities, and a biopsy taken from the terminal ileum showed unremarkable findings. She was treated conservatively with bowel rest and a course of IV hydrocortisone followed by oral prednisolone with the plan for further evaluation with relook colonoscopy and MRI scan. Two weeks later, she returned to the ED with recurrent small bowel obstruction and signs of small bowel volvulus, indicating a possible closed-loop obstruction due to twisting of the mesenteric pedicle. The decision was made to perform a laparoscopic right hemicolectomy. During the surgery, cicatrizing lesions were observed in the terminal ileum, and the histopathology results confirmed the presence of endometriosis in the small bowel and appendix.</p><p><b>361</b></p><p><b>Correlation between colonic mural thickening and endoscopy findings</b></p><p>Osamah Al-obaidi<sup>1</sup>, Hydar El Jamaly<sup>2</sup>, Noureddin Al-Hajjiri<sup>2</sup> and Mouhannad Jaber<sup>2</sup></p><p><sup>1</sup><i>Concord Hospital, Sydney, Australia;</i> <sup>2</sup><i>Wollongong Hospital, Wollongong, Australia</i></p><p><b><i>Background and Aim:</i></b> Colonic mural thickening (MT) is often reported on standard CT examinations of the abdomen and pelvis. It often presents a dilemma for the clinician on whether any further evaluation is needed, especially in the absence of any set guidelines. Our aim is to evaluate the significance of colonic MT and to assess its correlation with colonoscopy.</p><p><b><i>Methods:</i></b> We conducted a comprehensive literature search using a strategy in Medline and this was extended to Pubmed and Embase. The studies included patients with increased Colonic wall thickness on CT scans, who underwent endoscopic evaluation. We used a random-effects model using pooled positive predictive value (PPV) with 95% confidence intervals (CI).</p><p><b><i>Results:</i></b> A total of 15 cohort studies examining 1596 patients were selected having undergone both CT and colonoscopy. Of the 1596 patients with MT, 1152 had an abnormal colonoscopy. In the presence of MT of 3mm or more, the pooled positive predictive value (PPV) of malignancy was 0.23 (95% CI: 0.16-0.33) and that of all pathology was 0.65 (95% CI: 0.47-0.80). In the presence of MT of >5mm, the pooled positive predictive value (PPV) of malignancy was 0.15 (95% CI: 0.09-0.24) and that of all pathology was 0.71 (95% CI: 0.54-0.83). In patients with MT in the right colon, the pooled PPV of malignancy was 0.14 (95% CI: 7.4-23.7) and that of all pathology was 0.34 (95% CI: 0.18-0.55) as shown in Figure (1). In the left colon MT groups, the pooled PPV of malignancy was 0.18 (95% CI: 0.12-0.26) and that of all pathology was 0.74 (95% CI: 0.53-0.88).</p><p><b>369</b></p><p><b>Food bolus obstruction: what factors prevent clinicians from performing biopsies for eosinophilic oesophagitis during acute endoscopy?</b></p><p><b>Melissa Carroll</b><sup>1</sup>, Matilda Surtees<sup>1</sup> and Nick J Talley<sup>1,2</sup></p><p><sup>1</sup><i>NSW Health - John Hunter Hospital, Newcastle, Australia;</i> <sup>2</sup><i>University of Newcastle, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> Eosinophilic oesophagitis (EoE) is identified in up to 50% of patients who present with a food bolus obstruction (FBO). Accepted guidelines recommend oesophageal biopsy be performed at index endoscopy for prompt diagnosis and management of EoE, however, this occurs in only 40% of food bolus presentations. To understand factors that impact clinicians practice, we collected data from all food bolus obstructions that presented over a 3-year period with the aim to understand potential barriers to obtaining oesophageal biopsies for the diagnosis of EoE during an acute presentation.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort study of adult patients presenting with acute food bolus obstruction to a tertiary hospital from January 2020 to December 2022. Patient records were identified using endoscopy reporting software (ProvationMD) and International Classification of Disease (ICD) coding for ‘foreign body in oesophagus.’ Patients with intentional ingestion of foreign body objects were excluded. Patient demographics, medical comorbidities, drug therapy with anticoagulation and/or antiplatelet therapy and prior history of FBO was collected. Clinician reported macroscopic endoscopy findings, location and number of oesophageal biopsies, timing of procedure and histological findings were included. A diagnosis of EoE was confirmed where eosinophil-predominant inflammation was found (≥15 eos/hpf) on biopsy. Statistical analysis was performed using SPSS V.29 software and p-values <0.05 were considered significant. Pearson’s <i>χ</i><sup>2</sup> was used to assess for a significant relationship between timing and frequency of biopsy.</p><p><b><i>Results:</i></b> A total of 251 patients with food bolus obstruction were identified over the 3-year study period, with 239 undergoing endoscopy 95.2%. Of these, EoE was histologically confirmed in 54 cases (22.5%), with those most likely to present between 45 and 59 years of age (27.4%) and predominately male 71.4%. A prior food bolus obstruction was recorded in 50.2% of patients and 15% of patients had a history of atopy. 4.4% of patients were receiving treatment for EoE. A total of 119 patients (49.7%) had oesophageal biopsies at index endoscopy. Endoscopy was performed mostly in business hours (8am and 5pm), with 161 patients (67.3%) and of those, 84 patients had biopsies (52.1%). There was no significant relationship between timing of procedure and having a biopsy (p=0.703). There was a significant relationship with those on antiplatelet therapy and having a biopsy with 5 out of 38 patients biopsied (p < 0.001), but not with those on anticoagulation therapy, 9.2% biopsied Vs 60.8% not biopsied (p=0.272). Patients with a history of atopy were more likely to have a biopsy (p=0.019) than those with a cardiac history (67.5% Vs 32.3%). There was no significant relationship between having macroscopic findings consistent with EoE and having a biopsy, 51 patients with reported findings and 22 biopsied (43.1%, p=0.299). Of those who presented with a further food bolus obstruction within 3-years (44 total), a diagnosis of EoE was the most common underlying diagnosis, 13 patients (29.5%).</p><p><b><i>Conclusion:</i></b> Guidelines for the diagnosis and management of eosinophilic oesophagitis (EoE) recommend endoscopy and biopsy for histological diagnosis of EoE during acute food bolus obstruction. This study underscores the significant prevalence of EoE among patients presenting with food bolus obstruction, particularly among middle-aged males. It highlights the importance of considering patient history, such as prior obstructions and atopy, in managing and diagnosing EoE. The findings also suggest that while biopsy practices during endoscopy are influenced by factors like medication (specifically antiplatelet therapy) and patient history, the timing of the procedure does not appear to significantly affect biopsy rates. The recurrence of food bolus obstruction in patients with EoE emphasizes the need for ongoing management and potential treatment adjustments for these individuals.</p><p><b>370</b></p><p><b>Correlation between hypermetabolic PET/CT activity and clinically significant lesions found at endoscopic evaluation</b></p><p><b>Melissa Carroll</b>, Patrick Felton and Steven Bollipo</p><p><i>NSW Health, John Hunter Hospital, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> Hypermetabolic activity in the gastrointestinal tract prompting endoscopic evaluation is frequently encountered on PET/CT imaging performed for various clinical scenarios. Our aim was to collect data from endoscopic procedures performed for the indication “Abnormal PET scan of the GI Tract,” and analyze data to evaluate PET/CT avidity and the corresponding endoscopic and histological findings.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort analysis of all adult patients who underwent endoscopy at a tertiary hospital over a 3-year period from January 2019 to December 2023, for reported hypermetabolic activity in the gastrointestinal tract on positron emission tomography/computed tomography (PET/CT) imaging. Patients were identified through endoscopy reporting software (ProvationMD), with the indication “Abnormal PET scan of the GI tract.” Patient demographics and indication for imaging was collected. We specifically looked at the location of avidity on PET/CT and whether there was correlation with endoscopic findings. We collected data on lesion location and size, histological findings, and additional or incidental findings which were not reported from PET/CT imaging. Clinically significant lesions were considered as high-grade dysplasia, invasive carcinoma and malignant (adenocarcinoma, lymphoma, melanoma). Statistical analysis was performed using SPSS V.29 software and p-values <0.05 were considered significant. Pearson’s <i>χ</i><sup>2</sup> was used to assess for significant relationship between size, location and clinical significance of found lesions.</p><p><b><i>Results:</i></b> Of 331 patients who underwent endoscopy, a total of 62 patients (18.8%) were found to have a clinically significant lesion identified. There were 204 cases with a lesion identified at endoscopy correlating with hypermetabolic activity on PET/CT (61.6%), and of these 41 cases were clinically significant lesions 12.4%. An unknown primary malignancy was the most common indication for PET/CT (21.7%). There were 127 patients (38%) with a polypoid lesion found at endoscopy, with 68 lesions >20mm in size and of those, 47% were clinically significant (p = <0.05). Adenocarcinoma was the most common significant lesion (14%) on histology. PET/CT failed to detect 15 cases of clinically significant lesions (4.5%). There was a slight male predominance 55.9% Vs 44.1%, with endoscopy being performed more often in those who were aged 55 years or older (89%). Overall, 54 patients (16%) who underwent endoscopy had no macroscopic lesion identified during their endoscopic procedure.</p><p><b><i>Conclusion:</i></b> We conducted a retrospective analysis of data from adult patients who underwent gastroscopy and/or colonoscopy based on positron emission tomography/computed tomography (PET/CT) imaging with gastrointestinal findings. The study provides valuable insights into the prevalence, significance, and characteristics of PET/CT avid lesions detected in the gastrointestinal tract, as well as their correlation with endoscopic findings. These findings contribute to our understanding of the diagnostic approach to patients with incidental PET/CT findings, informing clinical decision-making in this context.</p><p><b>389</b></p><p><b>An unusual presentation of appendicitis detected on colonoscopy in a young female with coeliac disease</b></p><p>Eleanor Wheatley and <b>Mohammad Shir Ali</b></p><p><i>John Hunter Hospital, Newcastle, Australia</i></p><p><b><i>Introduction:</i></b> Appendicitis is classically a clinical diagnosis, with urgent surgical management. It is often an emergency presentation with symptoms including acute pain migrating from the peri-umbilical region to the right iliac fossa (RIF), nausea, anorexia, and fever. Physical examination findings include tenderness in the RIF with rebound pain and peritonism. Subacute appendicitis on the other hand can be a more evasive diagnosis. In addition, fibrous obliteration of the appendix which is a histological diagnosis, can mimic acute appendicitis. Here we present an unusual presentation of appendicitis (with fibrous obliteration) which went undetected on the initial clinical assessment and cross-sectional imaging but was eventually detected on colonoscopy.</p><p><b><i>Case report:</i></b> We report a 19-year-old female presenting with subacute/chronic RIF pain on a background of coeliac disease and type 1 diabetes. The patient had 3 prior emergency presentations with generalised abdominal pain spanning a 2-month period, each time having worsening RIF pain which had deteriorated over a series of days. The patient presented a final time to the emergency department with RIF pain and nausea. With no other classical symptoms of appendicitis other than generalised pain and guarding on admission, differentials included pelvic inflammatory disease (PID), urinary tract infection, ureteric calculus, inguinal hernia, and ovarian pathology. Diagnostic workup included abdominal ultrasound which excluded ureteric calculi and renal tract pathology, however displayed hyperaemia and mild mural thickening of the terminal ileum. Subsequent computed tomography (CT) scan showed similar findings suggestive of terminal ileitis. Notably, there were no features of appendicitis on this initial CT scan. Colonoscopy subsequently confirmed appendicitis by visualisation of pus emanating from the appendiceal orifice and congested mucosa at the site. The terminal ileum appeared completely normal on colonoscopy. A repeat preoperative CT showed an enlarged and inflamed retrocaecal appendix. The patient then underwent a laparoscopic appendicectomy without any sequelae. The histology of the surgical specimen revealed focal mucosal ulceration consistent with appendicitis. In addition there was prominent fibrous obliteration of the tip of the appendix a condition that can also mimic acute appendicitis.</p><p><b>398</b></p><p><b>Unexpected diagnosis: collagenous ileitis in a patient without diarrhea</b></p><p><b>Fei Yang Pan</b><sup>1</sup> and Ahmad Alrubaie<sup>1,2</sup></p><p><sup>1</sup><i>Macquarie University Hospital, Sydney, Australia;</i> <sup>2</sup><i>Bankstown-Lidcombe Hospital, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Collagenous ileitis (CI) is extremely rare, with only four reported cases. Two additional cases were medication-induced by mycophenolate and duloxetine. CI, part of collagenous enteritis, features thickening of the mucosal subepithelial collagen band, chronic inflammation, increased epithelial lymphocytes, and epithelial detachment. The cause of subepithelial collagen deposition in the GIT is unknown, but research suggests an inflammatory process with profibrogenic mediators. Symptoms include diarrhea, altered bowel habits, epigastric pain, and bloating. CI is isolated to the ileum, unlike collagenous sprue (CS), which affects the proximal small intestine. Diagnosis requires histopathology confirming a thickened subepithelial collagen band, typically over 10 μm, similar to the criteria for collagenous colitis (CC).</p><p><b><i>Case Report:</i></b> A 77-year-old female presented with recurrent melena and iron deficiency anaemia. A video capsule endoscopy revealed gastric antral vascular ectasia (GAVE) and mild to moderate circumferential congestion and erythema in the small bowel. Her medical history includes diverticulitis, hypertension, asthma, hypercholesterolemia, anxiety, reflux, and endometrial cancer, for which she underwent a hysterectomy and salpingo-oophorectomy. She is currently on rosuvastatin, rabeprazole, and sertraline. On 29/02/24, she underwent an antegrade double-balloon endoscopy, which provided views up to the proximal ileum which demonstrated a 60 to 70 cm segment of abnormal mucosa with erythematous changes and nodularity in the distal jejunum and proximal ileum. Biopsies of the distal jejunum showed normal mucosa except for mild oedema of the lamina propria, without increased inflammation or evidence of microscopic colitis. Biopsies of the proximal ileum revealed mildly oedematous ileal mucosa with some broadening of the villi and a patchy increase in the subepithelial collagen plate between 10 and 20 μm, confirmed by Masson trichrome staining. Interestingly, terminal ileum biopsies performed on 16/01/24 showed normal ileal mucosa. She was subsequently started on a daily dose of 9 mg of budesonide with good effect. A repeat colonoscopy is planned soon to assess both the colon and ileum for collagenous disorders.</p><p><b>410</b></p><p><b>Summary of pharmaceutical industry clinical trials of biologics for eosinophilic oesophagitis in Australia and internationally: Substantial contributions possible in Australia, but room for improvement</b></p><p>Rity Wong<sup>1</sup>, <b>Hamish Philpott</b><sup>1,2</sup> and Thomas Lokan<sup>1</sup></p><p><sup>1</sup><i>Northern Adelaide Local Health Network, Adelaide, Australia;</i> <sup>2</sup><i>University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> There is a need for additional medications to treat eosinophilic oesophagitis (EoE) due to a lack of efficacy or tolerability of current agents. Pharmaceutical companies are developing biologics often borrowed from related disease states (particularly inflammatory bowel disease, and atopic conditions such as asthma or dermatitis). Given our relatively small population overall, yet a high prevalence of EoE, we consider the Australian contribution to key international pharmaceutical industry studies of biologics in adult patients with EoE.</p><p><b><i>Methods:</i></b> We interrogated our own database, as well as the Annual Progress Report for each agent, and cross validated Australian and international data using the online trial registry https://clinicaltrials.gov. Individual trial name, biological class and mechanism of action, recruitment time time window, screening number and failure rate as well as Australian and total recruitment number was calculated.</p><p><b><i>Results:</i></b> Over the last 5 years (2019-2024), five (5) biologics have been trialled in Australia as part of international efforts (Table 1). The number of patients enrolled in these studies varied between 108 to 430, with the Australian contribution being between 10-26 patients per study (2-6%). There were between 4 and 12 sites in Australia for each study. Screen failure rates ranged from 0-57% at our site (Northern Adelaide Local Health Network - NALHN) and NALHN contributed between 25% and 66% of patients successfully enrolled in each of the 5 studies in Australia and overall, 43% of all Australian patients enrolled were from NALHN.</p><p>\n \n </p><p><b><i>Conclusion:</i></b> Australia can make a meaningful contribution to international pharmaceutical industry studies in EoE. To date, a small number of sites have enrolled a significant proportion of patients, suggesting that more focussed efforts in future can improve recruitment in Australia in future.</p><p><b>419</b></p><p><b>An early review of MetaPanel™ - a diagnostic metagenomic gastrointestinal pathogen assay</b></p><p><b>Michael Wehrhahn</b><sup>1</sup>, David Wood<sup>2</sup>, Nicola Angel<sup>2</sup>, Donovan Parks<sup>2</sup>, Rhys Newell<sup>2</sup>, Andrew Ginn<sup>1</sup>, Lutz Krause<sup>2</sup>, Paul Griffin<sup>2</sup> and Jim Newcombe<sup>1</sup></p><p><sup>1</sup><i>Douglass Hanly Moir Pathology, Sydney, Australia;</i> <sup>2</sup><i>Microba, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal infection is routinely diagnosed by culture, PCR or a combination of both. However, the diagnosis is limited to pathogens that are targets in the multiplex PCR assay or detected on routine culture media. In March 2024, a comprehensive faecal metagenomics assay (MetaPanel™) was introduced through Sonic Healthcare Australia Pathology laboratories. This assay reports 115 DNA pathogens including bacteria and selected bacterial virulence factors, protozoa, helminths, viruses, fungi and microsporidia, in addition to 60 antimicrobial resistance (AMR) genes and a research use only dysbiosis measure incorporating diversity and richness scores.</p><p><b><i>Methods:</i></b> A review of the first 79 MetaPanel samples was undertaken, focusing on type of referrer, patient demographics, detected pathogens, detected AMR genes, and proportion with low diversity and richness (defined as falling in the lowest decile of a healthy cohort).</p><p><b><i>Results:</i></b> The average age of the referred patient was 47 years (11% under 18 years) and 59% were female. The most common referrers were community practitioners (53%, with about 1/5 of these having an interest in integrative medicine), followed by gastroenterologists (30%), and other specialists (16%) comprising haematologists, oncologists, rheumatologists, infectious diseases physicians and immunologists. A putative pathogen was identified in 19% of samples, including: enteropathogenic <i>E. coli</i> (EPEC) (3), <i>Campylobacter concisus</i> (3), <i>Tropheryma whipplei</i> (2), toxigenic <i>Clostridium perfringens</i> (2), toxigenic <i>Staphylococcus aureus</i> (1), <i>Yersinia frederiksenii</i> (1), toxigenic <i>Clostridium difficile</i> (1), <i>Campylobacter jejuni</i> (1), <i>Aeromonas hydrophila</i> (1) and <i>Aeromonas caviae</i> (1) with the former 6 pathogens not routinely identifiable by PCR or culture. AMR genes were detected in 29% of samples with 61% of these including AMR genes not co-detected with common host organisms, indicating a higher risk of patient-to-patient transmission (CTX-M Extended Spectrum Betalactamas (ESBL) (5), qnrB quinolone resistance (2), rmtD aminoglycoside resistance (2) and vanA/B vancomycin resistance (3)). In 82% of samples, the gut microbiome was classified as being of low diversity and/or richness.</p><p><b><i>Conclusion:</i></b> Early results support the utility of a faecal metagenomics assay (MetaPanel) in diagnosing difficult-to-detect gastrointestinal pathogens and identifying carriage of clinically relevant antimicrobial resistance genes. Further studies are underway to investigate the impact of MetaPanel on patient management and clinical outcomes.</p><p><b>430</b></p><p><b>The first randomised controlled trial of Jorveza (budesonide) compared to PPI (pantoprazole) for eosinophilic oesophagitis: Progress report of a multi-site Australian study</b></p><p><b>Hamish Philpott</b><sup>1,2</sup>, Thomas Lokan<sup>1</sup> and Edward Young<sup>1</sup></p><p><sup>1</sup><i>Northern Adelaide Local Health Network, Adelaide, Australia;</i> <sup>2</sup><i>University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background:</i></b> Eosinophilic oesophagitis (EoE) is a chronic inflammatory condition that progresses to fibro-stenosis and recurrent food bolus impaction. Expert opinion proposes that Jorveza (budesonide) is more effective than PPI in resolving inflammation and reversing fibro-stenosis. The two agents have not been subject to a randomised controlled trial (RCT).</p><p><b><i>Methods:</i></b> Ethics review board clearance of a 12 site (multicentre) study across Australia, for adult patients with EoE aged 18 years and over, with established diagnosis of EoE (>15 eosinophils per HPF) and no previous use of Jorveza. Treatment naïve patients are randomised to Jorveza 1mg Po BD or Pantoprazole 40mg Po BD, with repeat endoscopy in 8-10 weeks, biopsies of the lower and middle oesophagus, endoscopic reference score (EREFs) and symptom scores (EoEsA1 PRO and EoE – QOL-A) being completed. At clinic review patients responding (<5/HPF) continue treatment for another 8-10 weeks, with endoscopy, EREF’s and symptom scores repeated at weeks 16-20. Patients failing initial treatment cross- over to the alternative medication (PPI or Jorveza) for a period of 8-10 weeks prior to repeat endoscopy, EREF’s and symptom scores, again at week 16-20 from enrolment. Consenting patients at specific trial sites will undergo EUS and EndoFlip at week 8-10 and week 16-20. Target sample size 72 (36 each for Jorveza and PPI, anticipated treatment effect difference 25%, power 0.80), recruitment from December 2023 to December 2025.</p><p><b><i>Results:</i></b> Enrolment commenced December 2023 and currently 5 of 12 sites are active (NALHN – Lyell McEwin and Modbury hospitals, Royal Adelaide Hospital, Flinders Medical Centre, Monash Medical Centre and Northern Hospital Epping). 19 patients have been enrolled (June 5<sup>th</sup>, 2024, all from NALHN) trial completed in 4 individuals. Patients mean age of 36 years (range 21-58) 12/19 (63%) being male. 15/19 patients (79%) presented with food bolus impaction, and all were on nil current treatment.</p><p><b><i>Conclusion:</i></b> The first randomised controlled trial of Jorveza vs PPI is underway, feasible and recruitment to schedule. More data to follow, additional sites to activate will speed recruitment and results.</p><p><b>448</b></p><p><b>Vertigo and pancreatic malabsorption</b></p><p><b>John Evans</b></p><p><i>Queen Elizabeth II Jubilee Hospital, Brisbane, Australia;</i> <i>St Andrew's War Memorial Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Vertigo is a functional disturbance in which there is an illusory sense of movement either of self or of the environment, the result of asymmetry in impulses impacting on the right or left vestibular system due to dysfunction of the semi-circular canals, vestibular nerve, or brain stem and is divided into peripheral and central causes. Peripheral causes are considered due to particles in the semi-circular canals. Vertigo was the most common presenting symptom from studies in Primary Care, Emergency Rooms, and Dizziness Clinics. Management of Vertigo is supportive. Particle positioning manoeuvres (Epley or Sermont) can be used although recurrences are frequent; and medication can be tried for the acute clinical situation (antihistamines, and/or benzodiazepines, and/or anti-emetics) or for recurrent episodes (betahistine and/or prochlorperazine) although there seems to be no evidence of these drugs’ long-term efficacy.</p><p><b><i>Case Reports:</i></b> Both husband & wife from a rural setting incidentally mentioned improvement in vertigo following management of pancreatic exocrine insufficiency (PEI). A further five female patients with PEI experienced vertigo. These patients also underwent tests of hearing, and Videonystagmography (Caloric testing) and were later reassessed. The manoeuvres or medications mentioned above were not utilised. All patients revealed prolonged symptomatic and objective improvement of Vertigo with management of malabsorption associated with PEI.</p><p>VERTIGO, VIDEONYSTAGMOGRAPHY, & PEI\n\n </p><p>+ rural couple</p><p><b><i>Conclusion:</i></b> Vertigo may be a hitherto unrecognised, uncommon association of malabsorption due to PEI but appropriate management of PEI revealed long term, effective management of Vertigo. These improvements occurred despite the considered presence of particles in the semi-circular canals. Consideration of malabsorption in patients with Vertigo may enhance management of Vertigo.</p><p><b>472</b></p><p><b>Transmural changes of microscopic colitis using intestinal ultrasound: a case report</b></p><p><b>Peter Litwin</b><sup>1</sup>, Bhuwan Tandon<sup>1,2</sup>, Aude Van Oosterwyck<sup>1,2</sup>, Robert Bryant<sup>1,2,3</sup> and Ryan M Mathias<sup>1,2,3</sup></p><p><sup>1</sup><i>Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>2</sup><i>Inflammatory Bowel Disease Service, Queen Elizabeth Hospital, Adelaide, Australia;</i> <sup>3</sup><i>The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> The use of Gastrointestinal Ultrasound (GIUS) is well established in the evaluation of patients with inflammatory bowel disease, which is not the case in microscopic (or collagenous) colitis. Whilst a 2022 study of 498 patients by Koop et al. demonstrated abnormal CT imaging in this disease, only a single case report of GIUS abnormalities can be found in the literature. However, there are no reports demonstrating its use case as a non-invasive treatment modality in assessing treatment response.</p><p><b><i>Case Report:</i></b> A 61-year-old female presented with a 12-week history of progressive diarrhoea and urgency (up to 14 times per day), initially watery but having become blood and mucous stained in the preceding 3 weeks. Her past medical history included high cholesterol, hypertension and anxiety, for which she was prescribed longstanding atorvastatin, amlodipine and venlafaxine. She was a non-smoker, had no recent antibiotic exposure, no over the counter medications and no family history of autoimmune disease. Biochemical abnormalities included hypokalaemia (2.6 mmol/L), an acute kidney injury (creatinine 110 umol/L) and an elevated C-reactive protein (40 mg/L). Stool samples were negative for infection and her faecal calprotectin was elevated at 189 ug/g (<50). Unprepared colonoscopy demonstrated a severe confluent pancolitis from the rectum to caecum with a normal terminal ileum. Gastrointestinal ultrasound (GIUS) demonstrated pancolitis with increased bowel wall thickening (maximum 5.6mm), modified Limberg 2 doppler activity and preserved wall stratification. Histology confirmed collagenous colitis with preserved crypt architecture, thickening of the subepithelial basement membrane and plasmacytosis. The patient was commenced on intravenous hydrocortisone 100mg QID with excellent clinical (bowel frequency reduced to 2) and biochemical response over a 48-hour period and was transitioned to prednisolone and later budesonide. Repeat GIUS 6 days post therapy demonstrated complete transmural healing with normalisation of bowel wall thickness and no increased colour doppler signal.</p><p><b>486</b></p><p><b>Not all right-sided colonic ulcers are Crohn’s disease: <i>Entamoeba histolytica</i> and <i>Mycobacterium tuberculosis</i> infections diagnosed at colonoscopy</b></p><p><b>Vanessa Chong</b><sup>1</sup>, <b>Jin Lin Tan</b><sup>1,2</sup>, Biju George<sup>1</sup>, Mohamed Asif Chinnaratha<sup>1,2</sup> and Damian Harding<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> Ulceration in the right colon is commonly caused by Crohn’s disease, but other causes including infection, malignancy and ischaemia should be considered. Distinguishing the aetiologies by symptoms alone can be difficult due to similar clinical presentations. Infectious causes are particularly relevant for those who have travelled or migrated from endemic areas. This case series outlines three cases of right-sided colonic ulceration caused by <i>Entamoeba histolytica</i> and <i>Mycobacterium tuberculosis</i>.</p><p><b><i>Case reports:</i> Case 1)</b> A 67-year-old female from Afghanistan experienced intermittent right iliac fossa pain and iron deficiency anaemia. Colonoscopy revealed discrete deep caecal ulceration. Biopsies sent for TB and amoebiasis PCR were positive for <i>E. histolytica,</i> with amoebic organisms seen on histology. Treatment with Tinidazole followed by paromomycin resulted in symptom resolution and endoscopic healing of colonic ulcers. <b>Case 2)</b> A 61-year-old female from Myanmar had several years of right-sided abdominal pain, diarrhea and weight loss. CT showed mural thickening in the caecum and ascending colon. Colonoscopy revealed a hemi-circumferential and ulcerated polypoid mass in the caecum. Biopsies were sent for TB PCR, culture (both positive for <i>M. tuberculosis</i>) and histology, which showed necrotising granulomatous inflammation. After 9 months of anti-tuberculous therapy her symptoms resolved. Follow-up colonoscopy showed resolution of the caecal mass. <b>Case 3)</b> A 31-year-old female from Nepal with previously diagnosed Crohn’s disease underwent a colonoscopy to evaluate worsening abdominal pain and altered bowel habits. CT showed extensive inflammation in the caecum and ascending colon accompanied with enlarged necrotic mesenteric nodes. Initial treatment with steroids and biologics was ineffective. Colonoscopy revealed deep ulcers luminal narrowing at the hepatic flexure. Biopsies were positive for <i>M. tuberculosis</i>. She was commenced on anti-tuberculous therapy with resolution of symptoms and currently scheduled for follow-up colonoscopy after 9 months of treatment.</p><p><b><i>Discussion:</i></b> Amoebiasis is transmitted through ingestion of amoebic cysts, which develop into trophozoites in the intestines that in some will cause invasive disease. Colonoscopy typically shows discrete, deep ulcers in the proximal colon, sparing the terminal ileum and distal colon. Histology may show “flask-shaped” ulcers with amoebic trophozoites. Intestinal tuberculosis (ITB) constitutes 2% of TB cases worldwide, often from latent TB reactivation or ingestion of tuberculous mycobacteria. Colonoscopy often reveals ileocaecal disease, and histology, caseating sub-mural granulomas, unlike the transmural granulomas associated with Crohn’s disease. Tissue biopsies for PCR and culture are essential for diagnosing amoebiasis and ITB and should be considered at the time of colonoscopy.</p><p><b>488</b></p><p><b>Aortoesophageal fistula with life-threatening upper gastrointestinal bleeding: a case report</b></p><p><b>Xiaomin Ma</b><sup>1,5</sup>, <b>Mohamed Reffai Syed Mohamed</b><sup>1</sup>, Bulent Baran<sup>1,4</sup>, Christine Welch<sup>1,4</sup>, Kevin Tian<sup>3,4</sup>, Donald Cameron<sup>2,4</sup>, Yew Toh Wong<sup>3,4</sup> and Rozemary Karamatic<sup>1,4</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Townsville University Hospital, Townsville, Australia;</i> <sup>2</sup><i>Department of General Surgery, Townsville University Hospital, Townsville, Australia;</i> <sup>3</sup><i>Department of Vascular Surgery, Townsville University Hospital, Townsville, Australia;</i> <sup>4</sup><i>School of Medicine, James Cook University, Townsville, Australia;</i> <sup>5</sup><i>School of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Aortoesophageal fistula (AEF) arises from an abnormal connection between the aorta and the oesophagus. It is defined by Chiari’s triad of mid-thoracic pain, sentinel arterial haemorrhage and exsanguination after a symptom-free interval. Only 20-45% of patients fulfil this criterion, and a high index of suspicion is required. AEF may result in fatal upper gastrointestinal bleeding (UGIB) if not promptly addressed, with a mortality rate of 47-77%. We present the case of a 71-year-old man with AEF-related unstable UGIB managed successfully with endoscopic and endovascular intervention.</p><p><b><i>Case Report:</i></b> A 71-year-old man presented to an Australian regional hospital with chest pain and haematemesis on a background of a gastro-oesophageal junction adenocarcinoma with nodal metastases treated with palliative chemoimmunotherapy and radiotherapy. He had previous oesophageal dilatations and stents for dysphagia complicated by tissue ingrowth and stent migration. Six weeks prior to presentation, a fully covered stent was placed across a tight stricture, with clips used to secure the proximal end and an 18mm balloon inflated inside the stent. On presentation, he was haemodynamically unstable requiring aggressive resuscitation. Computed Tomography Angiography (CTA) demonstrated distal migration of the stent with no bleeding source identified. He was transferred to the tertiary referral hospital after detailed CTA review due to high suspicion for AEF in view of prior radiotherapy and endotherapy. A multidisciplinary discussion involving gastroenterology, general surgery, vascular surgery, anaesthetics and intensive care unit (ICU) occurred prior to endoscopy to ensure appropriate personnel were available. At endoscopy, large amounts of blood clot were found throughout the oesophagus. The stent was found in the distal oesophagus, with ulceration at the proximal edge of the stent at the site of a clip. Following stent removal, an excavated ulcer covered with granulation tissue started exsanguinating, requiring activation of massive transfusion protocol. A partially covered metal stent was deployed to tamponade the bleeding and vascular surgery immediately proceeded to endovascular aortic stent graft insertion. He was transferred to ICU in a stable condition. The oesophageal stent was endoscopically removed the following day to avoid necrosis of tissue trapped between the oesophageal and aortic stents. The patient did not rebleed after stent removal.</p><p><b>496</b></p><p><b>High prevalence of ARFID and orthorexia nervosa in gastroenterology patients: an evaluation of disordered eating in a large gastroenterology clinics cohort</b></p><p><b>Amy Luo</b><sup>1</sup>, Hannah Kim<sup>1</sup>, Jessica Green<sup>1</sup>, Annalise Stanley<sup>1</sup>, Jamee Barugh<sup>1</sup>, Jessica Peters<sup>1</sup>, Linda Yang<sup>1,2</sup>, Angela Khera<sup>1,2</sup>, Michael Salzberg<sup>1,2</sup>, Michael Kamm<sup>1,2</sup> and Chamara Basnayake<sup>1,2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Disordered eating (DE) in gastrointestinal (GI) clinics is highly prevalent but not well-characterised. Specific eating disorders like avoidant/restrictive food intake disorder (ARFID) and orthorexia nervosa have not been adequately studied in this population. This study aimed to evaluate the prevalence and characteristics of DE in GI patients, with a focus on ARFID and orthorexia, using screening tools, across organic GI disorders, disorders of gut-brain interaction (DGBI), and controls.</p><p><b><i>Methods:</i></b> Consecutive patients at a single tertiary centre, from September 2022 to October 2023, were invited to complete an online questionnaire post clinic appointment. Patients with a GI disorder were invited if they had “organic” disease (inflammatory bowel disease (IBD) and/or coeliac disease), or DGBI, as per Rome IV criteria. Controls were defined as asymptomatic patients presenting for surveillance of polyps, positive faecal occult blood testing or those with H. pylori infection. The 63-item questionnaire included screening tools for ARFID (NIAS, EDY-Q), orthorexia nervosa (ORTO-7), GI-symptom specific anxiety (VSI), quality of life (EQ-5D-5L VAS), depression and anxiety (PHQ-4). DE is defined according to self-reported eating disorder (ED), recorded ED diagnosis on file, or established ED screening tool cut-off scores (NIAS: item 1-3 ≥ 10, and/or item 4-6 ≥ 9, and/or item 7-9 ≥10; EDY-Q: at least one of item 2, 10, 12 ≥ 4, and item 4 ≥ 4; ORTO-7 ≤ 19).</p><p><i><b>Results:</b> Demographics:</i> 292 patients completed the questionnaire from 1007 invitations (41.4% male, median age 46). 239 cases had a GI disorder (81.8%) and 53 were controls (18.2%). 64.4% had organic GI disorder (58.9% IBD, 4.5% coeliac disease, 1.0% both) and 17.5% had DGBI. 193 participants (66.1%) had DE; 23.3% with features of ARFID, 12.3% with features of orthorexia, 27.1% with features of ARFID and orthorexia, and 3.8% other. Patients with DGBI had the greatest likelihood of DE (82.4%), followed by organic GI disorder (65.4%) and controls (52.8%) (<i>p</i> = 0.006).</p><p><i>Patients with GI disorders:</i> There was higher DE severity (NIAS <i>p</i> = 0.010; EDY-Q <i>p</i> = 0.030; ORTO-7 <i>p</i> = 0.011), GI-specific anxiety (<i>p</i> < 0.001), lower QoL (<i>p</i> = 0.018), and more food restrictions (<i>p</i> = 0.006) in GI disorders compared to controls, while DGBI patients exhibited even greater DE severity, GI-specific anxiety, depression, anxiety, and lower QoL than both organic disorders and controls (all <i>p</i> < 0.001 for DGBI vs. controls). There was greater GI specific anxiety (<i>p</i> < 0.001) and more food restrictions (<i>p</i> = 0.042) in organic disorders compared to controls.</p><p><i>Patients with disordered eating (DE):</i> There was significantly higher GI specific anxiety, depression and anxiety, GI symptom severity, lower QoL and more food restrictions in those with DE compared to those without DE (all <i>p</i> < 0.001), and particularly in patients with both ARFID and orthorexia compared to those without DE (all <i>p</i> < 0.001). Participants displaying ARFID features had significantly greater GI specific anxiety (<i>p</i> < 0.001), GI symptom severity (<i>p</i> = 0.032) and lower QoL (<i>p</i> < 0.001) compared to those without DE. GI symptom severity was just significantly higher in ARFID than orthorexia (<i>p</i> = 0.049). Participants with DE had significantly higher GI symptom frequency (<i>p</i> = 0.035) and lower BMI (<i>p</i> = 0.046) than those without DE. There was no significant association between DE and GI disease activity or whether patients attended dieticians within the clinics.</p><p><b><i>Conclusion:</i></b> This study reveals a high prevalence and severity of disordered eating, among GI patients who completed an online questionnaire, particularly those with DGBI. DE severity, anxiety, QoL, and food restrictions were also significantly worse in patients with organic disorders and DGBI. These findings suggest that routine screening for DE should be integrated into GI clinics to better identify and manage these disorders. Further studies are required to explore if treatment of comorbid DE improves psychological and GI symptom outcomes for patients.</p><p><b>497</b></p><p><b>Haemosuccus pancreaticus: a rare cause of gastrointestinal bleeding</b></p><p><b>Niamh Buckley</b><sup>1</sup>, Santhi Swaroop Vege<sup>2</sup> and Christopher Blevins<sup>2</sup></p><p><sup>1</sup><i>Royal North Shore Hospital, Sydney, Australia;</i> <sup>2</sup><i>Mayo Clinic Rochester, Rochester, USA</i></p><p><b><i>Introduction:</i></b> Overt obscure gastrointestinal bleeding is a diagnostic challenge frequently faced by clinicians for which the possible etiologies are broad. We describe a rare case of Haemosuccus Pancreaticus occurring in the setting of chronic pancreatitis which should be considered as a differential in the correct clinical context.</p><p><b><i>Case Report:</i></b> We present the case of a 63-year-old man with a sixteen year history of recurrent obscure upper GI bleeding. The pattern of his episodes consisted of intense epigastric pain followed closely by melena which relieved the discomfort. This was often associated with a transient elevation of lipase. They occurred at approximately six month intervals and subsequently increased in frequency to every other month. He underwent extensive investigation which failed to uncover the source of the bleeding including multiple gastroscopies, duodenosocopies, colonoscopies, capsule endoscopies, a CT angiography and a tagged red blood cell study. CT abdomen and pelvis revealed a suspected saccular splenic artery pseudoaneurysm measuring 1.5 cm that abutted the pancreatic duct (Figure 1). There were changes observed that suggested chronic pancreatitis, the likely aetiology of the pseudoaneurysm. This clinical picture was suspicious for haemosuccus pancreaticus and was confirmed with EUS evaluation at the time of bleeding. During the same procedure, five microcoils (Nester 10 mm) were placed via EUS which completely cessated flow in one aspect of the pseudoaneurysm and significantly reduced it elsewhere (Figure 2). However, three days later the patient had melaena and features characteristic of his previous episodes. Repeat CT demonstrated enlargement of the aneurysm and embolization of the splenic artery was performed by interventional radiology. This has thus far been successful, with complete resolution of his symptoms.</p><p><b>References</b></p><p>\n 1. <span>Han, B</span>, <span>Song, ZF</span>, <span>Sun, B</span>. <span>Hemosuccus pancreaticus: a rare cause of gastrointestinal bleeding</span>. <i>Hepatobiliary Pancreat Dis Int.</i> <span>2012</span>; <span>11</span>(<span>5</span>): <span>479</span>-<span>488</span>.</p><p>\n 2. <span>Shah, AA</span>, <span>Charon, JP</span>. <span>Haemosuccus pancreaticus, an uncommon cause of upper gastro intestinal bleeding: Case report and review of the literature</span>. <i>J Pak Med Assoc.</i> <span>2015</span>; <span>65</span>(<span>6</span>): <span>669</span>-<span>671</span>.</p><p><b>502</b></p><p><b>Severe idiopathic secretory diarrhoea with a profound sustained response to somatostatin analogues</b></p><p><b>Geovanny Gandy</b><sup>1,2</sup>, Alex Prudence<sup>1,2</sup> and Miriam Tania Levy<sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology Department, Liverpool Hospital, Sydney, Australia;</i> <sup>2</sup><i>University of New South Wales, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Vasoactive intestinal peptide (VIP) secreting tumours are rare neuroendocrine neoplasms that present with chronic secretory diarrhoea and electrolyte derangements, with an incidence of 1 in 10 million people per year.<sup>1</sup> Raised VIP levels and radiological evidence of a lesion, most commonly pancreatic, confirm the diagnosis. However, this can prove challenging, as tumours only transiently secrete VIP and levels may not be elevated between diarrhoeal episodes.<sup>2</sup> We present a case of chronic secretory diarrhoea clinically compatible with a VIPoma, with rapid and sustained response to somatostatin analogue therapy despite negative investigations.</p><p><b><i>Case Report:</i></b> A 35-year-old Vietnamese female presented with progressively worsening non-bloody diarrhoea up to ten times daily, with hypotension and hypokalaemia requiring resuscitation in intensive care, on a background of two years of loose bowel motions. She reported no fevers, infective symptoms, sick contacts, recent antibiotic use, or recent overseas travel. Stool microscopy, extended PCR and cultures were negative; faecal calprotectin and faecal elastase were normal. Thyroid function was normal, tuberculosis gamma interferon assay and coeliac disease serology were negative. Faecal chemistry was consistent with secretory diarrhoea. Panendoscopy was unremarkable and biopsies excluded coeliac disease, microscopic colitis and inflammatory bowel disease. Neuroendocrine screening was negative, including serum VIP 16.9 pmol/L (normal <50 pmol/L). Ga-68 DOTATE PET, multiphase CT, and EUS revealed no lesions. On clinical suspicion of a VIPoma, octreotide was trialled with sustained response and patient was transitioned to lanreotide. Initial cessation of lanreotide precipitated a relapse, but it was weaned successfully after four years.</p><p><b>References</b></p><p>\n 1. <span>Yao, JC</span>, <span>Eisner, MP</span>, <span>Leary, C</span>, et al. <span>Population-based study of islet cell carcinoma</span>. <i>Ann Surg Oncol.</i> Dec <span>2007</span>; <span>14</span>(<span>12</span>): <span>3492</span>-<span>500</span>. https://doi.org/10.1245/s10434-007-9566-6</p><p>\n 2. <span>Ma, ZY</span>, <span>Gong, YF</span>, <span>Zhuang, HK</span>, et al. <span>Pancreatic neuroendocrine tumors: A review of serum biomarkers, staging, and management</span>. <i>World J Gastroenterol</i> May 21 <span>2020</span>; <span>26</span>(<span>19</span>): <span>2305</span>-<span>2322</span>. https://doi.org/10.3748/wjg.v26.i19.2305</p><p><b>511</b></p><p><b>Decoding gastrointestinal symptoms in systemic sclerosis: a cluster analysis of a large national prospective systemic sclerosis cohort</b></p><p>Alexander Strathmore<sup>1</sup>, Dylan Hansen<sup>1</sup>, Kathleen Morrisroe<sup>1,2</sup>, Alannah Quinlivan<sup>1,2</sup>, Susanna Proudman<sup>4</sup>, Jennifer Walker<sup>5</sup>, Joanne Sahhar<sup>3</sup>, Gene Siew-Ngian<sup>3</sup>, Lauren Host<sup>6</sup>, Wendy Stevens<sup>1</sup>, Mandana Nikpour<sup>1,2,7</sup>, Laura Ross<sup>1,2</sup> and <b>Chamara Basnayake</b><sup>1,2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia;</i> <sup>3</sup><i>Monash University, Melbourne, Australia;</i> <sup>4</sup><i>Royal Adelaide Hospital, Adelaide, Australia;</i> <sup>5</sup><i>Flinders Medical Centre, Adelaide, Australia;</i> <sup>6</sup><i>Fiona Stanley Hospital, Perth, Australia;</i> <sup>7</sup><i>Royal Prince Alfred Hospital, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal disease (GI) is present in over 90% of patients with systemic sclerosis (SSc). As the most common organ manifestation, it causes significant morbidity and has a negative impact on quality of life. There exists substantial heterogeneity in the presentation of GI manifestations of SSc. The aim of this study was to evaluate whether there is clustering of GI symptoms in SSc, and whether these clusters have prognostic implications.</p><p><b><i>Methods:</i></b> Adult patients (age ≥18 years) enrolled in the Australian Scleroderma Cohort Study (ASCS) with at least two study visits between 2007-2023 were eligible for inclusion. All patients had definite SSc, as defined by the 2013 ACR/EULAR classification criteria. Clinical data and patient-reported outcomes (PROMs) including HAQ-DI and UCLA GIT 2.0 Score, measuring physical function and GI severity, were collected annually. Seven variables were chosen and hierarchical cluster analysis with Jaccard similarity was performed using Ward’s linkage to identify subgroups. Univariate analysis with chi-square, ANOVA and Kruskal-Wallis rank tests, as appropriate, were performed to describe the differences between each subgroup. Kaplan-Meier survival analysis was performed to compare overall survival.</p><p><b><i>Results:</i></b> A total of 1,652 patients were included, 85.6% female with median follow-up of 4.47 (IQR 2.86-9.2) years. Clustering of patients based on GI symptoms identified four subgroups. We observed clustering based on frequency and severity of GI symptoms. This linked to disease duration. Longer disease duration was associated with more frequent and more severe GI involvement. More frequent GI symptoms were associated with poor physical function. There was no clustering of GI symptoms based on anatomical GI tract location. Cluster 1 (n=1116) was the largest cluster characterised by a high frequency of all GI symptoms, and was characterised by vomiting and faecal incontinence. Patients in Cluster 1 reported more severe GI disease (UCLA-SCTC GIT 2.0 score) and significantly impaired physical function (HAQ score) compared to Clusters 2-4. Cluster 3 and 4 were characterised by the absence of multiple GI manifestations. Survival analysis demonstrated better long-term survival in patients with severe GI manifestations (Cluster 1) compared to Clusters 2 and 3; perhaps accounted for by the lower prevalence of cardiopulmonary complications in Cluster 1.</p><p><b><i>Conclusion:</i></b> This large SSc cohort demonstrates that GI symptoms do not cluster into discrete upper and lower GI subgroups. Subgroups exist, with clear distinctions in frequency and severity of GI symptoms. Severe GI symptoms throughout the GI tract are a feature of longer disease duration and associated with significantly impaired physical function.</p><p><b>524</b></p><p><b>Surgery for non-malignant polyps continues to cause avoidable morbidity: Findings from a western cohort</b></p><p><b>Anthony Whitfield</b><sup>1,2</sup>, Julia Gauci<sup>3</sup>, Clarence Kerrison<sup>3,2</sup>, Sunil Gupta<sup>3,2</sup>, Oliver Cronin<sup>3,2</sup>, Timothy O'Sullivan<sup>3,2</sup>, Varan Perananthan<sup>3,2</sup>, Hunter Wang<sup>3,2</sup>, Francesco V Mandarino<sup>3</sup>, Brian Lam<sup>3</sup>, Eric Lee<sup>3,2</sup>, Nicholas Burgess<sup>3,2</sup> and Michael J Bourke<sup>3,2</sup></p><p><sup>1</sup><i>Blacktown Hospital, Sydney, Australia;</i> <sup>2</sup><i>Westmead Clinical School, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Westmead Hospital, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Most non-malignant colorectal polyps (NMCPs) can be removed endoscopically with minimal morbidity and negligible mortality. Despite this, a high rate of surgical resection still occurs in western populations resulting in avoidable cost to the patient and to the health budget. To establish better pathways for endoscopic resection of NMCPs in Australia, we sought to understand the prevalence and outcomes of surgery in a state-wide representative sample.</p><p><b><i>Methods:</i></b> A linked dataset provided by the Centre for Health Record Linkage (CHeReL), which included all admissions for surgery in patients aged 18 and over in New South Wales (NSW) between July 2007 and December 2017 was analysed. Australian classification of health interventions (ACHI) codes were used to filter the data set for colorectal surgery and International classification of diseases (ICD) codes were used to identify cases with a primary diagnosis of NMCP or colorectal cancer (CRC). Emergency surgery, inflammatory bowel disease and cases of total colectomy were excluded. Trends over two time periods (2008-2012 and 2013-2017) were compared. Major adverse events including mortality were captured 30 days from index surgery. Logistical regression was used to estimate risk ratios and 95% confidence intervals.</p><p><b><i>Results:</i></b> From July 2007 - December 2017, 36,257 surgeries for NMCP and CRC were performed in NSW. 4181 (11.4%) were performed for NMCP. Excluding the rectum, NMCPs accounted for 16.4% of surgery for neoplasia. 51.1% (2137/4181) were performed in private hospitals. Between 2008-2012 and 2013-2017 there was no major difference in volumes of surgery for NMCPs (2008-2012,1968 cases; 2013-2017, 1948 cases; p=0.774). No significant differences were observed (p=0.708) and this remained the case for all subgroups: teaching hospital vs non and major city vs regional. A major adverse event was encountered in 19.3% of surgery for NMCPs (808/4181). Predictors for major adverse event included age, male sex, rectal surgery, American society of anaesthesiologists physical classification system (ASA) III & IV and laparotomy. Full cover health insurance was a negative predictor (OR 0.72, p=0.05, 95% CI 0.52-0.99). Mean length of stay was 12.8 days when a major adverse event occurred compared to 6.9 days when one did not (p=<0.001).</p><p><b><i>Conclusion:</i></b> Surgery for NMCPs occurs at unacceptable rates in Australian Hospitals resulting in avoidable morbidity. Endoscopic resection pathways are required within public and private hospitals to address these avoidable poor outcomes for patients with NMCPs. Streamlining these patients to endoscopic resection will reduce inpatient workloads and associated health care costs.</p><p><b>529</b></p><p><b>Patients with functional gastrointestinal disorders spend less time in tertiary care when managed by a single clinician: Results of a multi-centre audit in South Australia</b></p><p><b>Ryan M Mathias</b><sup>1,2,3</sup>, Samantha Plush<sup>1,2</sup>, Elka Fairhead<sup>4</sup>, Benjamin Ngoi<sup>2,3</sup>, Louisa Edwards<sup>3</sup>, Alice Day<sup>1,2,3</sup> and Robert Bryant<sup>1,2,3</sup></p><p><sup>1</sup><i>Inflammatory Bowel Disease Service, The Queen Elizabeth Hospital, Adelaide, Australia;</i> <sup>2</sup><i>School of Medicine, The University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>4</sup><i>Department of Dietetics, The Queen Elizabeth Hospital, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Functional gastrointestinal disorders (FGID) are a group of disorders that manifest with abdominal symptoms. FGiDs have a serious impact on quality of life and represent a significant global burden on healthcare services. Guidelines now recommend an early, positive diagnosis in low-risk patients to reduce the risk of over-investigation. Establishing a strong clinician-patient relationship is a cornerstone of management. This requires both confidence in management and consistent messaging. The aim of this study was to identify factors that may contribute burden on two tertiary gastroenterology services.</p><p><b><i>Methods:</i></b> This multi-centre, retrospective chart review of electronic medical records evaluated adults attending general gastroenterology outpatient clinics at two teaching hospitals. Occasions of service (OOS) were characterised as being seen by either a single clinician or discontinuous care. Discontinuous care was defined as multiple clinicians of varying seniority reviewing the same patient from first encounter during their time in service. Time to diagnosis and discharge, OOS per patient and number of harmful investigations were assessed. A harmful investigation was defined as one that involved either an invasive procedure such as endoscopic assessment or ionising radiation. Statistical analysis was performed with ANOVA, Kaplan-Meier plots and multiple logistic regression analysis.</p><p><b><i>Results:</i></b> 275 patients (mean age 49 (SD 18), 72% female) were seen primarily for FGID between June 2021 - June 2022. When comparing single clinicians and discontinuous care, there was a protracted time to diagnosis between (42 vs 140 days, p<0.001) and time to discharge (158 versus 356 days, p<0.0001). Patients were more likely to receive a diagnosis early (HR 1.6, 95% CI 1.25; 2.04) and be discharged sooner (HR 1.83, 95% CI: 1.44,2.33) when seen by single clinicians compared with discontinuous care. Patients who received an early diagnosis by a single clinician spent less time in service following their diagnosis (80 days [IQR 0-183]) compared to those who experienced discontinuous care (378 days [IQR 217-616]); p<0.0001. There was a trend towards less harmful investigations in the single clinician group versus discontinuous care group (p=0.08).</p><p><b>530</b></p><p><b>Error and underestimation: capturing psychiatric complexity in disorders of gut-brain interaction</b></p><p><b>Paris Hoey</b><sup>1,3</sup>, <b>Lynne Heyes</b><sup>2</sup> and Trina Kellar<sup>1,3</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Department of Consultation-Liaison Psychiatry, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>3</sup><i>Faculty of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Disorders of gut-brain interaction (DGBI) are common, affecting 37.7% of Australians [1]. DGBI arise from past and present psychosocial stressors, via a complex interplay of nervous system, immune dysfunction, microbiome and mucosal-barrier dysfunction [2]. Whilst the prevalence of comorbid psychiatric disorders in DGBI is well established, medical literature oversimplifies the psychiatric profile of this population. Most studies use anxiety and depression self-reported screening measures for diagnosis [1]. Further, GI-psychologists and psychiatrists are few in medical services, leaving diagnosis to the primary physician. Post-traumatic stress disorder (PTSD), complex PTSD (C-PTSD), personality disorders (PD), eating disorders and persistent pain may be missed. We hypothesised that significant psychological factors contributing to complex DGBI were undiagnosed, thus untreated, in our cohort. This study aimed to compare the psychiatric profiles of patients with DGBI, pre- and post-psychologist formulation.</p><p><b><i>Methods:</i></b> Retrospective cohort study, in a metropolitan tertiary-level adult hospital, specialist multidisciplinary outpatient clinic. Inclusion criteria: consecutive patients who completed full neurogastroenterologist and gastro-psychologist assessment January 2023 to May 2024. Diagnoses were recorded using Rome IV, DSM-5 and ICD-11 diagnostic criteria.</p><p><b><i>Results:</i></b> 21 consecutive patients were included, 76% female, mean age 44. This represents a complex DGBI cohort, 57% had 3+ DGBI diagnoses, most commonly chronic nausea vomiting syndrome (52%), centrally mediated abdominal pain (43%), functional dyspepsia-postprandial distress syndrome (38%), and defecation disorders (33%). Prior to gastro-psychologist assessment, based on referral documentation and patient history, the primary psychiatric diagnosis was anxiety or major depressive disorder in 71% (n=15/21). PTSD in 1/21, C-PTSD 0/21, trauma without PTSD diagnosis 6/21. Active eating disorder 1/21, and PD 0/21. Notably, no psychiatric history was reported by 24%. Vastly more psychiatric complexity was uncovered following gastro-psychologist formulation (Figure 1). All met diagnostic criteria, with 52% suffering 3+ comorbid psychiatric disorders. Importantly, C-PTSD was present in 62%, PTSD 5%. 57% met criteria for active eating disorder (n=12/21), with 11/21 restrictive. PD present in 33%. Persistent pain disorder in 76%.</p><p><b>533</b></p><p><b>A double-blind, placebo-controlled, adaptive dose-response study to assess the acute effects of micro-doses of gluten in adults with treated coeliac disease (Gluten Threshold Study)</b></p><p><b>A James M Daveson</b><sup>1,2</sup>, Emma Craig<sup>1</sup>, Anuj Sehgal<sup>1</sup>, Jennifer Schaefer<sup>1</sup>, Michelle Colgrave<sup>3,4</sup>, Utpal Bose<sup>3,4</sup>, Melinda Hardy<sup>5</sup>, Jason Tye-Din<sup>5,6</sup> and Robert P Anderson<sup>7</sup></p><p><sup>1</sup><i>Wesley Research Institute, Brisbane, Australia;</i> <sup>3</sup><i>CSIRO Agriculture & Food, Brisbane, Australia;</i> <sup>2</sup><i>Coral Sea Clinical Research Institute, Mackay, Australia;</i> <sup>7</sup><i>Mackay Base Hospital, Mackay, Australia;</i> <sup>4</sup><i>ARC CIPPS Edith Cowan University, Perth, Australia;</i> <sup>5</sup><i>Immunology Division, The Walter & Eliza Hall Institute, Melbourne, Australia;</i> <sup>6</sup><i>Department of Gastroenterology, The Royal Melbourne Hospital, Melbourne, Australia</i></p><p><b><i>Background & Aim:</i></b> Evidence supporting a lower limit of gluten consumed in a gluten free diet (GFD) for Coeliac disease (CeD) is controversial. 20 mg per kg (20 parts per million) is accepted globally as the upper limit in gluten free foods except for Australia and New Zealand where “no detectable” gluten is enforced. We recently showed patients with CeD elevate serum interleukin-2 (IL-2) 2 – 6 hours after ingesting ~6 grams of vital wheat gluten (VWG). Reasoning serum IL-2 after a single gluten ingestion could be an objective, quantitative biomarker of gluten toxicity, our aim was to define an upper limit of gluten ingestion that did not elevate IL-2.</p><p><b><i>Methods:</i></b> We performed an adaptive, double-blind, placebo-controlled, dose-ranging safety study at a single site. 51 patients with CeD on a GFD were randomised in 4 sequential cohorts and dosed on three occasions each a month apart. Participants were observed for 6h post ingesting VWG or placebo in gelatin capsules. Cohort 1 received 1000mg gluten protein on 3 occasions as “positive control”. Three subsequent Cohorts were randomised to receive 3 of the 4 sequential dose levels: 610mg, 90mg, 13mg or placebo; 8mg, 5mg, 3mg or placebo; & 3mg, 2mg, 1mg of gluten or placebo. Primary endpoint was the % of IL-2 responders (defined as mean IL-2 at 2, 4 and 6 h more than two standard deviations above the upper limit of normal from the placebo group). Secondary outcomes included symptoms assessed by modified CeD PRO before and hourly post dosing. Faecal and urinary gluten immunogenic peptides (GIP) were exploratory endpoints to assess adherence to GFD.</p><p><b><i>Results:</i></b> The mean age was 53 (F25/M11)<b>.</b> IL-2 levels were significantly elevated in 94% (17/18) of CeD patients after 1000mg gluten; 83% (10/12) after 610mg; 41% (5/12) after 90mg; 38% (5/13) after 13mg; 25% (3/12) after 8mg; 16% (2/12) after 5mg; and 33% (4/12) after 3mg. There were no severe adverse events or significant correlation between dose of gluten and symptoms. All pre food challenge faecal GIPS were negative.</p><p><b><i>Conclusion:</i></b> All dose levels of gluten including <20mg were well tolerated but stimulated IL-2 elevation in CeD patients on a GFD. Low dose gluten challenges with serum IL-2 assessment may be useful for immune monitoring in clinical trials and may inform food regulations and support a no detectable gluten standard. CeD patients are unlikely to be aware of minute dietary exposures to gluten that reactivate gluten-specific immunity.</p><p><b>537</b></p><p><b>Effect of mushroom extract on patients with gastroesophageal reflux disease</b></p><p><b>William Wu</b><sup>1,2</sup>, Jerry Zhou<sup>2</sup> and Vincent Ho<sup>2</sup></p><p><sup>1</sup><i>Ryde Hospital, Sydney, Australia;</i> <sup>2</sup><i>Western Sydney University - School of Medicine, Campbelltown, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastro-oesophageal reflux disease (GORD) is a common condition that significantly impacts quality of life and imposes a substantial economic burden. Conventional treatments often have adverse effects and may not fully control symptoms, leading to interest in alternative therapies. Mushrooms have demonstrated gastroprotective properties in animal models and may offer a natural adjunct treatment for GORD. The aim of this study is to investigate the effects of a mushroom extract on GORD symptoms, quality of life, and biochemical markers in a single-blinded, randomized cross-over study.</p><p><b><i>Methods:</i></b> Participants with confirmed GORD on manometry and ambulatory pH monitoring will be recruited from outpatient clinics. Each participant will receive both the mushroom extract and a placebo for four weeks each, in a randomized order. Symptoms and quality of life will be assessed using validated questionnaires. Blood tests will be performed at set intervals to measure changes in biochemical markers. The study aims to recruit 50 participants which is the sample size calculated to observe a difference of 30% in the proportion of patients with GORD treated for such symptoms and cross-over group non-treated (placebo) considering α = 0.05, and β =0.80.</p><p><b><i>Results:</i></b> This study will provide initial data on the efficacy of mushroom extract in reducing GORD symptoms and improving quality of life. Changes in serum biomarkers will also be evaluated to understand potential mechanisms. This is a pilot study which is currently ongoing, preliminary results should be available at the time of presentation.</p><p><b>554</b></p><p><b>The effects of amyloidosis on the gastrointestinal tract in an Australian population</b></p><p><b>Myo Jin Tang</b>, Nikil Vootukuru, Jason Tjahyadi, Daniel Clayton-Chubb, Olga Motorna, Brendan Wisnioski, Stephen Ting, Stephen Bloom, Simon Gibbs, Rohit Sawhney and Ola Niewiadomski</p><p><i>Eastern Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal (GI) symptoms are common in systemic amyloidosis with a significant proportion attributed to amyloid deposition in the liver and GI tract. Patients with amyloidosis are also at risk of malnutrition. The aim of this study was to describe the GI and hepatic manifestations in patients with amyloidosis at time of diagnosis and over a follow up period of two years.</p><p><b><i>Methods:</i></b> This was a single centre prospective observational study of patients with newly diagnosed amyloidosis with characterisation at baseline and then follow-up assessments at 6-, 12- and 24-month intervals. Gastric involvement was identified as the key measure due to suspected high prevalence of upper GI symptoms in the amyloid population and availability of a non-invasive diagnostic test. Patients underwent a gastric emptying study (GES), serum biochemistry, micronutrient screening, liver ultrasound (US) and fibroscan at the outlined intervals. A scored patient generated subjective global assessment (PG-SGA) was completed at time of diagnosis to assess nutritional status. Patients over the age of 18 with biopsy proven systemic or localized AL amyloidosis were included. Patients with pre-existing chronic liver diseases or gastrointestinal motility disorders were excluded.</p><p><b><i>Results:</i></b> 16 patients were included in our study; 13 were diagnosed with ATTR and 3 with AL amyloidosis, respectively. The median age was 75 and with 87.5% male. Two patients only had serum biochemistry and micronutrient screening performed. Liver fibrosis was assessed with Fibroscan in 14 patients<b>.</b> The median liver stiffness measurement (LSM) at baseline was 8.4kPa. 10 patients had LSM tracked over the follow up period. 6 patients saw improvement to LSM with treatment while 4 patients saw worsened LSM despite treatment. At baseline, 5/14 patients had normal ALTs (median LSM 7.1(3.7-36.9)kPa) while 9/14 had elevated ALTs (median LSM 9.4(5.4 – 32.9)kPa). In the 9 patients with elevated ALTs, 6/9 saw improvement post treatment, 1/9 had increased ALTs and 2/9 did not have repeat ALTs. 13 patients had liver US performed. At baseline, 9/13 patients had normal liver US (median LSM in these 7.1(3.7 – 32.9)kPa), while 4/13 had hepatic steatosis on US (median LSM in these 12.4(6.8 – 36.9)kPa). In both cohorts, the majority (75% and 71% respectively) saw improvement in LSM after amyloidosis treatment. All 14 patients had normal hepatic synthetic function throughout the follow up period. 12/14 patients had elevated BNPs (which up-trended despite treatment). Four patients (28%) had abnormal GES; two at baseline (1x AL and 1x ATTR) and two developed on follow up (1x AL and 1x ATTR). None of these patients had GI symptoms. Three of these patients had mild gastric emptying delay which did not improve with treatment for their amyloidosis. One patient with ATTR amyloidosis and type 2 diabetes had moderate gastroparesis (on follow up) and did not receive treatment for amyloidosis. An additional two patients had upper GI symptoms but normal GES. Nutritional assessment as per the PG SGA was available in 10 patients. Seven patients were moderately malnourished (Score 4 or higher, category B); three of these patients had an abnormal GES. Micronutrient deficiencies were uncommon with only one patient with iron deficiency at baseline.</p><p><b><i>Conclusion:</i></b> Elevated LSM may be an early indicator of liver involvement given majority saw improvement in LSM post treatment. However, LSM has little relationship with synthetic hepatic function. Malnutrition is prevalent in amyloidosis patients, with delayed gastric emptying a possible contributing factor in some cases only.</p><p><b>573</b></p><p><b>Utility of mean nocturnal baseline impedance in the diagnosis of refractory gastroesophageal reflux disease</b></p><p>Paris Hoey<sup>1,2</sup>, Abdul Raheem Q Khan<sup>1</sup> and <b>Lei Lin</b><sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Faculty of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> The mean nocturnal baseline impedance (MNBI) is a new reflux metric, based on multichannel intraluminal impedance and pH monitoring (MII-pH) which reflects the burden of longitudinal reflux and the integrity of esophageal mucosa. MNBI may be useful in cases where the MII-pH metrics are inconclusive for pathological reflux. Our aim was to assess the diagnostic utility of MNBI in the setting of inconclusive acid exposure time (AET).</p><p><b><i>Methods:</i></b> We retrospectively identified all adult patients who underwent 24-48 hours pH impedance monitoring (Laborie and Medtronic) off Proton pump inhibitors (PPI) between January 2023 to May 2024 at two Brisbane metropolitan hospitals to investigate refractory reflux symptoms that did not adequately respond to PPI. MNBI was measured at the 5-cm impedance channel from three separate nocturnal 10-minute time periods. As per Lyon Consensus 2.0, we defined MNBI as positive when <1500 ohm, as inconclusive when between 1500-2500, and as negative when >2500 ohm. We defined AET as pathologic when >6%, as physiologic when <4%, and as inconclusive when between 4%–6%. Total reflux episodes (TRE) were defined as negative when <40/day, as inconclusive when between 40–80/day, and as positive when >80/day. The primary outcome was the rate of positive MNBI in patients with inconclusive AET to determine the yield of MNBI as an adjunctive evidence of reflux metric in the setting of diagnostic uncertainty.</p><p><b><i>Results:</i></b> 86 adult patients were included in the analysis, with an average age of 54 years, and female prevalence of 69%. There was moderate correlation between MNBI and AET in our cohort with R= -0.46 (linear regression, p <0.001), but the correlation between MNBI and TRE was not strong (R=0.21, p=0.05). In seven patients with inconclusive AET on pH-impedance testing, application of MNBI led to a diagnosis of pathologic acid exposure in four patients (57%). In three patients with both inclusive AET and inconclusive TRE, application of MNBI led to a diagnosis of pathologic acid exposure in 2 patients (67%).</p><p>\n \n </p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":null,"pages":null},"PeriodicalIF":3.7000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16704","citationCount":"0","resultStr":"{\"title\":\"Luminal Clinical\",\"authors\":\"\",\"doi\":\"10.1111/jgh.16704\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>7</b></p><p><b>Safety, efficacy and tolerability of an ultra-low volume bowel preparation (NER1006) – a real world experience</b></p><p><b>Anthony Sakiris</b>, Arvinf Rajandran, Jane Lynch, Myles Rivlin and Sneha John</p><p><i>Gold Coast University Hospital, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic assessment with colonoscopy allows for the detection of polyps and adenomas which are precursors to colorectal adenocarcinoma. The quality of bowel preparation is of significant importance to the outcome of a colonoscopy as poor bowel preparation results in prolonged procedure times, the need for repeat procedures and missed lesions. A split-dose regimen of 3-4L Polyethylene Glycol (PEG) has historically been the recommended form of bowel preparation. NER1006 is a 1L split-dose PEG bowel preparation that is comparatively novel to Australia and has been adopted within our service since 2020. NER1006 provides enhanced osmotic activity from the high-dose ascorbate that is present in the second dose. Given its ultra-low volume, the aim of this study was to assess the safety, efficacy and tolerability of NER1006 in a real-world setting within our hospital network.</p><p><i><b>Methods:</b></i> This study was a retrospective analysis of prospectively collected data for colonoscopy procedures at two centres within our hospital health service. Patients who underwent a colonoscopy between July 2020 and February 2024 and received NER1006 as bowel preparation with a split-dose regime were analysed. The study population consisted of patients who returned a positive faecal occult blood test from the Australian National Bowel Cancer Screening Program (NBCSP) as well as symptomatic patients referred through our nurse-led Direct Access Colonoscopy clinic. The quality of the bowel preparation was quantified through the Boston Bowel Preparation Scale (BBPS). The Polyp Detection Rate (PDR), Adenoma Detection Rate (ADR), Sessile Serrated Lesion Detection Rate (SSLDR) and Advanced Adenoma Rate (AADR) were also calculated as quality indicators of colonoscopy. Adverse events related to NER1006 were classified as either minor or major. Major adverse events were defined as those requiring hospitalisation or those that prevented the patient from adequately completing their bowel preparation.</p><p><b><i>Results:</i></b> A total of 2920 colonoscopies were performed on 2874 patients. There were 1571 males, 1301 females and 2 indeterminate with a mean age of 57 years. 2827/2920 (97%) of the colonoscopies performed produced a BPPS score equal to or greater than 6 (good or excellent), with an average score of 7.90. Analysis revealed a 72% PDR, 55% ADR, 16% SSLDR and 25% AADR. There were 2 cases (0.07%) of major adverse events. One patient was unable to complete their bowel preparation due to vomiting and one patient presented with an acute kidney injury. There 98 cases (3.36%) of minor adverse events. Tachycardia (>100 bpm) was the most common minor adverse event and involved 48 patients (2%). Nausea was the second most reported minor adverse event and occurred in 29 patients (1%) with only 10 cases (0.3%) associated with vomiting. 17 patients (0.6%) noted mild to moderate abdominal pain. Other non-specific minor adverse events involving 4 patients (0.14%) included headache and dizziness.</p><p><b><i>Conclusion:</i></b> This study highlights that a split-dose regime of NER1006 is a safe, effective and tolerable bowel preparation. Our utilisation of NER1006 surpasses the 90% standard for adequate bowel preparation suggested by the Quality Committee of the European Society of Gastrointestinal Endoscopy. Established targets of a 40% PDR and a 25% ADR were also exceeded in our population. In our real-world experience, only a small minority of patients who were administered NER1006 exhibited adverse effects. Clinical dehydration due to NER1006 has been demonstrated in previous studies and may have been a contributor for our patients with tachycardia. However, other factors such as anxiety should also be considered. The implementation of multimodal education regarding the process of bowel preparation has assisted in enhancing the overall safety and tolerability of NER1006 within our network. Instructions for our patients to sip the bowel preparation slowly through a straw to minimise taste, drinking clear savoury fluids to offset the sweetness of NER1006 and ensuring adequate clear fluid intake have all been suggested strategies. This is the largest study regarding ultra-low volume bowel preparation reported within the Australian context, however it is limited by its retrospective model. Larger multi-centre prospective studies are recommended to further identify the factors that contribute towards the potential adverse effects of ultra-low volume bowel preparation in order to better prevent or manage them.</p><p><b>9</b></p><p><b>The presence of hiatal hernia is a significant predictor for symptomatic recurrence after cessation of vonoprazan therapy for gastroesophageal reflux disease: A long-term observational study</b></p><p><b>Satoshi Shinozaki</b><sup>1</sup>, Hiroyuki Osawa<sup>2</sup>, Yoshimasa Miura<sup>3</sup>, Hirotsugu Sakamoto<sup>2</sup>, Yoshikazu Hayashi<sup>2</sup>, Tomonori Yano<sup>2</sup>, Edward Despott<sup>4</sup> and Hironori Yamamoto<sup>2</sup></p><p><sup>1</sup><i>Shinozaki Medical Clinic, Utsunomiya, Japan;</i> <sup>2</sup><i>Jichi Medical University, Shimotsuke, Japan;</i> <sup>3</sup><i>Nihon University, Chiyoda, Japan;</i> <sup>4</sup><i>Royal Free Hospital, London, UK</i></p><p><b><i>Background and Aim:</i></b> Gastroesophageal reflux disease (GERD) symptoms frequently recur after cessation of acid blockers. The presence of a hiatal hernia may worsen GERD symptoms and increase the risk of esophageal malignancy. The aim of this study is to clarify the timing and predictors for recurrence of GERD symptoms after cessation of vonoprazan (VPZ) therapy.</p><p><b><i>Methods:</i></b> A retrospective observational study involved 86 patients who underwent cessation of VPZ therapy for symptomatic GERD. Collated data from medical record review included the endoscopic findings and Izumo scale score.</p><p><b><i>Results:</i></b> The mean duration of continuous VPZ therapy before cessation was 7.9 months. GERD symptoms requiring the resumption of VPZ therapy recurred in 66 of 86 patients (77%). Kaplan-Meier analysis showed that overall recurrence-free rates at 6 months, one and two years after VPZ cessation were 44%, 32% and 23%, respectively. Alcohol use, the presence of a hiatal hernia and long-term therapy for more than six months were identified as significant positive predictors for symptomatic recurrence. Notably, hiatal hernia had the highest hazard ratio in both univariate and multivariate analyses. The recurrence-free rate in patients with a hiatal hernia was much lower at 6 months than in patients without a hiatal hernia (15% and 51%, respectively p=0.002). After the symptomatic recurrence, GERD symptoms improved significantly after one-month VPZ therapy.</p><p><b>11</b></p><p><b>Establishment of a tertiary faecal microbiota transplant service and 24 month outcomes</b></p><p><b>Emma Buckner</b><sup>1,2</sup> and Thomas Goodsall<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology, John Hunter Hospital, Newcastle, Australia;</i> <sup>2</sup><i>School of Medicine and Public Health, The University of Newcastle, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> <i>Clostridium difficile</i> infection (CDI) is the most common cause of nosocomial diarrhoea in Australia and results in morbidity, risk of mortality, increased length of admission and resource utilisation. Recurrent CDI risk after antibiotic treatment is 20% and morbidity and mortality risk increase to 26-36% after first recurrence. Faecal Microbiota Transplant (FMT) is recommended in Australia as the preferred management for second and subsequent recurrences of CDI and is effective in 90% of cases after one FMT and 98% after a second FMT. We report our experience introducing an FMT service to a tertiary hospital and report the 24-month patient outcomes.</p><p><b><i>Methods:</i></b> A business case was prepared and submitted to the New Interventional Procedures and Quality use of Medicines committee at our hospital for introduction of an FMT service using TGA approved stool sourced from a third-party Australian provider (BiomeBank, Adelaide, South Australia). Successful approval was granted based on supporting evidence for efficacy and safety, proposed use of TGA approved stool product, limited scope of practice to recurrent or refractory CDI, structured supervision and accreditation program with audit and governance oversight, a cost analysis demonstrated cost benefit of FMT compared with antibiotic therapy, and supply of a -80 degree freezer for local storage of donor stool product.</p><p><b><i>Results:</i></b> 21 FMT procedures were performed in 17 patients. Demographics and outcomes are presented in Table 1. Complete remission was achieved in 14/17 patients (82%) after the first FMT and of the three patients requiring repeat FMT, one achieved remission after the second FMT, one required colectomy for persistent <i>C. difficile</i> colitis and megacolon, and one experienced ongoing recurrence in the setting of prophylactic antibiotics for lung transplant. Another patient was diagnosed with intercurrent Crohn’s colitis at the time of FMT and required colectomy for refractory Crohn’s colitis despite steroids and infliximab 4 weeks after FMT; the stool was <i>C. difficile</i> PCR negative and there was no histological evidence of persistent <i>C. difficile</i> infection. One other patient had deep ileocolonic skip ulcers consistent with Crohn’s disease and responded to FMT and induction steroids, while another had endoscopic and histological evidence of ulcerative proctitis which clinically responded to FMT and was in clinical and biomarker remission at 6 months. One patient experienced persistent diarrhoea after FMT despite clearance characterised by negative stool PCR and was subsequently diagnosed with a duodenal neuroendocrine tumour requiring Whipple’s resection.</p><p><b><i>Conclusion:</i></b> A funded FMT model was successfully introduced at our hospital with Clinical Governance approval. Primary response and cure was achieved in 88% of patients consistent with published outcomes. IBD was diagnosed in 3/17 patients at the point of FMT and cured in one case. Risk factors for requiring subsequent FMT were severe CDI with colitis and ongoing antibiotic use. No significant adverse events or deaths were directly attributable to FMT. This model could be reproduced to support other centres wanting to introduce an FMT service to provide quality evidence-based care.</p><p><b>18</b></p><p><b>Haemosuccus pancreaticus: an interesting and rare presentation of upper gastrointestinal bleeding</b></p><p><b>Annabelle Faint</b><sup>1</sup>, <b>Laurence Vaitiekunas</b><sup>1,4</sup>, Muddassir Rashid<sup>2</sup>, Arjuna Somasundaram<sup>2</sup> and Alexander Huelsen<sup>1,3</sup></p><p><sup>1</sup><i>Digestive Health, Gold Coast University Hospital, Gold Coast, Australia;</i> <sup>2</sup><i>Department of Radiology, Gold Coast University Hospital, Gold Coast, Australia;</i> <sup>3</sup><i>School of Medicine, University of Queensland, Gold Coast, Australia;</i> <sup>4</sup><i>School of Medicine and Dentistry, Griffith University, Gold Coast, Australia</i></p><p><b><i>Introduction:</i></b> Haemosuccus pancreaticus (HP) is a rare and life-threatening cause of upper gastrointestinal bleeding and is characterised by haemorrhage into the main pancreatic duct.<sup>1,2</sup> HP has a mortality rate of up to 9.6%.<sup>3</sup> Typically associated with chronic pancreatitis, HP arises from prolonged enzymatic exposure of peripancreatic arterial walls, precipitating a bleeding event that fistulsed into the pancreatic ductal system.<sup>4</sup> Clinical manifestations include haematemesis, melaena, abdominal pain, and in severe cases, haemodynamic instability. Diagnostic challenges can often arise due to the failure of initial endoscopic evaluation to identify a source of bleeding, compounded by a general lack of familiarity and awareness of this entity.<sup>1,2</sup> Computed tomography angiography (CTA) remains the gold standard for diagnosis and can guide management which includes angiographic embolisation and surgery. Surgical treatment is typically reserved for uncontrolled haemorrhage or when embolisation fails.<sup>2</sup> We describe a case of a 29-year-old male with a background of chronic pancreatitis and pancreatic pseudocyst (PC), exhibiting clinical manifestations indicative of haemosuccus pancreaticus, wherein a distal splenic artery pseudoaneurysm had bled into a pancreatic pseudocyst and the pancreatic ductal system. This was treated successfully by angiographic embolisation of the splenic artery.</p><p><b><i>Case Report:</i></b> A 29-year-old male with a history of alcohol-related chronic pancreatitis and an 8cm pancreatic tail pseudocyst presented with a two-day history of hematemesis, melaena, and epigastric pain. He reported abstinence from alcohol for several months and he denied smoking and the use of anti-inflammatory medications. His last gastroscopy in 2022 showed chronic gastritis only. On examination, he was pale with a soft abdomen demonstrating severe epigastric tenderness. There was no melaena on rectal examination. He was tachycardic to 116bpm and his blood pressure was 124/64 mmHg. Biochemistry revealed a hemoglobin of 37g/L, ferritin 2ug/L, urea of 1mmol/L, total bilirubin 5umol/L, ALP 92U/L, GGT 257U/L, ALT 16U/L, AST 25U/L. Resuscitation with four units of packed red blood cells and intravenous fluids stabilised his condition. His haemoglobin incrementally increased to 71g/L without evidence of ongoing gastrointestinal bleeding during his admission. Urgent gastroscopy demonstrated gastric erythema and small erosions in the antrum, without stigmata of recent bleeding. A subsequent abdominal CTA showed a 7 x 6mm distal splenic artery pseudoaneurysm projecting inferiorly into a large, longstanding pseudocyst posterior to the pancreatic tail, not identifiable on initial contrast CT abdomen. On comparison with prior imaging, the PC had developed intracystic high density material, in keeping with interval haemorrhage (Image 2). Angiographic embolisation with three 5mm microcoils to the lower pole branch of the splenic artery was successful (Image 4). He remained clinically stable following the procedure and was discharged after a period of inpatient observation.</p><p><b>References</b></p><p>\\n 1. <span>Alshaikhli, A</span>, <span>Al-Hillan, A</span>. (<span>2023</span>). <span>Haemosuccus Pancreaticus. StatPearls. Treasure Island (FL)</span>. StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK570570/</p><p>\\n 2. <span>Yashavanth, H. S.</span>, <span>Jagtap, N.</span>, <span>Singh, J. R.</span>, <span>Ramchandani, M.</span>, <span>Lakhtakia, S.</span>, <span>Tandan, M.</span>, <span>Gupta, R.</span>, <span>Vamsi, M.</span>, <span>Bhaware, B.</span>, <span>Rao, G. V.</span>, and <span>Reddy, D. N.</span> (<span>2021</span>) <span>Hemosuccus Pancreaticus: A systematic approach</span>. <i>Journal of Gastroenterology and Hepatology</i>, <span>36</span>: <span>2101</span>–<span>2106</span>. https://doi.org/10.1111/jgh.15404.</p><p>\\n 3. <span>Yu, P</span>, <span>Gong, J</span>. <span>Hemosuccus pancreaticus: A mini-review</span>. <i>Ann Med Surg (Lond)</i>. <span>2018</span>; <span>28</span>: <span>45</span>-<span>48</span>. Published 2018 Mar 9. https://doi.org/10.1016/j.amsu.2018.03.002</p><p>\\n 4. <span>Mekheal, N.</span>, <span>Roman, S.</span>, <span>Alkomos, M. F.</span>, <span>Mekheal, E.</span>, <span>Farokhian, A.</span>, <span>Millet, C.</span>, <span>Shah, H.</span>, <span>Melki, G.</span>, & <span>Baddoura, W.</span> (<span>2022</span>). <span>Hemosuccus Pancreaticus: Challenging Diagnosis and Treatment</span>. <i>European Journal of Case Reports in Internal Medicine</i>, <span>9</span>(<span>5</span>), 003337. https://doi.org/10.12890/2022_003337</p><p><b>39</b></p><p><b>Comparative evaluation of Atmo Gas Capsule System and SmartPill GI Monitoring System for transit time assessment in motility disorders</b></p><p><b>Jerry Zhou</b><sup>1</sup>, Allen Lee<sup>2</sup>, Thomas Abell<sup>3</sup>, Ashok Attaluri<sup>4</sup>, Michael Cline<sup>5</sup>, William Hasler<sup>6</sup>, Vincent Ho<sup>1</sup>, Anthony Lembo<sup>5</sup>, Amir Masoud<sup>7</sup>, Richard McCallum<sup>8</sup>, Baharak Moshiree<sup>9</sup>, Eamonn Quigley<sup>10</sup>, Satish Rao<sup>11</sup>, Mayra Sanchez<sup>7</sup>, Irene Sarosiek<sup>8</sup>, Abigail Stocker<sup>3</sup>, Brian Surjanhata<sup>12</sup>, William Chey<sup>2</sup> and Braden Kuo<sup>11</sup></p><p><sup>1</sup><i>Western Sydney University, Sydney, Australia;</i> <sup>2</sup><i>University of Michigan, Ann Arbor, USA;</i> <sup>3</sup><i>University of Louisville, Louisville, USA;</i> <sup>4</sup><i>Alliance for Multispecialty Research, Kansas City, USA;</i> <sup>5</sup><i>Cleveland Clinic, Cleveland, USA;</i> <sup>6</sup><i>Mayo Clinic, Scottsdale, USA;</i> <sup>7</sup><i>Hartford Health, Fairfield, USA;</i> <sup>8</sup><i>Texas Tech University, El Paso, USA;</i> <sup>9</sup><i>Atrium Health Wake Forest Medical University, Charlotte, USA;</i> <sup>10</sup><i>Houston Methodist Research Institute, Houston, USA;</i> <sup>11</sup><i>Augusta University, Augusta, USA;</i> <sup>12</sup><i>Massachusetts General Hospital, Boston, USA</i></p><p><b><i>Background and Aim:</i></b> Motility disorders, such as gastroparesis and slow transit constipation (STC), are common gastrointestinal (GI) conditions affecting up to 5% of individuals worldwide. The symptoms of motility disorders can be debilitating, affecting quality of life and driving utilisation of healthcare systems. Diagnosis relies on evaluation of regional transit times, with delayed gastric and colonic transit indicated for gastroparesis and STC, respectively. The SmartPill GI Monitoring System (SmartPill), an FDA-cleared wireless motility capsule (WMC), has been used in the assessment of gastroparesis and STC since 2008 but has recently been discontinued, leaving a need for a like replacement. This study aimed to assess a new WMC, the Atmo Gas Capsule System (Atmo Capsule), against SmartPill for the assessment of regional transit time in these conditions.</p><p><b><i>Methods:</i></b> Individuals with upper, lower, or combined GI symptoms were recruited in a prospective multi-centre study. Participants concomitantly ingested the Atmo Capsule and SmartPill in a randomized order. Regional transit times including Gastric Emptying Time (GET) and Colonic Transit Time (CTT) were measured and compared between the devices, where paired data were available. GET >5 hours and CTT >59 hours were defined as delayed.</p><p><b><i>Results:</i></b> 213 participants were recruited across 12 sites: 177 yielded paired GET results, and 147 for CTT. Pearson correlation coefficients for GET and CTT comparisons between Atmo Capsule and SmartPill were 0.86 (0.81-0.89) and 0.74 (0.66 – 0.81) respectively. GET demonstrated a positive predicted value (PPV) of 78.00% (SE: 5.86%), negative predictive value (NPV) of 85.83% (SE: 3.09%), and overall agreement (OA) of 83.62% (SE: 2.78%). For CTT, PPV was 67.35% (SE: 6.70%), NPV was 92.89% (SE: 2.60%), and OA was 84.35% (SE: 3.00%). No serious adverse device effects were reported. 32.2% of the total GET evaluable cohort had delayed GET, 27.2% of the CTT evaluable cohort had delayed CTT. For the cohort that had measurement for all transit regions, 20% had delayed CTT only, 11% had delayed GET only and 18% had a delay in multiple GI regions as measured by Atmo.</p><p><b><i>Conclusion:</i></b> The Atmo Capsule exhibited substantial agreement with SmartPill in measuring both GET and CTT, highlighting its utility as a potential replacement for the discontinued SmartPill for assessment of motility disorders. Observations of multi-regional dysmotility further highlight the value of measuring multiple regional of the GI tract with a single test.\\n\\n </p><p><b>46</b></p><p><b>The efficacy of EndoClot® in the prevention of delayed bleeding following advanced endoscopic resection</b></p><p><b>Anthony Sakiris</b>, Christopher Graddon, Arvinf Rajandran and Sneha John</p><p><i>Gold Coast University Hospital, Gold Coast, Australia</i></p><p><b><i>Background and Aims:</i></b> Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD) are advanced endoscopic techniques that have been increasingly employed for the resection of large precancerous polyps or early gastrointestinal neoplasia. Delayed bleeding is a common adverse event related to endoscopic resection. Modalities such as thermocoagulation with haemostatic forceps and clipping are available options to control bleeding. Recently, topical haemostatic agents have been utilised as an alternative therapy and are applied over the bleeding resection site. EndoClot® is a novel topical haemostatic agent that consists of biocompatible, non-pyrogenic and starched derived polysaccharides. EndoClot® is able to effectively control bleeding by creating a gelled matrix that accelerates the clotting process by concentrating platelets, red blood cells and coagulation proteins at the resection site. The matrix lasts temporarily and can dissipate over a few hours to days. EndoClot® has recently been incorporated within our health network. The aim of our study was to assess the efficacy of EndoClot® in preventing delayed bleeding following the advanced endoscopic resection of high-risk lesions.</p><p><b><i>Methods:</i></b> This study was a retrospective analysis of prospectively collected data of advanced endoscopic resections at one centre within our hospital health service. Patients who underwent advanced endoscopic resection between March and April 2024 and received EndoClot® adhesive were analysed. EMR was performed as per standard technique with submucosal injection with gelofusin and methylene blue +\\\\- adrenaline at the endoscopist’s discretion. Indications for EndoClot® use within the colon and rectum included polyps proximal to the splenic flexure greater than 20mm resected with hot-snare EMR and polyps distal to the splenic flexure resected with hot-snare EMR or ESD in high-risk patients (i.e. use of antiplatelets or anticoagulation). Indications for EndoClot® use within the duodenum included polyps greater than 10mm resected with hot-snare EMR and any ampullectomy. Indications for EndoClot® in the oesophagus and stomach included any lesions resected with EMR or ESD in high-risk patients. We recorded basic patient demographics and the use of antiplatelets or anticoagulation. Lesion characteristics such as size, location and histology were documented. Delayed bleeding was defined as clinically evident gastrointestinal bleeding that occurred up to 14 days following the procedure which resulted in an emergency department presentation, required a blood transfusion or a repeat intervention.</p><p><b><i>Results:</i></b> EndoClot® was administered following the endoscopic resection of 11 lesions for a total of 10 patients. 90% were male with mean age 67 years (SD 8.62 years). 2 patients (20%) were taking either antiplatelets or anticoagulation. 64% of resections were in the colon or rectum, 27% in the duodenum and 9% in the oesophagus. EMR was the most utilised resection technique (91%). The most common lesion was a tubular adenoma (36%) and 27mm was the mean lesion size resected (SD 11.34mm). There was one delayed post-polypectomy bleed in a patient on Clopidogrel and Warfarin (re-commenced 48 hours post procedure with Enoxaparin bridging), who presented 10 days following a descending colon hot-snare EMR of a 25mm tubular adenoma. This patient underwent a total of 3 subsequent inpatient colonoscopies to definitively control the bleeding over 3 admissions, with evidence of a visible vessel requiring thermal therapy at the second colonoscopy and re-application of EndoClot® during one of the procedures.</p><p><b><i>Conclusion:</i></b> Our study demonstrates that EndoClot® is an effective haemostatic agent for the advanced endoscopic resection of high-risk lesions given no evidence of delayed bleeding for patients not on antiplatelet or anticoagulant therapy. Our single delayed bleeding case required 3 subsequent colonoscopy procedures with ongoing bleeding despite thermal therapy, and hence the rebleeding risk would unlikely have been mitigated by use of a topical hemostatic agent. EndoClot® appears to be safe with no noted adverse effects related to its administration. Our study is limited due to its retrospective nature with small sample size. Obtaining data from a larger cohort will enable higher-quality evidence regarding the use of EndoClot®.</p><p><b>54</b></p><p><b>Delayed autonomic ganglionopathy following nivolumab therapy in a patient with metastatic melanoma</b></p><p><b>Kai Dong Choong</b><sup>1,2</sup>, <b>Aung Du</b><sup>2</sup>, Milly Wong<sup>1</sup> and Digby Cullen<sup>1</sup></p><p><sup>1</sup><i>St John of God, Perth, Australia;</i> <sup>2</sup><i>Sir Charles Gairdner Hospital, Perth, Australia</i></p><p><b><i>Introduction:</i></b> Immune checkpoint inhibitors (ICI) have shown improved clinical outcomes in several malignancies; however, they have also been associated with immune-related adverse effects (irAE). Neurological irAE, in comparison to other systems are reported to be rare. Alongside clinical scarcity, the mechanisms contributing to neurotoxicity remain poorly understood, rendering diagnosis challenging and requiring a high degree of suspicion. Here, we report a case of delayed autonomic ganglionopathy, likely precipitated by use of ICI, nivolumab.</p><p><b><i>Case Report:</i></b> A 76-year-old man presented with diarrhoea, abdominal pain, anorexia, post-prandial fullness, dizziness and 24kg weight loss over 6 months. Significant medical history includes metastatic melanoma treated with nivolumab for one year, completed three months before onset of symptoms. On examination, he appeared cachectic. He was hypertensive (150/94 mmHg), had a regular heart rate (74 bpm) and postural drops of up to 70mmHg. Other examination findings were unremarkable. General haematology and biochemistry revealed hyponatraemia (129mmol/L). Thyroid function tests and screening for endocrine causes were unremarkable. Normal chromogranin-A levels excluded neuroendocrine tumours. Coeliac serology was negative. Stool microbiology was negative for pathogens. Metronidazole challenge did not alleviate gastrointestinal symptoms. Normal faecal calprotectin and C-reactive protein excluded enteral inflammation. Antinuclear antibodies were normal and paraneoplastic screen was also unremarkable. Protein electrophoresis, serum light chains were normal and intestinal biopsy excluded amyloidosis. PET-CT did not detect metastasis. Bedside and stress echocardiography were unremarkable. Gastroscopy unveiled large residual food boluses, suggestive of decreased gastric motility. After exclusion of infective, neoplastic, autoimmune and metabolic causes, we concluded that this was a case of delayed autonomic ganglionopathy secondary to nivolumab. Management focused on symptomatic relief and improving quality of life. Diarrhoea was partially managed by cholestyramine, pancreatic enzymes, loperamide, and domperidone. Abdominal pain was managed with mebeverine in combination with both sublingual and transdermal buprenorphine. Anorexia and post-prandial fullness were managed with nizatidine. Postural hypotension was partially alleviated with midodrine, fludrocortisone and sodium chloride supplements. Recent follow-up included dose adjustments to fludrocortisone and midodrine. Postural hypotension remained but did not precipitate falls or syncope. Diarrhoeal episodes decreased to 4-5 times daily. Our patient regained some independence and was able to engage in social activities.</p><p><b><i>Conclusion:</i></b> We report a case of delayed autonomic ganglionopathy caused by use of nivolumab monotherapy. As acute and subacute presentations of neurological irAE are rare, and delayed presentations are exceedingly rare, clinicians ought to maintain a high level of suspicion on patients receiving treatment with ICI.</p><p><b>73</b></p><p><b>Living with faecal incontinence: A qualitative investigation of patient experiences and preferred outcomes through semi-structured interviews</b></p><p><b>Sadé Assmann</b><sup>1,2,3</sup>, Daniel Keszthelyi<sup>2,3</sup>, Stephanie Breukink<sup>1,3,4</sup> and Merel Kimman<sup>5</sup></p><p><sup>1</sup><i>Department of Surgery and Colorectal Surgery, Maastricht University Medical Centre +, Maastricht, The Netherlands;</i> <sup>2</sup><i>Department of Gastroenterology-Hepatology, Maastricht University Medical Centre, Maastricht, The Netherlands;</i> <sup>3</sup><i>Research Institute of Nutrition and Translational Research in Metabolism (NUTRIM), Maastricht University, Maastricht, The Netherlands;</i> <sup>4</sup><i>Research Institute for Oncology and Reproduction (GROW), Maastricht University, Maastricht, The Netherlands;</i> <sup>5</sup><i>Department of Clinical Epidemiology and Medical Technology Assessment, Care and Public Health, Research Institute (CAPHRI), Maastricht University Medical Centre +, Maastricht, The Netherlands</i></p><p><b><i>Background and Aim:</i></b> Faecal incontinence (FI) is a prevalent and debilitating anorectal problem which can cause embarrassment, anxiety, social isolation and diminishes quality of life (QoL). Currently, there is no optimal treatment option for FI, consequently, treatments primarily focus on symptom reduction and improving QoL. In order to gain a clearer understanding of the challenge’s patients encounter, it is essential to actively listen to patients’ perspectives and experiences, as well as the specific outcomes they aim to achieve from treatment. This study aims to explore how FI impacts patients’ lives and identify important treatment outcomes as part of the development of a Core Outcome Set (COS).</p><p><b><i>Methods:</i></b> Patients with FI were recruited from surgery and gastroenterology outpatient clinics in the Netherlands. Semi-structured interviews were performed, audio recorded, transcribed per verbatim and coded. Thematic analysis using the framework method with an inductive open coding approach was performed to identify (sub)themes and categories relevant to the patients.</p><p><b><i>Results:</i></b> Twelve interviews were conducted before saturation was reached (75% female, 25% male, mean age 63, range 39-83 year). Four main themes emerged ‘Physical symptoms’, ‘Impact on daily life’, ‘Emotional impact’ and ‘Coping’. Patients expressed how FI severely limits daily activities and emotional wellbeing. Treatment priorities centred on resuming normal activities rather than solely on symptom reduction (table 1).</p><p><b><i>Conclusion:</i></b> The impact of FI extends far beyond uncontrolled loss of faeces, affecting psychological, emotional, and social wellbeing. Patients prioritise outcomes focussed on reclaiming normalcy and independence rather than focusing on physical symptoms alone. Integrating these patient-centered outcomes in future studies could enhance treatment satisfaction and patient-perceived treatment success. Furthermore, outcomes identified through this study will be combined with other outcomes identified through literature review, forming a comprehensive list for a Delphi survey with relevant stakeholders to establish a consensus on a final list of outcomes for a COS for FI.</p><p><b>100</b></p><p><b>Digitally-delivered gut-directed hypnotherapy is superior to an active control program in patients with irritable bowel syndrome: a randomised controlled trial</b></p><p><b>Ellen Anderson</b>, Simone Peters, Peter Gibson and Emma Halmos</p><p><i>Monash University and Alfred Health, Melbourne, Australia</i></p><p><b><i>Background:</i></b> Face-to-face gut-directed hypnotherapy (GDH) is an effective therapy for irritable bowel syndrome (IBS), but is currently considered third line due to limited accessibility. Nerva is a digitally-delivered GDH program, comprising of psychoeducation (that includes diaphragmatic breathing) and GDH, with the intention to improve access to the IBS population. Efficacy data are limited to a retrospective study, in which gastrointestinal and psychological outcomes improved.</p><p><b><i>Aim:</i></b> To perform a single-blinded randomised controlled trial to determine the efficacy of the app-delivered GDH program compared with an active control of psychoeducation alone on gastrointestinal symptoms and psychological outcomes in patients with IBS.</p><p><b><i>Results:</i></b> Of 244 enrolled participants, 45 withdrew prior to completing the first 14 sessions. Hence, 199 (96 GDH and 103 Control; median age 37 (IQR 30-46) years and 91% were female) were included in a modified intention to treat analysis. Baseline demographics, gastrointestinal symptoms, psychological indices and QoL were similar between the groups and there was an even distribution of participants from Australia and USA. At the conclusion of the intervention, GDH induced clinical response in 71% compared to 53% with Control (p=0.011; chi-squared). IBS-SSS was a median (IQR) of 200 (131-304) with GDH, which was lower than 246 (165-308) with Control (p=0.032; Mann-Whitney; Figure). This was a reduction of 97 (41-166) for GDH and 57 (0-123) for Control (p=0.008) from baseline. There was a divergence in symptom improvement from 28 sessions (see Figure). Improvement in IBS-VAS pain >30% was reported by 59% with GDH compared to 41% with Control (p=0.009). IBS-QOL improved by 9 (0-27) with GDH compared to 3 (0-15) with Control (p=0.017). Both interventions improved DASS-21and SCL-90 scores similarly. Six months following intervention, 138 (84% GDH and 75% Control) completed symptom measures. The improved IBS-SSS and IBS-VAS pain scores compared with baseline were maintained in those participants (p<0.0001 for both groups), but there were no longer differences between the groups.</p><p><b><i>Conclusion:</i></b> The digitally-delivered GDH intervention is superior to psychoeducation alone in alleviating IBS symptoms and in a greater proportion of participants and in improving participant QoL. Benefits appear to be durable. These results support the use of app-delivered GDH (with psychoeducation) that is cheaper and more accessible than in-person therapy for IBS sufferers.</p><p><b>103</b></p><p><b>Endoscopic intermuscular dissection: blurring the line between endoscopy and surgery</b></p><p><b>Niroshan Muwanwella</b><sup>1</sup> and Dilini Gunawardena<sup>2</sup></p><p><sup>1</sup><i>Royal Perth Hospital, Perth, Australia;</i> <sup>2</sup><i>PathWest Laboratory Medicine, Perth, Australia</i></p><p><b><i>Introduction:</i></b> Endoscopic Intermuscular Dissection (EID) is a novel endoscopic resection method where a lesion is resected including the inner circular muscle layer of the gastrointestinal tract. Published literature is limited, however shows promising results both as a means of obtaining accurate local staging as well as a curative, organ sparing, endoscopic resection method for T1 rectal malignancies suspicious for deep submucosal invasion (SMI). We present the first Australian report of EID utilised to resect a pT1 malignant rectal polyp with superficial SMI.</p><p><b><i>Case report:</i></b> A 70-year-old man was referred for resection of a large rectal polyp. Assessment revealed a 3cm Paris IIa+Is polyp. Kudo pit pattern was type III<sub>L</sub> in the periphery, type III<sub>S</sub> in the centre and a small area with type V<sub>I</sub> and V<sub>N</sub>. Imaging classification was malignant polyp suspicious for SMI. Therefore, decision was made to undertake EID to ensure complete (R0) resection. Circumference of the polyp was marked with diathermy. Standard lifting agent consisting of colloid, Indigo Carmine and dilute Adrenaline was injected submucosally into the periphery of the polyp. Using a Dual Knife J (Olympus endoscopy, Tokyo, Japan), mucosa was incised and the submucosa exposed. After applying traction, circular muscle layer was incised to expose intermuscular space. Dissection was performed in this plane and the polyp removed ensuring R0 resection leaving the outer longitudinal muscle layer intact. The defect was left open, intravenous antibiotic administered intra-procedure. Patient made an uneventful recovery and was discharged home the next day on oral antibiotics. Histopathology revealed a 13mm well differentiated invasive adenocarcinoma, pT1, SM1. Deep and circumferential margins were clear and there was no perineural or lymphatic invasion. However, venous invasion and tumour budding was identified. Therefore, patient was referred to colorectal surgical team for a discussion of completion surgery.</p><p>Selecting the optimal treatment modality for T1 rectal malignancies suspicious for deep SMI is important to be able to offer patients with organ sparing resections. Available imaging modalities are poor at differentiation between T1 and >T2 cancers. EID bridges a gap in this area. It can offer curative endoscopic resection for a considerable proportion of these patients while providing accurate staging for the remainder, justifying major abdominal surgery.</p><p><b>119</b></p><p><b>Faecal microbiota transplant in advanced Parkinson's disease, microbial changes and effects on motor and gastrointestinal function: A randomised placebo controlled crossover study</b></p><p>Lucy Bracken<sup>1,2</sup>, Fiona Tudehope<sup>1</sup>, William J Ryan<sup>3</sup>, Scott Read<sup>1,4</sup>, Duncan Wilson<sup>5</sup>, Tanya Golubchik<sup>6</sup>, Brian Gloss<sup>7</sup>, Sarah Bray<sup>5</sup>, Laura Williams<sup>5</sup>, Sophie Waller<sup>5</sup>, Jessica Qiu<sup>5</sup>, David Tsui<sup>5</sup>, Donna Galea<sup>5</sup>, Neil Mahant<sup>5</sup>, Hugo Morales Briceno<sup>5</sup>, Florence CF Chang<sup>5,2</sup>, Jane Griffith<sup>5</sup>, Sushil Bandodkar<sup>5</sup>, Xi Chen<sup>5</sup>, Victor Fung<sup>5,2</sup> and <b>David Van Der Poorten</b><sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology Department, Westmead, Australia;</i> <sup>2</sup><i>Faculty of Medicine, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>John Curtin School of Medical Research, Australian National University, Canberra, Australia;</i> <sup>4</sup><i>School of Medicine, Western Sydney University, Blacktown, Australia;</i> <sup>5</sup><i>Neurology Department, Westmead Hospital, Westmead, Australia;</i> <sup>6</sup><i>School of Medical Sciences, University of Sydney, Sydney, Australia;</i> <sup>7</sup><i>Westmead Institute for Medical Research, Westmead, Australia</i></p><p><b><i>Background and Aim:</i></b> Preliminary findings from case reports and small human studies suggest that faecal microbiota transplant (FMT) has therapeutic potential in Parkinson’s disease (PD) with effects on both motor and gastrointestinal symptoms. We aimed to determine whether FMT improves motor function, constipation and quality of life in patients with advanced PD and the specific microbiome changes associated with this.</p><p><b><i>Methods:</i></b> We conducted a randomised, blinded, placebo-controlled, crossover trial of FMT in patients with PD already on treatment with levodopa/carbidopa via a PEG-J tube. Patients had to be on a stable dose for 6 months and have ≥ 3 hours of OFF time. Patients were randomized 1:1 to FMT or Placebo and received infusions via PEG-J tube on week 0 and 2 and then had crossover therapy on weeks 6 and 8 after a four-week washout. Biomictra FMT (BiomeBank SA) was used with two different donors. The primary outcomes were safety/tolerability of FMT and change in daily OFF time. Secondary outcomes were change in constipation and quality of life (QOL) scores. Microbial composition was assessed at baseline, post FMT/Placebo and end of study and compared to clinical endpoints. Microbiome sequencing was performed on extracted DNA via the Illumina NextSeq 2000 platform. Species classification and analysis was performed using MetaPhlan.</p><p><b><i>Results:</i></b> We undertook preliminary analysis after recruiting nine patients who each had completed FMT and placebo infusions. The median age of the patients was 64 with the majority male (78%). There were no serious adverse events recorded. There were three (9%) infusion related blood pressure fluctuations that did not require treatment and six (17%) infusion related episodes of mild abdominal discomfort and bloating split equally between placebo and FMT. Compared to baseline, there was an increase in microbiome richness by Chao1 index post FMT (273 vs 311, p=0.04) and alpha diversity measured by Shannon index (3.89 vs 4.07, p=0.11). The five most common genera at baseline in study patients were <i>Bacteroides</i>, <i>Phocaeicola</i>, <i>Escherichia, Alistipes</i> and <i>Blautia</i>, while in donors it was <i>Bifidobacterium, Phocaeicola, Faecalibacterium, Lachnospiraceae</i> and <i>Bacteroides</i>. Post FMT patients had substantially more <i>Faecalibacterium</i> and <i>Bifidobacterium</i> in keeping with engraftment. Compared to baseline, six patients had improved OFF time, ON time and QOL scores after FMT, but only two had an improvement in constipation. When compared with Placebo, FMT was associated with an absolute reduction in 1.04 OFF hours (p=0.193) and an absolute increase in ON hours by 1.53 (p=0.113). In those with less OFF time and better QOL scores post FMT, baseline microbiome alpha diversity was increased (4.1 vs 3.61, p=0.11), as was post FMT richness (278 v 337, p=0.13). There was no difference in clinical or microbiome outcomes when comparing the two FMT donors.</p><p><b><i>Conclusions:</i></b> This preliminary analysis shows FMT in Parkinson’s disease patients via PEG-J tube is a safe and potentially effective treatment. Microbial changes related to richness and diversity appear to be associated with response to therapy. Specific changes at a genera and species level require further characterization.</p><p><b>138</b></p><p><b>A novel blood-based cytokine release assay shows high sensitivity and specificity for coeliac disease diagnosis even in people following a strict gluten-free diet</b></p><p><b>Olivia Moscatelli</b><sup>1</sup>, Amy Russell<sup>1</sup>, Lee Henneken<sup>2</sup>, Linda Fothergill<sup>1</sup>, Hugh Reid<sup>3</sup>, Jamie Rossjohn<sup>3</sup>, Melinda Hardy<sup>1</sup>, Vanessa Bryant<sup>1</sup> and Jason Tye-Din<sup>1</sup></p><p><sup>1</sup><i>Walter and Eliza Hall Institute, Melbourne, Australia;</i> <sup>2</sup><i>The Royal Melbourne Hospital, Melbourne, Australia;</i> <sup>3</sup><i>Monash University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> T-cell diagnostics in clinical practice are limited to tuberculosis but could eventually be used to replace histology in antigen-driven immune diseases, such as coeliac disease (CD), if they were more sensitive. Current diagnosis of CD is suboptimal. For patients already following a gluten-free diet (GFD), prolonged gluten challenge to establish a diagnosis is often poorly tolerated. Detection of gluten-specific CD4+ T cells is attractive for CD diagnosis but sophisticated techniques like HLA-DQ-gluten tetramers are impractical. We recently showed serum interleukin (IL)-2 release to gluten is a marker of gluten-specific T cells. We aimed to assess the diagnostic performance of an IL-2 whole blood assay (WBA) employing an “in-tube gluten challenge” and compared this to serum IL-2 levels after oral gluten and tetramer analysis.</p><p><b><i>Methods:</i></b> The IL-2 WBA was assessed in 79 adults with CD (71 on a GFD with negative CD serology and 8 consuming gluten; 75 HLA-DQ2.5) and 92 without CD (34 on GFD with self-reported non-celiac gluten sensitivity, NCGS, and 58 healthy controls consuming gluten; 35 HLA-DQ2.5). Fresh blood was incubated for 24 hours with gluten peptides and IL-2 assessed (MesoScale Discovery). Serum IL-2 levels at 0 and 4 h after single-bolus 10 g gluten challenge and tetramer frequency was also assessed in the treated CD and NCGS cohorts.</p><p><b><i>Results:</i></b> IL-2 WBA showed high accuracy to detect CD: sensitivity 85% (67/79), specificity 97% (89/92), AUC=0.93. Sensitivity increased to 88% (67/76) when CD patients with the atypical HLA-DQ8 genotype were excluded (AUC 0.95). The IL-2 WBA response correlates with both gluten-induced serum IL-2 (n=50, r=0.65, p < 0.0001) and the frequency of gluten-tetramer+ gut-homing T cells per million CD4+ T cells (n = 10, r=0.9, p < 0.0001). The IL-2 WBA was positive at tetramer frequencies as low as 1 per million CD4+ T cells. Higher baseline IL-2 WBA was associated with vomiting after gluten challenge.</p><p><b><i>Conclusion:</i></b> The IL-2 WBA demonstrates exceptional sensitivity equivalent to detecting a single gluten-specific T cell in a 4 ml blood vial. It is a simple, tube-based assay requiring < 10 mL whole blood and can predict the severity of gluten-induced symptoms. It shows high diagnostic accuracy for CD with the important advantage of detecting CD in patients following a GFD with negative transglutaminase-IgA. Ongoing refinements aim to improve diagnostic sensitivity. The IL-2 WBA has the potential to revolutionise CD diagnosis and overcome the current limitations of CD serology and histology.</p><p><b>159</b></p><p><b>Thionamide-induced neutropenic enterocolitis in a patient in thyroid storm: a rare clinical entity</b></p><p><b>Ibrahim Mian</b>, Aisling Hand and Katherine Griffin</p><p><i>Gold Coast University Hospital, Gold Coast, Australia</i></p><p><b><i>Introduction:</i></b> Neutropenic enterocolitis (NEC) is a severe, life-threatening condition characterized by inflammatory necrosis of the bowel wall, seen in neutropenic patients. Bowel wall inflammation in NEC progresses to ulceration and necrosis, which if not addressed promptly can cause bowel perforation. There have been no reported cases of NEC secondary to thionamide use and for a patient in thyroid storm.</p><p><b><i>Case Report:</i></b> A young woman in her thirties with a recent diagnosis of Graves' disease for which she took methimazole, presented to hospital with fevers, abdominal pain, and diarrhoea after recently returning from Thailand. She was febrile to 38.8°C, tachycardic to 140 bpm, and a blood pressure of 105/56 mmHg. Her exam was remarkable for exophthalmos, a large palpable goitre, and swollen exudative tonsils. She had an absolute neutrophil count of 0.00x 10^9/L (2.5-7x 10^9/L), free T4 63.5 pmol/L (10-20 pmol/L), free T3 28.9 pmol/L (2.8-6.8 pmol/L), and a TSH 0.00 mU/L (0.50-4.00 mU/L). Her presentation was in keeping with agranulocytosis secondary to thionamide use for her Graves’ disease complicated by thyroid storm from a bacterial tonsillitis. Her management was complicated as she was unable to use alternative antithyroid drugs for her thyroid storm. As such, she was managed with intravenous fluids, broad spectrum antibiotics, and granulocyte-colony stimulating factor (G-CSF) for her bacterial tonsillitis and neutropenic sepsis. Lugol’s iodine, glucocorticoids, and propranolol were used to manage her thyroid storm, whilst awaiting a thyroidectomy. On day 10 of her admission, she developed severe abdominal pain with associated haematochezia. She examined as peritonitic. Her CT abdominal imaging demonstrated features consistent with NEC. She was abruptly taken to theatre for an emergency laparotomy. Histology from her diseased bowel remained consistent with NEC. By day 31 of her admission, she underwent a total thyroidectomy without complications and was discharged in the following days.</p><p><b><i>Conclusion:</i></b> This case highlights the clinical challenges in managing a patient with NE in concomitant thyroid storm and neutropenic sepsis from thionamide-induced agranulocytosis. The patient's management was complicated by overlapping symptoms of thyrotoxicosis and NEC, underscoring the need for high clinical suspicion and early imaging in febrile neutropenic patients with gastrointestinal symptoms. Lugol's iodine served as a critical bridging therapy in managing thyrotoxicosis until surgical intervention was feasible. The case also raises considerations for the selective use of G-CSF in high-risk patients with NEC. Ultimately, thionamide-induced NEC, though rare, requires prompt recognition and management due to its high mortality risk.</p><p><b>172</b></p><p><b>Nasogastric delivery of fecal microbiota transplantation for treatment of <i>Clostridioides difficile</i> infection: a case report</b></p><p><b>Amitjeet Singh</b>, Edward Young and Arvind Rajagopalan</p><p><i>Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> <i>Clostridioides difficile</i> is a significant healthcare challenge due to its association with antibiotic-associated diarrhea, increasing incidence, and the emergence of highly virulent strains. Traditional treatments like metronidazole and oral vancomycin are becoming less effective due to rising resistance, while faecal microbiota transplantation (FMT) has shown promise, particularly via direct caecal delivery. This case report describes the successful use of nasogastric FMT to avoid colectomy in a patient with severe <i>C. difficile</i> infection (CDI) complicated by toxic megacolon.</p><p><b><i>Case Report:</i></b> A 46-year-old female with cirrhosis presented to the emergency department with haematemesis and haemodynamic instability. An emergency endoscopy demonstrated large oesophageal varices with high-risk stigmata, managed with band ligation. She was commenced on intravenous pantoprazole and ceftriaxone according to routine variceal bleeding protocols. Unfortunately, one week into her admission (after completing 5 days of ceftriaxone) she developed abdominal pain, diarrhoea and fevers to 38.1°C. Laboratory investigations showed a white cell count of 19x10<sup>9</sup>/L, C-reactive protein of 143mg/L and albumin of 21 g/dL. Computed tomography (CT) scan of her abdomen showed colitis involving the ascending colon and splenic flexure but no colonic dilation. A stool PCR was positive for <i>C. difficile</i> toxin. Treatment was initiated with oral vancomycin 250mg four times daily and intravenous metronidazole 500mg three times daily. Despite escalation of vancomycin to 500mg four times daily, the patient symptoms worsened, with increasing abdominal pain, diarrhea, and new onset hepatic encephalopathy. Repeat abdominal X-rays demonstrated significant colonic dilation, with a transverse colon diameter of up to 12cm. The decision was made to proceed with FMT, however colonoscopic delivery was not safe due to the toxic megacolon. Push enteroscopy was also deemed to be high-risk given the recent oesophageal banding, decompensated cirrhosis with ascites and encephalopathy, and ileus with resultant risk of aspiration. We administered the first 50ml syringe of FMT solution via enema without complication. Four hours after the enema, three syringes of FMT solution were administered at two-hour intervals via the nasogastric tube, with concurrent intravenous metoclopramide 10mg three times a day as an anti-emetic and prokinetic. The syringes were each delivered slowly over 10 minutes, ensuring no nausea or vomiting occurred. The following day the patient had a significant improvement in abdominal pain, diarrhea, and encephalopathy. A repeat abdominal X-ray showed the resolution of toxic megacolon with a normal amount of gas throughout the large bowel. There was significant improvement in her C-reactive protein and white cell count. The patient was discharged home with 14-days of oral vancomycin.</p><p><b><i>Discussion:</i></b> In this case, we have demonstrated successful salvage of a <i>C. difficile</i>-related toxic megacolon following administration of FMT via a nasogastric tube, where push enteroscopy was relatively contraindicated. Comparative studies on the efficacy of fecal transplantation based on the administration method have yielded mixed results. A systematic review found that the success rates of fecal transplantation were lower when administered via enteroscopy or nasoenteric tube (88%) compared to colonoscopy and enema (95%). Another review analysing colonoscopic versus nasogastric methods across 12 studies revealed a higher success rate for the colonoscopic approach (93%) over nasogastric (85%), though the difference was not statistically significant. Nevertheless, in severe cases there are often contraindications to traditional methods for FMT delivery, as was the case in our patient. There are few published articles on the use of FMT for patients with toxic megacolon. Evidence has shown that FMT is effective in patients with recurrent CDI while evidence and experience in the context of severe and fulminant <i>C. difficile</i> continues to grow. To our knowledge this is the first reported case where nasogastric delivery of FMT solution has led to resolution of a <i>C. difficile</i>-related toxic megacolon. There are inherent risks of aspiration with this method, however a colectomy would have resulted in extremely high morbidity and mortality given the patient’s decompensated cirrhosis. This highlights the importance of the awareness of various routes of FMT delivery in order to tailor delivery to specific patient circumstances.</p><p><b>173</b></p><p><b>Endoscopic submucosal dissection of complicated giant gastrointestinal lipomas - a tertiary care center experience</b></p><p><b>Wei Ling Teh</b>, Sherman Picardo, Niroshan Muwanwella and Marcus Chin</p><p><i>Royal Perth Hospital, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal (GI) lipomas are benign subepithelial lesions (SELs) composed of mature adipose tissue. While often asymptomatic, GI lipomas can cause complications such as bleeding, luminal obstruction, or intussusception, necessitating intervention. Currently, there is no standardized approach for the treatment of symptomatic GI lipomas. Most cases reported in the literature were resected surgically. Recently, endoscopic resection techniques have evolved, with endoscopic submucosal dissection (ESD) emerging as a promising approach for the management of GI lipomas. We aim to analyse the success and safety of ESD in resecting GI lipomas.</p><p><b><i>Methods:</i></b> This was a retrospective, observational case series study. We reviewed gastrointestinal lipomas resected by ESD at our hospital between March 2017 and October 2023<b>.</b> All upper ESDs were performed using either EG760Z (Fujifilm, Tokyo, Japan) or GIF-HQ190 (Olympus Medical, Tokyo, Japan) Gastroscope. Colonic ESD was performed with EC760ZVL Colonoscope (Fujifilm, Tokyo, Japan). Utilizing either Dual Knife J and/or IT-2 knife (Olympus Medical, Tokyo, Japan), we directly dissected the submucosal connective tissue beneath the lesion, achieving en-bloc resection.</p><p><b><i>Results:</i></b> Here, we present seven instances wherein giant GI lipomas were effectively excised using ESD. All patients included in our study exhibited sizable GI lipomas and were experiencing associated symptoms. The mean age of patients was 59 years (41-68). The average lipoma size was 79 mm (50-100mm). Histopathology examination confirmed the diagnosis of lipomas in six cases and one case of angiolipoma. All patients were followed up either in clinic to ensure resolution of symptoms or with surveillance endoscopies. We demonstrated the successful removal of three bleeding and three obstructive large GI lipomas, all without complications, including bleeding and perforation.</p><p><b>175</b></p><p><b>Effectiveness and long-term durability of cricopharyngeal peroral endoscopic myotomy for treating dysphagia with upper oesophageal sphincter dysfunction: a mixed aetiology study</b></p><p><b>Alvin Cheah</b><sup>1,2</sup>, Michal Szczesniak<sup>1,2</sup>, Dheeraj Pandey<sup>1,2</sup>, Julia Maclean<sup>1,2</sup> and Peter Wu<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, St George Hospital, Sydney, Australia;</i> <sup>2</sup><i>St George and Sutherland Clinical School, University of New South Wales, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Encouraging preliminary data shows that cricopharyngeal peroral endoscopic myotomy (C-POEM) improves oropharyngeal dysphagia (OPD) in Parkinson’s disease (PD) patients with upper oesophageal sphincter (UOS) dysfunction on pharyngeal high-resolution impedance manometry (PHRIM). UOS dysfunction can manifest in a spectrum of neuromyogenic disorders, including PD, cerebrovascular accidents (CVA), inflammatory myopathies and post head and neck cancer (HNC) treatment. The aim of this study is to assess the efficacy and the long-term durability of C-POEM as a treatment for dysphagia with mixed aetiologies with proven underlying UOS dysfunction.</p><p><b><i>Methods:</i></b> Consecutive patients with OPD underwent PHRIM and were offered C-POEM if failed UOS relaxation was observed. Analysis was carried out on Swallow Gateway and failed UOS relaxation was defined as increased integrated relaxation pressure (IRP<sub>0.25</sub>) above upper limit of normal for a liquid bolus (either thin IDDSI 0 or thick IDDSI 4) of highest volume tolerated without piecemeal swallowing. Sydney Swallow Questionnaire (SSQ) was obtained at baseline, 1 month and yearly up to 3 years after C-POEM to measure symptoms of swallow dysfunction. The mean change in total SSQ scores from pre-treatment to 1 month post were assessed using paired t-test. Long term trend in total SSQ score post-treatment was assessed using repeated measures mixed model.</p><p><b><i>Results:</i></b> Between September 2020 and Sept 2023 consecutive patients (n = 15) underwent C-POEM for OPD and UOS dysfunction demonstrated on PHRIM. Patients with OPD were of various aetiologies such as CVA (n=4), inflammatory myopathies (n=4), Parkinson’s disease (n=2) and HNC (n=5). In one HNC patient included in the analysis, C-POEM could not be completed due to extensive submucosal fibrosis. There was an improvement in mean SSQ scores 1-month post C-POEM (714, 95%CI [542-885]) from baseline (1133, 95% CI [951-1314]). The mean change was statistically significant (∆ 419, 95% CI [253-585], p=0.0001). We observed no deterioration in swallow function on SSQ post C-POEM on repeated measures mixed model. Mean follow-up period was 8 months and the SSQ score remained stable with minimal non-significant change of -0.69 per month, 95% CI [-9.02-2.29] (p=0.87). There were no complications identified in the study group.</p><p><b><i>Conclusion:</i></b> C-POEM is an effective and safe novel endoscopic technique that improves dysphagia symptoms in patients with neuromyogenic disorders and HNC by targeting spastic UOS, thus improving bolus flow during swallowing. Importantly, dysphagia symptoms remained stable post C-POEM. However, considering the small sample size, larger and longer prospective trials looking at the merits of C-POEM is warranted.</p><p><b>176</b></p><p><b>Evaluating hypopharyngeal post-swallow and contractile admittance as non-radiological markers of pharyngeal residue and clearance in dysphagia</b></p><p><b>Alvin Cheah</b><sup>1,2</sup>, Dheeraj Pandey<sup>1,2</sup>, Julia Maclean<sup>1,2</sup>, Peter Wu<sup>1,2</sup> and Michal Szczesniak<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, St George Hospital, Sydney, Australia;</i> <sup>2</sup><i>St George and Sutherland Clinical School, University of New South Wales, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Post-swallow residue and presence of pharyngeal space during pharyngeal constriction are swallowing impairment signs and pose aspiration risk. Analysis of admittance during pharyngeal high-resolution impedance manometry (PHRIM) offers a potential non-radiological marker of pharyngeal residue post-swallow and during pharyngeal contraction, providing quantitative interpretation at bedside. Additionally, absence of radiation exposure makes it appropriate for follow up studies with repeat progress measurements. The aim of this study was to compare estimates obtained with admittance against radiographic equivalents.</p><p><b><i>Methods:</i></b> We identified 98 patients with oropharyngeal dysphagia of various aetiologies who underwent concurrent videofluoroscopy and PHRIM. Using SwallowGateway (5ml liquid (IDDSI 0) swallows), hypopharyngeal post-swallow admittance (HpPostAdm) was calculated as mean admittance spanning the hypopharyngeal segment within 0.5s after the stripping wave. Hypopharyngeal contractile admittance (HpContAdm) was calculated as mean admittance during the period of hypopharyngeal contraction. In the same cohort, fluoroscopic videos of 5ml liquid (IDDSI 0) swallows in lateral projection were independently analysed after spatial calibration referenced to radio opaque PHRIM sensors. Areas (cm<sup>2</sup>) of post-swallow reside were calculated for vallecula (VR), pyriform sinuses (PR) and other pharyngeal areas (OR). These were summed to derive total pharyngeal residue (TR). Intraluminal area at maximum pharyngeal constriction (AMPC) was measured in the frame showing maximum obliteration of the space in the pharynx before the pharynx begins to relax. Sydney Swallow Questionnaire (SSQ) was routinely obtained prior to PHRIM assessment to measure baseline swallow dysfunction.</p><p><b><i>Results:</i></b> Patient backgrounds included Parkinson’s disease (12), head and neck cancer (55), inclusion body myositis (8), cerebrovascular accident (2), muscular dystrophy (3), MOGAD (1), multiple sclerosis (1), motor neuron disease (1) and idiopathic (15). Majority were male (70%) and mean SSQ was (588.92 ±SD 409.15). We observed significant correlation between HpPostAdm and residue area observed radiographically post-swallow in the lateral plane. Correlation was highest with PR (Spearman’s ρ=0.64, p<0.0001) followed by TR (ρ=0.59, p<0.0001) and VR (ρ=0.34, p=0.001). Correlation between HpContAdm and AMPC was also significant with ρ=0.341, p=0.0006.</p><p><b>177</b></p><p><b>Beyond metrics: esophageal hypervigilance better predicts esophageal symptom severity compared with pH study and HRM metrics</b></p><p><b>Lyman LIN</b><sup>1</sup>, Tamara Debreceni<sup>1</sup>, Ruby Han<sup>1</sup>, Dhivya Pandiaraja<sup>1</sup>, Melissa Braudigom<sup>1</sup>, Jacinta McMahon<sup>1</sup>, Shahreedhan Shahrani<sup>1</sup>, Santosh Sanagapalli<sup>2</sup> and Chamara Basnayake<sup>1,3</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>St Vincent's Hospital Sydney, Sydney, Australia;</i> <sup>3</sup><i>The University of Melbourne, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> In clinical practice, the results from manometry and pH studies are often insufficient to explain the symptom severity of dysphagia and gastroesophageal reflux disease symptoms (GORD) perceived by patients. Oesophageal hypervigilance is thought to be a contributor to symptom severity of dysphagia and GORD. The 7-item questionnaire Oesophageal Hypervigilance and Anxiety Scale (EHAS-7) was developed to assess oesophageal hypervigilance. Our study aims to investigate whether manometry/pH study metrics or EHAS-7 have a greater correlation with the symptom severity of GORD and dysphagia. We hypothesise oesophageal hypervigilance can better predict symptom severity for symptoms than physiological study metrics.</p><p><b><i>Methods:</i></b> Consecutive patients attending for high resolution manometry (HRM) with or without a 24-hour pH study at a tertiary referral centre, from March 2022 to October 2023, were prospectively included. Patients completed the following questionnaires: EHAS-7, Brief Esophageal Dysphagia Questionnaire (BEDQ) and Gastroesophageal Reflux Disease Questionnaire (GERDQ). Pearson’s correlation was used to determine the interrelationships between questionnaire results, HRM and pH study metrics.</p><p><b><i>Results:</i></b> 286 patients were included with 170 completing pH studies. The median age was 55 (IQR 42 – 66) and 181 (63.3%) were female. Chicago 4 diagnoses included 189 (66.1%) patients with a normal study, 40 (14.0%) with achalasia, 15 (5.2%) esophagogastric junction outflow obstruction (EGJOO), 25 (8.74%) ineffective oesophageal motility (IEM), 8 (2.80%) absent contractility, 3 (1.05%) diffuse oesophageal spasm (DES) and 6 (2.10%) Jackhammer oesophagus. In the whole cohort, symptom severity (BEDQ) was significantly correlated with EHAS-7 (r = 0.362, p < 0.001) and several HRM metrics: including median integrated relaxation pressure (IRP) for supine 5ml swallows (r = 0.320, p < 0.001), median IRP for upright 5ml swallows (r = 0.358, p < 0.001) and median IRP for 2cm bread swallows (r = 0.360, p = 0.001). Among patients with normal manometry findings, BEDQ had a significant correlation with EHAS-7 (r = 0.245, p = 0.002) and median DCI for upright swallows (r = 0.230, p = 0.046). In patients with achalasia, BEDQ was significantly associated with EHAS-7 (r = 0.414, p = 0.017) but not HRM metrics. For those with IEM, BEDQ was correlated with EHAS-7 (r = 0.594, p < 0.002) and median DCI for supine swallows (r = 0.542, p = 0.025). Regarding patients with absent contractility, symptoms were only correlated with EHAS-7 (r = 0.823, p = 0.023). BEDQ was not associated with either EHAS-7 or any manometry metrics for patients with DES or Jackhammer oesophagus. For patients presenting with GERD symptoms including heartburn and regurgitation, symptoms (GERDQ) were significantly associated with EHAS-7 (r = 0.148, p = 0.028) but not pH metrics. Age, sex, and BMI did not correlate with symptom severity for dysphagia or GORD.</p><p><b><i>Conclusion:</i></b> In this cohort, we observed a stronger correlation between dysphagia and GORD symptom severity with Oesophageal hypervigilance scores compared to physiological metrics. These findings suggest a potential utility of Oesophageal hypervigilance as a predictor for patient-reported Oesophageal symptom severity. Subsequent studies should be conducted to investigate whether treating oesophageal hypervigilance improves symptom severity.</p><p><b>211</b></p><p><b>Evaluating the use of faecal occult blood tests for bowel cancer screening in persons with established spinal cord injury aged 50 – 74 years</b></p><p><b>Michael Yulong Wu</b><sup>1,2,3</sup>, Carmen Tung<sup>1</sup>, Mccawley Clark-Dickson<sup>4</sup>, Samuel Arthurs<sup>1</sup> and Ian Norton<sup>1,2</sup></p><p><sup>1</sup><i>Royal North Shore Hospital, Gold Coast, Australia;</i> <sup>2</sup><i>Northern Clinical School, University of Sydney, Gold Coast, Australia;</i> <sup>3</sup><i>Faculty of Health Science and Medicine, Bond University, Gold Coast, Australia;</i> <sup>4</sup><i>Sydney Adventist Hospital, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> In 2006 the Australian Government established the National Bowel Cancer Screening Program (NBCSP) with an aim to reduce the morbidity and mortality of colorectal cancer by early detection of malignancy. The program involves sending a biennial faecal occult blood test (FOBT) kit to all Australians aged 50 – 74 years old and those who test positive are recommended to proceed with colonoscopy if appropriate. The role and accuracy of FOBT in the spinal cord injury (SCI) population is yet to be established in the literature. We have postulated that the frequent use of rectal enemas, digital stimulation, chronic constipation and associated anorectal disorders in SCI patients can lead to colonic microtrauma with higher rates of positive FOBT. Therefore, the purpose of this study is to investigate the proportion of positive FOBT among patients with established SCI compared to the general population as measured by the NBCSP. We hypothesised that patients with SCI have a higher false positive rate.</p><p><b><i>Methods:</i></b> A prospective study was conducted at a tertiary hospital with one of the two inpatient spinal injury units in New South Wales. All established SCI patients aged 50 – 74 years old were included. Patients outside of the age criteria, those with active per-rectal bleeding, haemorrhoids, per-vaginal bleeding, hematuria, SCI within 12 months, colonoscopy within 4 years, or had already completed FOBT as part of the NBCSP were excluded. Recruited patients had two separate faecal samples sent for FOBT. Those with at least one positive FOBT were offered either an inpatient colonoscopy or outpatient follow-up at their local hospital.</p><p><b><i>Results:</i></b> A total of 18 patients were included in the study with a mean age of 61.1 years. In total 44.4% of patients tested positive on at least one FOBT. Of those who tested positive, two patients agreed to proceed with colonoscopy. In both cases the colonoscopy was normal. The majority of patients declined follow-up colonoscopy due to perceived difficulty with bowel preparation and procedural risks. Most patients reported rectal enema use, digital simulation and manual evacuation as part of their routine bowel care (Table 1). Out of those who used enemas, digital stimulation or manual evacuation, 41.1% returned a positive FOBT.</p><p><b><i>Conclusion:</i></b> To date, there is a lack of prospective studies that have investigated the accuracy of FOBT in patients with SCI. In this study, patients with SCI have higher rates of positive FOBT compared to the general Australian population at 6.2%. Follow-up colonoscopy rates were poor and patient compliance can be improved by more streamlined inpatient bowel preparation protocols. Higher rates of positive FOBT may be attributed to colonic and anorectal microtrauma. Our results suggests that the FOBT may not be an accurate screening tool in this population and a primary screening colonoscopy strategy may be more appropriate.</p><p><b>212</b></p><p><b>Upadacitinib real-world efficacy and safety in treatment of inflammatory bowel disease: an Australian single-centre experience</b></p><p><b>Gordon Chen</b>, <b>Vikram Rao</b>, Sheng Wei Lo, Elaine Koh, Abha Kaul and Richard La Nauze</p><p><i>Peninsula Health, Frankston, Australia</i></p><p><b><i>Background and Aim:</i></b> Upadacitinib, a recently approved small molecule inhibitor of Janus kinase 1 (JAK1), has been subject to much excitement as a new effective therapy in the management of moderate to severe ulcerative colitis (UC) and moderate to severe Crohn’s disease (CD). There has been rapidly increasing evidence of efficacy in both forms of inflammatory bowel disease (IBD) in literature but still a relative paucity of safety data. This retrospective, single centre, observational study aimed to assess the clinical efficacy and audit the safety of this novel medication in the biologic-experienced IBD cohort.</p><p><b><i>Methods:</i></b> Retrospective review was undertaken for all IBD patients prescribed Upadacitinib between January 2023 and May 2024 at a single-centre IBD service in Melbourne, Australia. Patients that have had at least 6 months of follow-up were included. Clinical and biochemical parameters were assessed at baseline, end of induction and at 6-months. Datapoints included previous exposure to biologics/JAK inhibitors, bowel motion frequency, clinical score indices (SCCAI/HBI), C-reactive protein (CRP), faecal calprotectin (FCP), and any adverse events.</p><p><b><i>Results:</i></b> Four patients were identified for inclusion, three patients with UC and one patient with CD, with median follow-up time of 41.1 weeks (IQR 35.8-50.9). All were anti-tumour necrosis factor (TNF)-experienced. 75% (3/4) achieved the primary outcome of clinical remission at 6-months, all achieved the secondary outcomes of drug persistence at 6-months, corticosteroid-free remission and normalization of biomarkers (CRP, FCP) by end of induction, and maintained this through to 6-months. Adverse events occurred in 75% (3/4), 50% (2/4) of which were serious (requiring hospitalisation) within the 6-month follow up period. Patient 2 (Table 1), a 25-year-old female vaccinated with no comorbidities, was hospitalised for moderate-severity COVID. Patient 4 (Table 1), a 41 year-old female without significant comorbidities, was hospitalised for complicated cystourethritis. Two patients developed acne.</p><p><b><i>Conclusion:</i></b> This real-world data in Australia supports the efficacy of upadacitinib as another therapeutic option in the biologic-experienced IBD cohort. It is noted that the serious adverse event rate is higher than previously reported in safety trials which highlights the importance of ongoing real-world monitoring of this medication.</p><p><b>230</b></p><p><b>Machine learning with natural language processing to identify cases of Barrett’s oesophagus from electronic endoscopy reports</b></p><p><b>Madoka Inoue</b><sup>1,3</sup>, Hideo Tohira<sup>2,4,5</sup>, James Chen<sup>3</sup>, Shiv Meka<sup>6</sup>, Spiro Raftopoulos<sup>1,5,7</sup> and Krish Ragunath<sup>1,3</sup></p><p><sup>1</sup><i>Curtin Medical School, Curtin University, Perth, Australia;</i> <sup>2</sup><i>Curtin School of Nursing, Curtin University, Perth, Australia;</i> <sup>3</sup><i>Department of Gastroenterology, Royal Perth Hospital, Perth, Australia;</i> <sup>4</sup><i>Department of Emergency Medicine, Chibanishi General Hospital, Japan;</i> <sup>5</sup><i>UWA Medical School, University of Western Australia, Perth, Australia;</i> <sup>6</sup><i>Health in a Virtual Environment, East Metropolitan Health Service, Perth, Australia;</i> <sup>7</sup><i>Department of Gastroenterology, Sir Charles Gairdner Hospital, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Accurately identifying Barrett's oesophagus (BO) cases from electronic endoscopy reports is crucial for epidemiological studies but is often complicated by limitations in diagnostic coding systems and reporting structures. Few studies have applied natural language processing (NLP), a machine learning application for text classification, for this purpose. Thus, this study aimed to 1) develop machine learning models to identify BO cases using NLP to generate features from free-text descriptions in electronic endoscopy reports, and 2) evaluate the predictive performance of these models.</p><p><b><i>Methods:</i></b> This retrospective observational study utilised data from electronic endoscopy reports of patients (age ≥18 years) who underwent upper gastrointestinal endoscopy between January 1999 and December 2023, at four teaching hospitals in Perth, Western Australia. Endoscopists usually complete these reports post-procedure, including two free-textual sections: endoscopic findings (Findings) and a summary (Conclusion). BO cases were manually identified from a 20% random sample of these reports through free-text review. Three corpora were then created: 1) \\\"Findings\\\" only, 2) \\\"Conclusion\\\" only, and 3) \\\"Findings & Conclusion\\\". The sampled reports were divided into 70% for training and 30% for testing. NLP was used to compute the term frequency-inverse document frequency of each word, ranking their relevance. Three machine learning models—Random Forest (RF), Support Vector Machine (SVM), and XGBoost (XGB)—were developed based on each corpus. Optimal parameters were determined through 5-fold cross-validation, and model performance was evaluated using F1-measure (harmonic mean of recall and precision), recall (sensitivity), and precision (positive predictive value).</p><p><b><i>Results:</i></b> Among 186,896 electronic endoscopy reports, 37,396 were randomly sampled. Of the sampled reports, 42 and 90 were missing in the “Findings” and “Conclusion” sections, respectively. These reports were excluded when deriving models. A total of 26,177 reports were used for training and 11,219 for testing. We found that XGB performed best with an F1measure of 0.940, recall of 0.940, and precision of 0.939, derived using the combined corpus \\\"Findings & Conclusion\\\" as features. This was followed by RF with the combined corpus, achieving an F1-measure of 0.937, recall of 0.947, and precision of 0.928. SVM with the combined corpus attained an F1-measure of 0.922, recall of 0.895, and precision of 0.950.</p><p><b><i>Conclusion:</i></b> The machine learning model, using free-text findings and a summary in the endoscopy report as inputs, could identify BO cases with high recall and precision. Further improvement might involve including additional information like patient demographics and leveraging large language models for word embedding.</p><p>\\n \\n </p><p><b>238</b></p><p><b>Increased risk of future advanced neoplasia in individuals that have synchronous adenomas and clinically significant serrated polyps</b></p><p><b>Geraldine Laven-law</b><sup>1</sup>, Erin Symonds<sup>1,2</sup>, Kalindra Simpson<sup>1,2</sup>, Michelle Coats<sup>2</sup>, Mahinda De Silva<sup>2</sup>, Paul Hollington<sup>3</sup>, Charles Cock<sup>1,2</sup> and Molla M Wassie<sup>1</sup></p><p><sup>1</sup><i>Flinders University, College of Medicine and Public Health, Flinders Health and Medical Research Institute, Adelaide, Australia;</i> <sup>2</sup><i>Department of Gastroenterology and Hepatology, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia;</i> <sup>3</sup><i>Department of Colorectal Surgery, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Colorectal cancer (CRC) commonly develops from pre-cancerous neoplasia through the adenoma-carcinoma and serrated pathways. Individuals with prior history of adenoma and/or clinically significant serrated polyp (CSSP) are considered at above-average risk for CRC and undergo colonoscopy surveillance at intervals recommended by national guidelines. While individuals with synchronous adenoma and CSSP are recommended the same surveillance colonoscopy interval as those with only CSSP, there is limited evidence to support this recommendation. This study determined whether synchronous adenomas and CSSP increase the risk of future advanced neoplasia compared to no neoplasia, prior adenoma, or prior CSSP.</p><p><b><i>Methods:</i></b> This was a retrospective analysis of data from patients enrolled within a South Australian CRC surveillance program, and undergoing colonoscopies between 2010 – 2023 inclusive. Included patients were those that had a finding of no neoplasia or pre-cancerous neoplasia (adenoma and/or CSSP), who received a recommended surveillance interval and underwent another complete colonoscopy. Patients with inflammatory bowel disease, organ transplants, or CRC syndromes were excluded. Demographics and colonoscopy findings were extracted from clinical databases. Advanced neoplasia was defined as adenocarcinoma, advanced adenoma (adenoma ≥ 10 mm, high-grade dysplasia, and/or villous change), and/or advanced CSSP (sessile serrated lesions or hyperplastic polyps ≥ 10 mm, with dysplasia, and/or any traditional serrated adenoma). Multivariable Cox regression determined the effect of prior neoplasia on risk for developing future advanced neoplasia, controlling for age, sex, and colonoscopy interval. P < 0.05 was considered statistically significant.</p><p><b><i>Results:</i></b> A total of 11,134 colonoscopy pairs were included; 3,680 (33%) patients had no neoplasia, 5,884 (53%) had adenoma, 773 (7%) had CSSP, and 797 (7%) had synchronous adenoma and CSSP resected at the first colonoscopy of the pair. Patients were aged a median 65 (interquartile range 57 – 72) years, and 53% were male. Advanced neoplasia was found in 12% (1,336/11,134) of subsequent colonoscopies, but in 26% (140/536) of those with initial synchronous adenoma and CSSP when at least one lesion was advanced. Patients with synchronous advanced adenoma and non-advanced CSSP developed advanced neoplasia earlier than their advanced adenoma-only and non-advanced CSSP-only counterparts (Figure, p < 0.05).</p><p><b>239</b></p><p><b>Small bowel metastatic melanoma – a case report</b></p><p><b>Keith Brick</b> and Montri Gururatsakul</p><p><i>Queensland Health, Cairns, Australia</i></p><p><b><i>Introduction:</i></b> Melanoma is known to metastasize widely. The most frequent sites for metastatic melanoma are lymph nodes, lungs, liver, brain, bone and adrenal glands (1), but rarely gastrointestinal tract. The most common site of melanoma metastases to the gastrointestinal (GI) tract is the small intestine (1, 2). This case study reports a patient with small bowel metastatic melanoma who presented with recurrent iron deficiency anaemia.</p><p><b><i>Case Report:</i></b> A 73 year old male presented with iron deficiency anaemia. He initially had upper endoscopy and colonoscopy which were unremarkable, and subsequently had video capsule endoscopy which found a non bleeding ulcerated mass lesion at the proximal jejunum. He has a background of previous cholecystectomy, diverticular disease, multiple SCC and BCCs excisions, and in 2021 he had a melanoma in situ excised from his upper lip with at least 3 mm margins. A CT Enteroclysis identified a short segment (49mm) of abnormal mural thickening of the small bowel with a nodular appearance with some dilatation of the proximal bowel loop (figure 1). The lesion was not seen on a push enteroscopy. He underwent antegrade double balloon enteroscopy and a suspicious medium-sized ulcerated mass with no bleeding was found in the mid-jejunum, which was biopsied and tattooed (figure 2). The histopathology was non diagnostic. His case was discussed at both at radiology and histology MDT, and referred for surgical resection. He underwent successful robotic small bowel resection which has confirmed a diagnosis of metastatic melanoma. Subsequent somatic mutation testing for BRAF, KIT and NRAS were negative. He is now being considered for immunotherapy.</p><p><b>References</b></p><p>\\n 1. <span>Liang, KV</span>, <span>Sanderson, SO</span>, <span>Nowakowski, GS</span>, <span>Arora, AS</span>. <span>Metastatic Malignant Melanoma of the Gastrointestinal Tract</span>. <i>Mayo Clinic Proceedings.</i> <span>2006</span> <span>81</span>(<span>4</span>) <span>511</span>-<span>16</span>. https://doi.org/10.4065/81.4.511</p><p>\\n 2. <span>Lens, M</span>, <span>Bataille, V</span>, <span>Krivokapic, Z</span>. <span>Melanoma of the small intestine</span>. <i>Lancet Oncol.</i> <span>2009</span>; <span>10</span> (<span>5</span>): <span>516</span>–<span>521</span>. doi: https://doi.org/10.1016/S1470-2045(09)70036-1</p><p><b>240</b></p><p><b>A large choledochoduodenal fistula – a case report</b></p><p><b>Keith Brick</b>, Montri Gururatsakul and Shihaz Hussain</p><p><i>Queensland Health, Cairns, Australia</i></p><p><i><b>Introduction</b>:</i> A choledochoduodenal fistula is an abnormal communication between the common bile duct & the duodenum. It is often secondary to PUD, cholelithiasis, malignancy or iatrogenic (1). Presenting symptoms of cholangitis (fever, jaundice & abdominal pain) are common. This is a case report of an asymptomatic large choledochoduodenal fistula.</p><p><i><b>Case Report</b>:</i> A 65 year old female presented to hospital with hepatic encephalopathy & haematemesis. She has a background of Child-Pugh B cirrhosis secondary to Hepatitis C & alcohol on regular variceal screening, recently diagnosed metastatic rectal adenocarcinoma for palliative treatment, previous laparotomy for cholecystectomy & H. pylori infection. Of relevance she did not have a history of peptic ulcer disease (PUD), no recent biliary tract stones & was asymptomatic with no signs of cholangitis.</p><p>An upper endoscopy for bleeding was performed & identified a large 11mm choledochoduodenal fistula in the first part of the duodenum (fig 1), confirmed by bile draining through the fistula. The major papilla appeared normal without evidence of previous sphincterotomy. Previous staging CT abdomen for rectal cancer showed pneumobilia although no fistula apparent. Blood tests at presentation revealed a raised total bilirubin of 43. Liver enzymes ALP 87U/L, GGT 15U/L, ALT 24U/L & mildly raised AST 42U/L consistent with known decompensated cirrhosis. A cholestatic picture was not expected given the large size of the choledochoduodenal fistula. Due to her co-morbidities, dedicated imaging was not undertaken to further investigate, however a CT abdomen for a separate indication did identify the fistula (fig 2). Four previous surveillance UGIEs reported duodenal diverticulum, however no fistula documented. Her metastatic malignancy was diagnosed 6 weeks prior to the UGIE that identified the fistula.</p><p><b>Reference</b></p><p>\\n 1. <span>Wu, MB</span>, <span>Zhang, WF</span>, <span>Zhang, YL</span>, <span>Mu, D</span>, <span>Gong, JP</span>. <span>Choledochoduodenal fistula in Mainland China: a review of epidemiology, etiology, diagnosis and management</span>. <i>Ann Surg Treat Res.</i> <span>2015 Nov</span>; <span>89</span> (<span>5</span>) <span>240</span>-<span>6</span>. https://doi.org/10.4174/astr.2015.89.5.240</p><p><b>245</b></p><p><b>An unusual cause of dysphagia</b></p><p><b>Eliza Flanagan</b><sup>1,2</sup>, Carl Cosgrave<sup>1,2</sup>, Irene Lu<sup>1,2</sup> and Alvin Ting<sup>1,2</sup></p><p><sup>1</sup><i>Barwon Health, , Australia;</i> <sup>2</sup><i>Monash University, Australia</i></p><p><b><i>Introduction:</i></b> The most common causes of dysphagia include intrinsic oesophageal pathology, such as motor disorders and obstructive lesions. Extrinsic conditions are rarer and usually occur secondary to mediastinal masses or vascular compression. Mediastinal masses comprise a wide variety of benign and malignant lesions and are typically identified incidentally or due to investigations performed for symptoms arising from mass effect. The differential diagnoses for mediastinal masses include thymoma, neurogenic tumours, lymphomas, cysts and germ cell tumours. Symptoms secondary to mass effect may include dyspnoea, cough, chest discomfort, dysphagia, or neurologic issues such as Horner’s syndrome. Imaging via CT chest provides detailed information regarding location and assists with differential diagnosis. Patient management relies on tissue diagnosis obtained via biopsy or during planned resection. Inflammatory myofibroblastic tumours (IMTs) are a rare intermediate-grade neoplasm, considered to be a subtype of sarcoma. They have high recurrence rates following resection and low metastatic potential [1]. They are most often found in children, and occur predominantly in the abdomen (up to 75%), lung, pelvis and retroperitoneum; however, any site can be involved [1, 2]. Most cases have a benign course and depending on the location, are often asymptomatic. Diagnosis is made by histologic findings characterized by spindle cell proliferation and an inflammatory infiltrate [1]. The anaplastic lymphoma kinase (ALK) gene has a critical role in the biology of many IMTs, and approximately 50% of IMTs contain a translocation in the ALK gene, resulting in tyrosine kinase activation. Complete surgical resection is the standard of care [1, 2] and if recurrence occurs, re-resection would be offered plus consideration of chemotherapy [3].</p><p><b><i>Case Report:</i></b> A 41-year-old lady with no significant past medical history was referred to hospital with chest discomfort and mildly elevated troponin 42ng/L [0-40]. She described a history of four months of progressive dysphagia to both solids and liquids, with worsening dyspnoea and orthopnea. Her electrocardiogram was normal and repeat troponin was stable. A computed-tomography (CT) scan of her chest was performed which demonstrated a large posterior mediastinal mass measuring 60x50x70mm in size, with compression of the oesophagus and trachea. She underwent an endoscopic ultrasound which was unable to pass the extrinsic compression but core lesional biopsies (fine needle biopsy) were able to be taken to expedite diagnosis. She subsequently underwent a thoracotomy and complete resection of the mass, with histopathology confirming an inflammatory myofibroblastic tumour with ALK gene rearrangement. Following tumour resection, her dysphagia resolved; and she is being followed up with regular surveillance CT imaging.</p><p><b>References</b></p><p>\\n 1. <span>Siemion, K.</span>, et al., <span>What do we know about inflammatory myofibroblastic tumors? - A systematic review</span>. <i>Adv Med Sci</i>, <span>2022</span>. <span>67</span>(<span>1</span>): p. <span>129</span>-<span>138</span>.</p><p>\\n 2. <span>Kovach, S.J.</span>, et al., <span>Inflammatory myofibroblastic tumors</span>. <i>J Surg Oncol</i>, <span>2006</span>. <span>94</span>(<span>5</span>): p. <span>385</span>-<span>91</span>.</p><p>\\n 3. <span>Wang, Q.A.</span>, et al., <span>Update of Diagnosis and Targeted Therapy for ALK(+) Inflammation Myofibroblastic Tumor</span>. <i>Curr Treat Options Oncol</i>, <span>2023</span>. <span>24</span>(<span>12</span>): p. <span>1683</span>-<span>1702</span>.</p><p><b>246</b></p><p><b>Prolonged wireless ambulatory reflux testing - technical success and clinical findings</b></p><p><b>Ash Rankine</b> and Emily Stimson and <b>Magnus Halland</b></p><p><i>Newcastle Gastroenterology, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastro-oesophageal reflux disease (GORD) is common, but symptoms overlap with many other upper gastrointestinal conditions and objective evidence of GORD on endoscopy is uncommon. Thus, an objective diagnosis of GORD is often sought with ambulatory 24-hour catheter-based pH test. However, the test is limited by tolerability and false negative diagnoses due to the relatively short duration of monitoring. Endoscopically placed, wireless prolonged pH testing is another alternative. We aimed to determine; (i) Technical success of introducing a wireless pH testing service, (ii) Indications and outcomes of wireless pH testing and (iii) Compare outcomes among patients who underwent both standard 24-hour pH impedance testing AND subsequent prolonged ambulatory wireless testing.</p><p><b><i>Methods:</i></b> Chart review of patients who underwent wireless pH testing at a single gastroenterology practice between April 2022 and April 2024. Descriptive analysis of clinical characteristics and pH variables was performed.</p><p><b><i>Results:</i></b> 40 wireless pH studies were conducted, all were initially technically successful, however two studies had premature dislodgement (<24h). LA Grade B esophagitis was observed in 5 patients. All tests were performed off PPI therapy and gastric pH was confirmed to be <4 in all patients prior to device placement. The mean age was 47.5 years (range 21-74) and 60% were female. The mean duration of pH data collection was 75.2 hours (SD 11.2). The indication for the test was “Reflux “in 78%, “Atypical GORD” in 15% and “globus or vomiting” in 7%. A positive study, defined as at least one 24-hour period with >6.5% esophageal acid exposure (AET), occurred in 18 patients (45%). Graph 1 shows the proportion of abnormal days of acid exposure among all patients. 3 of the 40 patients had completed an ambulatory pH testing prior to the prolonged wire-less test. In one of these 3 patients severe GORD was present on prolonged wireless testing whereas a concordant result was present in 2. There were no anesthetic or significant endoscopic complications. Mild and moderate chest discomfort was reported in 5 patients and 3 patients respectively.</p><p><b>271</b></p><p><b>The prevalence and predictors of oesophago-pharyngeal reflux in lung transplant recipients</b></p><p><b>Alyce Lonsdale</b>, Mary Eid, David Darley, Mark Danta, Nick Olsen and Santosh Sanagapalli</p><p><i>St Vincent's Clinical School, University of New South Wales Medicine, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Lung transplantation is an important therapeutic option for patients with end-stage lung disease, however, outcomes are poorer than other types of solid organ transplantation. While gastro-oesophageal reflux disease has been linked to lung allograft rejection, existing evidence is of poor quality. This study hypothesised that microaspiration of gastric contents via the pharynx into the lungs contributes to lung allograft injury. Accordingly, it aims to (1) identify the incidence of proximal oesophageal reflux events among lung transplant recipients; and (2) assess the effect of sex, age, body mass index (BMI), oesophageal dysmotility, and the type of pretransplant end-stage lung disease as risk factors for oesophago-pharyngeal reflux.</p><p><b><i>Methods:</i></b> This cross-sectional study assessed lung transplant recipients at three to six months post-transplant, who underwent oesophageal multichannel intraluminal manometry and 24-hour pH testing between March and August 2023. Proximal and distal reflux episodes, and total acid exposure time (AET) were measured using a catheter with one distal pH-probe and eight impedance rings, spanning from 6cm above the manometrically determined lower oesophageal sphincter (LOS).</p><p><b><i>Results:</i></b> Among the fourteen lung transplant recipients included in the study (8 [57.1%] female; median age, 56.5 years [IQR, 46-62]; median BMI, 22.7 kg/m<sup>2</sup> [IQR, 20.2-27.9]), six patients (42.9%) experienced an abnormal number of total impedance-detected reflux episodes, and eight patients (57.1%) had an abnormal total AET. Five patients (35.7%) experienced an abnormal number of impedance-detected proximal oesophageal reflux episodes, with three (21.4%) and seven (50.0%) experiencing an abnormal number of acidic and weakly acidic events, respectively. Univariate Poisson regression with bootstrapped confidence intervals (CI) identified that male sex (IRR=2.08, 95%CI [1.01,5.17], p=0.04), and a reduction in oesophageal motility parameters such as LOS basal pressure respiratory mean (IRR=0.96, 95%CI [0.94,0.98], p<0.001), LOS residual pressure median (IRR=0.93, 95%CI [0.88, 0.98], p=0.004) and distal contractile integral (IRR=0.63, 95%CI [0.48, 0.77], p=0.001), in addition to the presence of cystic fibrosis (IRR=1.77, 95%CI [1.23, 3.00], p=0.04) and the absence of pretransplant chronic obstructive pulmonary disease (IRR=0.48, 95%CI [0.16, 0.96], p<0.05), were predictors of increased proximal oesophageal reflux episodes (p<0.05). BMI (IRR=0.982, 95%CI [-0.168,0.079], p=0.737) and age (IRR=0.975, 95%CI [-0.085,0.018], p=0.124) were not statistically significant predictors.</p><p><b><i>Conclusion:</i></b> This study concludes that lung transplant recipients have greater episodes of proximal oesophageal reflux, compared to a healthy population, which may have implications for patient outcomes post-transplantation. Further research should explore the relationship between proximal oesophageal reflux episodes and lung function in lung transplant recipients.</p><p><b>273</b></p><p><b>Clinical characteristics and current clinical practice in patients with acute pancreatitis at a large tertiary centre</b></p><p><b>Cindy Ho</b>, Hardesh Dhillon, Kyle Williams, Eliza Flanagan, Faris Gondal, Sally Bell and Simon Hew</p><p><i>Monash Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Acute pancreatitis (AP) is a prevalent and potentially serious gastrointestinal illness. Contemporary studies evaluating the characteristics and management of patients with AP in large Australian tertiary centres are limited. Our study aims to detail the clinical characteristics of patients with AP and evaluate current clinical practices.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort study including all inpatients with AP at a large tertiary health service in Melbourne, Australia, from May 2022 to 2023. Data on demographics, fluid resuscitation, interventions, and nutrition were collected. Serious complications were defined as necrotising pancreatitis (NP), intensive care unit (ICU) admission, or death. For gallstone-related AP, time to laparoscopic cholecystectomy and readmission rates were calculated.</p><p><b><i>Results:</i></b> 553 patients with 639 admissions had AP. Most were male (51.4%) with a median age of 54 years (IQR 38-70) and BISAP of 1 (IQR 0-1). Gallstones (35.8%) were the commonest cause, followed by alcohol (26.6%) and idiopathic or unclear aetiology (16.6%). The mean intravenous fluid, mostly Hartmann’s (87.3%), administered within 24 hours of AP diagnosis was 4.5 litres (SD 0.4). NP, observed in 32 patients (5.0%), was associated with increased length of stay (LOS) (p<0.0001) and higher intervention rates for peri-pancreatic collections (OR 5.9, 95% CI 2.0-17.5) (Figure 1). Interventions included endoscopic (56.3%), percutaneous (18.8%), surgical (18.8%), or combined approaches (6.3%). The median time to drainage was 23.5 days (IQR 22.0-32.0). Nutritional support was required in 39 patients (6.1%), particularly those with NP (OR 4.6, 95% CI 1.8-11.5). The median time to light diet was 2 days (IQR 1-3). 36 patients needed ICU admission (5.6%), with a median ICU stay of 4.2 days (IQR 1.9-9.7) and a total hospital stay of 18.0 days (IQR 9.5-43.0). Higher BISAP scores correlated with increased ICU admissions (OR 10.9, 95% CI 5.2-22.2). Overall median LOS was 4 days (IQR 2-6), with a 2.2% mortality rate. 154 patients with gallstone-associated AP underwent laparoscopic cholecystectomy (80.7%), primarily as inpatients (76.0%), with a median time to surgery of 3 days (IQR 2-4) and 39 days (IQR 19-61) for outpatients. 37 patients (19.3%) did not undergo surgery due to comorbidities, patient wishes, or death. Nine readmissions occurred, three preventable by timely surgery.</p><p><b>274</b></p><p><b>Autoimmune enteropathy associated with COVID-19 infection - a case report</b></p><p><b>Wei Ling Teh</b>, Siaw Chai, Dilini Gunawardena and Jesica Makanyanga</p><p><i>Fiona Stanley Hospital, Perth, Australia</i></p><p><b><i>Introduction:</i></b> Autoimmune enteropathy (AIE) is a rare cause of chronic diarrhea that can occur as a primary condition or secondary to another immune-mediated process. Autoantibodies are not necessary for diagnosis, making AIE challenging to diagnose due to its overlap with other diseases characterized by villous atrophy. There is no standard treatment. Typically, patients are treated with glucocorticoids, sometimes combined with other immunosuppressive agents. This case highlights an AIE case whose symptoms began following COVID-19 infection, successfully managed with prednisolone and vedolizumab.</p><p><b><i>Case report:</i></b> A previously well 31-year-old woman was referred in March 2023 for months of severe watery diarrhea and vomiting, leading to electrolyte disturbances and weight loss. The diarrhea began after a mild COVID-19 infection in December 2022 and worsened after taking amoxicillin for an ear infection. She was not on regular medications. Her aunt had Crohn’s disease. ANA, ANCA, and coeliac antibodies were negative. Immunoglobulin levels were normal. HLA-B27 was negative, but HLA-DQ 2.5 indicated susceptibility to coeliac disease. Faecal tests were negative for infective causes. A secretory diarrhea screen (calcitonin, chromogranin A, gastrin, VIP) was negative. Endoscopy revealed mild gastritis and atrophic mucosa in the duodenum and terminal ileum, with normal colonic mucosa. Duodenal and ileal samples showed marked villous atrophy, active neutrophilic inflammation, absence of goblet cells, and a paucity of plasma cells and intraepithelial lymphocytes. Colonic biopsies showed focal active colitis without ulceration or CMV inclusion bodies. Anti-enterocyte and anti-goblet cell immunofluorescent staining were negative. She did not experience sustained benefit from corticosteroids or infliximab. Azathioprine was discontinued due to pancreatitis. Empirical trials of gluten free diet, octreotide and rifaximin were ineffective. In August 2023, vedolizumab, slow corticosteroid taper and partial parenteral nutrition (PN) were started. She showed gradual clinical improvement and reduced dependence on PN, eventually stopping it in April 2024. Repeat endoscopy in February 2024 showed epithelial cell regeneration and improved cryptitis, though goblet cells were still absent. She is currently on vedolizumab and 15mg of prednisolone daily, and in symptomatic remission.</p><p><b>275</b></p><p><b>The role of drug and alcohol services for patients with alcohol-associated acute pancreatitis at a large tertiary centre</b></p><p><b>Cindy Ho</b>, Hardesh Dhillon, Alex Mitropoulos, Eliza Flanagan, David Jacka, Sally Bell and Simon Hew</p><p><i>Monash Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Alcohol is a common cause of acute pancreatitis (AP), and ongoing consumption increases the risk of recurrent episodes. No specific guidelines exist for behavioural or pharmacological interventions to reduce recurrence of alcohol-associated AP. Studies exploring the role of addiction medicine for patients with alcohol-induced pancreatitis are limited. Our study aims to describe the utilization of the addiction medicine unit (AMU), a drug and alcohol physician-led inpatient consultation service, for patients admitted to a tertiary hospital with alcohol-associated AP.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort study including all inpatients diagnosed with alcohol-associated AP at a tertiary health service in Melbourne, Australia between May 2022 to 2023. Data on AMU referrals and assessment, recommended interventions, and outpatient follow-ups were collected. Re-admission rates for AP within this timeframe were calculated. Serious complications of AP were defined as those with necrotising pancreatitis, requiring intensive care unit (ICU) admission, or death.</p><p><b><i>Results:</i></b> 141 patients with 170 admissions were admitted with alcohol-associated AP. Most were males (76.6%), with a median age of 47 years (IQR 35-57) and median BISAP score of 0 (IQR 0-1). Fourteen patients (8.2%) had necrotizing pancreatitis, 13 (7.6%) required ICU admission, and 2 (1.4%) patients died. Fifty-seven patients (33.5%) were referred to the AMU. Of those referred, 98.2% were reviewed, either in person (73.2%) or via phone advice to clinicians (26.8%). Multi-disciplinary interventions including medications for addiction and outpatient services were recommended most (53.0%), followed by outpatient services alone (30.3%), and medications alone (16.7%). Outpatient services included follow-up in the AMU outpatient clinic, or more commonly, self-referrals to SECADA, a consortium for drug and alcohol addiction services including counselling and detox programs<b>.</b> 44 patients were recommended to commence or up-titrate medications for addiction by the AMU, which included naltrexone (61.4%), topiramate (38.6%), baclofen (6.8%), disulfiram (2.3%), either as single agents or in combination. Eighteen patients were re-admitted with alcohol-associated AP, with 11 (61.1%) not seen by the AMU during their initial admission. Of the 113 patients (66.5%) not referred to the AMU, contributing factors included patient refusal and weekend admissions.</p><p><b><i>Conclusion:</i></b> Within the limits of a single centre cohort with a short follow-up interval, our study demonstrated that approximately one-third of patients with alcohol-associated AP were referred to the AMU. Combination pharmacological and outpatient follow up were the most common interventions recommended. Efforts to improve referral patterns during index admissions may be helpful to reduce readmissions for alcohol-associated AP.</p><p><b>293</b></p><p><b>Enterocolitis with rectal and ileal stenosis: A rare presentation of metastatic urothelial carcinoma</b></p><p><b>Nicholas Smith</b>, Andrew Taylor and Jennifer Borowsky</p><p><i>Princess Alexandra Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Urothelial carcinoma is the most common histologic subtype accounting for approximately 90% of bladder cancers [1]. The most common sites of distant metastasis include liver, lung, and lymph nodes. Gastrointestinal tract involvement is rare [1].</p><p><b><i>Case Report:</i></b> An 81-year-old man presented with 3-months of vomiting, diarrhoea and abdominal pain. His background included; hypertension, benign prostatic hypertrophy and stage 3 chronic kidney disease. He was a non-smoker and lacked a family history of colorectal or urological malignancy. His medications included; perindopril, atenolol, aspirin and dutaasteride-tamsulosin. There was no non-steroidal anti-inflammatory exposure. Computer tomography revealed extensive mural thickening of both his small and large bowel suggestive of enterocolitis with pneumatosis intestinalis and a thickened bladder wall. Blood investigations were unremarkable apart from his known renal dysfunction and a mild leukocytosis of 11.5x10<sup>9</sup>/L and eosinophilia of 0.40x10<sup>9</sup>/L. C-reactive protein was 11mg/L. Colonoscopy showed congested and nodular mucosa throughout the entire colon with rectal and terminal ileal steosis, only traversable with a paediatric gastroscope (Figure 1.A). There was mucosal friability and loss of the normal haustral folds and vascular pattern. Histology revealed malignant cells present within lymphatics of the terminal ileum and colonic specimens. Immunohistochemistry showed positive staining of these cells with CK7, GATA3, and 34βE12 (Figure 1.B). There was no significant staining with CK20, PAX8, p53, TTF1 or CDX2. Urine cytology found atypical urothelial cells suggestive of a high-grade urothelial cell carcinoma. Cystoscopy revealed widespread erythema and cystitis with bullous areas with histology confirming the diagnosis of urothelial carcinoma, plasmacytoid subtype. Fludeoxyglucose positron emission tomography showed the expected uptake in the bladder and small and large bowel with small volume avid ascites. With the diagnosis of metastatic urothelial carcinoma, the patient was referred for palliative chemotherapy.</p><p><b><i>Discussion:</i></b> The mechanism of urothelial carcinoma related stenosis remains unclear. With rectal invasion, it has been hypothesized that a locally aggressive cancer of the bladder can penetrate Denonvilliers’ fascia and encircle the rectum [2]. It has also been thought that the cancer cells may spread along the lateral bladder pedicles to reach the posterior rectal wall [2]. Several case reports have detailed gastrointestinal tract metastases of urothelial carcinoma [2,3,4,5]. Wasfie [5] presents a case with stenotic small bowel disease. Liu [3] and Takeuchi [2] report cases with stenotic rectal disease. Ours is the only report with extensive entero-colitis with both rectal and ileal stenosis. This highlights the important but rare differential of metastatic disease in presentation of enterocolitis.</p><p><b>References</b></p><p>\\n 1 <span>Shinagare, AB</span>, <span>Ramaiya, NH</span>, <span>Jagannathan, JP</span>, <span>Fennessy, FM</span>, <span>Taplin, ME</span>, <span>Van den Abbeele, AD</span>. <span>Metastatic pattern of bladder cancer: correlation with the characteristics of the primary tumor</span>. <i>AJR Am J Roentgenol.</i> <span>2011 Jan</span>; <span>196</span>(<span>1</span>): <span>117</span>-<span>22</span>.</p><p>\\n 2 <span>Takeuchi, H</span>, <span>Tokuyama, N</span>, <span>Kuroda, I</span>, <span>Aoyagi, T</span>. <span>Annular rectal constriction caused by infiltrating bladder cancer: A case report</span>. <i>Mol Clin Oncol.</i> <span>2016 Dec</span>; <span>5</span>(<span>6</span>): <span>842</span>-<span>844</span>.</p><p>\\n 3 <span>Liu, YH</span>, <span>Pu, TW</span>, <span>Yu, HW</span>, <span>Kang, JC</span>, <span>Yen, CH</span>, <span>Chen, CY</span>. <span>Invasive urothelial carcinoma of urinary bladder presenting with annular constriction and mimicking proctitis observed by colonoscopy: A case report</span>. <i>Int J Surg Case Rep.</i> <span>2021 May</span>; <span>82</span>: <span>105785</span>.</p><p>\\n 4 <span>Tse, CS</span>, <span>Elfanagely, Y</span>, <span>Fine, S</span>. <span>Metastatic urothelial bladder cancer involving the rectum/Practical Gastro</span>. <span>2020</span> Nov; Vol XLIV, Issue 11.</p><p><b>296</b></p><p><b>Gastro-oesophageal reflux, determined with 24-hour pH-impedance monitoring, is highly prevalent in patients with chronic respiratory conditions, with many being asymptomatic or having extra-oesophageal symptoms</b></p><p><b>Michael Yulong Wu</b><sup>1,2,3</sup>, Ross Hansen<sup>1</sup>, Julia Mathers<sup>2</sup>, Vincent Liu<sup>2</sup>, David Joffe<sup>1,2</sup> and May YW Wong<sup>1,2</sup></p><p><sup>1</sup><i>Royal North Shore Hospital, Sydney, Australia;</i> <sup>2</sup><i>Northern Clinical School, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Faculty of Health Science and Medicine, Bond University, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> It is theorised that gastro-oesophageal reflux disease (GORD) can precipitate respiratory conditions due to aspiration of gastric contents into the respiratory tract provoking inflammation and neural reflexes which may trigger tracheobronchial constriction and hyperresponsiveness. However reflux symptoms can be unreliable indicators of the presence or absence of reflux. The primary aim of this study is to examine the prevalence of GORD using objective 24-hour pH-impedance monitoring in patients with chronic respiratory diseases (chronic obstructive pulmonary disease, bronchiectasis, asthma, interstitial lung disease). Secondary aims were to determine whether oesophageal symptoms and extra-oesophageal symptoms could predict presence of GORD, and whether respiratory function testing reflected severity of GORD.</p><p><b><i>Methods:</i></b> This is a retrospective cohort study using data collected between 2003 – 2023 in a quaternary referral centre. Patients over 18 years, referred for 24-hour pH-impedance monitoring for investigations into respiratory disease were included. An AET >4.2% was positive for GORD. A patient reported symptom questionnaire was used to categorise patients into those with oesophageal symptoms and extra-oesophageal symptoms. Oesophageal symptoms included chest pain and heartburn, and extra-oesophageal symptoms included cough, recurrent airway infections, vocal changes and throat symptoms such as irritation, constant clearing and laryngopharyngitis.</p><p><b><i>Results:</i></b> A total of 438 patients were included. The mean age was 60 years. Concurrent asthma and COPD (72.1%, n=316) were the most common respiratory diagnoses. Almost half of all patients had GORD (49%, n=217). GORD was present in a large proportion of asymptomatic patients (38.0%, n=82) and those with extra-oesophageal symptoms (32.9%, n=71) (Figure 1). Chronic cough and throat symptoms were the most common extra-oesophageal manifestations of reflux (61.4%, n=269 and 29.8%, n=71). Those with recurrent airway infection had the highest proportion of patients with GORD (59%, n=27). There were no significant differences in FEV<sub>1</sub> (p=0.55) , FVC (p=0.42) or FEV<sub>1</sub>/FVC (p=0.99) between those with and without diagnosis of GORD.</p><p><b>310</b></p><p><b>Case report: ocrelizumab induced colitis</b></p><p><b>Karly Potts</b> and David Scott</p><p><i>Hunter New England Health, Newcastle, Australia</i></p><p><b><i>Introduction:</i></b> Ocrelizumab is a humanised anti CD20 monoclonal antibody that is the sole disease modifying therapy for primary progressive multiple sclerosis. Fourteen case reports describing ocrelizumab associated colitis have been published. The majority describe disease onset within a few weeks therapy initiation. We herein report a case of severe ocrelizumab induced colitis following five years of therapy.</p><p><b><i>Case report:</i></b> A 68-year-old male presented with a four-week history of non-bloody diarrhoea and associated generalised abdominal pain. Pertinent medical history consisted of primary progressive multiple sclerosis, managed with 6 monthly ocrelizumab for the proceeding five years. Abdominal CT revealed mild mural thickening from the caecum to the descending colon. Stool testing for was positive for Blastocystic species, but otherwise negative for bacterial, viral, and parasitic pathogens. Colonoscopy demonstrated multiple deep ulcers in the left colon and normal intervening mucosa. There was near complete denudation of the right colon. Biopsy showed extensive ulceration with focal ischaemic changes and an inflammatory infiltrate characterised by an absence of B cells (figure 1). CMV was excluded by serology and biopsy. The patient failed to improve following 48 hours of empirical intravenous ceftriaxone and metronidazole. Oral budesonide and 100mg intravenous methylprednisone were commenced for severe drug induced colitis. A surgical opinion was sought for consideration of colectomy, but symptoms improved following steroid initiation, and no intervention was required. Prednisone was commenced at 60mg daily, to be gradually tapered. On day 17 of prednisone therapy the patient experienced worsening abdominal pain. Inflammatory markers, previously down trending, had increased. Repeat CT abdomen demonstrated overall improved appearances, and stool culture was negative. Treatment was escalated to a three-day course of methylprednisone and tofacitinib added to ongoing budesonide. This resulted in clinical and biochemical improvement and was followed by prednisone taper. Three months later, the patient remained well, with normalisation of biochemical parameters. Budesonide and prednisone were weaned, and he continued tofacitinib.</p><p><b>325</b></p><p><b>Expect the unexpected: A rare case of duodenal-type follicular lymphoma</b></p><p><b>Joel Thio</b></p><p><i>Department of Gastroenterology and Hepatology, Logan Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Duodenal-type follicular lymphoma is a rare entity that usually follows an indolent course. Most cases usually present asymptomatic and are found incidentally on endoscopic examination of the small bowel. The most common finding on endoscopic examination is that of white polypoid nodules. We present a case of an incidental finding of duodenal-type follicular lymphoma in a 61-year-old male.</p><p><b><i>Case report:</i></b> A 61-year-old Indian male presented to our service for further investigation of his iron deficiency anaemia with symptoms of generalised fatigue without obvious bleeding. He had a background of hypertension, ischemic heart disease, and benign prostate hypertrophy. Regular medications included perindopril, clopidogrel, rosuvastatin, and tamsulosin with dutasteride. Laboratory investigations revealed a haemoglobin of 127 g/L and a ferritin of 29 micrograms/L. He had a recent colonoscopy which was normal.</p><p><b><i>Discussion:</i></b> Follicular lymphoma typically follows an indolent course, and management mainly involves close monitoring and commencing treatment once symptoms manifest. This case highlights the importance of increased vigilance of this condition with the potential for subtle appearances on endoscopy.</p><p><b>327</b></p><p><b>Does a restrictive blood transfusion strategy have better outcomes in upper gastrointestinal bleeding? Six years of real world data</b></p><p><b>Hirannya Karunadasa</b>, Daniel Clayton-chubb, Stuart Roberts, Gregor Brown and <b>Shara Ket</b></p><p><i>Alfred Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Transfusion of blood products is an important component of resuscitation in the management of upper gastrointestinal bleeding (UGIB). Randomised studies have suggested that use of a restrictive transfusion strategy is associated with reduced all-cause mortality and rebleeding rates. The applicability and generalisability of a restrictive transfusion strategy in clinical practice remains unclear. The aim of this study was to evaluate and compare outcomes of restrictive versus liberal transfusion strategies in patients with UGIB over a six-year period in a real-world setting.</p><p><b><i>Methods:</i></b> A retrospective audit of patients presenting with or developing UGIB during admission in a quaternary referral hospital between 2018 to 2023 was conducted. Participants were excluded if they had lower gastrointestinal bleeding, had exsanguinating bleeding, were managed with outpatient gastroscopy or refused transfusion of blood products. Data collected included demographics, pathology results, transfusions, interventions and outcome data. Patients with a 24-hour nadir haemoglobin between 70g/L and 90g/L were stratified into a liberal transfusion group if packed red blood cells (PRBC) were transfused in that 24-hour period or into a restrictive transfusion group if they did not receive PRBC. The primary outcomes were mortality and rebleeding within 30 days of UGIB.</p><p><b><i>Results:</i></b> Of the 1089 patients included, 413 (37.9%) patients had a 24-hour nadir haemoglobin between 70g/L and 90g/L qualifying for evaluation of restrictive versus liberal transfusion strategies. The male gender accounted for 64.4% (n=266/413) of patients. The median age was 72 years (IQR 57-82 years), and the median Charlson Comorbidity Index was 6 (IQR 4-8). The median 24-hour nadir Hb was 78g/L (IQR 74-84 g/L). The leading cause of bleeding was peptic ulcers at 35.1% (n=145/413), while 10.2% (n=42/413) of patients had variceal bleeding. Most patients were stratified into the liberal transfusion group with 298 (72.2%) patients being transfused PRBC within the first 24 hours, with a median of 2 units (IQR 1-3 units) transfused within 24 hours. Regarding primary interventions, 40.9% (n=169/413) of patients required endoscopic intervention, with 4 (1.0%) requiring angiographic intervention and 2 (0.5%) requiring surgical intervention. A significantly greater proportion of patients in the liberal transfusion group experienced rebleeding within 30 days (n=43/298, 14.4% vs n=8/115, 7.0%; p=0.04). Although a numerically higher occurrence of all-cause mortality within 30 days was noted in the liberal transfusion group, this difference did not reach statistical significance (n=27/298, 9.1% vs n=6/115, 5.2%; p=0.23). In terms of secondary outcomes, the liberal transfusion group had poorer outcomes with significantly higher proportions of cardiac and pulmonary complications, acute kidney injury and bacterial infection (see Table 1, p<0.05).</p><p><b><i>Conclusion:</i></b> In the management of UGIB, a restrictive transfusion strategy appears to be associated with a significantly lower proportion of rebleeding and complications within 30 days of UGIB. This lends strength to current guidelines recommending restrictive transfusion strategy in the management of non-exsanguinating UGIB.</p><p><b>328</b></p><p><b>The effectiveness of budesonide orodispersible tablets in the real-world is lower than in clinical trials: a multicentre cohort study</b></p><p><b>Sarah Taylor</b><sup>1</sup>, Emily Barwick<sup>2</sup>, Varan Perananthan<sup>3</sup>, Sarah Lucas<sup>1</sup>, Ayushi Chauhan<sup>1</sup>, Catherine Yu<sup>1</sup>, Katrina Tan<sup>1</sup>, Diana Lewis<sup>1</sup>, Chamara Basnayake<sup>4</sup>, Hamish Philpott<sup>5</sup>, Sanjay Nandurkar<sup>6</sup>, Rebecca Burgell<sup>3</sup> and Mayur Garg<sup>1,2</sup></p><p><sup>1</sup><i>Northern Health, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia;</i> <sup>3</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>4</sup><i>St Vincents Hospital, Melbourne, Australia;</i> <sup>5</sup><i>Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>6</sup><i>Eastern Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Eosinophilic oesophagitis (EoE) is a chronic immune-mediated disorder that causes oesophageal dysfunction secondary to eosinophil-predominant inflammation. A budesonide orodispersible tablet (BOT) formulation has been shown to induce clincohistological remission in 57% of patients after 6 weeks of treatment, with histological remission in 93%. Real-world data for this medication however is currently limited. Previous Pharmaceutical Benefits Scheme (PBS) prescribing criteria mandated evidence of histological remission as defined by a peak eosinophil count of fewer than 5 eosinophils per high power field (hpf) within 12 weeks, but this has now been changed to allow treatment for up to 48 weeks. This study aimed to evaluate the real-world efficacy and adherence of patients with EoE treated with BOT at five tertiary centres in Victoria and South Australia.</p><p><b><i>Methods:</i></b> A retrospective medical record review of patients aged 18 years and over with a confirmed histological diagnosis of EoE (>15 eosinophils per hpf) and that were treated with BOT between July 2019 until February 2024 at five tertiary centers was performed. Data collected included patient demographics, endoscopy reports, histopathology, clinical symptoms, and previous medical treatments. Outcomes were reported using descriptive statistics.</p><p><b><i>Results:</i></b> 83 patients (69 [83%] male, median age 37 [range 19-79] years) on 1mg BD BOT were identified, with follow-up data for median 11 (IQR 10-16) months following commencement of BOT. The peak median eosinophil count prior to commencement on BOTs was 40 (IQR 30-50) per hpf. Patients had a median duration of disease prior to BOT therapy of 3 (IQR 2-6) years. 65% of patients had an allergic diathesis (asthma, hay fever, eczema, allergic rhinitis, or an allergy). Other therapies had been trialed prior to BOT commencement in 92 % of patients, with the majority (81%) having had proton pump inhibitor therapy. 14 patients (17%) had required previous oesophageal dilatation. Prior to BOT therapy, 40% of patients had experienced a food bolus obstruction with none occurring post commencement of BOT. Fewer than half (47%) had a repeat gastroscopy performed within 12 weeks of BOT commencement (median 80 days, IQR 67-112). The median peak eosinophil count on repeat gastroscopy post induction with BOT was 2 (IQR 0-30). Histological remission was noted in 48 (58%), clinical remission (defined as absence of symptoms) in 35 (42%) and endoscopic remission (no endoscopic features of EoE) in 26 (32%). 14 (17%) of patients were noted on clinic review to be using the medication incorrectly, with none of these patients achieving histological remission. Adverse events were reported by 15% of patients, with the most common being altered taste and oesophageal candidiasis (6% and 4.76 %, respectively).</p><p><b>353</b></p><p><b>Intrusive endometriosis involving the small bowel: a case report</b></p><p><b>Thant Zaw</b><sup>1</sup>, Peter Boyd<sup>1,2</sup> and Montri Gururatsakul<sup>1,2</sup></p><p><sup>1</sup><i>Cairns Hospital, Cairns, Australia;</i> <sup>2</sup><i>James Cook University, Cairns, Australia</i></p><p><b><i>Introduction:</i></b> Endometriosis, a condition characterized by the presence of endometrial tissue outside the uterine cavity, is a well-known affliction affecting approximately 10% of women of reproductive age. However, the occurrence of endometriosis in the small bowel remains a rare and intriguing phenomenon. This is a case report of a patient with small bowel endometriosis.</p><p><b><i>Case report:</i></b> A 40-year-old woman with a history of severe endometriosis presented at the Emergency Department with severe, recurring abdominal pain localized around the peri-umbilical area. She reported minimal relief from analgesics and had one episode of vomiting along with a single occurrence of loose stool, without any signs of blood in the stool or diarrhea. Notably, she had undergone a lower segment Caesarean section in 2017. A CT scan of the abdomen and pelvis revealed multiple segments of thickened, inflamed small bowel near the terminal ileum, raising concerns of Crohn's disease (Picture 1). Subsequent colonoscopy revealed luminal narrowing at the terminal ileum without any obvious mucosal abnormalities, and a biopsy taken from the terminal ileum showed unremarkable findings. She was treated conservatively with bowel rest and a course of IV hydrocortisone followed by oral prednisolone with the plan for further evaluation with relook colonoscopy and MRI scan. Two weeks later, she returned to the ED with recurrent small bowel obstruction and signs of small bowel volvulus, indicating a possible closed-loop obstruction due to twisting of the mesenteric pedicle. The decision was made to perform a laparoscopic right hemicolectomy. During the surgery, cicatrizing lesions were observed in the terminal ileum, and the histopathology results confirmed the presence of endometriosis in the small bowel and appendix.</p><p><b>361</b></p><p><b>Correlation between colonic mural thickening and endoscopy findings</b></p><p>Osamah Al-obaidi<sup>1</sup>, Hydar El Jamaly<sup>2</sup>, Noureddin Al-Hajjiri<sup>2</sup> and Mouhannad Jaber<sup>2</sup></p><p><sup>1</sup><i>Concord Hospital, Sydney, Australia;</i> <sup>2</sup><i>Wollongong Hospital, Wollongong, Australia</i></p><p><b><i>Background and Aim:</i></b> Colonic mural thickening (MT) is often reported on standard CT examinations of the abdomen and pelvis. It often presents a dilemma for the clinician on whether any further evaluation is needed, especially in the absence of any set guidelines. Our aim is to evaluate the significance of colonic MT and to assess its correlation with colonoscopy.</p><p><b><i>Methods:</i></b> We conducted a comprehensive literature search using a strategy in Medline and this was extended to Pubmed and Embase. The studies included patients with increased Colonic wall thickness on CT scans, who underwent endoscopic evaluation. We used a random-effects model using pooled positive predictive value (PPV) with 95% confidence intervals (CI).</p><p><b><i>Results:</i></b> A total of 15 cohort studies examining 1596 patients were selected having undergone both CT and colonoscopy. Of the 1596 patients with MT, 1152 had an abnormal colonoscopy. In the presence of MT of 3mm or more, the pooled positive predictive value (PPV) of malignancy was 0.23 (95% CI: 0.16-0.33) and that of all pathology was 0.65 (95% CI: 0.47-0.80). In the presence of MT of >5mm, the pooled positive predictive value (PPV) of malignancy was 0.15 (95% CI: 0.09-0.24) and that of all pathology was 0.71 (95% CI: 0.54-0.83). In patients with MT in the right colon, the pooled PPV of malignancy was 0.14 (95% CI: 7.4-23.7) and that of all pathology was 0.34 (95% CI: 0.18-0.55) as shown in Figure (1). In the left colon MT groups, the pooled PPV of malignancy was 0.18 (95% CI: 0.12-0.26) and that of all pathology was 0.74 (95% CI: 0.53-0.88).</p><p><b>369</b></p><p><b>Food bolus obstruction: what factors prevent clinicians from performing biopsies for eosinophilic oesophagitis during acute endoscopy?</b></p><p><b>Melissa Carroll</b><sup>1</sup>, Matilda Surtees<sup>1</sup> and Nick J Talley<sup>1,2</sup></p><p><sup>1</sup><i>NSW Health - John Hunter Hospital, Newcastle, Australia;</i> <sup>2</sup><i>University of Newcastle, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> Eosinophilic oesophagitis (EoE) is identified in up to 50% of patients who present with a food bolus obstruction (FBO). Accepted guidelines recommend oesophageal biopsy be performed at index endoscopy for prompt diagnosis and management of EoE, however, this occurs in only 40% of food bolus presentations. To understand factors that impact clinicians practice, we collected data from all food bolus obstructions that presented over a 3-year period with the aim to understand potential barriers to obtaining oesophageal biopsies for the diagnosis of EoE during an acute presentation.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort study of adult patients presenting with acute food bolus obstruction to a tertiary hospital from January 2020 to December 2022. Patient records were identified using endoscopy reporting software (ProvationMD) and International Classification of Disease (ICD) coding for ‘foreign body in oesophagus.’ Patients with intentional ingestion of foreign body objects were excluded. Patient demographics, medical comorbidities, drug therapy with anticoagulation and/or antiplatelet therapy and prior history of FBO was collected. Clinician reported macroscopic endoscopy findings, location and number of oesophageal biopsies, timing of procedure and histological findings were included. A diagnosis of EoE was confirmed where eosinophil-predominant inflammation was found (≥15 eos/hpf) on biopsy. Statistical analysis was performed using SPSS V.29 software and p-values <0.05 were considered significant. Pearson’s <i>χ</i><sup>2</sup> was used to assess for a significant relationship between timing and frequency of biopsy.</p><p><b><i>Results:</i></b> A total of 251 patients with food bolus obstruction were identified over the 3-year study period, with 239 undergoing endoscopy 95.2%. Of these, EoE was histologically confirmed in 54 cases (22.5%), with those most likely to present between 45 and 59 years of age (27.4%) and predominately male 71.4%. A prior food bolus obstruction was recorded in 50.2% of patients and 15% of patients had a history of atopy. 4.4% of patients were receiving treatment for EoE. A total of 119 patients (49.7%) had oesophageal biopsies at index endoscopy. Endoscopy was performed mostly in business hours (8am and 5pm), with 161 patients (67.3%) and of those, 84 patients had biopsies (52.1%). There was no significant relationship between timing of procedure and having a biopsy (p=0.703). There was a significant relationship with those on antiplatelet therapy and having a biopsy with 5 out of 38 patients biopsied (p < 0.001), but not with those on anticoagulation therapy, 9.2% biopsied Vs 60.8% not biopsied (p=0.272). Patients with a history of atopy were more likely to have a biopsy (p=0.019) than those with a cardiac history (67.5% Vs 32.3%). There was no significant relationship between having macroscopic findings consistent with EoE and having a biopsy, 51 patients with reported findings and 22 biopsied (43.1%, p=0.299). Of those who presented with a further food bolus obstruction within 3-years (44 total), a diagnosis of EoE was the most common underlying diagnosis, 13 patients (29.5%).</p><p><b><i>Conclusion:</i></b> Guidelines for the diagnosis and management of eosinophilic oesophagitis (EoE) recommend endoscopy and biopsy for histological diagnosis of EoE during acute food bolus obstruction. This study underscores the significant prevalence of EoE among patients presenting with food bolus obstruction, particularly among middle-aged males. It highlights the importance of considering patient history, such as prior obstructions and atopy, in managing and diagnosing EoE. The findings also suggest that while biopsy practices during endoscopy are influenced by factors like medication (specifically antiplatelet therapy) and patient history, the timing of the procedure does not appear to significantly affect biopsy rates. The recurrence of food bolus obstruction in patients with EoE emphasizes the need for ongoing management and potential treatment adjustments for these individuals.</p><p><b>370</b></p><p><b>Correlation between hypermetabolic PET/CT activity and clinically significant lesions found at endoscopic evaluation</b></p><p><b>Melissa Carroll</b>, Patrick Felton and Steven Bollipo</p><p><i>NSW Health, John Hunter Hospital, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> Hypermetabolic activity in the gastrointestinal tract prompting endoscopic evaluation is frequently encountered on PET/CT imaging performed for various clinical scenarios. Our aim was to collect data from endoscopic procedures performed for the indication “Abnormal PET scan of the GI Tract,” and analyze data to evaluate PET/CT avidity and the corresponding endoscopic and histological findings.</p><p><b><i>Methods:</i></b> We conducted a retrospective cohort analysis of all adult patients who underwent endoscopy at a tertiary hospital over a 3-year period from January 2019 to December 2023, for reported hypermetabolic activity in the gastrointestinal tract on positron emission tomography/computed tomography (PET/CT) imaging. Patients were identified through endoscopy reporting software (ProvationMD), with the indication “Abnormal PET scan of the GI tract.” Patient demographics and indication for imaging was collected. We specifically looked at the location of avidity on PET/CT and whether there was correlation with endoscopic findings. We collected data on lesion location and size, histological findings, and additional or incidental findings which were not reported from PET/CT imaging. Clinically significant lesions were considered as high-grade dysplasia, invasive carcinoma and malignant (adenocarcinoma, lymphoma, melanoma). Statistical analysis was performed using SPSS V.29 software and p-values <0.05 were considered significant. Pearson’s <i>χ</i><sup>2</sup> was used to assess for significant relationship between size, location and clinical significance of found lesions.</p><p><b><i>Results:</i></b> Of 331 patients who underwent endoscopy, a total of 62 patients (18.8%) were found to have a clinically significant lesion identified. There were 204 cases with a lesion identified at endoscopy correlating with hypermetabolic activity on PET/CT (61.6%), and of these 41 cases were clinically significant lesions 12.4%. An unknown primary malignancy was the most common indication for PET/CT (21.7%). There were 127 patients (38%) with a polypoid lesion found at endoscopy, with 68 lesions >20mm in size and of those, 47% were clinically significant (p = <0.05). Adenocarcinoma was the most common significant lesion (14%) on histology. PET/CT failed to detect 15 cases of clinically significant lesions (4.5%). There was a slight male predominance 55.9% Vs 44.1%, with endoscopy being performed more often in those who were aged 55 years or older (89%). Overall, 54 patients (16%) who underwent endoscopy had no macroscopic lesion identified during their endoscopic procedure.</p><p><b><i>Conclusion:</i></b> We conducted a retrospective analysis of data from adult patients who underwent gastroscopy and/or colonoscopy based on positron emission tomography/computed tomography (PET/CT) imaging with gastrointestinal findings. The study provides valuable insights into the prevalence, significance, and characteristics of PET/CT avid lesions detected in the gastrointestinal tract, as well as their correlation with endoscopic findings. These findings contribute to our understanding of the diagnostic approach to patients with incidental PET/CT findings, informing clinical decision-making in this context.</p><p><b>389</b></p><p><b>An unusual presentation of appendicitis detected on colonoscopy in a young female with coeliac disease</b></p><p>Eleanor Wheatley and <b>Mohammad Shir Ali</b></p><p><i>John Hunter Hospital, Newcastle, Australia</i></p><p><b><i>Introduction:</i></b> Appendicitis is classically a clinical diagnosis, with urgent surgical management. It is often an emergency presentation with symptoms including acute pain migrating from the peri-umbilical region to the right iliac fossa (RIF), nausea, anorexia, and fever. Physical examination findings include tenderness in the RIF with rebound pain and peritonism. Subacute appendicitis on the other hand can be a more evasive diagnosis. In addition, fibrous obliteration of the appendix which is a histological diagnosis, can mimic acute appendicitis. Here we present an unusual presentation of appendicitis (with fibrous obliteration) which went undetected on the initial clinical assessment and cross-sectional imaging but was eventually detected on colonoscopy.</p><p><b><i>Case report:</i></b> We report a 19-year-old female presenting with subacute/chronic RIF pain on a background of coeliac disease and type 1 diabetes. The patient had 3 prior emergency presentations with generalised abdominal pain spanning a 2-month period, each time having worsening RIF pain which had deteriorated over a series of days. The patient presented a final time to the emergency department with RIF pain and nausea. With no other classical symptoms of appendicitis other than generalised pain and guarding on admission, differentials included pelvic inflammatory disease (PID), urinary tract infection, ureteric calculus, inguinal hernia, and ovarian pathology. Diagnostic workup included abdominal ultrasound which excluded ureteric calculi and renal tract pathology, however displayed hyperaemia and mild mural thickening of the terminal ileum. Subsequent computed tomography (CT) scan showed similar findings suggestive of terminal ileitis. Notably, there were no features of appendicitis on this initial CT scan. Colonoscopy subsequently confirmed appendicitis by visualisation of pus emanating from the appendiceal orifice and congested mucosa at the site. The terminal ileum appeared completely normal on colonoscopy. A repeat preoperative CT showed an enlarged and inflamed retrocaecal appendix. The patient then underwent a laparoscopic appendicectomy without any sequelae. The histology of the surgical specimen revealed focal mucosal ulceration consistent with appendicitis. In addition there was prominent fibrous obliteration of the tip of the appendix a condition that can also mimic acute appendicitis.</p><p><b>398</b></p><p><b>Unexpected diagnosis: collagenous ileitis in a patient without diarrhea</b></p><p><b>Fei Yang Pan</b><sup>1</sup> and Ahmad Alrubaie<sup>1,2</sup></p><p><sup>1</sup><i>Macquarie University Hospital, Sydney, Australia;</i> <sup>2</sup><i>Bankstown-Lidcombe Hospital, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Collagenous ileitis (CI) is extremely rare, with only four reported cases. Two additional cases were medication-induced by mycophenolate and duloxetine. CI, part of collagenous enteritis, features thickening of the mucosal subepithelial collagen band, chronic inflammation, increased epithelial lymphocytes, and epithelial detachment. The cause of subepithelial collagen deposition in the GIT is unknown, but research suggests an inflammatory process with profibrogenic mediators. Symptoms include diarrhea, altered bowel habits, epigastric pain, and bloating. CI is isolated to the ileum, unlike collagenous sprue (CS), which affects the proximal small intestine. Diagnosis requires histopathology confirming a thickened subepithelial collagen band, typically over 10 μm, similar to the criteria for collagenous colitis (CC).</p><p><b><i>Case Report:</i></b> A 77-year-old female presented with recurrent melena and iron deficiency anaemia. A video capsule endoscopy revealed gastric antral vascular ectasia (GAVE) and mild to moderate circumferential congestion and erythema in the small bowel. Her medical history includes diverticulitis, hypertension, asthma, hypercholesterolemia, anxiety, reflux, and endometrial cancer, for which she underwent a hysterectomy and salpingo-oophorectomy. She is currently on rosuvastatin, rabeprazole, and sertraline. On 29/02/24, she underwent an antegrade double-balloon endoscopy, which provided views up to the proximal ileum which demonstrated a 60 to 70 cm segment of abnormal mucosa with erythematous changes and nodularity in the distal jejunum and proximal ileum. Biopsies of the distal jejunum showed normal mucosa except for mild oedema of the lamina propria, without increased inflammation or evidence of microscopic colitis. Biopsies of the proximal ileum revealed mildly oedematous ileal mucosa with some broadening of the villi and a patchy increase in the subepithelial collagen plate between 10 and 20 μm, confirmed by Masson trichrome staining. Interestingly, terminal ileum biopsies performed on 16/01/24 showed normal ileal mucosa. She was subsequently started on a daily dose of 9 mg of budesonide with good effect. A repeat colonoscopy is planned soon to assess both the colon and ileum for collagenous disorders.</p><p><b>410</b></p><p><b>Summary of pharmaceutical industry clinical trials of biologics for eosinophilic oesophagitis in Australia and internationally: Substantial contributions possible in Australia, but room for improvement</b></p><p>Rity Wong<sup>1</sup>, <b>Hamish Philpott</b><sup>1,2</sup> and Thomas Lokan<sup>1</sup></p><p><sup>1</sup><i>Northern Adelaide Local Health Network, Adelaide, Australia;</i> <sup>2</sup><i>University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> There is a need for additional medications to treat eosinophilic oesophagitis (EoE) due to a lack of efficacy or tolerability of current agents. Pharmaceutical companies are developing biologics often borrowed from related disease states (particularly inflammatory bowel disease, and atopic conditions such as asthma or dermatitis). Given our relatively small population overall, yet a high prevalence of EoE, we consider the Australian contribution to key international pharmaceutical industry studies of biologics in adult patients with EoE.</p><p><b><i>Methods:</i></b> We interrogated our own database, as well as the Annual Progress Report for each agent, and cross validated Australian and international data using the online trial registry https://clinicaltrials.gov. Individual trial name, biological class and mechanism of action, recruitment time time window, screening number and failure rate as well as Australian and total recruitment number was calculated.</p><p><b><i>Results:</i></b> Over the last 5 years (2019-2024), five (5) biologics have been trialled in Australia as part of international efforts (Table 1). The number of patients enrolled in these studies varied between 108 to 430, with the Australian contribution being between 10-26 patients per study (2-6%). There were between 4 and 12 sites in Australia for each study. Screen failure rates ranged from 0-57% at our site (Northern Adelaide Local Health Network - NALHN) and NALHN contributed between 25% and 66% of patients successfully enrolled in each of the 5 studies in Australia and overall, 43% of all Australian patients enrolled were from NALHN.</p><p>\\n \\n </p><p><b><i>Conclusion:</i></b> Australia can make a meaningful contribution to international pharmaceutical industry studies in EoE. To date, a small number of sites have enrolled a significant proportion of patients, suggesting that more focussed efforts in future can improve recruitment in Australia in future.</p><p><b>419</b></p><p><b>An early review of MetaPanel™ - a diagnostic metagenomic gastrointestinal pathogen assay</b></p><p><b>Michael Wehrhahn</b><sup>1</sup>, David Wood<sup>2</sup>, Nicola Angel<sup>2</sup>, Donovan Parks<sup>2</sup>, Rhys Newell<sup>2</sup>, Andrew Ginn<sup>1</sup>, Lutz Krause<sup>2</sup>, Paul Griffin<sup>2</sup> and Jim Newcombe<sup>1</sup></p><p><sup>1</sup><i>Douglass Hanly Moir Pathology, Sydney, Australia;</i> <sup>2</sup><i>Microba, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal infection is routinely diagnosed by culture, PCR or a combination of both. However, the diagnosis is limited to pathogens that are targets in the multiplex PCR assay or detected on routine culture media. In March 2024, a comprehensive faecal metagenomics assay (MetaPanel™) was introduced through Sonic Healthcare Australia Pathology laboratories. This assay reports 115 DNA pathogens including bacteria and selected bacterial virulence factors, protozoa, helminths, viruses, fungi and microsporidia, in addition to 60 antimicrobial resistance (AMR) genes and a research use only dysbiosis measure incorporating diversity and richness scores.</p><p><b><i>Methods:</i></b> A review of the first 79 MetaPanel samples was undertaken, focusing on type of referrer, patient demographics, detected pathogens, detected AMR genes, and proportion with low diversity and richness (defined as falling in the lowest decile of a healthy cohort).</p><p><b><i>Results:</i></b> The average age of the referred patient was 47 years (11% under 18 years) and 59% were female. The most common referrers were community practitioners (53%, with about 1/5 of these having an interest in integrative medicine), followed by gastroenterologists (30%), and other specialists (16%) comprising haematologists, oncologists, rheumatologists, infectious diseases physicians and immunologists. A putative pathogen was identified in 19% of samples, including: enteropathogenic <i>E. coli</i> (EPEC) (3), <i>Campylobacter concisus</i> (3), <i>Tropheryma whipplei</i> (2), toxigenic <i>Clostridium perfringens</i> (2), toxigenic <i>Staphylococcus aureus</i> (1), <i>Yersinia frederiksenii</i> (1), toxigenic <i>Clostridium difficile</i> (1), <i>Campylobacter jejuni</i> (1), <i>Aeromonas hydrophila</i> (1) and <i>Aeromonas caviae</i> (1) with the former 6 pathogens not routinely identifiable by PCR or culture. AMR genes were detected in 29% of samples with 61% of these including AMR genes not co-detected with common host organisms, indicating a higher risk of patient-to-patient transmission (CTX-M Extended Spectrum Betalactamas (ESBL) (5), qnrB quinolone resistance (2), rmtD aminoglycoside resistance (2) and vanA/B vancomycin resistance (3)). In 82% of samples, the gut microbiome was classified as being of low diversity and/or richness.</p><p><b><i>Conclusion:</i></b> Early results support the utility of a faecal metagenomics assay (MetaPanel) in diagnosing difficult-to-detect gastrointestinal pathogens and identifying carriage of clinically relevant antimicrobial resistance genes. Further studies are underway to investigate the impact of MetaPanel on patient management and clinical outcomes.</p><p><b>430</b></p><p><b>The first randomised controlled trial of Jorveza (budesonide) compared to PPI (pantoprazole) for eosinophilic oesophagitis: Progress report of a multi-site Australian study</b></p><p><b>Hamish Philpott</b><sup>1,2</sup>, Thomas Lokan<sup>1</sup> and Edward Young<sup>1</sup></p><p><sup>1</sup><i>Northern Adelaide Local Health Network, Adelaide, Australia;</i> <sup>2</sup><i>University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background:</i></b> Eosinophilic oesophagitis (EoE) is a chronic inflammatory condition that progresses to fibro-stenosis and recurrent food bolus impaction. Expert opinion proposes that Jorveza (budesonide) is more effective than PPI in resolving inflammation and reversing fibro-stenosis. The two agents have not been subject to a randomised controlled trial (RCT).</p><p><b><i>Methods:</i></b> Ethics review board clearance of a 12 site (multicentre) study across Australia, for adult patients with EoE aged 18 years and over, with established diagnosis of EoE (>15 eosinophils per HPF) and no previous use of Jorveza. Treatment naïve patients are randomised to Jorveza 1mg Po BD or Pantoprazole 40mg Po BD, with repeat endoscopy in 8-10 weeks, biopsies of the lower and middle oesophagus, endoscopic reference score (EREFs) and symptom scores (EoEsA1 PRO and EoE – QOL-A) being completed. At clinic review patients responding (<5/HPF) continue treatment for another 8-10 weeks, with endoscopy, EREF’s and symptom scores repeated at weeks 16-20. Patients failing initial treatment cross- over to the alternative medication (PPI or Jorveza) for a period of 8-10 weeks prior to repeat endoscopy, EREF’s and symptom scores, again at week 16-20 from enrolment. Consenting patients at specific trial sites will undergo EUS and EndoFlip at week 8-10 and week 16-20. Target sample size 72 (36 each for Jorveza and PPI, anticipated treatment effect difference 25%, power 0.80), recruitment from December 2023 to December 2025.</p><p><b><i>Results:</i></b> Enrolment commenced December 2023 and currently 5 of 12 sites are active (NALHN – Lyell McEwin and Modbury hospitals, Royal Adelaide Hospital, Flinders Medical Centre, Monash Medical Centre and Northern Hospital Epping). 19 patients have been enrolled (June 5<sup>th</sup>, 2024, all from NALHN) trial completed in 4 individuals. Patients mean age of 36 years (range 21-58) 12/19 (63%) being male. 15/19 patients (79%) presented with food bolus impaction, and all were on nil current treatment.</p><p><b><i>Conclusion:</i></b> The first randomised controlled trial of Jorveza vs PPI is underway, feasible and recruitment to schedule. More data to follow, additional sites to activate will speed recruitment and results.</p><p><b>448</b></p><p><b>Vertigo and pancreatic malabsorption</b></p><p><b>John Evans</b></p><p><i>Queen Elizabeth II Jubilee Hospital, Brisbane, Australia;</i> <i>St Andrew's War Memorial Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Vertigo is a functional disturbance in which there is an illusory sense of movement either of self or of the environment, the result of asymmetry in impulses impacting on the right or left vestibular system due to dysfunction of the semi-circular canals, vestibular nerve, or brain stem and is divided into peripheral and central causes. Peripheral causes are considered due to particles in the semi-circular canals. Vertigo was the most common presenting symptom from studies in Primary Care, Emergency Rooms, and Dizziness Clinics. Management of Vertigo is supportive. Particle positioning manoeuvres (Epley or Sermont) can be used although recurrences are frequent; and medication can be tried for the acute clinical situation (antihistamines, and/or benzodiazepines, and/or anti-emetics) or for recurrent episodes (betahistine and/or prochlorperazine) although there seems to be no evidence of these drugs’ long-term efficacy.</p><p><b><i>Case Reports:</i></b> Both husband & wife from a rural setting incidentally mentioned improvement in vertigo following management of pancreatic exocrine insufficiency (PEI). A further five female patients with PEI experienced vertigo. These patients also underwent tests of hearing, and Videonystagmography (Caloric testing) and were later reassessed. The manoeuvres or medications mentioned above were not utilised. All patients revealed prolonged symptomatic and objective improvement of Vertigo with management of malabsorption associated with PEI.</p><p>VERTIGO, VIDEONYSTAGMOGRAPHY, & PEI\\n\\n </p><p>+ rural couple</p><p><b><i>Conclusion:</i></b> Vertigo may be a hitherto unrecognised, uncommon association of malabsorption due to PEI but appropriate management of PEI revealed long term, effective management of Vertigo. These improvements occurred despite the considered presence of particles in the semi-circular canals. Consideration of malabsorption in patients with Vertigo may enhance management of Vertigo.</p><p><b>472</b></p><p><b>Transmural changes of microscopic colitis using intestinal ultrasound: a case report</b></p><p><b>Peter Litwin</b><sup>1</sup>, Bhuwan Tandon<sup>1,2</sup>, Aude Van Oosterwyck<sup>1,2</sup>, Robert Bryant<sup>1,2,3</sup> and Ryan M Mathias<sup>1,2,3</sup></p><p><sup>1</sup><i>Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>2</sup><i>Inflammatory Bowel Disease Service, Queen Elizabeth Hospital, Adelaide, Australia;</i> <sup>3</sup><i>The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> The use of Gastrointestinal Ultrasound (GIUS) is well established in the evaluation of patients with inflammatory bowel disease, which is not the case in microscopic (or collagenous) colitis. Whilst a 2022 study of 498 patients by Koop et al. demonstrated abnormal CT imaging in this disease, only a single case report of GIUS abnormalities can be found in the literature. However, there are no reports demonstrating its use case as a non-invasive treatment modality in assessing treatment response.</p><p><b><i>Case Report:</i></b> A 61-year-old female presented with a 12-week history of progressive diarrhoea and urgency (up to 14 times per day), initially watery but having become blood and mucous stained in the preceding 3 weeks. Her past medical history included high cholesterol, hypertension and anxiety, for which she was prescribed longstanding atorvastatin, amlodipine and venlafaxine. She was a non-smoker, had no recent antibiotic exposure, no over the counter medications and no family history of autoimmune disease. Biochemical abnormalities included hypokalaemia (2.6 mmol/L), an acute kidney injury (creatinine 110 umol/L) and an elevated C-reactive protein (40 mg/L). Stool samples were negative for infection and her faecal calprotectin was elevated at 189 ug/g (<50). Unprepared colonoscopy demonstrated a severe confluent pancolitis from the rectum to caecum with a normal terminal ileum. Gastrointestinal ultrasound (GIUS) demonstrated pancolitis with increased bowel wall thickening (maximum 5.6mm), modified Limberg 2 doppler activity and preserved wall stratification. Histology confirmed collagenous colitis with preserved crypt architecture, thickening of the subepithelial basement membrane and plasmacytosis. The patient was commenced on intravenous hydrocortisone 100mg QID with excellent clinical (bowel frequency reduced to 2) and biochemical response over a 48-hour period and was transitioned to prednisolone and later budesonide. Repeat GIUS 6 days post therapy demonstrated complete transmural healing with normalisation of bowel wall thickness and no increased colour doppler signal.</p><p><b>486</b></p><p><b>Not all right-sided colonic ulcers are Crohn’s disease: <i>Entamoeba histolytica</i> and <i>Mycobacterium tuberculosis</i> infections diagnosed at colonoscopy</b></p><p><b>Vanessa Chong</b><sup>1</sup>, <b>Jin Lin Tan</b><sup>1,2</sup>, Biju George<sup>1</sup>, Mohamed Asif Chinnaratha<sup>1,2</sup> and Damian Harding<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> Ulceration in the right colon is commonly caused by Crohn’s disease, but other causes including infection, malignancy and ischaemia should be considered. Distinguishing the aetiologies by symptoms alone can be difficult due to similar clinical presentations. Infectious causes are particularly relevant for those who have travelled or migrated from endemic areas. This case series outlines three cases of right-sided colonic ulceration caused by <i>Entamoeba histolytica</i> and <i>Mycobacterium tuberculosis</i>.</p><p><b><i>Case reports:</i> Case 1)</b> A 67-year-old female from Afghanistan experienced intermittent right iliac fossa pain and iron deficiency anaemia. Colonoscopy revealed discrete deep caecal ulceration. Biopsies sent for TB and amoebiasis PCR were positive for <i>E. histolytica,</i> with amoebic organisms seen on histology. Treatment with Tinidazole followed by paromomycin resulted in symptom resolution and endoscopic healing of colonic ulcers. <b>Case 2)</b> A 61-year-old female from Myanmar had several years of right-sided abdominal pain, diarrhea and weight loss. CT showed mural thickening in the caecum and ascending colon. Colonoscopy revealed a hemi-circumferential and ulcerated polypoid mass in the caecum. Biopsies were sent for TB PCR, culture (both positive for <i>M. tuberculosis</i>) and histology, which showed necrotising granulomatous inflammation. After 9 months of anti-tuberculous therapy her symptoms resolved. Follow-up colonoscopy showed resolution of the caecal mass. <b>Case 3)</b> A 31-year-old female from Nepal with previously diagnosed Crohn’s disease underwent a colonoscopy to evaluate worsening abdominal pain and altered bowel habits. CT showed extensive inflammation in the caecum and ascending colon accompanied with enlarged necrotic mesenteric nodes. Initial treatment with steroids and biologics was ineffective. Colonoscopy revealed deep ulcers luminal narrowing at the hepatic flexure. Biopsies were positive for <i>M. tuberculosis</i>. She was commenced on anti-tuberculous therapy with resolution of symptoms and currently scheduled for follow-up colonoscopy after 9 months of treatment.</p><p><b><i>Discussion:</i></b> Amoebiasis is transmitted through ingestion of amoebic cysts, which develop into trophozoites in the intestines that in some will cause invasive disease. Colonoscopy typically shows discrete, deep ulcers in the proximal colon, sparing the terminal ileum and distal colon. Histology may show “flask-shaped” ulcers with amoebic trophozoites. Intestinal tuberculosis (ITB) constitutes 2% of TB cases worldwide, often from latent TB reactivation or ingestion of tuberculous mycobacteria. Colonoscopy often reveals ileocaecal disease, and histology, caseating sub-mural granulomas, unlike the transmural granulomas associated with Crohn’s disease. Tissue biopsies for PCR and culture are essential for diagnosing amoebiasis and ITB and should be considered at the time of colonoscopy.</p><p><b>488</b></p><p><b>Aortoesophageal fistula with life-threatening upper gastrointestinal bleeding: a case report</b></p><p><b>Xiaomin Ma</b><sup>1,5</sup>, <b>Mohamed Reffai Syed Mohamed</b><sup>1</sup>, Bulent Baran<sup>1,4</sup>, Christine Welch<sup>1,4</sup>, Kevin Tian<sup>3,4</sup>, Donald Cameron<sup>2,4</sup>, Yew Toh Wong<sup>3,4</sup> and Rozemary Karamatic<sup>1,4</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Townsville University Hospital, Townsville, Australia;</i> <sup>2</sup><i>Department of General Surgery, Townsville University Hospital, Townsville, Australia;</i> <sup>3</sup><i>Department of Vascular Surgery, Townsville University Hospital, Townsville, Australia;</i> <sup>4</sup><i>School of Medicine, James Cook University, Townsville, Australia;</i> <sup>5</sup><i>School of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Aortoesophageal fistula (AEF) arises from an abnormal connection between the aorta and the oesophagus. It is defined by Chiari’s triad of mid-thoracic pain, sentinel arterial haemorrhage and exsanguination after a symptom-free interval. Only 20-45% of patients fulfil this criterion, and a high index of suspicion is required. AEF may result in fatal upper gastrointestinal bleeding (UGIB) if not promptly addressed, with a mortality rate of 47-77%. We present the case of a 71-year-old man with AEF-related unstable UGIB managed successfully with endoscopic and endovascular intervention.</p><p><b><i>Case Report:</i></b> A 71-year-old man presented to an Australian regional hospital with chest pain and haematemesis on a background of a gastro-oesophageal junction adenocarcinoma with nodal metastases treated with palliative chemoimmunotherapy and radiotherapy. He had previous oesophageal dilatations and stents for dysphagia complicated by tissue ingrowth and stent migration. Six weeks prior to presentation, a fully covered stent was placed across a tight stricture, with clips used to secure the proximal end and an 18mm balloon inflated inside the stent. On presentation, he was haemodynamically unstable requiring aggressive resuscitation. Computed Tomography Angiography (CTA) demonstrated distal migration of the stent with no bleeding source identified. He was transferred to the tertiary referral hospital after detailed CTA review due to high suspicion for AEF in view of prior radiotherapy and endotherapy. A multidisciplinary discussion involving gastroenterology, general surgery, vascular surgery, anaesthetics and intensive care unit (ICU) occurred prior to endoscopy to ensure appropriate personnel were available. At endoscopy, large amounts of blood clot were found throughout the oesophagus. The stent was found in the distal oesophagus, with ulceration at the proximal edge of the stent at the site of a clip. Following stent removal, an excavated ulcer covered with granulation tissue started exsanguinating, requiring activation of massive transfusion protocol. A partially covered metal stent was deployed to tamponade the bleeding and vascular surgery immediately proceeded to endovascular aortic stent graft insertion. He was transferred to ICU in a stable condition. The oesophageal stent was endoscopically removed the following day to avoid necrosis of tissue trapped between the oesophageal and aortic stents. The patient did not rebleed after stent removal.</p><p><b>496</b></p><p><b>High prevalence of ARFID and orthorexia nervosa in gastroenterology patients: an evaluation of disordered eating in a large gastroenterology clinics cohort</b></p><p><b>Amy Luo</b><sup>1</sup>, Hannah Kim<sup>1</sup>, Jessica Green<sup>1</sup>, Annalise Stanley<sup>1</sup>, Jamee Barugh<sup>1</sup>, Jessica Peters<sup>1</sup>, Linda Yang<sup>1,2</sup>, Angela Khera<sup>1,2</sup>, Michael Salzberg<sup>1,2</sup>, Michael Kamm<sup>1,2</sup> and Chamara Basnayake<sup>1,2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Disordered eating (DE) in gastrointestinal (GI) clinics is highly prevalent but not well-characterised. Specific eating disorders like avoidant/restrictive food intake disorder (ARFID) and orthorexia nervosa have not been adequately studied in this population. This study aimed to evaluate the prevalence and characteristics of DE in GI patients, with a focus on ARFID and orthorexia, using screening tools, across organic GI disorders, disorders of gut-brain interaction (DGBI), and controls.</p><p><b><i>Methods:</i></b> Consecutive patients at a single tertiary centre, from September 2022 to October 2023, were invited to complete an online questionnaire post clinic appointment. Patients with a GI disorder were invited if they had “organic” disease (inflammatory bowel disease (IBD) and/or coeliac disease), or DGBI, as per Rome IV criteria. Controls were defined as asymptomatic patients presenting for surveillance of polyps, positive faecal occult blood testing or those with H. pylori infection. The 63-item questionnaire included screening tools for ARFID (NIAS, EDY-Q), orthorexia nervosa (ORTO-7), GI-symptom specific anxiety (VSI), quality of life (EQ-5D-5L VAS), depression and anxiety (PHQ-4). DE is defined according to self-reported eating disorder (ED), recorded ED diagnosis on file, or established ED screening tool cut-off scores (NIAS: item 1-3 ≥ 10, and/or item 4-6 ≥ 9, and/or item 7-9 ≥10; EDY-Q: at least one of item 2, 10, 12 ≥ 4, and item 4 ≥ 4; ORTO-7 ≤ 19).</p><p><i><b>Results:</b> Demographics:</i> 292 patients completed the questionnaire from 1007 invitations (41.4% male, median age 46). 239 cases had a GI disorder (81.8%) and 53 were controls (18.2%). 64.4% had organic GI disorder (58.9% IBD, 4.5% coeliac disease, 1.0% both) and 17.5% had DGBI. 193 participants (66.1%) had DE; 23.3% with features of ARFID, 12.3% with features of orthorexia, 27.1% with features of ARFID and orthorexia, and 3.8% other. Patients with DGBI had the greatest likelihood of DE (82.4%), followed by organic GI disorder (65.4%) and controls (52.8%) (<i>p</i> = 0.006).</p><p><i>Patients with GI disorders:</i> There was higher DE severity (NIAS <i>p</i> = 0.010; EDY-Q <i>p</i> = 0.030; ORTO-7 <i>p</i> = 0.011), GI-specific anxiety (<i>p</i> < 0.001), lower QoL (<i>p</i> = 0.018), and more food restrictions (<i>p</i> = 0.006) in GI disorders compared to controls, while DGBI patients exhibited even greater DE severity, GI-specific anxiety, depression, anxiety, and lower QoL than both organic disorders and controls (all <i>p</i> < 0.001 for DGBI vs. controls). There was greater GI specific anxiety (<i>p</i> < 0.001) and more food restrictions (<i>p</i> = 0.042) in organic disorders compared to controls.</p><p><i>Patients with disordered eating (DE):</i> There was significantly higher GI specific anxiety, depression and anxiety, GI symptom severity, lower QoL and more food restrictions in those with DE compared to those without DE (all <i>p</i> < 0.001), and particularly in patients with both ARFID and orthorexia compared to those without DE (all <i>p</i> < 0.001). Participants displaying ARFID features had significantly greater GI specific anxiety (<i>p</i> < 0.001), GI symptom severity (<i>p</i> = 0.032) and lower QoL (<i>p</i> < 0.001) compared to those without DE. GI symptom severity was just significantly higher in ARFID than orthorexia (<i>p</i> = 0.049). Participants with DE had significantly higher GI symptom frequency (<i>p</i> = 0.035) and lower BMI (<i>p</i> = 0.046) than those without DE. There was no significant association between DE and GI disease activity or whether patients attended dieticians within the clinics.</p><p><b><i>Conclusion:</i></b> This study reveals a high prevalence and severity of disordered eating, among GI patients who completed an online questionnaire, particularly those with DGBI. DE severity, anxiety, QoL, and food restrictions were also significantly worse in patients with organic disorders and DGBI. These findings suggest that routine screening for DE should be integrated into GI clinics to better identify and manage these disorders. Further studies are required to explore if treatment of comorbid DE improves psychological and GI symptom outcomes for patients.</p><p><b>497</b></p><p><b>Haemosuccus pancreaticus: a rare cause of gastrointestinal bleeding</b></p><p><b>Niamh Buckley</b><sup>1</sup>, Santhi Swaroop Vege<sup>2</sup> and Christopher Blevins<sup>2</sup></p><p><sup>1</sup><i>Royal North Shore Hospital, Sydney, Australia;</i> <sup>2</sup><i>Mayo Clinic Rochester, Rochester, USA</i></p><p><b><i>Introduction:</i></b> Overt obscure gastrointestinal bleeding is a diagnostic challenge frequently faced by clinicians for which the possible etiologies are broad. We describe a rare case of Haemosuccus Pancreaticus occurring in the setting of chronic pancreatitis which should be considered as a differential in the correct clinical context.</p><p><b><i>Case Report:</i></b> We present the case of a 63-year-old man with a sixteen year history of recurrent obscure upper GI bleeding. The pattern of his episodes consisted of intense epigastric pain followed closely by melena which relieved the discomfort. This was often associated with a transient elevation of lipase. They occurred at approximately six month intervals and subsequently increased in frequency to every other month. He underwent extensive investigation which failed to uncover the source of the bleeding including multiple gastroscopies, duodenosocopies, colonoscopies, capsule endoscopies, a CT angiography and a tagged red blood cell study. CT abdomen and pelvis revealed a suspected saccular splenic artery pseudoaneurysm measuring 1.5 cm that abutted the pancreatic duct (Figure 1). There were changes observed that suggested chronic pancreatitis, the likely aetiology of the pseudoaneurysm. This clinical picture was suspicious for haemosuccus pancreaticus and was confirmed with EUS evaluation at the time of bleeding. During the same procedure, five microcoils (Nester 10 mm) were placed via EUS which completely cessated flow in one aspect of the pseudoaneurysm and significantly reduced it elsewhere (Figure 2). However, three days later the patient had melaena and features characteristic of his previous episodes. Repeat CT demonstrated enlargement of the aneurysm and embolization of the splenic artery was performed by interventional radiology. This has thus far been successful, with complete resolution of his symptoms.</p><p><b>References</b></p><p>\\n 1. <span>Han, B</span>, <span>Song, ZF</span>, <span>Sun, B</span>. <span>Hemosuccus pancreaticus: a rare cause of gastrointestinal bleeding</span>. <i>Hepatobiliary Pancreat Dis Int.</i> <span>2012</span>; <span>11</span>(<span>5</span>): <span>479</span>-<span>488</span>.</p><p>\\n 2. <span>Shah, AA</span>, <span>Charon, JP</span>. <span>Haemosuccus pancreaticus, an uncommon cause of upper gastro intestinal bleeding: Case report and review of the literature</span>. <i>J Pak Med Assoc.</i> <span>2015</span>; <span>65</span>(<span>6</span>): <span>669</span>-<span>671</span>.</p><p><b>502</b></p><p><b>Severe idiopathic secretory diarrhoea with a profound sustained response to somatostatin analogues</b></p><p><b>Geovanny Gandy</b><sup>1,2</sup>, Alex Prudence<sup>1,2</sup> and Miriam Tania Levy<sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology Department, Liverpool Hospital, Sydney, Australia;</i> <sup>2</sup><i>University of New South Wales, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Vasoactive intestinal peptide (VIP) secreting tumours are rare neuroendocrine neoplasms that present with chronic secretory diarrhoea and electrolyte derangements, with an incidence of 1 in 10 million people per year.<sup>1</sup> Raised VIP levels and radiological evidence of a lesion, most commonly pancreatic, confirm the diagnosis. However, this can prove challenging, as tumours only transiently secrete VIP and levels may not be elevated between diarrhoeal episodes.<sup>2</sup> We present a case of chronic secretory diarrhoea clinically compatible with a VIPoma, with rapid and sustained response to somatostatin analogue therapy despite negative investigations.</p><p><b><i>Case Report:</i></b> A 35-year-old Vietnamese female presented with progressively worsening non-bloody diarrhoea up to ten times daily, with hypotension and hypokalaemia requiring resuscitation in intensive care, on a background of two years of loose bowel motions. She reported no fevers, infective symptoms, sick contacts, recent antibiotic use, or recent overseas travel. Stool microscopy, extended PCR and cultures were negative; faecal calprotectin and faecal elastase were normal. Thyroid function was normal, tuberculosis gamma interferon assay and coeliac disease serology were negative. Faecal chemistry was consistent with secretory diarrhoea. Panendoscopy was unremarkable and biopsies excluded coeliac disease, microscopic colitis and inflammatory bowel disease. Neuroendocrine screening was negative, including serum VIP 16.9 pmol/L (normal <50 pmol/L). Ga-68 DOTATE PET, multiphase CT, and EUS revealed no lesions. On clinical suspicion of a VIPoma, octreotide was trialled with sustained response and patient was transitioned to lanreotide. Initial cessation of lanreotide precipitated a relapse, but it was weaned successfully after four years.</p><p><b>References</b></p><p>\\n 1. <span>Yao, JC</span>, <span>Eisner, MP</span>, <span>Leary, C</span>, et al. <span>Population-based study of islet cell carcinoma</span>. <i>Ann Surg Oncol.</i> Dec <span>2007</span>; <span>14</span>(<span>12</span>): <span>3492</span>-<span>500</span>. https://doi.org/10.1245/s10434-007-9566-6</p><p>\\n 2. <span>Ma, ZY</span>, <span>Gong, YF</span>, <span>Zhuang, HK</span>, et al. <span>Pancreatic neuroendocrine tumors: A review of serum biomarkers, staging, and management</span>. <i>World J Gastroenterol</i> May 21 <span>2020</span>; <span>26</span>(<span>19</span>): <span>2305</span>-<span>2322</span>. https://doi.org/10.3748/wjg.v26.i19.2305</p><p><b>511</b></p><p><b>Decoding gastrointestinal symptoms in systemic sclerosis: a cluster analysis of a large national prospective systemic sclerosis cohort</b></p><p>Alexander Strathmore<sup>1</sup>, Dylan Hansen<sup>1</sup>, Kathleen Morrisroe<sup>1,2</sup>, Alannah Quinlivan<sup>1,2</sup>, Susanna Proudman<sup>4</sup>, Jennifer Walker<sup>5</sup>, Joanne Sahhar<sup>3</sup>, Gene Siew-Ngian<sup>3</sup>, Lauren Host<sup>6</sup>, Wendy Stevens<sup>1</sup>, Mandana Nikpour<sup>1,2,7</sup>, Laura Ross<sup>1,2</sup> and <b>Chamara Basnayake</b><sup>1,2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>University of Melbourne, Melbourne, Australia;</i> <sup>3</sup><i>Monash University, Melbourne, Australia;</i> <sup>4</sup><i>Royal Adelaide Hospital, Adelaide, Australia;</i> <sup>5</sup><i>Flinders Medical Centre, Adelaide, Australia;</i> <sup>6</sup><i>Fiona Stanley Hospital, Perth, Australia;</i> <sup>7</sup><i>Royal Prince Alfred Hospital, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal disease (GI) is present in over 90% of patients with systemic sclerosis (SSc). As the most common organ manifestation, it causes significant morbidity and has a negative impact on quality of life. There exists substantial heterogeneity in the presentation of GI manifestations of SSc. The aim of this study was to evaluate whether there is clustering of GI symptoms in SSc, and whether these clusters have prognostic implications.</p><p><b><i>Methods:</i></b> Adult patients (age ≥18 years) enrolled in the Australian Scleroderma Cohort Study (ASCS) with at least two study visits between 2007-2023 were eligible for inclusion. All patients had definite SSc, as defined by the 2013 ACR/EULAR classification criteria. Clinical data and patient-reported outcomes (PROMs) including HAQ-DI and UCLA GIT 2.0 Score, measuring physical function and GI severity, were collected annually. Seven variables were chosen and hierarchical cluster analysis with Jaccard similarity was performed using Ward’s linkage to identify subgroups. Univariate analysis with chi-square, ANOVA and Kruskal-Wallis rank tests, as appropriate, were performed to describe the differences between each subgroup. Kaplan-Meier survival analysis was performed to compare overall survival.</p><p><b><i>Results:</i></b> A total of 1,652 patients were included, 85.6% female with median follow-up of 4.47 (IQR 2.86-9.2) years. Clustering of patients based on GI symptoms identified four subgroups. We observed clustering based on frequency and severity of GI symptoms. This linked to disease duration. Longer disease duration was associated with more frequent and more severe GI involvement. More frequent GI symptoms were associated with poor physical function. There was no clustering of GI symptoms based on anatomical GI tract location. Cluster 1 (n=1116) was the largest cluster characterised by a high frequency of all GI symptoms, and was characterised by vomiting and faecal incontinence. Patients in Cluster 1 reported more severe GI disease (UCLA-SCTC GIT 2.0 score) and significantly impaired physical function (HAQ score) compared to Clusters 2-4. Cluster 3 and 4 were characterised by the absence of multiple GI manifestations. Survival analysis demonstrated better long-term survival in patients with severe GI manifestations (Cluster 1) compared to Clusters 2 and 3; perhaps accounted for by the lower prevalence of cardiopulmonary complications in Cluster 1.</p><p><b><i>Conclusion:</i></b> This large SSc cohort demonstrates that GI symptoms do not cluster into discrete upper and lower GI subgroups. Subgroups exist, with clear distinctions in frequency and severity of GI symptoms. Severe GI symptoms throughout the GI tract are a feature of longer disease duration and associated with significantly impaired physical function.</p><p><b>524</b></p><p><b>Surgery for non-malignant polyps continues to cause avoidable morbidity: Findings from a western cohort</b></p><p><b>Anthony Whitfield</b><sup>1,2</sup>, Julia Gauci<sup>3</sup>, Clarence Kerrison<sup>3,2</sup>, Sunil Gupta<sup>3,2</sup>, Oliver Cronin<sup>3,2</sup>, Timothy O'Sullivan<sup>3,2</sup>, Varan Perananthan<sup>3,2</sup>, Hunter Wang<sup>3,2</sup>, Francesco V Mandarino<sup>3</sup>, Brian Lam<sup>3</sup>, Eric Lee<sup>3,2</sup>, Nicholas Burgess<sup>3,2</sup> and Michael J Bourke<sup>3,2</sup></p><p><sup>1</sup><i>Blacktown Hospital, Sydney, Australia;</i> <sup>2</sup><i>Westmead Clinical School, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Westmead Hospital, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Most non-malignant colorectal polyps (NMCPs) can be removed endoscopically with minimal morbidity and negligible mortality. Despite this, a high rate of surgical resection still occurs in western populations resulting in avoidable cost to the patient and to the health budget. To establish better pathways for endoscopic resection of NMCPs in Australia, we sought to understand the prevalence and outcomes of surgery in a state-wide representative sample.</p><p><b><i>Methods:</i></b> A linked dataset provided by the Centre for Health Record Linkage (CHeReL), which included all admissions for surgery in patients aged 18 and over in New South Wales (NSW) between July 2007 and December 2017 was analysed. Australian classification of health interventions (ACHI) codes were used to filter the data set for colorectal surgery and International classification of diseases (ICD) codes were used to identify cases with a primary diagnosis of NMCP or colorectal cancer (CRC). Emergency surgery, inflammatory bowel disease and cases of total colectomy were excluded. Trends over two time periods (2008-2012 and 2013-2017) were compared. Major adverse events including mortality were captured 30 days from index surgery. Logistical regression was used to estimate risk ratios and 95% confidence intervals.</p><p><b><i>Results:</i></b> From July 2007 - December 2017, 36,257 surgeries for NMCP and CRC were performed in NSW. 4181 (11.4%) were performed for NMCP. Excluding the rectum, NMCPs accounted for 16.4% of surgery for neoplasia. 51.1% (2137/4181) were performed in private hospitals. Between 2008-2012 and 2013-2017 there was no major difference in volumes of surgery for NMCPs (2008-2012,1968 cases; 2013-2017, 1948 cases; p=0.774). No significant differences were observed (p=0.708) and this remained the case for all subgroups: teaching hospital vs non and major city vs regional. A major adverse event was encountered in 19.3% of surgery for NMCPs (808/4181). Predictors for major adverse event included age, male sex, rectal surgery, American society of anaesthesiologists physical classification system (ASA) III & IV and laparotomy. Full cover health insurance was a negative predictor (OR 0.72, p=0.05, 95% CI 0.52-0.99). Mean length of stay was 12.8 days when a major adverse event occurred compared to 6.9 days when one did not (p=<0.001).</p><p><b><i>Conclusion:</i></b> Surgery for NMCPs occurs at unacceptable rates in Australian Hospitals resulting in avoidable morbidity. Endoscopic resection pathways are required within public and private hospitals to address these avoidable poor outcomes for patients with NMCPs. Streamlining these patients to endoscopic resection will reduce inpatient workloads and associated health care costs.</p><p><b>529</b></p><p><b>Patients with functional gastrointestinal disorders spend less time in tertiary care when managed by a single clinician: Results of a multi-centre audit in South Australia</b></p><p><b>Ryan M Mathias</b><sup>1,2,3</sup>, Samantha Plush<sup>1,2</sup>, Elka Fairhead<sup>4</sup>, Benjamin Ngoi<sup>2,3</sup>, Louisa Edwards<sup>3</sup>, Alice Day<sup>1,2,3</sup> and Robert Bryant<sup>1,2,3</sup></p><p><sup>1</sup><i>Inflammatory Bowel Disease Service, The Queen Elizabeth Hospital, Adelaide, Australia;</i> <sup>2</sup><i>School of Medicine, The University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>4</sup><i>Department of Dietetics, The Queen Elizabeth Hospital, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Functional gastrointestinal disorders (FGID) are a group of disorders that manifest with abdominal symptoms. FGiDs have a serious impact on quality of life and represent a significant global burden on healthcare services. Guidelines now recommend an early, positive diagnosis in low-risk patients to reduce the risk of over-investigation. Establishing a strong clinician-patient relationship is a cornerstone of management. This requires both confidence in management and consistent messaging. The aim of this study was to identify factors that may contribute burden on two tertiary gastroenterology services.</p><p><b><i>Methods:</i></b> This multi-centre, retrospective chart review of electronic medical records evaluated adults attending general gastroenterology outpatient clinics at two teaching hospitals. Occasions of service (OOS) were characterised as being seen by either a single clinician or discontinuous care. Discontinuous care was defined as multiple clinicians of varying seniority reviewing the same patient from first encounter during their time in service. Time to diagnosis and discharge, OOS per patient and number of harmful investigations were assessed. A harmful investigation was defined as one that involved either an invasive procedure such as endoscopic assessment or ionising radiation. Statistical analysis was performed with ANOVA, Kaplan-Meier plots and multiple logistic regression analysis.</p><p><b><i>Results:</i></b> 275 patients (mean age 49 (SD 18), 72% female) were seen primarily for FGID between June 2021 - June 2022. When comparing single clinicians and discontinuous care, there was a protracted time to diagnosis between (42 vs 140 days, p<0.001) and time to discharge (158 versus 356 days, p<0.0001). Patients were more likely to receive a diagnosis early (HR 1.6, 95% CI 1.25; 2.04) and be discharged sooner (HR 1.83, 95% CI: 1.44,2.33) when seen by single clinicians compared with discontinuous care. Patients who received an early diagnosis by a single clinician spent less time in service following their diagnosis (80 days [IQR 0-183]) compared to those who experienced discontinuous care (378 days [IQR 217-616]); p<0.0001. There was a trend towards less harmful investigations in the single clinician group versus discontinuous care group (p=0.08).</p><p><b>530</b></p><p><b>Error and underestimation: capturing psychiatric complexity in disorders of gut-brain interaction</b></p><p><b>Paris Hoey</b><sup>1,3</sup>, <b>Lynne Heyes</b><sup>2</sup> and Trina Kellar<sup>1,3</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Department of Consultation-Liaison Psychiatry, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>3</sup><i>Faculty of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Disorders of gut-brain interaction (DGBI) are common, affecting 37.7% of Australians [1]. DGBI arise from past and present psychosocial stressors, via a complex interplay of nervous system, immune dysfunction, microbiome and mucosal-barrier dysfunction [2]. Whilst the prevalence of comorbid psychiatric disorders in DGBI is well established, medical literature oversimplifies the psychiatric profile of this population. Most studies use anxiety and depression self-reported screening measures for diagnosis [1]. Further, GI-psychologists and psychiatrists are few in medical services, leaving diagnosis to the primary physician. Post-traumatic stress disorder (PTSD), complex PTSD (C-PTSD), personality disorders (PD), eating disorders and persistent pain may be missed. We hypothesised that significant psychological factors contributing to complex DGBI were undiagnosed, thus untreated, in our cohort. This study aimed to compare the psychiatric profiles of patients with DGBI, pre- and post-psychologist formulation.</p><p><b><i>Methods:</i></b> Retrospective cohort study, in a metropolitan tertiary-level adult hospital, specialist multidisciplinary outpatient clinic. Inclusion criteria: consecutive patients who completed full neurogastroenterologist and gastro-psychologist assessment January 2023 to May 2024. Diagnoses were recorded using Rome IV, DSM-5 and ICD-11 diagnostic criteria.</p><p><b><i>Results:</i></b> 21 consecutive patients were included, 76% female, mean age 44. This represents a complex DGBI cohort, 57% had 3+ DGBI diagnoses, most commonly chronic nausea vomiting syndrome (52%), centrally mediated abdominal pain (43%), functional dyspepsia-postprandial distress syndrome (38%), and defecation disorders (33%). Prior to gastro-psychologist assessment, based on referral documentation and patient history, the primary psychiatric diagnosis was anxiety or major depressive disorder in 71% (n=15/21). PTSD in 1/21, C-PTSD 0/21, trauma without PTSD diagnosis 6/21. Active eating disorder 1/21, and PD 0/21. Notably, no psychiatric history was reported by 24%. Vastly more psychiatric complexity was uncovered following gastro-psychologist formulation (Figure 1). All met diagnostic criteria, with 52% suffering 3+ comorbid psychiatric disorders. Importantly, C-PTSD was present in 62%, PTSD 5%. 57% met criteria for active eating disorder (n=12/21), with 11/21 restrictive. PD present in 33%. Persistent pain disorder in 76%.</p><p><b>533</b></p><p><b>A double-blind, placebo-controlled, adaptive dose-response study to assess the acute effects of micro-doses of gluten in adults with treated coeliac disease (Gluten Threshold Study)</b></p><p><b>A James M Daveson</b><sup>1,2</sup>, Emma Craig<sup>1</sup>, Anuj Sehgal<sup>1</sup>, Jennifer Schaefer<sup>1</sup>, Michelle Colgrave<sup>3,4</sup>, Utpal Bose<sup>3,4</sup>, Melinda Hardy<sup>5</sup>, Jason Tye-Din<sup>5,6</sup> and Robert P Anderson<sup>7</sup></p><p><sup>1</sup><i>Wesley Research Institute, Brisbane, Australia;</i> <sup>3</sup><i>CSIRO Agriculture & Food, Brisbane, Australia;</i> <sup>2</sup><i>Coral Sea Clinical Research Institute, Mackay, Australia;</i> <sup>7</sup><i>Mackay Base Hospital, Mackay, Australia;</i> <sup>4</sup><i>ARC CIPPS Edith Cowan University, Perth, Australia;</i> <sup>5</sup><i>Immunology Division, The Walter & Eliza Hall Institute, Melbourne, Australia;</i> <sup>6</sup><i>Department of Gastroenterology, The Royal Melbourne Hospital, Melbourne, Australia</i></p><p><b><i>Background & Aim:</i></b> Evidence supporting a lower limit of gluten consumed in a gluten free diet (GFD) for Coeliac disease (CeD) is controversial. 20 mg per kg (20 parts per million) is accepted globally as the upper limit in gluten free foods except for Australia and New Zealand where “no detectable” gluten is enforced. We recently showed patients with CeD elevate serum interleukin-2 (IL-2) 2 – 6 hours after ingesting ~6 grams of vital wheat gluten (VWG). Reasoning serum IL-2 after a single gluten ingestion could be an objective, quantitative biomarker of gluten toxicity, our aim was to define an upper limit of gluten ingestion that did not elevate IL-2.</p><p><b><i>Methods:</i></b> We performed an adaptive, double-blind, placebo-controlled, dose-ranging safety study at a single site. 51 patients with CeD on a GFD were randomised in 4 sequential cohorts and dosed on three occasions each a month apart. Participants were observed for 6h post ingesting VWG or placebo in gelatin capsules. Cohort 1 received 1000mg gluten protein on 3 occasions as “positive control”. Three subsequent Cohorts were randomised to receive 3 of the 4 sequential dose levels: 610mg, 90mg, 13mg or placebo; 8mg, 5mg, 3mg or placebo; & 3mg, 2mg, 1mg of gluten or placebo. Primary endpoint was the % of IL-2 responders (defined as mean IL-2 at 2, 4 and 6 h more than two standard deviations above the upper limit of normal from the placebo group). Secondary outcomes included symptoms assessed by modified CeD PRO before and hourly post dosing. Faecal and urinary gluten immunogenic peptides (GIP) were exploratory endpoints to assess adherence to GFD.</p><p><b><i>Results:</i></b> The mean age was 53 (F25/M11)<b>.</b> IL-2 levels were significantly elevated in 94% (17/18) of CeD patients after 1000mg gluten; 83% (10/12) after 610mg; 41% (5/12) after 90mg; 38% (5/13) after 13mg; 25% (3/12) after 8mg; 16% (2/12) after 5mg; and 33% (4/12) after 3mg. There were no severe adverse events or significant correlation between dose of gluten and symptoms. All pre food challenge faecal GIPS were negative.</p><p><b><i>Conclusion:</i></b> All dose levels of gluten including <20mg were well tolerated but stimulated IL-2 elevation in CeD patients on a GFD. Low dose gluten challenges with serum IL-2 assessment may be useful for immune monitoring in clinical trials and may inform food regulations and support a no detectable gluten standard. CeD patients are unlikely to be aware of minute dietary exposures to gluten that reactivate gluten-specific immunity.</p><p><b>537</b></p><p><b>Effect of mushroom extract on patients with gastroesophageal reflux disease</b></p><p><b>William Wu</b><sup>1,2</sup>, Jerry Zhou<sup>2</sup> and Vincent Ho<sup>2</sup></p><p><sup>1</sup><i>Ryde Hospital, Sydney, Australia;</i> <sup>2</sup><i>Western Sydney University - School of Medicine, Campbelltown, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastro-oesophageal reflux disease (GORD) is a common condition that significantly impacts quality of life and imposes a substantial economic burden. Conventional treatments often have adverse effects and may not fully control symptoms, leading to interest in alternative therapies. Mushrooms have demonstrated gastroprotective properties in animal models and may offer a natural adjunct treatment for GORD. The aim of this study is to investigate the effects of a mushroom extract on GORD symptoms, quality of life, and biochemical markers in a single-blinded, randomized cross-over study.</p><p><b><i>Methods:</i></b> Participants with confirmed GORD on manometry and ambulatory pH monitoring will be recruited from outpatient clinics. Each participant will receive both the mushroom extract and a placebo for four weeks each, in a randomized order. Symptoms and quality of life will be assessed using validated questionnaires. Blood tests will be performed at set intervals to measure changes in biochemical markers. The study aims to recruit 50 participants which is the sample size calculated to observe a difference of 30% in the proportion of patients with GORD treated for such symptoms and cross-over group non-treated (placebo) considering α = 0.05, and β =0.80.</p><p><b><i>Results:</i></b> This study will provide initial data on the efficacy of mushroom extract in reducing GORD symptoms and improving quality of life. Changes in serum biomarkers will also be evaluated to understand potential mechanisms. This is a pilot study which is currently ongoing, preliminary results should be available at the time of presentation.</p><p><b>554</b></p><p><b>The effects of amyloidosis on the gastrointestinal tract in an Australian population</b></p><p><b>Myo Jin Tang</b>, Nikil Vootukuru, Jason Tjahyadi, Daniel Clayton-Chubb, Olga Motorna, Brendan Wisnioski, Stephen Ting, Stephen Bloom, Simon Gibbs, Rohit Sawhney and Ola Niewiadomski</p><p><i>Eastern Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Gastrointestinal (GI) symptoms are common in systemic amyloidosis with a significant proportion attributed to amyloid deposition in the liver and GI tract. Patients with amyloidosis are also at risk of malnutrition. The aim of this study was to describe the GI and hepatic manifestations in patients with amyloidosis at time of diagnosis and over a follow up period of two years.</p><p><b><i>Methods:</i></b> This was a single centre prospective observational study of patients with newly diagnosed amyloidosis with characterisation at baseline and then follow-up assessments at 6-, 12- and 24-month intervals. Gastric involvement was identified as the key measure due to suspected high prevalence of upper GI symptoms in the amyloid population and availability of a non-invasive diagnostic test. Patients underwent a gastric emptying study (GES), serum biochemistry, micronutrient screening, liver ultrasound (US) and fibroscan at the outlined intervals. A scored patient generated subjective global assessment (PG-SGA) was completed at time of diagnosis to assess nutritional status. Patients over the age of 18 with biopsy proven systemic or localized AL amyloidosis were included. Patients with pre-existing chronic liver diseases or gastrointestinal motility disorders were excluded.</p><p><b><i>Results:</i></b> 16 patients were included in our study; 13 were diagnosed with ATTR and 3 with AL amyloidosis, respectively. The median age was 75 and with 87.5% male. Two patients only had serum biochemistry and micronutrient screening performed. Liver fibrosis was assessed with Fibroscan in 14 patients<b>.</b> The median liver stiffness measurement (LSM) at baseline was 8.4kPa. 10 patients had LSM tracked over the follow up period. 6 patients saw improvement to LSM with treatment while 4 patients saw worsened LSM despite treatment. At baseline, 5/14 patients had normal ALTs (median LSM 7.1(3.7-36.9)kPa) while 9/14 had elevated ALTs (median LSM 9.4(5.4 – 32.9)kPa). In the 9 patients with elevated ALTs, 6/9 saw improvement post treatment, 1/9 had increased ALTs and 2/9 did not have repeat ALTs. 13 patients had liver US performed. At baseline, 9/13 patients had normal liver US (median LSM in these 7.1(3.7 – 32.9)kPa), while 4/13 had hepatic steatosis on US (median LSM in these 12.4(6.8 – 36.9)kPa). In both cohorts, the majority (75% and 71% respectively) saw improvement in LSM after amyloidosis treatment. All 14 patients had normal hepatic synthetic function throughout the follow up period. 12/14 patients had elevated BNPs (which up-trended despite treatment). Four patients (28%) had abnormal GES; two at baseline (1x AL and 1x ATTR) and two developed on follow up (1x AL and 1x ATTR). None of these patients had GI symptoms. Three of these patients had mild gastric emptying delay which did not improve with treatment for their amyloidosis. One patient with ATTR amyloidosis and type 2 diabetes had moderate gastroparesis (on follow up) and did not receive treatment for amyloidosis. An additional two patients had upper GI symptoms but normal GES. Nutritional assessment as per the PG SGA was available in 10 patients. Seven patients were moderately malnourished (Score 4 or higher, category B); three of these patients had an abnormal GES. Micronutrient deficiencies were uncommon with only one patient with iron deficiency at baseline.</p><p><b><i>Conclusion:</i></b> Elevated LSM may be an early indicator of liver involvement given majority saw improvement in LSM post treatment. However, LSM has little relationship with synthetic hepatic function. Malnutrition is prevalent in amyloidosis patients, with delayed gastric emptying a possible contributing factor in some cases only.</p><p><b>573</b></p><p><b>Utility of mean nocturnal baseline impedance in the diagnosis of refractory gastroesophageal reflux disease</b></p><p>Paris Hoey<sup>1,2</sup>, Abdul Raheem Q Khan<sup>1</sup> and <b>Lei Lin</b><sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Faculty of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> The mean nocturnal baseline impedance (MNBI) is a new reflux metric, based on multichannel intraluminal impedance and pH monitoring (MII-pH) which reflects the burden of longitudinal reflux and the integrity of esophageal mucosa. MNBI may be useful in cases where the MII-pH metrics are inconclusive for pathological reflux. Our aim was to assess the diagnostic utility of MNBI in the setting of inconclusive acid exposure time (AET).</p><p><b><i>Methods:</i></b> We retrospectively identified all adult patients who underwent 24-48 hours pH impedance monitoring (Laborie and Medtronic) off Proton pump inhibitors (PPI) between January 2023 to May 2024 at two Brisbane metropolitan hospitals to investigate refractory reflux symptoms that did not adequately respond to PPI. MNBI was measured at the 5-cm impedance channel from three separate nocturnal 10-minute time periods. As per Lyon Consensus 2.0, we defined MNBI as positive when <1500 ohm, as inconclusive when between 1500-2500, and as negative when >2500 ohm. We defined AET as pathologic when >6%, as physiologic when <4%, and as inconclusive when between 4%–6%. Total reflux episodes (TRE) were defined as negative when <40/day, as inconclusive when between 40–80/day, and as positive when >80/day. The primary outcome was the rate of positive MNBI in patients with inconclusive AET to determine the yield of MNBI as an adjunctive evidence of reflux metric in the setting of diagnostic uncertainty.</p><p><b><i>Results:</i></b> 86 adult patients were included in the analysis, with an average age of 54 years, and female prevalence of 69%. There was moderate correlation between MNBI and AET in our cohort with R= -0.46 (linear regression, p <0.001), but the correlation between MNBI and TRE was not strong (R=0.21, p=0.05). In seven patients with inconclusive AET on pH-impedance testing, application of MNBI led to a diagnosis of pathologic acid exposure in four patients (57%). In three patients with both inclusive AET and inconclusive TRE, application of MNBI led to a diagnosis of pathologic acid exposure in 2 patients (67%).</p><p>\\n \\n </p>\",\"PeriodicalId\":15877,\"journal\":{\"name\":\"Journal of Gastroenterology and Hepatology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2024-09-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16704\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Gastroenterology and Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16704\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16704","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
138 基于血液的新型细胞因子释放测定显示,即使在严格遵守无麸质饮食的人群中,也能对乳糜泻的诊断显示出较高的灵敏度和特异性Olivia Moscatelli1、Amy Russell1、Lee Henneken2、Linda Fothergill1、Hugh Reid3、Jamie Rossjohn3、Melinda Hardy1、Vanessa Bryant1 和 Jason Tye-Din11Walter and Eliza Hall Institute,澳大利亚墨尔本;2 澳大利亚墨尔本皇家医院;3 澳大利亚墨尔本莫纳什大学背景与目的:临床实践中的 T 细胞诊断仅限于结核病,但如果 T 细胞诊断更灵敏的话,最终可用于替代组织学诊断抗原驱动的免疫性疾病,如乳糜泻(CD)。目前对 CD 的诊断并不理想。对于已经采用无麸质饮食(GFD)的患者来说,为确诊而进行的长时间麸质挑战往往耐受性很差。检测麸质特异性 CD4+ T 细胞对 CD 诊断很有吸引力,但像 HLA-DQ-麸质四聚体这样的复杂技术并不实用。我们最近发现血清白细胞介素(IL)-2 对麸质的释放是麸质特异性 T 细胞的标记。我们的目的是评估采用 "管内麸质挑战 "的 IL-2 全血测定(WBA)的诊断性能,并将其与口服麸质和四聚体分析后的血清 IL-2 水平进行比较:对 79 名 CD 成人(71 名服用 GFD 且 CD 血清学阴性,8 名食用麸质;75 名 HLA-DQ2.5)和 92 名非 CD 成人(34 名服用 GFD 且自我报告为非乳糜泻性麸质敏感,NCGS,58 名健康对照组食用麸质;35 名 HLA-DQ2.5)进行了 IL-2 WBA 评估。新鲜血液与麸质肽培养 24 小时,然后评估 IL-2(MesoScale Discovery)。在单次10克麸质挑战后0小时和4小时评估血清IL-2水平,并评估治疗CD和NCGS队列中的四聚体频率:IL-2 WBA检测CD的准确性很高:灵敏度为85%(67/79),特异性为97%(89/92),AUC=0.93。当排除非典型HLA-DQ8基因型的CD患者时,灵敏度增加到88%(67/76)(AUC=0.95)。IL-2 WBA反应与麸质诱导的血清IL-2(n=50,r=0.65,p <0.0001)和每百万CD4+ T细胞中麸质四聚体+肠道归巢T细胞的频率(n=10,r=0.9,p <0.0001)相关。当四聚体频率低至每百万 CD4+ T 细胞 1 个时,IL-2 WBA 呈阳性。较高的基线 IL-2 WBA 与麸质挑战后的呕吐有关:结论:IL-2 WBA 的灵敏度极高,相当于在 4 毫升血瓶中检测到一个麸质特异性 T 细胞。它是一种简单的管式检测方法,需要 10 毫升全血,可预测麸质诱发症状的严重程度。它对 CD 的诊断准确率很高,其重要优点是可以检测出转谷氨酶-IgA 阴性的 GFD 患者的 CD。正在进行的改进旨在提高诊断灵敏度。IL-2 WBA 有可能彻底改变 CD 诊断,并克服目前 CD 血清学和组织学的局限性:中性粒细胞减少性肠炎(NEC)是一种严重的危及生命的疾病,其特征是肠壁炎症性坏死,多见于中性粒细胞减少的患者。NEC 中的肠壁炎症会发展为溃疡和坏死,如果不及时处理,可能会导致肠穿孔。目前还没有因使用硫酰胺和甲状腺风暴患者继发 NEC 的病例报告:一名三十多岁的年轻女性最近被诊断患有巴塞杜氏病,并服用了甲巯咪唑,最近从泰国返回后因发烧、腹痛和腹泻到医院就诊。她发热达 38.8°C,心动过速达 140 bpm,血压为 105/56 mmHg。她的检查结果为眼球突出、可触及巨大甲状腺肿和扁桃体肿大。她的绝对中性粒细胞计数为 0.00x 10^9/L(2.5-7x 10^9/L),游离 T4 为 63.5 pmol/L(10-20 pmol/L),游离 T3 为 28.9 pmol/L(2.8-6.8 pmol/L),促甲状腺激素为 0.00 mU/L(0.50-4.00 mU/L)。她的表现与因使用硫酰胺治疗巴塞杜氏病而继发的粒细胞减少以及细菌性扁桃体炎引起的甲状腺风暴一致。由于她无法使用其他抗甲状腺药物来治疗甲状腺风暴,因此治疗过程非常复杂。因此,她接受了静脉输液、广谱抗生素和粒细胞集落刺激因子(G-CSF)治疗细菌性扁桃体炎和中性败血症。在等待甲状腺切除术期间,她使用了鲁戈尔碘、糖皮质激素和普萘洛尔来控制甲状腺风暴。入院第10天,她出现剧烈腹痛并伴有便血。经检查,她患有腹膜炎。
Safety, efficacy and tolerability of an ultra-low volume bowel preparation (NER1006) – a real world experience
Anthony Sakiris, Arvinf Rajandran, Jane Lynch, Myles Rivlin and Sneha John
Gold Coast University Hospital, Gold Coast, Australia
Background and Aim: Endoscopic assessment with colonoscopy allows for the detection of polyps and adenomas which are precursors to colorectal adenocarcinoma. The quality of bowel preparation is of significant importance to the outcome of a colonoscopy as poor bowel preparation results in prolonged procedure times, the need for repeat procedures and missed lesions. A split-dose regimen of 3-4L Polyethylene Glycol (PEG) has historically been the recommended form of bowel preparation. NER1006 is a 1L split-dose PEG bowel preparation that is comparatively novel to Australia and has been adopted within our service since 2020. NER1006 provides enhanced osmotic activity from the high-dose ascorbate that is present in the second dose. Given its ultra-low volume, the aim of this study was to assess the safety, efficacy and tolerability of NER1006 in a real-world setting within our hospital network.
Methods: This study was a retrospective analysis of prospectively collected data for colonoscopy procedures at two centres within our hospital health service. Patients who underwent a colonoscopy between July 2020 and February 2024 and received NER1006 as bowel preparation with a split-dose regime were analysed. The study population consisted of patients who returned a positive faecal occult blood test from the Australian National Bowel Cancer Screening Program (NBCSP) as well as symptomatic patients referred through our nurse-led Direct Access Colonoscopy clinic. The quality of the bowel preparation was quantified through the Boston Bowel Preparation Scale (BBPS). The Polyp Detection Rate (PDR), Adenoma Detection Rate (ADR), Sessile Serrated Lesion Detection Rate (SSLDR) and Advanced Adenoma Rate (AADR) were also calculated as quality indicators of colonoscopy. Adverse events related to NER1006 were classified as either minor or major. Major adverse events were defined as those requiring hospitalisation or those that prevented the patient from adequately completing their bowel preparation.
Results: A total of 2920 colonoscopies were performed on 2874 patients. There were 1571 males, 1301 females and 2 indeterminate with a mean age of 57 years. 2827/2920 (97%) of the colonoscopies performed produced a BPPS score equal to or greater than 6 (good or excellent), with an average score of 7.90. Analysis revealed a 72% PDR, 55% ADR, 16% SSLDR and 25% AADR. There were 2 cases (0.07%) of major adverse events. One patient was unable to complete their bowel preparation due to vomiting and one patient presented with an acute kidney injury. There 98 cases (3.36%) of minor adverse events. Tachycardia (>100 bpm) was the most common minor adverse event and involved 48 patients (2%). Nausea was the second most reported minor adverse event and occurred in 29 patients (1%) with only 10 cases (0.3%) associated with vomiting. 17 patients (0.6%) noted mild to moderate abdominal pain. Other non-specific minor adverse events involving 4 patients (0.14%) included headache and dizziness.
Conclusion: This study highlights that a split-dose regime of NER1006 is a safe, effective and tolerable bowel preparation. Our utilisation of NER1006 surpasses the 90% standard for adequate bowel preparation suggested by the Quality Committee of the European Society of Gastrointestinal Endoscopy. Established targets of a 40% PDR and a 25% ADR were also exceeded in our population. In our real-world experience, only a small minority of patients who were administered NER1006 exhibited adverse effects. Clinical dehydration due to NER1006 has been demonstrated in previous studies and may have been a contributor for our patients with tachycardia. However, other factors such as anxiety should also be considered. The implementation of multimodal education regarding the process of bowel preparation has assisted in enhancing the overall safety and tolerability of NER1006 within our network. Instructions for our patients to sip the bowel preparation slowly through a straw to minimise taste, drinking clear savoury fluids to offset the sweetness of NER1006 and ensuring adequate clear fluid intake have all been suggested strategies. This is the largest study regarding ultra-low volume bowel preparation reported within the Australian context, however it is limited by its retrospective model. Larger multi-centre prospective studies are recommended to further identify the factors that contribute towards the potential adverse effects of ultra-low volume bowel preparation in order to better prevent or manage them.
9
The presence of hiatal hernia is a significant predictor for symptomatic recurrence after cessation of vonoprazan therapy for gastroesophageal reflux disease: A long-term observational study
Satoshi Shinozaki1, Hiroyuki Osawa2, Yoshimasa Miura3, Hirotsugu Sakamoto2, Yoshikazu Hayashi2, Tomonori Yano2, Edward Despott4 and Hironori Yamamoto2
1Shinozaki Medical Clinic, Utsunomiya, Japan;2Jichi Medical University, Shimotsuke, Japan;3Nihon University, Chiyoda, Japan;4Royal Free Hospital, London, UK
Background and Aim: Gastroesophageal reflux disease (GERD) symptoms frequently recur after cessation of acid blockers. The presence of a hiatal hernia may worsen GERD symptoms and increase the risk of esophageal malignancy. The aim of this study is to clarify the timing and predictors for recurrence of GERD symptoms after cessation of vonoprazan (VPZ) therapy.
Methods: A retrospective observational study involved 86 patients who underwent cessation of VPZ therapy for symptomatic GERD. Collated data from medical record review included the endoscopic findings and Izumo scale score.
Results: The mean duration of continuous VPZ therapy before cessation was 7.9 months. GERD symptoms requiring the resumption of VPZ therapy recurred in 66 of 86 patients (77%). Kaplan-Meier analysis showed that overall recurrence-free rates at 6 months, one and two years after VPZ cessation were 44%, 32% and 23%, respectively. Alcohol use, the presence of a hiatal hernia and long-term therapy for more than six months were identified as significant positive predictors for symptomatic recurrence. Notably, hiatal hernia had the highest hazard ratio in both univariate and multivariate analyses. The recurrence-free rate in patients with a hiatal hernia was much lower at 6 months than in patients without a hiatal hernia (15% and 51%, respectively p=0.002). After the symptomatic recurrence, GERD symptoms improved significantly after one-month VPZ therapy.
11
Establishment of a tertiary faecal microbiota transplant service and 24 month outcomes
Emma Buckner1,2 and Thomas Goodsall1,2
1Department of Gastroenterology, John Hunter Hospital, Newcastle, Australia;2School of Medicine and Public Health, The University of Newcastle, Newcastle, Australia
Background and Aim:Clostridium difficile infection (CDI) is the most common cause of nosocomial diarrhoea in Australia and results in morbidity, risk of mortality, increased length of admission and resource utilisation. Recurrent CDI risk after antibiotic treatment is 20% and morbidity and mortality risk increase to 26-36% after first recurrence. Faecal Microbiota Transplant (FMT) is recommended in Australia as the preferred management for second and subsequent recurrences of CDI and is effective in 90% of cases after one FMT and 98% after a second FMT. We report our experience introducing an FMT service to a tertiary hospital and report the 24-month patient outcomes.
Methods: A business case was prepared and submitted to the New Interventional Procedures and Quality use of Medicines committee at our hospital for introduction of an FMT service using TGA approved stool sourced from a third-party Australian provider (BiomeBank, Adelaide, South Australia). Successful approval was granted based on supporting evidence for efficacy and safety, proposed use of TGA approved stool product, limited scope of practice to recurrent or refractory CDI, structured supervision and accreditation program with audit and governance oversight, a cost analysis demonstrated cost benefit of FMT compared with antibiotic therapy, and supply of a -80 degree freezer for local storage of donor stool product.
Results: 21 FMT procedures were performed in 17 patients. Demographics and outcomes are presented in Table 1. Complete remission was achieved in 14/17 patients (82%) after the first FMT and of the three patients requiring repeat FMT, one achieved remission after the second FMT, one required colectomy for persistent C. difficile colitis and megacolon, and one experienced ongoing recurrence in the setting of prophylactic antibiotics for lung transplant. Another patient was diagnosed with intercurrent Crohn’s colitis at the time of FMT and required colectomy for refractory Crohn’s colitis despite steroids and infliximab 4 weeks after FMT; the stool was C. difficile PCR negative and there was no histological evidence of persistent C. difficile infection. One other patient had deep ileocolonic skip ulcers consistent with Crohn’s disease and responded to FMT and induction steroids, while another had endoscopic and histological evidence of ulcerative proctitis which clinically responded to FMT and was in clinical and biomarker remission at 6 months. One patient experienced persistent diarrhoea after FMT despite clearance characterised by negative stool PCR and was subsequently diagnosed with a duodenal neuroendocrine tumour requiring Whipple’s resection.
Conclusion: A funded FMT model was successfully introduced at our hospital with Clinical Governance approval. Primary response and cure was achieved in 88% of patients consistent with published outcomes. IBD was diagnosed in 3/17 patients at the point of FMT and cured in one case. Risk factors for requiring subsequent FMT were severe CDI with colitis and ongoing antibiotic use. No significant adverse events or deaths were directly attributable to FMT. This model could be reproduced to support other centres wanting to introduce an FMT service to provide quality evidence-based care.
18
Haemosuccus pancreaticus: an interesting and rare presentation of upper gastrointestinal bleeding
Annabelle Faint1, Laurence Vaitiekunas1,4, Muddassir Rashid2, Arjuna Somasundaram2 and Alexander Huelsen1,3
1Digestive Health, Gold Coast University Hospital, Gold Coast, Australia;2Department of Radiology, Gold Coast University Hospital, Gold Coast, Australia;3School of Medicine, University of Queensland, Gold Coast, Australia;4School of Medicine and Dentistry, Griffith University, Gold Coast, Australia
Introduction: Haemosuccus pancreaticus (HP) is a rare and life-threatening cause of upper gastrointestinal bleeding and is characterised by haemorrhage into the main pancreatic duct.1,2 HP has a mortality rate of up to 9.6%.3 Typically associated with chronic pancreatitis, HP arises from prolonged enzymatic exposure of peripancreatic arterial walls, precipitating a bleeding event that fistulsed into the pancreatic ductal system.4 Clinical manifestations include haematemesis, melaena, abdominal pain, and in severe cases, haemodynamic instability. Diagnostic challenges can often arise due to the failure of initial endoscopic evaluation to identify a source of bleeding, compounded by a general lack of familiarity and awareness of this entity.1,2 Computed tomography angiography (CTA) remains the gold standard for diagnosis and can guide management which includes angiographic embolisation and surgery. Surgical treatment is typically reserved for uncontrolled haemorrhage or when embolisation fails.2 We describe a case of a 29-year-old male with a background of chronic pancreatitis and pancreatic pseudocyst (PC), exhibiting clinical manifestations indicative of haemosuccus pancreaticus, wherein a distal splenic artery pseudoaneurysm had bled into a pancreatic pseudocyst and the pancreatic ductal system. This was treated successfully by angiographic embolisation of the splenic artery.
Case Report: A 29-year-old male with a history of alcohol-related chronic pancreatitis and an 8cm pancreatic tail pseudocyst presented with a two-day history of hematemesis, melaena, and epigastric pain. He reported abstinence from alcohol for several months and he denied smoking and the use of anti-inflammatory medications. His last gastroscopy in 2022 showed chronic gastritis only. On examination, he was pale with a soft abdomen demonstrating severe epigastric tenderness. There was no melaena on rectal examination. He was tachycardic to 116bpm and his blood pressure was 124/64 mmHg. Biochemistry revealed a hemoglobin of 37g/L, ferritin 2ug/L, urea of 1mmol/L, total bilirubin 5umol/L, ALP 92U/L, GGT 257U/L, ALT 16U/L, AST 25U/L. Resuscitation with four units of packed red blood cells and intravenous fluids stabilised his condition. His haemoglobin incrementally increased to 71g/L without evidence of ongoing gastrointestinal bleeding during his admission. Urgent gastroscopy demonstrated gastric erythema and small erosions in the antrum, without stigmata of recent bleeding. A subsequent abdominal CTA showed a 7 x 6mm distal splenic artery pseudoaneurysm projecting inferiorly into a large, longstanding pseudocyst posterior to the pancreatic tail, not identifiable on initial contrast CT abdomen. On comparison with prior imaging, the PC had developed intracystic high density material, in keeping with interval haemorrhage (Image 2). Angiographic embolisation with three 5mm microcoils to the lower pole branch of the splenic artery was successful (Image 4). He remained clinically stable following the procedure and was discharged after a period of inpatient observation.
References
1. Alshaikhli, A, Al-Hillan, A. (2023). Haemosuccus Pancreaticus. StatPearls. Treasure Island (FL). StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK570570/
2. Yashavanth, H. S., Jagtap, N., Singh, J. R., Ramchandani, M., Lakhtakia, S., Tandan, M., Gupta, R., Vamsi, M., Bhaware, B., Rao, G. V., and Reddy, D. N. (2021) Hemosuccus Pancreaticus: A systematic approach. Journal of Gastroenterology and Hepatology, 36: 2101–2106. https://doi.org/10.1111/jgh.15404.
3. Yu, P, Gong, J. Hemosuccus pancreaticus: A mini-review. Ann Med Surg (Lond). 2018; 28: 45-48. Published 2018 Mar 9. https://doi.org/10.1016/j.amsu.2018.03.002
4. Mekheal, N., Roman, S., Alkomos, M. F., Mekheal, E., Farokhian, A., Millet, C., Shah, H., Melki, G., & Baddoura, W. (2022). Hemosuccus Pancreaticus: Challenging Diagnosis and Treatment. European Journal of Case Reports in Internal Medicine, 9(5), 003337. https://doi.org/10.12890/2022_003337
39
Comparative evaluation of Atmo Gas Capsule System and SmartPill GI Monitoring System for transit time assessment in motility disorders
Jerry Zhou1, Allen Lee2, Thomas Abell3, Ashok Attaluri4, Michael Cline5, William Hasler6, Vincent Ho1, Anthony Lembo5, Amir Masoud7, Richard McCallum8, Baharak Moshiree9, Eamonn Quigley10, Satish Rao11, Mayra Sanchez7, Irene Sarosiek8, Abigail Stocker3, Brian Surjanhata12, William Chey2 and Braden Kuo11
1Western Sydney University, Sydney, Australia;2University of Michigan, Ann Arbor, USA;3University of Louisville, Louisville, USA;4Alliance for Multispecialty Research, Kansas City, USA;5Cleveland Clinic, Cleveland, USA;6Mayo Clinic, Scottsdale, USA;7Hartford Health, Fairfield, USA;8Texas Tech University, El Paso, USA;9Atrium Health Wake Forest Medical University, Charlotte, USA;10Houston Methodist Research Institute, Houston, USA;11Augusta University, Augusta, USA;12Massachusetts General Hospital, Boston, USA
Background and Aim: Motility disorders, such as gastroparesis and slow transit constipation (STC), are common gastrointestinal (GI) conditions affecting up to 5% of individuals worldwide. The symptoms of motility disorders can be debilitating, affecting quality of life and driving utilisation of healthcare systems. Diagnosis relies on evaluation of regional transit times, with delayed gastric and colonic transit indicated for gastroparesis and STC, respectively. The SmartPill GI Monitoring System (SmartPill), an FDA-cleared wireless motility capsule (WMC), has been used in the assessment of gastroparesis and STC since 2008 but has recently been discontinued, leaving a need for a like replacement. This study aimed to assess a new WMC, the Atmo Gas Capsule System (Atmo Capsule), against SmartPill for the assessment of regional transit time in these conditions.
Methods: Individuals with upper, lower, or combined GI symptoms were recruited in a prospective multi-centre study. Participants concomitantly ingested the Atmo Capsule and SmartPill in a randomized order. Regional transit times including Gastric Emptying Time (GET) and Colonic Transit Time (CTT) were measured and compared between the devices, where paired data were available. GET >5 hours and CTT >59 hours were defined as delayed.
Results: 213 participants were recruited across 12 sites: 177 yielded paired GET results, and 147 for CTT. Pearson correlation coefficients for GET and CTT comparisons between Atmo Capsule and SmartPill were 0.86 (0.81-0.89) and 0.74 (0.66 – 0.81) respectively. GET demonstrated a positive predicted value (PPV) of 78.00% (SE: 5.86%), negative predictive value (NPV) of 85.83% (SE: 3.09%), and overall agreement (OA) of 83.62% (SE: 2.78%). For CTT, PPV was 67.35% (SE: 6.70%), NPV was 92.89% (SE: 2.60%), and OA was 84.35% (SE: 3.00%). No serious adverse device effects were reported. 32.2% of the total GET evaluable cohort had delayed GET, 27.2% of the CTT evaluable cohort had delayed CTT. For the cohort that had measurement for all transit regions, 20% had delayed CTT only, 11% had delayed GET only and 18% had a delay in multiple GI regions as measured by Atmo.
Conclusion: The Atmo Capsule exhibited substantial agreement with SmartPill in measuring both GET and CTT, highlighting its utility as a potential replacement for the discontinued SmartPill for assessment of motility disorders. Observations of multi-regional dysmotility further highlight the value of measuring multiple regional of the GI tract with a single test.
46
The efficacy of EndoClot® in the prevention of delayed bleeding following advanced endoscopic resection
Anthony Sakiris, Christopher Graddon, Arvinf Rajandran and Sneha John
Gold Coast University Hospital, Gold Coast, Australia
Background and Aims: Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD) are advanced endoscopic techniques that have been increasingly employed for the resection of large precancerous polyps or early gastrointestinal neoplasia. Delayed bleeding is a common adverse event related to endoscopic resection. Modalities such as thermocoagulation with haemostatic forceps and clipping are available options to control bleeding. Recently, topical haemostatic agents have been utilised as an alternative therapy and are applied over the bleeding resection site. EndoClot® is a novel topical haemostatic agent that consists of biocompatible, non-pyrogenic and starched derived polysaccharides. EndoClot® is able to effectively control bleeding by creating a gelled matrix that accelerates the clotting process by concentrating platelets, red blood cells and coagulation proteins at the resection site. The matrix lasts temporarily and can dissipate over a few hours to days. EndoClot® has recently been incorporated within our health network. The aim of our study was to assess the efficacy of EndoClot® in preventing delayed bleeding following the advanced endoscopic resection of high-risk lesions.
Methods: This study was a retrospective analysis of prospectively collected data of advanced endoscopic resections at one centre within our hospital health service. Patients who underwent advanced endoscopic resection between March and April 2024 and received EndoClot® adhesive were analysed. EMR was performed as per standard technique with submucosal injection with gelofusin and methylene blue +\- adrenaline at the endoscopist’s discretion. Indications for EndoClot® use within the colon and rectum included polyps proximal to the splenic flexure greater than 20mm resected with hot-snare EMR and polyps distal to the splenic flexure resected with hot-snare EMR or ESD in high-risk patients (i.e. use of antiplatelets or anticoagulation). Indications for EndoClot® use within the duodenum included polyps greater than 10mm resected with hot-snare EMR and any ampullectomy. Indications for EndoClot® in the oesophagus and stomach included any lesions resected with EMR or ESD in high-risk patients. We recorded basic patient demographics and the use of antiplatelets or anticoagulation. Lesion characteristics such as size, location and histology were documented. Delayed bleeding was defined as clinically evident gastrointestinal bleeding that occurred up to 14 days following the procedure which resulted in an emergency department presentation, required a blood transfusion or a repeat intervention.
Results: EndoClot® was administered following the endoscopic resection of 11 lesions for a total of 10 patients. 90% were male with mean age 67 years (SD 8.62 years). 2 patients (20%) were taking either antiplatelets or anticoagulation. 64% of resections were in the colon or rectum, 27% in the duodenum and 9% in the oesophagus. EMR was the most utilised resection technique (91%). The most common lesion was a tubular adenoma (36%) and 27mm was the mean lesion size resected (SD 11.34mm). There was one delayed post-polypectomy bleed in a patient on Clopidogrel and Warfarin (re-commenced 48 hours post procedure with Enoxaparin bridging), who presented 10 days following a descending colon hot-snare EMR of a 25mm tubular adenoma. This patient underwent a total of 3 subsequent inpatient colonoscopies to definitively control the bleeding over 3 admissions, with evidence of a visible vessel requiring thermal therapy at the second colonoscopy and re-application of EndoClot® during one of the procedures.
Conclusion: Our study demonstrates that EndoClot® is an effective haemostatic agent for the advanced endoscopic resection of high-risk lesions given no evidence of delayed bleeding for patients not on antiplatelet or anticoagulant therapy. Our single delayed bleeding case required 3 subsequent colonoscopy procedures with ongoing bleeding despite thermal therapy, and hence the rebleeding risk would unlikely have been mitigated by use of a topical hemostatic agent. EndoClot® appears to be safe with no noted adverse effects related to its administration. Our study is limited due to its retrospective nature with small sample size. Obtaining data from a larger cohort will enable higher-quality evidence regarding the use of EndoClot®.
54
Delayed autonomic ganglionopathy following nivolumab therapy in a patient with metastatic melanoma
Kai Dong Choong1,2, Aung Du2, Milly Wong1 and Digby Cullen1
1St John of God, Perth, Australia;2Sir Charles Gairdner Hospital, Perth, Australia
Introduction: Immune checkpoint inhibitors (ICI) have shown improved clinical outcomes in several malignancies; however, they have also been associated with immune-related adverse effects (irAE). Neurological irAE, in comparison to other systems are reported to be rare. Alongside clinical scarcity, the mechanisms contributing to neurotoxicity remain poorly understood, rendering diagnosis challenging and requiring a high degree of suspicion. Here, we report a case of delayed autonomic ganglionopathy, likely precipitated by use of ICI, nivolumab.
Case Report: A 76-year-old man presented with diarrhoea, abdominal pain, anorexia, post-prandial fullness, dizziness and 24kg weight loss over 6 months. Significant medical history includes metastatic melanoma treated with nivolumab for one year, completed three months before onset of symptoms. On examination, he appeared cachectic. He was hypertensive (150/94 mmHg), had a regular heart rate (74 bpm) and postural drops of up to 70mmHg. Other examination findings were unremarkable. General haematology and biochemistry revealed hyponatraemia (129mmol/L). Thyroid function tests and screening for endocrine causes were unremarkable. Normal chromogranin-A levels excluded neuroendocrine tumours. Coeliac serology was negative. Stool microbiology was negative for pathogens. Metronidazole challenge did not alleviate gastrointestinal symptoms. Normal faecal calprotectin and C-reactive protein excluded enteral inflammation. Antinuclear antibodies were normal and paraneoplastic screen was also unremarkable. Protein electrophoresis, serum light chains were normal and intestinal biopsy excluded amyloidosis. PET-CT did not detect metastasis. Bedside and stress echocardiography were unremarkable. Gastroscopy unveiled large residual food boluses, suggestive of decreased gastric motility. After exclusion of infective, neoplastic, autoimmune and metabolic causes, we concluded that this was a case of delayed autonomic ganglionopathy secondary to nivolumab. Management focused on symptomatic relief and improving quality of life. Diarrhoea was partially managed by cholestyramine, pancreatic enzymes, loperamide, and domperidone. Abdominal pain was managed with mebeverine in combination with both sublingual and transdermal buprenorphine. Anorexia and post-prandial fullness were managed with nizatidine. Postural hypotension was partially alleviated with midodrine, fludrocortisone and sodium chloride supplements. Recent follow-up included dose adjustments to fludrocortisone and midodrine. Postural hypotension remained but did not precipitate falls or syncope. Diarrhoeal episodes decreased to 4-5 times daily. Our patient regained some independence and was able to engage in social activities.
Conclusion: We report a case of delayed autonomic ganglionopathy caused by use of nivolumab monotherapy. As acute and subacute presentations of neurological irAE are rare, and delayed presentations are exceedingly rare, clinicians ought to maintain a high level of suspicion on patients receiving treatment with ICI.
73
Living with faecal incontinence: A qualitative investigation of patient experiences and preferred outcomes through semi-structured interviews
Sadé Assmann1,2,3, Daniel Keszthelyi2,3, Stephanie Breukink1,3,4 and Merel Kimman5
1Department of Surgery and Colorectal Surgery, Maastricht University Medical Centre +, Maastricht, The Netherlands;2Department of Gastroenterology-Hepatology, Maastricht University Medical Centre, Maastricht, The Netherlands;3Research Institute of Nutrition and Translational Research in Metabolism (NUTRIM), Maastricht University, Maastricht, The Netherlands;4Research Institute for Oncology and Reproduction (GROW), Maastricht University, Maastricht, The Netherlands;5Department of Clinical Epidemiology and Medical Technology Assessment, Care and Public Health, Research Institute (CAPHRI), Maastricht University Medical Centre +, Maastricht, The Netherlands
Background and Aim: Faecal incontinence (FI) is a prevalent and debilitating anorectal problem which can cause embarrassment, anxiety, social isolation and diminishes quality of life (QoL). Currently, there is no optimal treatment option for FI, consequently, treatments primarily focus on symptom reduction and improving QoL. In order to gain a clearer understanding of the challenge’s patients encounter, it is essential to actively listen to patients’ perspectives and experiences, as well as the specific outcomes they aim to achieve from treatment. This study aims to explore how FI impacts patients’ lives and identify important treatment outcomes as part of the development of a Core Outcome Set (COS).
Methods: Patients with FI were recruited from surgery and gastroenterology outpatient clinics in the Netherlands. Semi-structured interviews were performed, audio recorded, transcribed per verbatim and coded. Thematic analysis using the framework method with an inductive open coding approach was performed to identify (sub)themes and categories relevant to the patients.
Results: Twelve interviews were conducted before saturation was reached (75% female, 25% male, mean age 63, range 39-83 year). Four main themes emerged ‘Physical symptoms’, ‘Impact on daily life’, ‘Emotional impact’ and ‘Coping’. Patients expressed how FI severely limits daily activities and emotional wellbeing. Treatment priorities centred on resuming normal activities rather than solely on symptom reduction (table 1).
Conclusion: The impact of FI extends far beyond uncontrolled loss of faeces, affecting psychological, emotional, and social wellbeing. Patients prioritise outcomes focussed on reclaiming normalcy and independence rather than focusing on physical symptoms alone. Integrating these patient-centered outcomes in future studies could enhance treatment satisfaction and patient-perceived treatment success. Furthermore, outcomes identified through this study will be combined with other outcomes identified through literature review, forming a comprehensive list for a Delphi survey with relevant stakeholders to establish a consensus on a final list of outcomes for a COS for FI.
100
Digitally-delivered gut-directed hypnotherapy is superior to an active control program in patients with irritable bowel syndrome: a randomised controlled trial
Ellen Anderson, Simone Peters, Peter Gibson and Emma Halmos
Monash University and Alfred Health, Melbourne, Australia
Background: Face-to-face gut-directed hypnotherapy (GDH) is an effective therapy for irritable bowel syndrome (IBS), but is currently considered third line due to limited accessibility. Nerva is a digitally-delivered GDH program, comprising of psychoeducation (that includes diaphragmatic breathing) and GDH, with the intention to improve access to the IBS population. Efficacy data are limited to a retrospective study, in which gastrointestinal and psychological outcomes improved.
Aim: To perform a single-blinded randomised controlled trial to determine the efficacy of the app-delivered GDH program compared with an active control of psychoeducation alone on gastrointestinal symptoms and psychological outcomes in patients with IBS.
Results: Of 244 enrolled participants, 45 withdrew prior to completing the first 14 sessions. Hence, 199 (96 GDH and 103 Control; median age 37 (IQR 30-46) years and 91% were female) were included in a modified intention to treat analysis. Baseline demographics, gastrointestinal symptoms, psychological indices and QoL were similar between the groups and there was an even distribution of participants from Australia and USA. At the conclusion of the intervention, GDH induced clinical response in 71% compared to 53% with Control (p=0.011; chi-squared). IBS-SSS was a median (IQR) of 200 (131-304) with GDH, which was lower than 246 (165-308) with Control (p=0.032; Mann-Whitney; Figure). This was a reduction of 97 (41-166) for GDH and 57 (0-123) for Control (p=0.008) from baseline. There was a divergence in symptom improvement from 28 sessions (see Figure). Improvement in IBS-VAS pain >30% was reported by 59% with GDH compared to 41% with Control (p=0.009). IBS-QOL improved by 9 (0-27) with GDH compared to 3 (0-15) with Control (p=0.017). Both interventions improved DASS-21and SCL-90 scores similarly. Six months following intervention, 138 (84% GDH and 75% Control) completed symptom measures. The improved IBS-SSS and IBS-VAS pain scores compared with baseline were maintained in those participants (p<0.0001 for both groups), but there were no longer differences between the groups.
Conclusion: The digitally-delivered GDH intervention is superior to psychoeducation alone in alleviating IBS symptoms and in a greater proportion of participants and in improving participant QoL. Benefits appear to be durable. These results support the use of app-delivered GDH (with psychoeducation) that is cheaper and more accessible than in-person therapy for IBS sufferers.
103
Endoscopic intermuscular dissection: blurring the line between endoscopy and surgery
Niroshan Muwanwella1 and Dilini Gunawardena2
1Royal Perth Hospital, Perth, Australia;2PathWest Laboratory Medicine, Perth, Australia
Introduction: Endoscopic Intermuscular Dissection (EID) is a novel endoscopic resection method where a lesion is resected including the inner circular muscle layer of the gastrointestinal tract. Published literature is limited, however shows promising results both as a means of obtaining accurate local staging as well as a curative, organ sparing, endoscopic resection method for T1 rectal malignancies suspicious for deep submucosal invasion (SMI). We present the first Australian report of EID utilised to resect a pT1 malignant rectal polyp with superficial SMI.
Case report: A 70-year-old man was referred for resection of a large rectal polyp. Assessment revealed a 3cm Paris IIa+Is polyp. Kudo pit pattern was type IIIL in the periphery, type IIIS in the centre and a small area with type VI and VN. Imaging classification was malignant polyp suspicious for SMI. Therefore, decision was made to undertake EID to ensure complete (R0) resection. Circumference of the polyp was marked with diathermy. Standard lifting agent consisting of colloid, Indigo Carmine and dilute Adrenaline was injected submucosally into the periphery of the polyp. Using a Dual Knife J (Olympus endoscopy, Tokyo, Japan), mucosa was incised and the submucosa exposed. After applying traction, circular muscle layer was incised to expose intermuscular space. Dissection was performed in this plane and the polyp removed ensuring R0 resection leaving the outer longitudinal muscle layer intact. The defect was left open, intravenous antibiotic administered intra-procedure. Patient made an uneventful recovery and was discharged home the next day on oral antibiotics. Histopathology revealed a 13mm well differentiated invasive adenocarcinoma, pT1, SM1. Deep and circumferential margins were clear and there was no perineural or lymphatic invasion. However, venous invasion and tumour budding was identified. Therefore, patient was referred to colorectal surgical team for a discussion of completion surgery.
Selecting the optimal treatment modality for T1 rectal malignancies suspicious for deep SMI is important to be able to offer patients with organ sparing resections. Available imaging modalities are poor at differentiation between T1 and >T2 cancers. EID bridges a gap in this area. It can offer curative endoscopic resection for a considerable proportion of these patients while providing accurate staging for the remainder, justifying major abdominal surgery.
119
Faecal microbiota transplant in advanced Parkinson's disease, microbial changes and effects on motor and gastrointestinal function: A randomised placebo controlled crossover study
Lucy Bracken1,2, Fiona Tudehope1, William J Ryan3, Scott Read1,4, Duncan Wilson5, Tanya Golubchik6, Brian Gloss7, Sarah Bray5, Laura Williams5, Sophie Waller5, Jessica Qiu5, David Tsui5, Donna Galea5, Neil Mahant5, Hugo Morales Briceno5, Florence CF Chang5,2, Jane Griffith5, Sushil Bandodkar5, Xi Chen5, Victor Fung5,2 and David Van Der Poorten1,2
1Gastroenterology Department, Westmead, Australia;2Faculty of Medicine, University of Sydney, Sydney, Australia;3John Curtin School of Medical Research, Australian National University, Canberra, Australia;4School of Medicine, Western Sydney University, Blacktown, Australia;5Neurology Department, Westmead Hospital, Westmead, Australia;6School of Medical Sciences, University of Sydney, Sydney, Australia;7Westmead Institute for Medical Research, Westmead, Australia
Background and Aim: Preliminary findings from case reports and small human studies suggest that faecal microbiota transplant (FMT) has therapeutic potential in Parkinson’s disease (PD) with effects on both motor and gastrointestinal symptoms. We aimed to determine whether FMT improves motor function, constipation and quality of life in patients with advanced PD and the specific microbiome changes associated with this.
Methods: We conducted a randomised, blinded, placebo-controlled, crossover trial of FMT in patients with PD already on treatment with levodopa/carbidopa via a PEG-J tube. Patients had to be on a stable dose for 6 months and have ≥ 3 hours of OFF time. Patients were randomized 1:1 to FMT or Placebo and received infusions via PEG-J tube on week 0 and 2 and then had crossover therapy on weeks 6 and 8 after a four-week washout. Biomictra FMT (BiomeBank SA) was used with two different donors. The primary outcomes were safety/tolerability of FMT and change in daily OFF time. Secondary outcomes were change in constipation and quality of life (QOL) scores. Microbial composition was assessed at baseline, post FMT/Placebo and end of study and compared to clinical endpoints. Microbiome sequencing was performed on extracted DNA via the Illumina NextSeq 2000 platform. Species classification and analysis was performed using MetaPhlan.
Results: We undertook preliminary analysis after recruiting nine patients who each had completed FMT and placebo infusions. The median age of the patients was 64 with the majority male (78%). There were no serious adverse events recorded. There were three (9%) infusion related blood pressure fluctuations that did not require treatment and six (17%) infusion related episodes of mild abdominal discomfort and bloating split equally between placebo and FMT. Compared to baseline, there was an increase in microbiome richness by Chao1 index post FMT (273 vs 311, p=0.04) and alpha diversity measured by Shannon index (3.89 vs 4.07, p=0.11). The five most common genera at baseline in study patients were Bacteroides, Phocaeicola, Escherichia, Alistipes and Blautia, while in donors it was Bifidobacterium, Phocaeicola, Faecalibacterium, Lachnospiraceae and Bacteroides. Post FMT patients had substantially more Faecalibacterium and Bifidobacterium in keeping with engraftment. Compared to baseline, six patients had improved OFF time, ON time and QOL scores after FMT, but only two had an improvement in constipation. When compared with Placebo, FMT was associated with an absolute reduction in 1.04 OFF hours (p=0.193) and an absolute increase in ON hours by 1.53 (p=0.113). In those with less OFF time and better QOL scores post FMT, baseline microbiome alpha diversity was increased (4.1 vs 3.61, p=0.11), as was post FMT richness (278 v 337, p=0.13). There was no difference in clinical or microbiome outcomes when comparing the two FMT donors.
Conclusions: This preliminary analysis shows FMT in Parkinson’s disease patients via PEG-J tube is a safe and potentially effective treatment. Microbial changes related to richness and diversity appear to be associated with response to therapy. Specific changes at a genera and species level require further characterization.
138
A novel blood-based cytokine release assay shows high sensitivity and specificity for coeliac disease diagnosis even in people following a strict gluten-free diet
Olivia Moscatelli1, Amy Russell1, Lee Henneken2, Linda Fothergill1, Hugh Reid3, Jamie Rossjohn3, Melinda Hardy1, Vanessa Bryant1 and Jason Tye-Din1
1Walter and Eliza Hall Institute, Melbourne, Australia;2The Royal Melbourne Hospital, Melbourne, Australia;3Monash University, Melbourne, Australia
Background and Aim: T-cell diagnostics in clinical practice are limited to tuberculosis but could eventually be used to replace histology in antigen-driven immune diseases, such as coeliac disease (CD), if they were more sensitive. Current diagnosis of CD is suboptimal. For patients already following a gluten-free diet (GFD), prolonged gluten challenge to establish a diagnosis is often poorly tolerated. Detection of gluten-specific CD4+ T cells is attractive for CD diagnosis but sophisticated techniques like HLA-DQ-gluten tetramers are impractical. We recently showed serum interleukin (IL)-2 release to gluten is a marker of gluten-specific T cells. We aimed to assess the diagnostic performance of an IL-2 whole blood assay (WBA) employing an “in-tube gluten challenge” and compared this to serum IL-2 levels after oral gluten and tetramer analysis.
Methods: The IL-2 WBA was assessed in 79 adults with CD (71 on a GFD with negative CD serology and 8 consuming gluten; 75 HLA-DQ2.5) and 92 without CD (34 on GFD with self-reported non-celiac gluten sensitivity, NCGS, and 58 healthy controls consuming gluten; 35 HLA-DQ2.5). Fresh blood was incubated for 24 hours with gluten peptides and IL-2 assessed (MesoScale Discovery). Serum IL-2 levels at 0 and 4 h after single-bolus 10 g gluten challenge and tetramer frequency was also assessed in the treated CD and NCGS cohorts.
Results: IL-2 WBA showed high accuracy to detect CD: sensitivity 85% (67/79), specificity 97% (89/92), AUC=0.93. Sensitivity increased to 88% (67/76) when CD patients with the atypical HLA-DQ8 genotype were excluded (AUC 0.95). The IL-2 WBA response correlates with both gluten-induced serum IL-2 (n=50, r=0.65, p < 0.0001) and the frequency of gluten-tetramer+ gut-homing T cells per million CD4+ T cells (n = 10, r=0.9, p < 0.0001). The IL-2 WBA was positive at tetramer frequencies as low as 1 per million CD4+ T cells. Higher baseline IL-2 WBA was associated with vomiting after gluten challenge.
Conclusion: The IL-2 WBA demonstrates exceptional sensitivity equivalent to detecting a single gluten-specific T cell in a 4 ml blood vial. It is a simple, tube-based assay requiring < 10 mL whole blood and can predict the severity of gluten-induced symptoms. It shows high diagnostic accuracy for CD with the important advantage of detecting CD in patients following a GFD with negative transglutaminase-IgA. Ongoing refinements aim to improve diagnostic sensitivity. The IL-2 WBA has the potential to revolutionise CD diagnosis and overcome the current limitations of CD serology and histology.
159
Thionamide-induced neutropenic enterocolitis in a patient in thyroid storm: a rare clinical entity
Ibrahim Mian, Aisling Hand and Katherine Griffin
Gold Coast University Hospital, Gold Coast, Australia
Introduction: Neutropenic enterocolitis (NEC) is a severe, life-threatening condition characterized by inflammatory necrosis of the bowel wall, seen in neutropenic patients. Bowel wall inflammation in NEC progresses to ulceration and necrosis, which if not addressed promptly can cause bowel perforation. There have been no reported cases of NEC secondary to thionamide use and for a patient in thyroid storm.
Case Report: A young woman in her thirties with a recent diagnosis of Graves' disease for which she took methimazole, presented to hospital with fevers, abdominal pain, and diarrhoea after recently returning from Thailand. She was febrile to 38.8°C, tachycardic to 140 bpm, and a blood pressure of 105/56 mmHg. Her exam was remarkable for exophthalmos, a large palpable goitre, and swollen exudative tonsils. She had an absolute neutrophil count of 0.00x 10^9/L (2.5-7x 10^9/L), free T4 63.5 pmol/L (10-20 pmol/L), free T3 28.9 pmol/L (2.8-6.8 pmol/L), and a TSH 0.00 mU/L (0.50-4.00 mU/L). Her presentation was in keeping with agranulocytosis secondary to thionamide use for her Graves’ disease complicated by thyroid storm from a bacterial tonsillitis. Her management was complicated as she was unable to use alternative antithyroid drugs for her thyroid storm. As such, she was managed with intravenous fluids, broad spectrum antibiotics, and granulocyte-colony stimulating factor (G-CSF) for her bacterial tonsillitis and neutropenic sepsis. Lugol’s iodine, glucocorticoids, and propranolol were used to manage her thyroid storm, whilst awaiting a thyroidectomy. On day 10 of her admission, she developed severe abdominal pain with associated haematochezia. She examined as peritonitic. Her CT abdominal imaging demonstrated features consistent with NEC. She was abruptly taken to theatre for an emergency laparotomy. Histology from her diseased bowel remained consistent with NEC. By day 31 of her admission, she underwent a total thyroidectomy without complications and was discharged in the following days.
Conclusion: This case highlights the clinical challenges in managing a patient with NE in concomitant thyroid storm and neutropenic sepsis from thionamide-induced agranulocytosis. The patient's management was complicated by overlapping symptoms of thyrotoxicosis and NEC, underscoring the need for high clinical suspicion and early imaging in febrile neutropenic patients with gastrointestinal symptoms. Lugol's iodine served as a critical bridging therapy in managing thyrotoxicosis until surgical intervention was feasible. The case also raises considerations for the selective use of G-CSF in high-risk patients with NEC. Ultimately, thionamide-induced NEC, though rare, requires prompt recognition and management due to its high mortality risk.
172
Nasogastric delivery of fecal microbiota transplantation for treatment of Clostridioides difficile infection: a case report
Amitjeet Singh, Edward Young and Arvind Rajagopalan
Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia
Introduction:Clostridioides difficile is a significant healthcare challenge due to its association with antibiotic-associated diarrhea, increasing incidence, and the emergence of highly virulent strains. Traditional treatments like metronidazole and oral vancomycin are becoming less effective due to rising resistance, while faecal microbiota transplantation (FMT) has shown promise, particularly via direct caecal delivery. This case report describes the successful use of nasogastric FMT to avoid colectomy in a patient with severe C. difficile infection (CDI) complicated by toxic megacolon.
Case Report: A 46-year-old female with cirrhosis presented to the emergency department with haematemesis and haemodynamic instability. An emergency endoscopy demonstrated large oesophageal varices with high-risk stigmata, managed with band ligation. She was commenced on intravenous pantoprazole and ceftriaxone according to routine variceal bleeding protocols. Unfortunately, one week into her admission (after completing 5 days of ceftriaxone) she developed abdominal pain, diarrhoea and fevers to 38.1°C. Laboratory investigations showed a white cell count of 19x109/L, C-reactive protein of 143mg/L and albumin of 21 g/dL. Computed tomography (CT) scan of her abdomen showed colitis involving the ascending colon and splenic flexure but no colonic dilation. A stool PCR was positive for C. difficile toxin. Treatment was initiated with oral vancomycin 250mg four times daily and intravenous metronidazole 500mg three times daily. Despite escalation of vancomycin to 500mg four times daily, the patient symptoms worsened, with increasing abdominal pain, diarrhea, and new onset hepatic encephalopathy. Repeat abdominal X-rays demonstrated significant colonic dilation, with a transverse colon diameter of up to 12cm. The decision was made to proceed with FMT, however colonoscopic delivery was not safe due to the toxic megacolon. Push enteroscopy was also deemed to be high-risk given the recent oesophageal banding, decompensated cirrhosis with ascites and encephalopathy, and ileus with resultant risk of aspiration. We administered the first 50ml syringe of FMT solution via enema without complication. Four hours after the enema, three syringes of FMT solution were administered at two-hour intervals via the nasogastric tube, with concurrent intravenous metoclopramide 10mg three times a day as an anti-emetic and prokinetic. The syringes were each delivered slowly over 10 minutes, ensuring no nausea or vomiting occurred. The following day the patient had a significant improvement in abdominal pain, diarrhea, and encephalopathy. A repeat abdominal X-ray showed the resolution of toxic megacolon with a normal amount of gas throughout the large bowel. There was significant improvement in her C-reactive protein and white cell count. The patient was discharged home with 14-days of oral vancomycin.
Discussion: In this case, we have demonstrated successful salvage of a C. difficile-related toxic megacolon following administration of FMT via a nasogastric tube, where push enteroscopy was relatively contraindicated. Comparative studies on the efficacy of fecal transplantation based on the administration method have yielded mixed results. A systematic review found that the success rates of fecal transplantation were lower when administered via enteroscopy or nasoenteric tube (88%) compared to colonoscopy and enema (95%). Another review analysing colonoscopic versus nasogastric methods across 12 studies revealed a higher success rate for the colonoscopic approach (93%) over nasogastric (85%), though the difference was not statistically significant. Nevertheless, in severe cases there are often contraindications to traditional methods for FMT delivery, as was the case in our patient. There are few published articles on the use of FMT for patients with toxic megacolon. Evidence has shown that FMT is effective in patients with recurrent CDI while evidence and experience in the context of severe and fulminant C. difficile continues to grow. To our knowledge this is the first reported case where nasogastric delivery of FMT solution has led to resolution of a C. difficile-related toxic megacolon. There are inherent risks of aspiration with this method, however a colectomy would have resulted in extremely high morbidity and mortality given the patient’s decompensated cirrhosis. This highlights the importance of the awareness of various routes of FMT delivery in order to tailor delivery to specific patient circumstances.
173
Endoscopic submucosal dissection of complicated giant gastrointestinal lipomas - a tertiary care center experience
Wei Ling Teh, Sherman Picardo, Niroshan Muwanwella and Marcus Chin
Royal Perth Hospital, Perth, Australia
Background and Aim: Gastrointestinal (GI) lipomas are benign subepithelial lesions (SELs) composed of mature adipose tissue. While often asymptomatic, GI lipomas can cause complications such as bleeding, luminal obstruction, or intussusception, necessitating intervention. Currently, there is no standardized approach for the treatment of symptomatic GI lipomas. Most cases reported in the literature were resected surgically. Recently, endoscopic resection techniques have evolved, with endoscopic submucosal dissection (ESD) emerging as a promising approach for the management of GI lipomas. We aim to analyse the success and safety of ESD in resecting GI lipomas.
Methods: This was a retrospective, observational case series study. We reviewed gastrointestinal lipomas resected by ESD at our hospital between March 2017 and October 2023. All upper ESDs were performed using either EG760Z (Fujifilm, Tokyo, Japan) or GIF-HQ190 (Olympus Medical, Tokyo, Japan) Gastroscope. Colonic ESD was performed with EC760ZVL Colonoscope (Fujifilm, Tokyo, Japan). Utilizing either Dual Knife J and/or IT-2 knife (Olympus Medical, Tokyo, Japan), we directly dissected the submucosal connective tissue beneath the lesion, achieving en-bloc resection.
Results: Here, we present seven instances wherein giant GI lipomas were effectively excised using ESD. All patients included in our study exhibited sizable GI lipomas and were experiencing associated symptoms. The mean age of patients was 59 years (41-68). The average lipoma size was 79 mm (50-100mm). Histopathology examination confirmed the diagnosis of lipomas in six cases and one case of angiolipoma. All patients were followed up either in clinic to ensure resolution of symptoms or with surveillance endoscopies. We demonstrated the successful removal of three bleeding and three obstructive large GI lipomas, all without complications, including bleeding and perforation.
175
Effectiveness and long-term durability of cricopharyngeal peroral endoscopic myotomy for treating dysphagia with upper oesophageal sphincter dysfunction: a mixed aetiology study
Alvin Cheah1,2, Michal Szczesniak1,2, Dheeraj Pandey1,2, Julia Maclean1,2 and Peter Wu1,2
1Department of Gastroenterology and Hepatology, St George Hospital, Sydney, Australia;2St George and Sutherland Clinical School, University of New South Wales, Sydney, Australia
Background and Aim: Encouraging preliminary data shows that cricopharyngeal peroral endoscopic myotomy (C-POEM) improves oropharyngeal dysphagia (OPD) in Parkinson’s disease (PD) patients with upper oesophageal sphincter (UOS) dysfunction on pharyngeal high-resolution impedance manometry (PHRIM). UOS dysfunction can manifest in a spectrum of neuromyogenic disorders, including PD, cerebrovascular accidents (CVA), inflammatory myopathies and post head and neck cancer (HNC) treatment. The aim of this study is to assess the efficacy and the long-term durability of C-POEM as a treatment for dysphagia with mixed aetiologies with proven underlying UOS dysfunction.
Methods: Consecutive patients with OPD underwent PHRIM and were offered C-POEM if failed UOS relaxation was observed. Analysis was carried out on Swallow Gateway and failed UOS relaxation was defined as increased integrated relaxation pressure (IRP0.25) above upper limit of normal for a liquid bolus (either thin IDDSI 0 or thick IDDSI 4) of highest volume tolerated without piecemeal swallowing. Sydney Swallow Questionnaire (SSQ) was obtained at baseline, 1 month and yearly up to 3 years after C-POEM to measure symptoms of swallow dysfunction. The mean change in total SSQ scores from pre-treatment to 1 month post were assessed using paired t-test. Long term trend in total SSQ score post-treatment was assessed using repeated measures mixed model.
Results: Between September 2020 and Sept 2023 consecutive patients (n = 15) underwent C-POEM for OPD and UOS dysfunction demonstrated on PHRIM. Patients with OPD were of various aetiologies such as CVA (n=4), inflammatory myopathies (n=4), Parkinson’s disease (n=2) and HNC (n=5). In one HNC patient included in the analysis, C-POEM could not be completed due to extensive submucosal fibrosis. There was an improvement in mean SSQ scores 1-month post C-POEM (714, 95%CI [542-885]) from baseline (1133, 95% CI [951-1314]). The mean change was statistically significant (∆ 419, 95% CI [253-585], p=0.0001). We observed no deterioration in swallow function on SSQ post C-POEM on repeated measures mixed model. Mean follow-up period was 8 months and the SSQ score remained stable with minimal non-significant change of -0.69 per month, 95% CI [-9.02-2.29] (p=0.87). There were no complications identified in the study group.
Conclusion: C-POEM is an effective and safe novel endoscopic technique that improves dysphagia symptoms in patients with neuromyogenic disorders and HNC by targeting spastic UOS, thus improving bolus flow during swallowing. Importantly, dysphagia symptoms remained stable post C-POEM. However, considering the small sample size, larger and longer prospective trials looking at the merits of C-POEM is warranted.
176
Evaluating hypopharyngeal post-swallow and contractile admittance as non-radiological markers of pharyngeal residue and clearance in dysphagia
Alvin Cheah1,2, Dheeraj Pandey1,2, Julia Maclean1,2, Peter Wu1,2 and Michal Szczesniak1,2
1Department of Gastroenterology and Hepatology, St George Hospital, Sydney, Australia;2St George and Sutherland Clinical School, University of New South Wales, Sydney, Australia
Background and Aim: Post-swallow residue and presence of pharyngeal space during pharyngeal constriction are swallowing impairment signs and pose aspiration risk. Analysis of admittance during pharyngeal high-resolution impedance manometry (PHRIM) offers a potential non-radiological marker of pharyngeal residue post-swallow and during pharyngeal contraction, providing quantitative interpretation at bedside. Additionally, absence of radiation exposure makes it appropriate for follow up studies with repeat progress measurements. The aim of this study was to compare estimates obtained with admittance against radiographic equivalents.
Methods: We identified 98 patients with oropharyngeal dysphagia of various aetiologies who underwent concurrent videofluoroscopy and PHRIM. Using SwallowGateway (5ml liquid (IDDSI 0) swallows), hypopharyngeal post-swallow admittance (HpPostAdm) was calculated as mean admittance spanning the hypopharyngeal segment within 0.5s after the stripping wave. Hypopharyngeal contractile admittance (HpContAdm) was calculated as mean admittance during the period of hypopharyngeal contraction. In the same cohort, fluoroscopic videos of 5ml liquid (IDDSI 0) swallows in lateral projection were independently analysed after spatial calibration referenced to radio opaque PHRIM sensors. Areas (cm2) of post-swallow reside were calculated for vallecula (VR), pyriform sinuses (PR) and other pharyngeal areas (OR). These were summed to derive total pharyngeal residue (TR). Intraluminal area at maximum pharyngeal constriction (AMPC) was measured in the frame showing maximum obliteration of the space in the pharynx before the pharynx begins to relax. Sydney Swallow Questionnaire (SSQ) was routinely obtained prior to PHRIM assessment to measure baseline swallow dysfunction.
Results: Patient backgrounds included Parkinson’s disease (12), head and neck cancer (55), inclusion body myositis (8), cerebrovascular accident (2), muscular dystrophy (3), MOGAD (1), multiple sclerosis (1), motor neuron disease (1) and idiopathic (15). Majority were male (70%) and mean SSQ was (588.92 ±SD 409.15). We observed significant correlation between HpPostAdm and residue area observed radiographically post-swallow in the lateral plane. Correlation was highest with PR (Spearman’s ρ=0.64, p<0.0001) followed by TR (ρ=0.59, p<0.0001) and VR (ρ=0.34, p=0.001). Correlation between HpContAdm and AMPC was also significant with ρ=0.341, p=0.0006.
177
Beyond metrics: esophageal hypervigilance better predicts esophageal symptom severity compared with pH study and HRM metrics
1St Vincent's Hospital Melbourne, Melbourne, Australia;2St Vincent's Hospital Sydney, Sydney, Australia;3The University of Melbourne, Melbourne, Australia
Background and Aim: In clinical practice, the results from manometry and pH studies are often insufficient to explain the symptom severity of dysphagia and gastroesophageal reflux disease symptoms (GORD) perceived by patients. Oesophageal hypervigilance is thought to be a contributor to symptom severity of dysphagia and GORD. The 7-item questionnaire Oesophageal Hypervigilance and Anxiety Scale (EHAS-7) was developed to assess oesophageal hypervigilance. Our study aims to investigate whether manometry/pH study metrics or EHAS-7 have a greater correlation with the symptom severity of GORD and dysphagia. We hypothesise oesophageal hypervigilance can better predict symptom severity for symptoms than physiological study metrics.
Methods: Consecutive patients attending for high resolution manometry (HRM) with or without a 24-hour pH study at a tertiary referral centre, from March 2022 to October 2023, were prospectively included. Patients completed the following questionnaires: EHAS-7, Brief Esophageal Dysphagia Questionnaire (BEDQ) and Gastroesophageal Reflux Disease Questionnaire (GERDQ). Pearson’s correlation was used to determine the interrelationships between questionnaire results, HRM and pH study metrics.
Results: 286 patients were included with 170 completing pH studies. The median age was 55 (IQR 42 – 66) and 181 (63.3%) were female. Chicago 4 diagnoses included 189 (66.1%) patients with a normal study, 40 (14.0%) with achalasia, 15 (5.2%) esophagogastric junction outflow obstruction (EGJOO), 25 (8.74%) ineffective oesophageal motility (IEM), 8 (2.80%) absent contractility, 3 (1.05%) diffuse oesophageal spasm (DES) and 6 (2.10%) Jackhammer oesophagus. In the whole cohort, symptom severity (BEDQ) was significantly correlated with EHAS-7 (r = 0.362, p < 0.001) and several HRM metrics: including median integrated relaxation pressure (IRP) for supine 5ml swallows (r = 0.320, p < 0.001), median IRP for upright 5ml swallows (r = 0.358, p < 0.001) and median IRP for 2cm bread swallows (r = 0.360, p = 0.001). Among patients with normal manometry findings, BEDQ had a significant correlation with EHAS-7 (r = 0.245, p = 0.002) and median DCI for upright swallows (r = 0.230, p = 0.046). In patients with achalasia, BEDQ was significantly associated with EHAS-7 (r = 0.414, p = 0.017) but not HRM metrics. For those with IEM, BEDQ was correlated with EHAS-7 (r = 0.594, p < 0.002) and median DCI for supine swallows (r = 0.542, p = 0.025). Regarding patients with absent contractility, symptoms were only correlated with EHAS-7 (r = 0.823, p = 0.023). BEDQ was not associated with either EHAS-7 or any manometry metrics for patients with DES or Jackhammer oesophagus. For patients presenting with GERD symptoms including heartburn and regurgitation, symptoms (GERDQ) were significantly associated with EHAS-7 (r = 0.148, p = 0.028) but not pH metrics. Age, sex, and BMI did not correlate with symptom severity for dysphagia or GORD.
Conclusion: In this cohort, we observed a stronger correlation between dysphagia and GORD symptom severity with Oesophageal hypervigilance scores compared to physiological metrics. These findings suggest a potential utility of Oesophageal hypervigilance as a predictor for patient-reported Oesophageal symptom severity. Subsequent studies should be conducted to investigate whether treating oesophageal hypervigilance improves symptom severity.
211
Evaluating the use of faecal occult blood tests for bowel cancer screening in persons with established spinal cord injury aged 50 – 74 years
Michael Yulong Wu1,2,3, Carmen Tung1, Mccawley Clark-Dickson4, Samuel Arthurs1 and Ian Norton1,2
1Royal North Shore Hospital, Gold Coast, Australia;2Northern Clinical School, University of Sydney, Gold Coast, Australia;3Faculty of Health Science and Medicine, Bond University, Gold Coast, Australia;4Sydney Adventist Hospital, Gold Coast, Australia
Background and Aim: In 2006 the Australian Government established the National Bowel Cancer Screening Program (NBCSP) with an aim to reduce the morbidity and mortality of colorectal cancer by early detection of malignancy. The program involves sending a biennial faecal occult blood test (FOBT) kit to all Australians aged 50 – 74 years old and those who test positive are recommended to proceed with colonoscopy if appropriate. The role and accuracy of FOBT in the spinal cord injury (SCI) population is yet to be established in the literature. We have postulated that the frequent use of rectal enemas, digital stimulation, chronic constipation and associated anorectal disorders in SCI patients can lead to colonic microtrauma with higher rates of positive FOBT. Therefore, the purpose of this study is to investigate the proportion of positive FOBT among patients with established SCI compared to the general population as measured by the NBCSP. We hypothesised that patients with SCI have a higher false positive rate.
Methods: A prospective study was conducted at a tertiary hospital with one of the two inpatient spinal injury units in New South Wales. All established SCI patients aged 50 – 74 years old were included. Patients outside of the age criteria, those with active per-rectal bleeding, haemorrhoids, per-vaginal bleeding, hematuria, SCI within 12 months, colonoscopy within 4 years, or had already completed FOBT as part of the NBCSP were excluded. Recruited patients had two separate faecal samples sent for FOBT. Those with at least one positive FOBT were offered either an inpatient colonoscopy or outpatient follow-up at their local hospital.
Results: A total of 18 patients were included in the study with a mean age of 61.1 years. In total 44.4% of patients tested positive on at least one FOBT. Of those who tested positive, two patients agreed to proceed with colonoscopy. In both cases the colonoscopy was normal. The majority of patients declined follow-up colonoscopy due to perceived difficulty with bowel preparation and procedural risks. Most patients reported rectal enema use, digital simulation and manual evacuation as part of their routine bowel care (Table 1). Out of those who used enemas, digital stimulation or manual evacuation, 41.1% returned a positive FOBT.
Conclusion: To date, there is a lack of prospective studies that have investigated the accuracy of FOBT in patients with SCI. In this study, patients with SCI have higher rates of positive FOBT compared to the general Australian population at 6.2%. Follow-up colonoscopy rates were poor and patient compliance can be improved by more streamlined inpatient bowel preparation protocols. Higher rates of positive FOBT may be attributed to colonic and anorectal microtrauma. Our results suggests that the FOBT may not be an accurate screening tool in this population and a primary screening colonoscopy strategy may be more appropriate.
212
Upadacitinib real-world efficacy and safety in treatment of inflammatory bowel disease: an Australian single-centre experience
Gordon Chen, Vikram Rao, Sheng Wei Lo, Elaine Koh, Abha Kaul and Richard La Nauze
Peninsula Health, Frankston, Australia
Background and Aim: Upadacitinib, a recently approved small molecule inhibitor of Janus kinase 1 (JAK1), has been subject to much excitement as a new effective therapy in the management of moderate to severe ulcerative colitis (UC) and moderate to severe Crohn’s disease (CD). There has been rapidly increasing evidence of efficacy in both forms of inflammatory bowel disease (IBD) in literature but still a relative paucity of safety data. This retrospective, single centre, observational study aimed to assess the clinical efficacy and audit the safety of this novel medication in the biologic-experienced IBD cohort.
Methods: Retrospective review was undertaken for all IBD patients prescribed Upadacitinib between January 2023 and May 2024 at a single-centre IBD service in Melbourne, Australia. Patients that have had at least 6 months of follow-up were included. Clinical and biochemical parameters were assessed at baseline, end of induction and at 6-months. Datapoints included previous exposure to biologics/JAK inhibitors, bowel motion frequency, clinical score indices (SCCAI/HBI), C-reactive protein (CRP), faecal calprotectin (FCP), and any adverse events.
Results: Four patients were identified for inclusion, three patients with UC and one patient with CD, with median follow-up time of 41.1 weeks (IQR 35.8-50.9). All were anti-tumour necrosis factor (TNF)-experienced. 75% (3/4) achieved the primary outcome of clinical remission at 6-months, all achieved the secondary outcomes of drug persistence at 6-months, corticosteroid-free remission and normalization of biomarkers (CRP, FCP) by end of induction, and maintained this through to 6-months. Adverse events occurred in 75% (3/4), 50% (2/4) of which were serious (requiring hospitalisation) within the 6-month follow up period. Patient 2 (Table 1), a 25-year-old female vaccinated with no comorbidities, was hospitalised for moderate-severity COVID. Patient 4 (Table 1), a 41 year-old female without significant comorbidities, was hospitalised for complicated cystourethritis. Two patients developed acne.
Conclusion: This real-world data in Australia supports the efficacy of upadacitinib as another therapeutic option in the biologic-experienced IBD cohort. It is noted that the serious adverse event rate is higher than previously reported in safety trials which highlights the importance of ongoing real-world monitoring of this medication.
230
Machine learning with natural language processing to identify cases of Barrett’s oesophagus from electronic endoscopy reports
Madoka Inoue1,3, Hideo Tohira2,4,5, James Chen3, Shiv Meka6, Spiro Raftopoulos1,5,7 and Krish Ragunath1,3
1Curtin Medical School, Curtin University, Perth, Australia;2Curtin School of Nursing, Curtin University, Perth, Australia;3Department of Gastroenterology, Royal Perth Hospital, Perth, Australia;4Department of Emergency Medicine, Chibanishi General Hospital, Japan;5UWA Medical School, University of Western Australia, Perth, Australia;6Health in a Virtual Environment, East Metropolitan Health Service, Perth, Australia;7Department of Gastroenterology, Sir Charles Gairdner Hospital, Perth, Australia
Background and Aim: Accurately identifying Barrett's oesophagus (BO) cases from electronic endoscopy reports is crucial for epidemiological studies but is often complicated by limitations in diagnostic coding systems and reporting structures. Few studies have applied natural language processing (NLP), a machine learning application for text classification, for this purpose. Thus, this study aimed to 1) develop machine learning models to identify BO cases using NLP to generate features from free-text descriptions in electronic endoscopy reports, and 2) evaluate the predictive performance of these models.
Methods: This retrospective observational study utilised data from electronic endoscopy reports of patients (age ≥18 years) who underwent upper gastrointestinal endoscopy between January 1999 and December 2023, at four teaching hospitals in Perth, Western Australia. Endoscopists usually complete these reports post-procedure, including two free-textual sections: endoscopic findings (Findings) and a summary (Conclusion). BO cases were manually identified from a 20% random sample of these reports through free-text review. Three corpora were then created: 1) "Findings" only, 2) "Conclusion" only, and 3) "Findings & Conclusion". The sampled reports were divided into 70% for training and 30% for testing. NLP was used to compute the term frequency-inverse document frequency of each word, ranking their relevance. Three machine learning models—Random Forest (RF), Support Vector Machine (SVM), and XGBoost (XGB)—were developed based on each corpus. Optimal parameters were determined through 5-fold cross-validation, and model performance was evaluated using F1-measure (harmonic mean of recall and precision), recall (sensitivity), and precision (positive predictive value).
Results: Among 186,896 electronic endoscopy reports, 37,396 were randomly sampled. Of the sampled reports, 42 and 90 were missing in the “Findings” and “Conclusion” sections, respectively. These reports were excluded when deriving models. A total of 26,177 reports were used for training and 11,219 for testing. We found that XGB performed best with an F1measure of 0.940, recall of 0.940, and precision of 0.939, derived using the combined corpus "Findings & Conclusion" as features. This was followed by RF with the combined corpus, achieving an F1-measure of 0.937, recall of 0.947, and precision of 0.928. SVM with the combined corpus attained an F1-measure of 0.922, recall of 0.895, and precision of 0.950.
Conclusion: The machine learning model, using free-text findings and a summary in the endoscopy report as inputs, could identify BO cases with high recall and precision. Further improvement might involve including additional information like patient demographics and leveraging large language models for word embedding.
238
Increased risk of future advanced neoplasia in individuals that have synchronous adenomas and clinically significant serrated polyps
Geraldine Laven-law1, Erin Symonds1,2, Kalindra Simpson1,2, Michelle Coats2, Mahinda De Silva2, Paul Hollington3, Charles Cock1,2 and Molla M Wassie1
1Flinders University, College of Medicine and Public Health, Flinders Health and Medical Research Institute, Adelaide, Australia;2Department of Gastroenterology and Hepatology, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia;3Department of Colorectal Surgery, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia
Background and Aim: Colorectal cancer (CRC) commonly develops from pre-cancerous neoplasia through the adenoma-carcinoma and serrated pathways. Individuals with prior history of adenoma and/or clinically significant serrated polyp (CSSP) are considered at above-average risk for CRC and undergo colonoscopy surveillance at intervals recommended by national guidelines. While individuals with synchronous adenoma and CSSP are recommended the same surveillance colonoscopy interval as those with only CSSP, there is limited evidence to support this recommendation. This study determined whether synchronous adenomas and CSSP increase the risk of future advanced neoplasia compared to no neoplasia, prior adenoma, or prior CSSP.
Methods: This was a retrospective analysis of data from patients enrolled within a South Australian CRC surveillance program, and undergoing colonoscopies between 2010 – 2023 inclusive. Included patients were those that had a finding of no neoplasia or pre-cancerous neoplasia (adenoma and/or CSSP), who received a recommended surveillance interval and underwent another complete colonoscopy. Patients with inflammatory bowel disease, organ transplants, or CRC syndromes were excluded. Demographics and colonoscopy findings were extracted from clinical databases. Advanced neoplasia was defined as adenocarcinoma, advanced adenoma (adenoma ≥ 10 mm, high-grade dysplasia, and/or villous change), and/or advanced CSSP (sessile serrated lesions or hyperplastic polyps ≥ 10 mm, with dysplasia, and/or any traditional serrated adenoma). Multivariable Cox regression determined the effect of prior neoplasia on risk for developing future advanced neoplasia, controlling for age, sex, and colonoscopy interval. P < 0.05 was considered statistically significant.
Results: A total of 11,134 colonoscopy pairs were included; 3,680 (33%) patients had no neoplasia, 5,884 (53%) had adenoma, 773 (7%) had CSSP, and 797 (7%) had synchronous adenoma and CSSP resected at the first colonoscopy of the pair. Patients were aged a median 65 (interquartile range 57 – 72) years, and 53% were male. Advanced neoplasia was found in 12% (1,336/11,134) of subsequent colonoscopies, but in 26% (140/536) of those with initial synchronous adenoma and CSSP when at least one lesion was advanced. Patients with synchronous advanced adenoma and non-advanced CSSP developed advanced neoplasia earlier than their advanced adenoma-only and non-advanced CSSP-only counterparts (Figure, p < 0.05).
239
Small bowel metastatic melanoma – a case report
Keith Brick and Montri Gururatsakul
Queensland Health, Cairns, Australia
Introduction: Melanoma is known to metastasize widely. The most frequent sites for metastatic melanoma are lymph nodes, lungs, liver, brain, bone and adrenal glands (1), but rarely gastrointestinal tract. The most common site of melanoma metastases to the gastrointestinal (GI) tract is the small intestine (1, 2). This case study reports a patient with small bowel metastatic melanoma who presented with recurrent iron deficiency anaemia.
Case Report: A 73 year old male presented with iron deficiency anaemia. He initially had upper endoscopy and colonoscopy which were unremarkable, and subsequently had video capsule endoscopy which found a non bleeding ulcerated mass lesion at the proximal jejunum. He has a background of previous cholecystectomy, diverticular disease, multiple SCC and BCCs excisions, and in 2021 he had a melanoma in situ excised from his upper lip with at least 3 mm margins. A CT Enteroclysis identified a short segment (49mm) of abnormal mural thickening of the small bowel with a nodular appearance with some dilatation of the proximal bowel loop (figure 1). The lesion was not seen on a push enteroscopy. He underwent antegrade double balloon enteroscopy and a suspicious medium-sized ulcerated mass with no bleeding was found in the mid-jejunum, which was biopsied and tattooed (figure 2). The histopathology was non diagnostic. His case was discussed at both at radiology and histology MDT, and referred for surgical resection. He underwent successful robotic small bowel resection which has confirmed a diagnosis of metastatic melanoma. Subsequent somatic mutation testing for BRAF, KIT and NRAS were negative. He is now being considered for immunotherapy.
References
1. Liang, KV, Sanderson, SO, Nowakowski, GS, Arora, AS. Metastatic Malignant Melanoma of the Gastrointestinal Tract. Mayo Clinic Proceedings.200681(4) 511-16. https://doi.org/10.4065/81.4.511
2. Lens, M, Bataille, V, Krivokapic, Z. Melanoma of the small intestine. Lancet Oncol.2009; 10 (5): 516–521. doi: https://doi.org/10.1016/S1470-2045(09)70036-1
240
A large choledochoduodenal fistula – a case report
Keith Brick, Montri Gururatsakul and Shihaz Hussain
Queensland Health, Cairns, Australia
Introduction: A choledochoduodenal fistula is an abnormal communication between the common bile duct & the duodenum. It is often secondary to PUD, cholelithiasis, malignancy or iatrogenic (1). Presenting symptoms of cholangitis (fever, jaundice & abdominal pain) are common. This is a case report of an asymptomatic large choledochoduodenal fistula.
Case Report: A 65 year old female presented to hospital with hepatic encephalopathy & haematemesis. She has a background of Child-Pugh B cirrhosis secondary to Hepatitis C & alcohol on regular variceal screening, recently diagnosed metastatic rectal adenocarcinoma for palliative treatment, previous laparotomy for cholecystectomy & H. pylori infection. Of relevance she did not have a history of peptic ulcer disease (PUD), no recent biliary tract stones & was asymptomatic with no signs of cholangitis.
An upper endoscopy for bleeding was performed & identified a large 11mm choledochoduodenal fistula in the first part of the duodenum (fig 1), confirmed by bile draining through the fistula. The major papilla appeared normal without evidence of previous sphincterotomy. Previous staging CT abdomen for rectal cancer showed pneumobilia although no fistula apparent. Blood tests at presentation revealed a raised total bilirubin of 43. Liver enzymes ALP 87U/L, GGT 15U/L, ALT 24U/L & mildly raised AST 42U/L consistent with known decompensated cirrhosis. A cholestatic picture was not expected given the large size of the choledochoduodenal fistula. Due to her co-morbidities, dedicated imaging was not undertaken to further investigate, however a CT abdomen for a separate indication did identify the fistula (fig 2). Four previous surveillance UGIEs reported duodenal diverticulum, however no fistula documented. Her metastatic malignancy was diagnosed 6 weeks prior to the UGIE that identified the fistula.
Reference
1. Wu, MB, Zhang, WF, Zhang, YL, Mu, D, Gong, JP. Choledochoduodenal fistula in Mainland China: a review of epidemiology, etiology, diagnosis and management. Ann Surg Treat Res.2015 Nov; 89 (5) 240-6. https://doi.org/10.4174/astr.2015.89.5.240
245
An unusual cause of dysphagia
Eliza Flanagan1,2, Carl Cosgrave1,2, Irene Lu1,2 and Alvin Ting1,2
1Barwon Health, , Australia;2Monash University, Australia
Introduction: The most common causes of dysphagia include intrinsic oesophageal pathology, such as motor disorders and obstructive lesions. Extrinsic conditions are rarer and usually occur secondary to mediastinal masses or vascular compression. Mediastinal masses comprise a wide variety of benign and malignant lesions and are typically identified incidentally or due to investigations performed for symptoms arising from mass effect. The differential diagnoses for mediastinal masses include thymoma, neurogenic tumours, lymphomas, cysts and germ cell tumours. Symptoms secondary to mass effect may include dyspnoea, cough, chest discomfort, dysphagia, or neurologic issues such as Horner’s syndrome. Imaging via CT chest provides detailed information regarding location and assists with differential diagnosis. Patient management relies on tissue diagnosis obtained via biopsy or during planned resection. Inflammatory myofibroblastic tumours (IMTs) are a rare intermediate-grade neoplasm, considered to be a subtype of sarcoma. They have high recurrence rates following resection and low metastatic potential [1]. They are most often found in children, and occur predominantly in the abdomen (up to 75%), lung, pelvis and retroperitoneum; however, any site can be involved [1, 2]. Most cases have a benign course and depending on the location, are often asymptomatic. Diagnosis is made by histologic findings characterized by spindle cell proliferation and an inflammatory infiltrate [1]. The anaplastic lymphoma kinase (ALK) gene has a critical role in the biology of many IMTs, and approximately 50% of IMTs contain a translocation in the ALK gene, resulting in tyrosine kinase activation. Complete surgical resection is the standard of care [1, 2] and if recurrence occurs, re-resection would be offered plus consideration of chemotherapy [3].
Case Report: A 41-year-old lady with no significant past medical history was referred to hospital with chest discomfort and mildly elevated troponin 42ng/L [0-40]. She described a history of four months of progressive dysphagia to both solids and liquids, with worsening dyspnoea and orthopnea. Her electrocardiogram was normal and repeat troponin was stable. A computed-tomography (CT) scan of her chest was performed which demonstrated a large posterior mediastinal mass measuring 60x50x70mm in size, with compression of the oesophagus and trachea. She underwent an endoscopic ultrasound which was unable to pass the extrinsic compression but core lesional biopsies (fine needle biopsy) were able to be taken to expedite diagnosis. She subsequently underwent a thoracotomy and complete resection of the mass, with histopathology confirming an inflammatory myofibroblastic tumour with ALK gene rearrangement. Following tumour resection, her dysphagia resolved; and she is being followed up with regular surveillance CT imaging.
References
1. Siemion, K., et al., What do we know about inflammatory myofibroblastic tumors? - A systematic review. Adv Med Sci, 2022. 67(1): p. 129-138.
2. Kovach, S.J., et al., Inflammatory myofibroblastic tumors. J Surg Oncol, 2006. 94(5): p. 385-91.
3. Wang, Q.A., et al., Update of Diagnosis and Targeted Therapy for ALK(+) Inflammation Myofibroblastic Tumor. Curr Treat Options Oncol, 2023. 24(12): p. 1683-1702.
Background and Aim: Gastro-oesophageal reflux disease (GORD) is common, but symptoms overlap with many other upper gastrointestinal conditions and objective evidence of GORD on endoscopy is uncommon. Thus, an objective diagnosis of GORD is often sought with ambulatory 24-hour catheter-based pH test. However, the test is limited by tolerability and false negative diagnoses due to the relatively short duration of monitoring. Endoscopically placed, wireless prolonged pH testing is another alternative. We aimed to determine; (i) Technical success of introducing a wireless pH testing service, (ii) Indications and outcomes of wireless pH testing and (iii) Compare outcomes among patients who underwent both standard 24-hour pH impedance testing AND subsequent prolonged ambulatory wireless testing.
Methods: Chart review of patients who underwent wireless pH testing at a single gastroenterology practice between April 2022 and April 2024. Descriptive analysis of clinical characteristics and pH variables was performed.
Results: 40 wireless pH studies were conducted, all were initially technically successful, however two studies had premature dislodgement (<24h). LA Grade B esophagitis was observed in 5 patients. All tests were performed off PPI therapy and gastric pH was confirmed to be <4 in all patients prior to device placement. The mean age was 47.5 years (range 21-74) and 60% were female. The mean duration of pH data collection was 75.2 hours (SD 11.2). The indication for the test was “Reflux “in 78%, “Atypical GORD” in 15% and “globus or vomiting” in 7%. A positive study, defined as at least one 24-hour period with >6.5% esophageal acid exposure (AET), occurred in 18 patients (45%). Graph 1 shows the proportion of abnormal days of acid exposure among all patients. 3 of the 40 patients had completed an ambulatory pH testing prior to the prolonged wire-less test. In one of these 3 patients severe GORD was present on prolonged wireless testing whereas a concordant result was present in 2. There were no anesthetic or significant endoscopic complications. Mild and moderate chest discomfort was reported in 5 patients and 3 patients respectively.
271
The prevalence and predictors of oesophago-pharyngeal reflux in lung transplant recipients
Alyce Lonsdale, Mary Eid, David Darley, Mark Danta, Nick Olsen and Santosh Sanagapalli
St Vincent's Clinical School, University of New South Wales Medicine, Sydney, Australia
Background and Aim: Lung transplantation is an important therapeutic option for patients with end-stage lung disease, however, outcomes are poorer than other types of solid organ transplantation. While gastro-oesophageal reflux disease has been linked to lung allograft rejection, existing evidence is of poor quality. This study hypothesised that microaspiration of gastric contents via the pharynx into the lungs contributes to lung allograft injury. Accordingly, it aims to (1) identify the incidence of proximal oesophageal reflux events among lung transplant recipients; and (2) assess the effect of sex, age, body mass index (BMI), oesophageal dysmotility, and the type of pretransplant end-stage lung disease as risk factors for oesophago-pharyngeal reflux.
Methods: This cross-sectional study assessed lung transplant recipients at three to six months post-transplant, who underwent oesophageal multichannel intraluminal manometry and 24-hour pH testing between March and August 2023. Proximal and distal reflux episodes, and total acid exposure time (AET) were measured using a catheter with one distal pH-probe and eight impedance rings, spanning from 6cm above the manometrically determined lower oesophageal sphincter (LOS).
Results: Among the fourteen lung transplant recipients included in the study (8 [57.1%] female; median age, 56.5 years [IQR, 46-62]; median BMI, 22.7 kg/m2 [IQR, 20.2-27.9]), six patients (42.9%) experienced an abnormal number of total impedance-detected reflux episodes, and eight patients (57.1%) had an abnormal total AET. Five patients (35.7%) experienced an abnormal number of impedance-detected proximal oesophageal reflux episodes, with three (21.4%) and seven (50.0%) experiencing an abnormal number of acidic and weakly acidic events, respectively. Univariate Poisson regression with bootstrapped confidence intervals (CI) identified that male sex (IRR=2.08, 95%CI [1.01,5.17], p=0.04), and a reduction in oesophageal motility parameters such as LOS basal pressure respiratory mean (IRR=0.96, 95%CI [0.94,0.98], p<0.001), LOS residual pressure median (IRR=0.93, 95%CI [0.88, 0.98], p=0.004) and distal contractile integral (IRR=0.63, 95%CI [0.48, 0.77], p=0.001), in addition to the presence of cystic fibrosis (IRR=1.77, 95%CI [1.23, 3.00], p=0.04) and the absence of pretransplant chronic obstructive pulmonary disease (IRR=0.48, 95%CI [0.16, 0.96], p<0.05), were predictors of increased proximal oesophageal reflux episodes (p<0.05). BMI (IRR=0.982, 95%CI [-0.168,0.079], p=0.737) and age (IRR=0.975, 95%CI [-0.085,0.018], p=0.124) were not statistically significant predictors.
Conclusion: This study concludes that lung transplant recipients have greater episodes of proximal oesophageal reflux, compared to a healthy population, which may have implications for patient outcomes post-transplantation. Further research should explore the relationship between proximal oesophageal reflux episodes and lung function in lung transplant recipients.
273
Clinical characteristics and current clinical practice in patients with acute pancreatitis at a large tertiary centre
Cindy Ho, Hardesh Dhillon, Kyle Williams, Eliza Flanagan, Faris Gondal, Sally Bell and Simon Hew
Monash Health, Melbourne, Australia
Background and Aim: Acute pancreatitis (AP) is a prevalent and potentially serious gastrointestinal illness. Contemporary studies evaluating the characteristics and management of patients with AP in large Australian tertiary centres are limited. Our study aims to detail the clinical characteristics of patients with AP and evaluate current clinical practices.
Methods: We conducted a retrospective cohort study including all inpatients with AP at a large tertiary health service in Melbourne, Australia, from May 2022 to 2023. Data on demographics, fluid resuscitation, interventions, and nutrition were collected. Serious complications were defined as necrotising pancreatitis (NP), intensive care unit (ICU) admission, or death. For gallstone-related AP, time to laparoscopic cholecystectomy and readmission rates were calculated.
Results: 553 patients with 639 admissions had AP. Most were male (51.4%) with a median age of 54 years (IQR 38-70) and BISAP of 1 (IQR 0-1). Gallstones (35.8%) were the commonest cause, followed by alcohol (26.6%) and idiopathic or unclear aetiology (16.6%). The mean intravenous fluid, mostly Hartmann’s (87.3%), administered within 24 hours of AP diagnosis was 4.5 litres (SD 0.4). NP, observed in 32 patients (5.0%), was associated with increased length of stay (LOS) (p<0.0001) and higher intervention rates for peri-pancreatic collections (OR 5.9, 95% CI 2.0-17.5) (Figure 1). Interventions included endoscopic (56.3%), percutaneous (18.8%), surgical (18.8%), or combined approaches (6.3%). The median time to drainage was 23.5 days (IQR 22.0-32.0). Nutritional support was required in 39 patients (6.1%), particularly those with NP (OR 4.6, 95% CI 1.8-11.5). The median time to light diet was 2 days (IQR 1-3). 36 patients needed ICU admission (5.6%), with a median ICU stay of 4.2 days (IQR 1.9-9.7) and a total hospital stay of 18.0 days (IQR 9.5-43.0). Higher BISAP scores correlated with increased ICU admissions (OR 10.9, 95% CI 5.2-22.2). Overall median LOS was 4 days (IQR 2-6), with a 2.2% mortality rate. 154 patients with gallstone-associated AP underwent laparoscopic cholecystectomy (80.7%), primarily as inpatients (76.0%), with a median time to surgery of 3 days (IQR 2-4) and 39 days (IQR 19-61) for outpatients. 37 patients (19.3%) did not undergo surgery due to comorbidities, patient wishes, or death. Nine readmissions occurred, three preventable by timely surgery.
274
Autoimmune enteropathy associated with COVID-19 infection - a case report
Wei Ling Teh, Siaw Chai, Dilini Gunawardena and Jesica Makanyanga
Fiona Stanley Hospital, Perth, Australia
Introduction: Autoimmune enteropathy (AIE) is a rare cause of chronic diarrhea that can occur as a primary condition or secondary to another immune-mediated process. Autoantibodies are not necessary for diagnosis, making AIE challenging to diagnose due to its overlap with other diseases characterized by villous atrophy. There is no standard treatment. Typically, patients are treated with glucocorticoids, sometimes combined with other immunosuppressive agents. This case highlights an AIE case whose symptoms began following COVID-19 infection, successfully managed with prednisolone and vedolizumab.
Case report: A previously well 31-year-old woman was referred in March 2023 for months of severe watery diarrhea and vomiting, leading to electrolyte disturbances and weight loss. The diarrhea began after a mild COVID-19 infection in December 2022 and worsened after taking amoxicillin for an ear infection. She was not on regular medications. Her aunt had Crohn’s disease. ANA, ANCA, and coeliac antibodies were negative. Immunoglobulin levels were normal. HLA-B27 was negative, but HLA-DQ 2.5 indicated susceptibility to coeliac disease. Faecal tests were negative for infective causes. A secretory diarrhea screen (calcitonin, chromogranin A, gastrin, VIP) was negative. Endoscopy revealed mild gastritis and atrophic mucosa in the duodenum and terminal ileum, with normal colonic mucosa. Duodenal and ileal samples showed marked villous atrophy, active neutrophilic inflammation, absence of goblet cells, and a paucity of plasma cells and intraepithelial lymphocytes. Colonic biopsies showed focal active colitis without ulceration or CMV inclusion bodies. Anti-enterocyte and anti-goblet cell immunofluorescent staining were negative. She did not experience sustained benefit from corticosteroids or infliximab. Azathioprine was discontinued due to pancreatitis. Empirical trials of gluten free diet, octreotide and rifaximin were ineffective. In August 2023, vedolizumab, slow corticosteroid taper and partial parenteral nutrition (PN) were started. She showed gradual clinical improvement and reduced dependence on PN, eventually stopping it in April 2024. Repeat endoscopy in February 2024 showed epithelial cell regeneration and improved cryptitis, though goblet cells were still absent. She is currently on vedolizumab and 15mg of prednisolone daily, and in symptomatic remission.
275
The role of drug and alcohol services for patients with alcohol-associated acute pancreatitis at a large tertiary centre
Cindy Ho, Hardesh Dhillon, Alex Mitropoulos, Eliza Flanagan, David Jacka, Sally Bell and Simon Hew
Monash Health, Melbourne, Australia
Background and Aim: Alcohol is a common cause of acute pancreatitis (AP), and ongoing consumption increases the risk of recurrent episodes. No specific guidelines exist for behavioural or pharmacological interventions to reduce recurrence of alcohol-associated AP. Studies exploring the role of addiction medicine for patients with alcohol-induced pancreatitis are limited. Our study aims to describe the utilization of the addiction medicine unit (AMU), a drug and alcohol physician-led inpatient consultation service, for patients admitted to a tertiary hospital with alcohol-associated AP.
Methods: We conducted a retrospective cohort study including all inpatients diagnosed with alcohol-associated AP at a tertiary health service in Melbourne, Australia between May 2022 to 2023. Data on AMU referrals and assessment, recommended interventions, and outpatient follow-ups were collected. Re-admission rates for AP within this timeframe were calculated. Serious complications of AP were defined as those with necrotising pancreatitis, requiring intensive care unit (ICU) admission, or death.
Results: 141 patients with 170 admissions were admitted with alcohol-associated AP. Most were males (76.6%), with a median age of 47 years (IQR 35-57) and median BISAP score of 0 (IQR 0-1). Fourteen patients (8.2%) had necrotizing pancreatitis, 13 (7.6%) required ICU admission, and 2 (1.4%) patients died. Fifty-seven patients (33.5%) were referred to the AMU. Of those referred, 98.2% were reviewed, either in person (73.2%) or via phone advice to clinicians (26.8%). Multi-disciplinary interventions including medications for addiction and outpatient services were recommended most (53.0%), followed by outpatient services alone (30.3%), and medications alone (16.7%). Outpatient services included follow-up in the AMU outpatient clinic, or more commonly, self-referrals to SECADA, a consortium for drug and alcohol addiction services including counselling and detox programs. 44 patients were recommended to commence or up-titrate medications for addiction by the AMU, which included naltrexone (61.4%), topiramate (38.6%), baclofen (6.8%), disulfiram (2.3%), either as single agents or in combination. Eighteen patients were re-admitted with alcohol-associated AP, with 11 (61.1%) not seen by the AMU during their initial admission. Of the 113 patients (66.5%) not referred to the AMU, contributing factors included patient refusal and weekend admissions.
Conclusion: Within the limits of a single centre cohort with a short follow-up interval, our study demonstrated that approximately one-third of patients with alcohol-associated AP were referred to the AMU. Combination pharmacological and outpatient follow up were the most common interventions recommended. Efforts to improve referral patterns during index admissions may be helpful to reduce readmissions for alcohol-associated AP.
293
Enterocolitis with rectal and ileal stenosis: A rare presentation of metastatic urothelial carcinoma
Nicholas Smith, Andrew Taylor and Jennifer Borowsky
Princess Alexandra Hospital, Brisbane, Australia
Introduction: Urothelial carcinoma is the most common histologic subtype accounting for approximately 90% of bladder cancers [1]. The most common sites of distant metastasis include liver, lung, and lymph nodes. Gastrointestinal tract involvement is rare [1].
Case Report: An 81-year-old man presented with 3-months of vomiting, diarrhoea and abdominal pain. His background included; hypertension, benign prostatic hypertrophy and stage 3 chronic kidney disease. He was a non-smoker and lacked a family history of colorectal or urological malignancy. His medications included; perindopril, atenolol, aspirin and dutaasteride-tamsulosin. There was no non-steroidal anti-inflammatory exposure. Computer tomography revealed extensive mural thickening of both his small and large bowel suggestive of enterocolitis with pneumatosis intestinalis and a thickened bladder wall. Blood investigations were unremarkable apart from his known renal dysfunction and a mild leukocytosis of 11.5x109/L and eosinophilia of 0.40x109/L. C-reactive protein was 11mg/L. Colonoscopy showed congested and nodular mucosa throughout the entire colon with rectal and terminal ileal steosis, only traversable with a paediatric gastroscope (Figure 1.A). There was mucosal friability and loss of the normal haustral folds and vascular pattern. Histology revealed malignant cells present within lymphatics of the terminal ileum and colonic specimens. Immunohistochemistry showed positive staining of these cells with CK7, GATA3, and 34βE12 (Figure 1.B). There was no significant staining with CK20, PAX8, p53, TTF1 or CDX2. Urine cytology found atypical urothelial cells suggestive of a high-grade urothelial cell carcinoma. Cystoscopy revealed widespread erythema and cystitis with bullous areas with histology confirming the diagnosis of urothelial carcinoma, plasmacytoid subtype. Fludeoxyglucose positron emission tomography showed the expected uptake in the bladder and small and large bowel with small volume avid ascites. With the diagnosis of metastatic urothelial carcinoma, the patient was referred for palliative chemotherapy.
Discussion: The mechanism of urothelial carcinoma related stenosis remains unclear. With rectal invasion, it has been hypothesized that a locally aggressive cancer of the bladder can penetrate Denonvilliers’ fascia and encircle the rectum [2]. It has also been thought that the cancer cells may spread along the lateral bladder pedicles to reach the posterior rectal wall [2]. Several case reports have detailed gastrointestinal tract metastases of urothelial carcinoma [2,3,4,5]. Wasfie [5] presents a case with stenotic small bowel disease. Liu [3] and Takeuchi [2] report cases with stenotic rectal disease. Ours is the only report with extensive entero-colitis with both rectal and ileal stenosis. This highlights the important but rare differential of metastatic disease in presentation of enterocolitis.
References
1 Shinagare, AB, Ramaiya, NH, Jagannathan, JP, Fennessy, FM, Taplin, ME, Van den Abbeele, AD. Metastatic pattern of bladder cancer: correlation with the characteristics of the primary tumor. AJR Am J Roentgenol.2011 Jan; 196(1): 117-22.
2 Takeuchi, H, Tokuyama, N, Kuroda, I, Aoyagi, T. Annular rectal constriction caused by infiltrating bladder cancer: A case report. Mol Clin Oncol.2016 Dec; 5(6): 842-844.
3 Liu, YH, Pu, TW, Yu, HW, Kang, JC, Yen, CH, Chen, CY. Invasive urothelial carcinoma of urinary bladder presenting with annular constriction and mimicking proctitis observed by colonoscopy: A case report. Int J Surg Case Rep.2021 May; 82: 105785.
4 Tse, CS, Elfanagely, Y, Fine, S. Metastatic urothelial bladder cancer involving the rectum/Practical Gastro. 2020 Nov; Vol XLIV, Issue 11.
296
Gastro-oesophageal reflux, determined with 24-hour pH-impedance monitoring, is highly prevalent in patients with chronic respiratory conditions, with many being asymptomatic or having extra-oesophageal symptoms
Michael Yulong Wu1,2,3, Ross Hansen1, Julia Mathers2, Vincent Liu2, David Joffe1,2 and May YW Wong1,2
1Royal North Shore Hospital, Sydney, Australia;2Northern Clinical School, University of Sydney, Sydney, Australia;3Faculty of Health Science and Medicine, Bond University, Gold Coast, Australia
Background and Aim: It is theorised that gastro-oesophageal reflux disease (GORD) can precipitate respiratory conditions due to aspiration of gastric contents into the respiratory tract provoking inflammation and neural reflexes which may trigger tracheobronchial constriction and hyperresponsiveness. However reflux symptoms can be unreliable indicators of the presence or absence of reflux. The primary aim of this study is to examine the prevalence of GORD using objective 24-hour pH-impedance monitoring in patients with chronic respiratory diseases (chronic obstructive pulmonary disease, bronchiectasis, asthma, interstitial lung disease). Secondary aims were to determine whether oesophageal symptoms and extra-oesophageal symptoms could predict presence of GORD, and whether respiratory function testing reflected severity of GORD.
Methods: This is a retrospective cohort study using data collected between 2003 – 2023 in a quaternary referral centre. Patients over 18 years, referred for 24-hour pH-impedance monitoring for investigations into respiratory disease were included. An AET >4.2% was positive for GORD. A patient reported symptom questionnaire was used to categorise patients into those with oesophageal symptoms and extra-oesophageal symptoms. Oesophageal symptoms included chest pain and heartburn, and extra-oesophageal symptoms included cough, recurrent airway infections, vocal changes and throat symptoms such as irritation, constant clearing and laryngopharyngitis.
Results: A total of 438 patients were included. The mean age was 60 years. Concurrent asthma and COPD (72.1%, n=316) were the most common respiratory diagnoses. Almost half of all patients had GORD (49%, n=217). GORD was present in a large proportion of asymptomatic patients (38.0%, n=82) and those with extra-oesophageal symptoms (32.9%, n=71) (Figure 1). Chronic cough and throat symptoms were the most common extra-oesophageal manifestations of reflux (61.4%, n=269 and 29.8%, n=71). Those with recurrent airway infection had the highest proportion of patients with GORD (59%, n=27). There were no significant differences in FEV1 (p=0.55) , FVC (p=0.42) or FEV1/FVC (p=0.99) between those with and without diagnosis of GORD.
310
Case report: ocrelizumab induced colitis
Karly Potts and David Scott
Hunter New England Health, Newcastle, Australia
Introduction: Ocrelizumab is a humanised anti CD20 monoclonal antibody that is the sole disease modifying therapy for primary progressive multiple sclerosis. Fourteen case reports describing ocrelizumab associated colitis have been published. The majority describe disease onset within a few weeks therapy initiation. We herein report a case of severe ocrelizumab induced colitis following five years of therapy.
Case report: A 68-year-old male presented with a four-week history of non-bloody diarrhoea and associated generalised abdominal pain. Pertinent medical history consisted of primary progressive multiple sclerosis, managed with 6 monthly ocrelizumab for the proceeding five years. Abdominal CT revealed mild mural thickening from the caecum to the descending colon. Stool testing for was positive for Blastocystic species, but otherwise negative for bacterial, viral, and parasitic pathogens. Colonoscopy demonstrated multiple deep ulcers in the left colon and normal intervening mucosa. There was near complete denudation of the right colon. Biopsy showed extensive ulceration with focal ischaemic changes and an inflammatory infiltrate characterised by an absence of B cells (figure 1). CMV was excluded by serology and biopsy. The patient failed to improve following 48 hours of empirical intravenous ceftriaxone and metronidazole. Oral budesonide and 100mg intravenous methylprednisone were commenced for severe drug induced colitis. A surgical opinion was sought for consideration of colectomy, but symptoms improved following steroid initiation, and no intervention was required. Prednisone was commenced at 60mg daily, to be gradually tapered. On day 17 of prednisone therapy the patient experienced worsening abdominal pain. Inflammatory markers, previously down trending, had increased. Repeat CT abdomen demonstrated overall improved appearances, and stool culture was negative. Treatment was escalated to a three-day course of methylprednisone and tofacitinib added to ongoing budesonide. This resulted in clinical and biochemical improvement and was followed by prednisone taper. Three months later, the patient remained well, with normalisation of biochemical parameters. Budesonide and prednisone were weaned, and he continued tofacitinib.
325
Expect the unexpected: A rare case of duodenal-type follicular lymphoma
Joel Thio
Department of Gastroenterology and Hepatology, Logan Hospital, Brisbane, Australia
Introduction: Duodenal-type follicular lymphoma is a rare entity that usually follows an indolent course. Most cases usually present asymptomatic and are found incidentally on endoscopic examination of the small bowel. The most common finding on endoscopic examination is that of white polypoid nodules. We present a case of an incidental finding of duodenal-type follicular lymphoma in a 61-year-old male.
Case report: A 61-year-old Indian male presented to our service for further investigation of his iron deficiency anaemia with symptoms of generalised fatigue without obvious bleeding. He had a background of hypertension, ischemic heart disease, and benign prostate hypertrophy. Regular medications included perindopril, clopidogrel, rosuvastatin, and tamsulosin with dutasteride. Laboratory investigations revealed a haemoglobin of 127 g/L and a ferritin of 29 micrograms/L. He had a recent colonoscopy which was normal.
Discussion: Follicular lymphoma typically follows an indolent course, and management mainly involves close monitoring and commencing treatment once symptoms manifest. This case highlights the importance of increased vigilance of this condition with the potential for subtle appearances on endoscopy.
327
Does a restrictive blood transfusion strategy have better outcomes in upper gastrointestinal bleeding? Six years of real world data
Hirannya Karunadasa, Daniel Clayton-chubb, Stuart Roberts, Gregor Brown and Shara Ket
Alfred Health, Melbourne, Australia
Background and Aim: Transfusion of blood products is an important component of resuscitation in the management of upper gastrointestinal bleeding (UGIB). Randomised studies have suggested that use of a restrictive transfusion strategy is associated with reduced all-cause mortality and rebleeding rates. The applicability and generalisability of a restrictive transfusion strategy in clinical practice remains unclear. The aim of this study was to evaluate and compare outcomes of restrictive versus liberal transfusion strategies in patients with UGIB over a six-year period in a real-world setting.
Methods: A retrospective audit of patients presenting with or developing UGIB during admission in a quaternary referral hospital between 2018 to 2023 was conducted. Participants were excluded if they had lower gastrointestinal bleeding, had exsanguinating bleeding, were managed with outpatient gastroscopy or refused transfusion of blood products. Data collected included demographics, pathology results, transfusions, interventions and outcome data. Patients with a 24-hour nadir haemoglobin between 70g/L and 90g/L were stratified into a liberal transfusion group if packed red blood cells (PRBC) were transfused in that 24-hour period or into a restrictive transfusion group if they did not receive PRBC. The primary outcomes were mortality and rebleeding within 30 days of UGIB.
Results: Of the 1089 patients included, 413 (37.9%) patients had a 24-hour nadir haemoglobin between 70g/L and 90g/L qualifying for evaluation of restrictive versus liberal transfusion strategies. The male gender accounted for 64.4% (n=266/413) of patients. The median age was 72 years (IQR 57-82 years), and the median Charlson Comorbidity Index was 6 (IQR 4-8). The median 24-hour nadir Hb was 78g/L (IQR 74-84 g/L). The leading cause of bleeding was peptic ulcers at 35.1% (n=145/413), while 10.2% (n=42/413) of patients had variceal bleeding. Most patients were stratified into the liberal transfusion group with 298 (72.2%) patients being transfused PRBC within the first 24 hours, with a median of 2 units (IQR 1-3 units) transfused within 24 hours. Regarding primary interventions, 40.9% (n=169/413) of patients required endoscopic intervention, with 4 (1.0%) requiring angiographic intervention and 2 (0.5%) requiring surgical intervention. A significantly greater proportion of patients in the liberal transfusion group experienced rebleeding within 30 days (n=43/298, 14.4% vs n=8/115, 7.0%; p=0.04). Although a numerically higher occurrence of all-cause mortality within 30 days was noted in the liberal transfusion group, this difference did not reach statistical significance (n=27/298, 9.1% vs n=6/115, 5.2%; p=0.23). In terms of secondary outcomes, the liberal transfusion group had poorer outcomes with significantly higher proportions of cardiac and pulmonary complications, acute kidney injury and bacterial infection (see Table 1, p<0.05).
Conclusion: In the management of UGIB, a restrictive transfusion strategy appears to be associated with a significantly lower proportion of rebleeding and complications within 30 days of UGIB. This lends strength to current guidelines recommending restrictive transfusion strategy in the management of non-exsanguinating UGIB.
328
The effectiveness of budesonide orodispersible tablets in the real-world is lower than in clinical trials: a multicentre cohort study
Sarah Taylor1, Emily Barwick2, Varan Perananthan3, Sarah Lucas1, Ayushi Chauhan1, Catherine Yu1, Katrina Tan1, Diana Lewis1, Chamara Basnayake4, Hamish Philpott5, Sanjay Nandurkar6, Rebecca Burgell3 and Mayur Garg1,2
Background and Aim: Eosinophilic oesophagitis (EoE) is a chronic immune-mediated disorder that causes oesophageal dysfunction secondary to eosinophil-predominant inflammation. A budesonide orodispersible tablet (BOT) formulation has been shown to induce clincohistological remission in 57% of patients after 6 weeks of treatment, with histological remission in 93%. Real-world data for this medication however is currently limited. Previous Pharmaceutical Benefits Scheme (PBS) prescribing criteria mandated evidence of histological remission as defined by a peak eosinophil count of fewer than 5 eosinophils per high power field (hpf) within 12 weeks, but this has now been changed to allow treatment for up to 48 weeks. This study aimed to evaluate the real-world efficacy and adherence of patients with EoE treated with BOT at five tertiary centres in Victoria and South Australia.
Methods: A retrospective medical record review of patients aged 18 years and over with a confirmed histological diagnosis of EoE (>15 eosinophils per hpf) and that were treated with BOT between July 2019 until February 2024 at five tertiary centers was performed. Data collected included patient demographics, endoscopy reports, histopathology, clinical symptoms, and previous medical treatments. Outcomes were reported using descriptive statistics.
Results: 83 patients (69 [83%] male, median age 37 [range 19-79] years) on 1mg BD BOT were identified, with follow-up data for median 11 (IQR 10-16) months following commencement of BOT. The peak median eosinophil count prior to commencement on BOTs was 40 (IQR 30-50) per hpf. Patients had a median duration of disease prior to BOT therapy of 3 (IQR 2-6) years. 65% of patients had an allergic diathesis (asthma, hay fever, eczema, allergic rhinitis, or an allergy). Other therapies had been trialed prior to BOT commencement in 92 % of patients, with the majority (81%) having had proton pump inhibitor therapy. 14 patients (17%) had required previous oesophageal dilatation. Prior to BOT therapy, 40% of patients had experienced a food bolus obstruction with none occurring post commencement of BOT. Fewer than half (47%) had a repeat gastroscopy performed within 12 weeks of BOT commencement (median 80 days, IQR 67-112). The median peak eosinophil count on repeat gastroscopy post induction with BOT was 2 (IQR 0-30). Histological remission was noted in 48 (58%), clinical remission (defined as absence of symptoms) in 35 (42%) and endoscopic remission (no endoscopic features of EoE) in 26 (32%). 14 (17%) of patients were noted on clinic review to be using the medication incorrectly, with none of these patients achieving histological remission. Adverse events were reported by 15% of patients, with the most common being altered taste and oesophageal candidiasis (6% and 4.76 %, respectively).
353
Intrusive endometriosis involving the small bowel: a case report
Thant Zaw1, Peter Boyd1,2 and Montri Gururatsakul1,2
1Cairns Hospital, Cairns, Australia;2James Cook University, Cairns, Australia
Introduction: Endometriosis, a condition characterized by the presence of endometrial tissue outside the uterine cavity, is a well-known affliction affecting approximately 10% of women of reproductive age. However, the occurrence of endometriosis in the small bowel remains a rare and intriguing phenomenon. This is a case report of a patient with small bowel endometriosis.
Case report: A 40-year-old woman with a history of severe endometriosis presented at the Emergency Department with severe, recurring abdominal pain localized around the peri-umbilical area. She reported minimal relief from analgesics and had one episode of vomiting along with a single occurrence of loose stool, without any signs of blood in the stool or diarrhea. Notably, she had undergone a lower segment Caesarean section in 2017. A CT scan of the abdomen and pelvis revealed multiple segments of thickened, inflamed small bowel near the terminal ileum, raising concerns of Crohn's disease (Picture 1). Subsequent colonoscopy revealed luminal narrowing at the terminal ileum without any obvious mucosal abnormalities, and a biopsy taken from the terminal ileum showed unremarkable findings. She was treated conservatively with bowel rest and a course of IV hydrocortisone followed by oral prednisolone with the plan for further evaluation with relook colonoscopy and MRI scan. Two weeks later, she returned to the ED with recurrent small bowel obstruction and signs of small bowel volvulus, indicating a possible closed-loop obstruction due to twisting of the mesenteric pedicle. The decision was made to perform a laparoscopic right hemicolectomy. During the surgery, cicatrizing lesions were observed in the terminal ileum, and the histopathology results confirmed the presence of endometriosis in the small bowel and appendix.
361
Correlation between colonic mural thickening and endoscopy findings
Osamah Al-obaidi1, Hydar El Jamaly2, Noureddin Al-Hajjiri2 and Mouhannad Jaber2
1Concord Hospital, Sydney, Australia;2Wollongong Hospital, Wollongong, Australia
Background and Aim: Colonic mural thickening (MT) is often reported on standard CT examinations of the abdomen and pelvis. It often presents a dilemma for the clinician on whether any further evaluation is needed, especially in the absence of any set guidelines. Our aim is to evaluate the significance of colonic MT and to assess its correlation with colonoscopy.
Methods: We conducted a comprehensive literature search using a strategy in Medline and this was extended to Pubmed and Embase. The studies included patients with increased Colonic wall thickness on CT scans, who underwent endoscopic evaluation. We used a random-effects model using pooled positive predictive value (PPV) with 95% confidence intervals (CI).
Results: A total of 15 cohort studies examining 1596 patients were selected having undergone both CT and colonoscopy. Of the 1596 patients with MT, 1152 had an abnormal colonoscopy. In the presence of MT of 3mm or more, the pooled positive predictive value (PPV) of malignancy was 0.23 (95% CI: 0.16-0.33) and that of all pathology was 0.65 (95% CI: 0.47-0.80). In the presence of MT of >5mm, the pooled positive predictive value (PPV) of malignancy was 0.15 (95% CI: 0.09-0.24) and that of all pathology was 0.71 (95% CI: 0.54-0.83). In patients with MT in the right colon, the pooled PPV of malignancy was 0.14 (95% CI: 7.4-23.7) and that of all pathology was 0.34 (95% CI: 0.18-0.55) as shown in Figure (1). In the left colon MT groups, the pooled PPV of malignancy was 0.18 (95% CI: 0.12-0.26) and that of all pathology was 0.74 (95% CI: 0.53-0.88).
369
Food bolus obstruction: what factors prevent clinicians from performing biopsies for eosinophilic oesophagitis during acute endoscopy?
Melissa Carroll1, Matilda Surtees1 and Nick J Talley1,2
1NSW Health - John Hunter Hospital, Newcastle, Australia;2University of Newcastle, Newcastle, Australia
Background and Aim: Eosinophilic oesophagitis (EoE) is identified in up to 50% of patients who present with a food bolus obstruction (FBO). Accepted guidelines recommend oesophageal biopsy be performed at index endoscopy for prompt diagnosis and management of EoE, however, this occurs in only 40% of food bolus presentations. To understand factors that impact clinicians practice, we collected data from all food bolus obstructions that presented over a 3-year period with the aim to understand potential barriers to obtaining oesophageal biopsies for the diagnosis of EoE during an acute presentation.
Methods: We conducted a retrospective cohort study of adult patients presenting with acute food bolus obstruction to a tertiary hospital from January 2020 to December 2022. Patient records were identified using endoscopy reporting software (ProvationMD) and International Classification of Disease (ICD) coding for ‘foreign body in oesophagus.’ Patients with intentional ingestion of foreign body objects were excluded. Patient demographics, medical comorbidities, drug therapy with anticoagulation and/or antiplatelet therapy and prior history of FBO was collected. Clinician reported macroscopic endoscopy findings, location and number of oesophageal biopsies, timing of procedure and histological findings were included. A diagnosis of EoE was confirmed where eosinophil-predominant inflammation was found (≥15 eos/hpf) on biopsy. Statistical analysis was performed using SPSS V.29 software and p-values <0.05 were considered significant. Pearson’s χ2 was used to assess for a significant relationship between timing and frequency of biopsy.
Results: A total of 251 patients with food bolus obstruction were identified over the 3-year study period, with 239 undergoing endoscopy 95.2%. Of these, EoE was histologically confirmed in 54 cases (22.5%), with those most likely to present between 45 and 59 years of age (27.4%) and predominately male 71.4%. A prior food bolus obstruction was recorded in 50.2% of patients and 15% of patients had a history of atopy. 4.4% of patients were receiving treatment for EoE. A total of 119 patients (49.7%) had oesophageal biopsies at index endoscopy. Endoscopy was performed mostly in business hours (8am and 5pm), with 161 patients (67.3%) and of those, 84 patients had biopsies (52.1%). There was no significant relationship between timing of procedure and having a biopsy (p=0.703). There was a significant relationship with those on antiplatelet therapy and having a biopsy with 5 out of 38 patients biopsied (p < 0.001), but not with those on anticoagulation therapy, 9.2% biopsied Vs 60.8% not biopsied (p=0.272). Patients with a history of atopy were more likely to have a biopsy (p=0.019) than those with a cardiac history (67.5% Vs 32.3%). There was no significant relationship between having macroscopic findings consistent with EoE and having a biopsy, 51 patients with reported findings and 22 biopsied (43.1%, p=0.299). Of those who presented with a further food bolus obstruction within 3-years (44 total), a diagnosis of EoE was the most common underlying diagnosis, 13 patients (29.5%).
Conclusion: Guidelines for the diagnosis and management of eosinophilic oesophagitis (EoE) recommend endoscopy and biopsy for histological diagnosis of EoE during acute food bolus obstruction. This study underscores the significant prevalence of EoE among patients presenting with food bolus obstruction, particularly among middle-aged males. It highlights the importance of considering patient history, such as prior obstructions and atopy, in managing and diagnosing EoE. The findings also suggest that while biopsy practices during endoscopy are influenced by factors like medication (specifically antiplatelet therapy) and patient history, the timing of the procedure does not appear to significantly affect biopsy rates. The recurrence of food bolus obstruction in patients with EoE emphasizes the need for ongoing management and potential treatment adjustments for these individuals.
370
Correlation between hypermetabolic PET/CT activity and clinically significant lesions found at endoscopic evaluation
Melissa Carroll, Patrick Felton and Steven Bollipo
NSW Health, John Hunter Hospital, Newcastle, Australia
Background and Aim: Hypermetabolic activity in the gastrointestinal tract prompting endoscopic evaluation is frequently encountered on PET/CT imaging performed for various clinical scenarios. Our aim was to collect data from endoscopic procedures performed for the indication “Abnormal PET scan of the GI Tract,” and analyze data to evaluate PET/CT avidity and the corresponding endoscopic and histological findings.
Methods: We conducted a retrospective cohort analysis of all adult patients who underwent endoscopy at a tertiary hospital over a 3-year period from January 2019 to December 2023, for reported hypermetabolic activity in the gastrointestinal tract on positron emission tomography/computed tomography (PET/CT) imaging. Patients were identified through endoscopy reporting software (ProvationMD), with the indication “Abnormal PET scan of the GI tract.” Patient demographics and indication for imaging was collected. We specifically looked at the location of avidity on PET/CT and whether there was correlation with endoscopic findings. We collected data on lesion location and size, histological findings, and additional or incidental findings which were not reported from PET/CT imaging. Clinically significant lesions were considered as high-grade dysplasia, invasive carcinoma and malignant (adenocarcinoma, lymphoma, melanoma). Statistical analysis was performed using SPSS V.29 software and p-values <0.05 were considered significant. Pearson’s χ2 was used to assess for significant relationship between size, location and clinical significance of found lesions.
Results: Of 331 patients who underwent endoscopy, a total of 62 patients (18.8%) were found to have a clinically significant lesion identified. There were 204 cases with a lesion identified at endoscopy correlating with hypermetabolic activity on PET/CT (61.6%), and of these 41 cases were clinically significant lesions 12.4%. An unknown primary malignancy was the most common indication for PET/CT (21.7%). There were 127 patients (38%) with a polypoid lesion found at endoscopy, with 68 lesions >20mm in size and of those, 47% were clinically significant (p = <0.05). Adenocarcinoma was the most common significant lesion (14%) on histology. PET/CT failed to detect 15 cases of clinically significant lesions (4.5%). There was a slight male predominance 55.9% Vs 44.1%, with endoscopy being performed more often in those who were aged 55 years or older (89%). Overall, 54 patients (16%) who underwent endoscopy had no macroscopic lesion identified during their endoscopic procedure.
Conclusion: We conducted a retrospective analysis of data from adult patients who underwent gastroscopy and/or colonoscopy based on positron emission tomography/computed tomography (PET/CT) imaging with gastrointestinal findings. The study provides valuable insights into the prevalence, significance, and characteristics of PET/CT avid lesions detected in the gastrointestinal tract, as well as their correlation with endoscopic findings. These findings contribute to our understanding of the diagnostic approach to patients with incidental PET/CT findings, informing clinical decision-making in this context.
389
An unusual presentation of appendicitis detected on colonoscopy in a young female with coeliac disease
Eleanor Wheatley and Mohammad Shir Ali
John Hunter Hospital, Newcastle, Australia
Introduction: Appendicitis is classically a clinical diagnosis, with urgent surgical management. It is often an emergency presentation with symptoms including acute pain migrating from the peri-umbilical region to the right iliac fossa (RIF), nausea, anorexia, and fever. Physical examination findings include tenderness in the RIF with rebound pain and peritonism. Subacute appendicitis on the other hand can be a more evasive diagnosis. In addition, fibrous obliteration of the appendix which is a histological diagnosis, can mimic acute appendicitis. Here we present an unusual presentation of appendicitis (with fibrous obliteration) which went undetected on the initial clinical assessment and cross-sectional imaging but was eventually detected on colonoscopy.
Case report: We report a 19-year-old female presenting with subacute/chronic RIF pain on a background of coeliac disease and type 1 diabetes. The patient had 3 prior emergency presentations with generalised abdominal pain spanning a 2-month period, each time having worsening RIF pain which had deteriorated over a series of days. The patient presented a final time to the emergency department with RIF pain and nausea. With no other classical symptoms of appendicitis other than generalised pain and guarding on admission, differentials included pelvic inflammatory disease (PID), urinary tract infection, ureteric calculus, inguinal hernia, and ovarian pathology. Diagnostic workup included abdominal ultrasound which excluded ureteric calculi and renal tract pathology, however displayed hyperaemia and mild mural thickening of the terminal ileum. Subsequent computed tomography (CT) scan showed similar findings suggestive of terminal ileitis. Notably, there were no features of appendicitis on this initial CT scan. Colonoscopy subsequently confirmed appendicitis by visualisation of pus emanating from the appendiceal orifice and congested mucosa at the site. The terminal ileum appeared completely normal on colonoscopy. A repeat preoperative CT showed an enlarged and inflamed retrocaecal appendix. The patient then underwent a laparoscopic appendicectomy without any sequelae. The histology of the surgical specimen revealed focal mucosal ulceration consistent with appendicitis. In addition there was prominent fibrous obliteration of the tip of the appendix a condition that can also mimic acute appendicitis.
398
Unexpected diagnosis: collagenous ileitis in a patient without diarrhea
Fei Yang Pan1 and Ahmad Alrubaie1,2
1Macquarie University Hospital, Sydney, Australia;2Bankstown-Lidcombe Hospital, Sydney, Australia
Introduction: Collagenous ileitis (CI) is extremely rare, with only four reported cases. Two additional cases were medication-induced by mycophenolate and duloxetine. CI, part of collagenous enteritis, features thickening of the mucosal subepithelial collagen band, chronic inflammation, increased epithelial lymphocytes, and epithelial detachment. The cause of subepithelial collagen deposition in the GIT is unknown, but research suggests an inflammatory process with profibrogenic mediators. Symptoms include diarrhea, altered bowel habits, epigastric pain, and bloating. CI is isolated to the ileum, unlike collagenous sprue (CS), which affects the proximal small intestine. Diagnosis requires histopathology confirming a thickened subepithelial collagen band, typically over 10 μm, similar to the criteria for collagenous colitis (CC).
Case Report: A 77-year-old female presented with recurrent melena and iron deficiency anaemia. A video capsule endoscopy revealed gastric antral vascular ectasia (GAVE) and mild to moderate circumferential congestion and erythema in the small bowel. Her medical history includes diverticulitis, hypertension, asthma, hypercholesterolemia, anxiety, reflux, and endometrial cancer, for which she underwent a hysterectomy and salpingo-oophorectomy. She is currently on rosuvastatin, rabeprazole, and sertraline. On 29/02/24, she underwent an antegrade double-balloon endoscopy, which provided views up to the proximal ileum which demonstrated a 60 to 70 cm segment of abnormal mucosa with erythematous changes and nodularity in the distal jejunum and proximal ileum. Biopsies of the distal jejunum showed normal mucosa except for mild oedema of the lamina propria, without increased inflammation or evidence of microscopic colitis. Biopsies of the proximal ileum revealed mildly oedematous ileal mucosa with some broadening of the villi and a patchy increase in the subepithelial collagen plate between 10 and 20 μm, confirmed by Masson trichrome staining. Interestingly, terminal ileum biopsies performed on 16/01/24 showed normal ileal mucosa. She was subsequently started on a daily dose of 9 mg of budesonide with good effect. A repeat colonoscopy is planned soon to assess both the colon and ileum for collagenous disorders.
410
Summary of pharmaceutical industry clinical trials of biologics for eosinophilic oesophagitis in Australia and internationally: Substantial contributions possible in Australia, but room for improvement
Rity Wong1, Hamish Philpott1,2 and Thomas Lokan1
1Northern Adelaide Local Health Network, Adelaide, Australia;2University of Adelaide, Adelaide, Australia
Background and Aim: There is a need for additional medications to treat eosinophilic oesophagitis (EoE) due to a lack of efficacy or tolerability of current agents. Pharmaceutical companies are developing biologics often borrowed from related disease states (particularly inflammatory bowel disease, and atopic conditions such as asthma or dermatitis). Given our relatively small population overall, yet a high prevalence of EoE, we consider the Australian contribution to key international pharmaceutical industry studies of biologics in adult patients with EoE.
Methods: We interrogated our own database, as well as the Annual Progress Report for each agent, and cross validated Australian and international data using the online trial registry https://clinicaltrials.gov. Individual trial name, biological class and mechanism of action, recruitment time time window, screening number and failure rate as well as Australian and total recruitment number was calculated.
Results: Over the last 5 years (2019-2024), five (5) biologics have been trialled in Australia as part of international efforts (Table 1). The number of patients enrolled in these studies varied between 108 to 430, with the Australian contribution being between 10-26 patients per study (2-6%). There were between 4 and 12 sites in Australia for each study. Screen failure rates ranged from 0-57% at our site (Northern Adelaide Local Health Network - NALHN) and NALHN contributed between 25% and 66% of patients successfully enrolled in each of the 5 studies in Australia and overall, 43% of all Australian patients enrolled were from NALHN.
Conclusion: Australia can make a meaningful contribution to international pharmaceutical industry studies in EoE. To date, a small number of sites have enrolled a significant proportion of patients, suggesting that more focussed efforts in future can improve recruitment in Australia in future.
419
An early review of MetaPanel™ - a diagnostic metagenomic gastrointestinal pathogen assay
Michael Wehrhahn1, David Wood2, Nicola Angel2, Donovan Parks2, Rhys Newell2, Andrew Ginn1, Lutz Krause2, Paul Griffin2 and Jim Newcombe1
1Douglass Hanly Moir Pathology, Sydney, Australia;2Microba, Brisbane, Australia
Background and Aim: Gastrointestinal infection is routinely diagnosed by culture, PCR or a combination of both. However, the diagnosis is limited to pathogens that are targets in the multiplex PCR assay or detected on routine culture media. In March 2024, a comprehensive faecal metagenomics assay (MetaPanel™) was introduced through Sonic Healthcare Australia Pathology laboratories. This assay reports 115 DNA pathogens including bacteria and selected bacterial virulence factors, protozoa, helminths, viruses, fungi and microsporidia, in addition to 60 antimicrobial resistance (AMR) genes and a research use only dysbiosis measure incorporating diversity and richness scores.
Methods: A review of the first 79 MetaPanel samples was undertaken, focusing on type of referrer, patient demographics, detected pathogens, detected AMR genes, and proportion with low diversity and richness (defined as falling in the lowest decile of a healthy cohort).
Results: The average age of the referred patient was 47 years (11% under 18 years) and 59% were female. The most common referrers were community practitioners (53%, with about 1/5 of these having an interest in integrative medicine), followed by gastroenterologists (30%), and other specialists (16%) comprising haematologists, oncologists, rheumatologists, infectious diseases physicians and immunologists. A putative pathogen was identified in 19% of samples, including: enteropathogenic E. coli (EPEC) (3), Campylobacter concisus (3), Tropheryma whipplei (2), toxigenic Clostridium perfringens (2), toxigenic Staphylococcus aureus (1), Yersinia frederiksenii (1), toxigenic Clostridium difficile (1), Campylobacter jejuni (1), Aeromonas hydrophila (1) and Aeromonas caviae (1) with the former 6 pathogens not routinely identifiable by PCR or culture. AMR genes were detected in 29% of samples with 61% of these including AMR genes not co-detected with common host organisms, indicating a higher risk of patient-to-patient transmission (CTX-M Extended Spectrum Betalactamas (ESBL) (5), qnrB quinolone resistance (2), rmtD aminoglycoside resistance (2) and vanA/B vancomycin resistance (3)). In 82% of samples, the gut microbiome was classified as being of low diversity and/or richness.
Conclusion: Early results support the utility of a faecal metagenomics assay (MetaPanel) in diagnosing difficult-to-detect gastrointestinal pathogens and identifying carriage of clinically relevant antimicrobial resistance genes. Further studies are underway to investigate the impact of MetaPanel on patient management and clinical outcomes.
430
The first randomised controlled trial of Jorveza (budesonide) compared to PPI (pantoprazole) for eosinophilic oesophagitis: Progress report of a multi-site Australian study
Hamish Philpott1,2, Thomas Lokan1 and Edward Young1
1Northern Adelaide Local Health Network, Adelaide, Australia;2University of Adelaide, Adelaide, Australia
Background: Eosinophilic oesophagitis (EoE) is a chronic inflammatory condition that progresses to fibro-stenosis and recurrent food bolus impaction. Expert opinion proposes that Jorveza (budesonide) is more effective than PPI in resolving inflammation and reversing fibro-stenosis. The two agents have not been subject to a randomised controlled trial (RCT).
Methods: Ethics review board clearance of a 12 site (multicentre) study across Australia, for adult patients with EoE aged 18 years and over, with established diagnosis of EoE (>15 eosinophils per HPF) and no previous use of Jorveza. Treatment naïve patients are randomised to Jorveza 1mg Po BD or Pantoprazole 40mg Po BD, with repeat endoscopy in 8-10 weeks, biopsies of the lower and middle oesophagus, endoscopic reference score (EREFs) and symptom scores (EoEsA1 PRO and EoE – QOL-A) being completed. At clinic review patients responding (<5/HPF) continue treatment for another 8-10 weeks, with endoscopy, EREF’s and symptom scores repeated at weeks 16-20. Patients failing initial treatment cross- over to the alternative medication (PPI or Jorveza) for a period of 8-10 weeks prior to repeat endoscopy, EREF’s and symptom scores, again at week 16-20 from enrolment. Consenting patients at specific trial sites will undergo EUS and EndoFlip at week 8-10 and week 16-20. Target sample size 72 (36 each for Jorveza and PPI, anticipated treatment effect difference 25%, power 0.80), recruitment from December 2023 to December 2025.
Results: Enrolment commenced December 2023 and currently 5 of 12 sites are active (NALHN – Lyell McEwin and Modbury hospitals, Royal Adelaide Hospital, Flinders Medical Centre, Monash Medical Centre and Northern Hospital Epping). 19 patients have been enrolled (June 5th, 2024, all from NALHN) trial completed in 4 individuals. Patients mean age of 36 years (range 21-58) 12/19 (63%) being male. 15/19 patients (79%) presented with food bolus impaction, and all were on nil current treatment.
Conclusion: The first randomised controlled trial of Jorveza vs PPI is underway, feasible and recruitment to schedule. More data to follow, additional sites to activate will speed recruitment and results.
448
Vertigo and pancreatic malabsorption
John Evans
Queen Elizabeth II Jubilee Hospital, Brisbane, Australia;St Andrew's War Memorial Hospital, Brisbane, Australia
Introduction: Vertigo is a functional disturbance in which there is an illusory sense of movement either of self or of the environment, the result of asymmetry in impulses impacting on the right or left vestibular system due to dysfunction of the semi-circular canals, vestibular nerve, or brain stem and is divided into peripheral and central causes. Peripheral causes are considered due to particles in the semi-circular canals. Vertigo was the most common presenting symptom from studies in Primary Care, Emergency Rooms, and Dizziness Clinics. Management of Vertigo is supportive. Particle positioning manoeuvres (Epley or Sermont) can be used although recurrences are frequent; and medication can be tried for the acute clinical situation (antihistamines, and/or benzodiazepines, and/or anti-emetics) or for recurrent episodes (betahistine and/or prochlorperazine) although there seems to be no evidence of these drugs’ long-term efficacy.
Case Reports: Both husband & wife from a rural setting incidentally mentioned improvement in vertigo following management of pancreatic exocrine insufficiency (PEI). A further five female patients with PEI experienced vertigo. These patients also underwent tests of hearing, and Videonystagmography (Caloric testing) and were later reassessed. The manoeuvres or medications mentioned above were not utilised. All patients revealed prolonged symptomatic and objective improvement of Vertigo with management of malabsorption associated with PEI.
VERTIGO, VIDEONYSTAGMOGRAPHY, & PEI
+ rural couple
Conclusion: Vertigo may be a hitherto unrecognised, uncommon association of malabsorption due to PEI but appropriate management of PEI revealed long term, effective management of Vertigo. These improvements occurred despite the considered presence of particles in the semi-circular canals. Consideration of malabsorption in patients with Vertigo may enhance management of Vertigo.
472
Transmural changes of microscopic colitis using intestinal ultrasound: a case report
Peter Litwin1, Bhuwan Tandon1,2, Aude Van Oosterwyck1,2, Robert Bryant1,2,3 and Ryan M Mathias1,2,3
1Central Adelaide Local Health Network, Adelaide, Australia;2Inflammatory Bowel Disease Service, Queen Elizabeth Hospital, Adelaide, Australia;3The University of Adelaide, Adelaide, Australia
Introduction: The use of Gastrointestinal Ultrasound (GIUS) is well established in the evaluation of patients with inflammatory bowel disease, which is not the case in microscopic (or collagenous) colitis. Whilst a 2022 study of 498 patients by Koop et al. demonstrated abnormal CT imaging in this disease, only a single case report of GIUS abnormalities can be found in the literature. However, there are no reports demonstrating its use case as a non-invasive treatment modality in assessing treatment response.
Case Report: A 61-year-old female presented with a 12-week history of progressive diarrhoea and urgency (up to 14 times per day), initially watery but having become blood and mucous stained in the preceding 3 weeks. Her past medical history included high cholesterol, hypertension and anxiety, for which she was prescribed longstanding atorvastatin, amlodipine and venlafaxine. She was a non-smoker, had no recent antibiotic exposure, no over the counter medications and no family history of autoimmune disease. Biochemical abnormalities included hypokalaemia (2.6 mmol/L), an acute kidney injury (creatinine 110 umol/L) and an elevated C-reactive protein (40 mg/L). Stool samples were negative for infection and her faecal calprotectin was elevated at 189 ug/g (<50). Unprepared colonoscopy demonstrated a severe confluent pancolitis from the rectum to caecum with a normal terminal ileum. Gastrointestinal ultrasound (GIUS) demonstrated pancolitis with increased bowel wall thickening (maximum 5.6mm), modified Limberg 2 doppler activity and preserved wall stratification. Histology confirmed collagenous colitis with preserved crypt architecture, thickening of the subepithelial basement membrane and plasmacytosis. The patient was commenced on intravenous hydrocortisone 100mg QID with excellent clinical (bowel frequency reduced to 2) and biochemical response over a 48-hour period and was transitioned to prednisolone and later budesonide. Repeat GIUS 6 days post therapy demonstrated complete transmural healing with normalisation of bowel wall thickness and no increased colour doppler signal.
486
Not all right-sided colonic ulcers are Crohn’s disease: Entamoeba histolytica and Mycobacterium tuberculosis infections diagnosed at colonoscopy
Vanessa Chong1, Jin Lin Tan1,2, Biju George1, Mohamed Asif Chinnaratha1,2 and Damian Harding1,2
1Department of Gastroenterology and Hepatology, Lyell McEwin Hospital, Adelaide, Australia;2Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia
Introduction: Ulceration in the right colon is commonly caused by Crohn’s disease, but other causes including infection, malignancy and ischaemia should be considered. Distinguishing the aetiologies by symptoms alone can be difficult due to similar clinical presentations. Infectious causes are particularly relevant for those who have travelled or migrated from endemic areas. This case series outlines three cases of right-sided colonic ulceration caused by Entamoeba histolytica and Mycobacterium tuberculosis.
Case reports: Case 1) A 67-year-old female from Afghanistan experienced intermittent right iliac fossa pain and iron deficiency anaemia. Colonoscopy revealed discrete deep caecal ulceration. Biopsies sent for TB and amoebiasis PCR were positive for E. histolytica, with amoebic organisms seen on histology. Treatment with Tinidazole followed by paromomycin resulted in symptom resolution and endoscopic healing of colonic ulcers. Case 2) A 61-year-old female from Myanmar had several years of right-sided abdominal pain, diarrhea and weight loss. CT showed mural thickening in the caecum and ascending colon. Colonoscopy revealed a hemi-circumferential and ulcerated polypoid mass in the caecum. Biopsies were sent for TB PCR, culture (both positive for M. tuberculosis) and histology, which showed necrotising granulomatous inflammation. After 9 months of anti-tuberculous therapy her symptoms resolved. Follow-up colonoscopy showed resolution of the caecal mass. Case 3) A 31-year-old female from Nepal with previously diagnosed Crohn’s disease underwent a colonoscopy to evaluate worsening abdominal pain and altered bowel habits. CT showed extensive inflammation in the caecum and ascending colon accompanied with enlarged necrotic mesenteric nodes. Initial treatment with steroids and biologics was ineffective. Colonoscopy revealed deep ulcers luminal narrowing at the hepatic flexure. Biopsies were positive for M. tuberculosis. She was commenced on anti-tuberculous therapy with resolution of symptoms and currently scheduled for follow-up colonoscopy after 9 months of treatment.
Discussion: Amoebiasis is transmitted through ingestion of amoebic cysts, which develop into trophozoites in the intestines that in some will cause invasive disease. Colonoscopy typically shows discrete, deep ulcers in the proximal colon, sparing the terminal ileum and distal colon. Histology may show “flask-shaped” ulcers with amoebic trophozoites. Intestinal tuberculosis (ITB) constitutes 2% of TB cases worldwide, often from latent TB reactivation or ingestion of tuberculous mycobacteria. Colonoscopy often reveals ileocaecal disease, and histology, caseating sub-mural granulomas, unlike the transmural granulomas associated with Crohn’s disease. Tissue biopsies for PCR and culture are essential for diagnosing amoebiasis and ITB and should be considered at the time of colonoscopy.
488
Aortoesophageal fistula with life-threatening upper gastrointestinal bleeding: a case report
Xiaomin Ma1,5, Mohamed Reffai Syed Mohamed1, Bulent Baran1,4, Christine Welch1,4, Kevin Tian3,4, Donald Cameron2,4, Yew Toh Wong3,4 and Rozemary Karamatic1,4
1Department of Gastroenterology, Townsville University Hospital, Townsville, Australia;2Department of General Surgery, Townsville University Hospital, Townsville, Australia;3Department of Vascular Surgery, Townsville University Hospital, Townsville, Australia;4School of Medicine, James Cook University, Townsville, Australia;5School of Medicine, University of Queensland, Brisbane, Australia
Introduction: Aortoesophageal fistula (AEF) arises from an abnormal connection between the aorta and the oesophagus. It is defined by Chiari’s triad of mid-thoracic pain, sentinel arterial haemorrhage and exsanguination after a symptom-free interval. Only 20-45% of patients fulfil this criterion, and a high index of suspicion is required. AEF may result in fatal upper gastrointestinal bleeding (UGIB) if not promptly addressed, with a mortality rate of 47-77%. We present the case of a 71-year-old man with AEF-related unstable UGIB managed successfully with endoscopic and endovascular intervention.
Case Report: A 71-year-old man presented to an Australian regional hospital with chest pain and haematemesis on a background of a gastro-oesophageal junction adenocarcinoma with nodal metastases treated with palliative chemoimmunotherapy and radiotherapy. He had previous oesophageal dilatations and stents for dysphagia complicated by tissue ingrowth and stent migration. Six weeks prior to presentation, a fully covered stent was placed across a tight stricture, with clips used to secure the proximal end and an 18mm balloon inflated inside the stent. On presentation, he was haemodynamically unstable requiring aggressive resuscitation. Computed Tomography Angiography (CTA) demonstrated distal migration of the stent with no bleeding source identified. He was transferred to the tertiary referral hospital after detailed CTA review due to high suspicion for AEF in view of prior radiotherapy and endotherapy. A multidisciplinary discussion involving gastroenterology, general surgery, vascular surgery, anaesthetics and intensive care unit (ICU) occurred prior to endoscopy to ensure appropriate personnel were available. At endoscopy, large amounts of blood clot were found throughout the oesophagus. The stent was found in the distal oesophagus, with ulceration at the proximal edge of the stent at the site of a clip. Following stent removal, an excavated ulcer covered with granulation tissue started exsanguinating, requiring activation of massive transfusion protocol. A partially covered metal stent was deployed to tamponade the bleeding and vascular surgery immediately proceeded to endovascular aortic stent graft insertion. He was transferred to ICU in a stable condition. The oesophageal stent was endoscopically removed the following day to avoid necrosis of tissue trapped between the oesophageal and aortic stents. The patient did not rebleed after stent removal.
496
High prevalence of ARFID and orthorexia nervosa in gastroenterology patients: an evaluation of disordered eating in a large gastroenterology clinics cohort
Amy Luo1, Hannah Kim1, Jessica Green1, Annalise Stanley1, Jamee Barugh1, Jessica Peters1, Linda Yang1,2, Angela Khera1,2, Michael Salzberg1,2, Michael Kamm1,2 and Chamara Basnayake1,2
1St Vincent's Hospital Melbourne, Melbourne, Australia;2University of Melbourne, Melbourne, Australia
Background and Aim: Disordered eating (DE) in gastrointestinal (GI) clinics is highly prevalent but not well-characterised. Specific eating disorders like avoidant/restrictive food intake disorder (ARFID) and orthorexia nervosa have not been adequately studied in this population. This study aimed to evaluate the prevalence and characteristics of DE in GI patients, with a focus on ARFID and orthorexia, using screening tools, across organic GI disorders, disorders of gut-brain interaction (DGBI), and controls.
Methods: Consecutive patients at a single tertiary centre, from September 2022 to October 2023, were invited to complete an online questionnaire post clinic appointment. Patients with a GI disorder were invited if they had “organic” disease (inflammatory bowel disease (IBD) and/or coeliac disease), or DGBI, as per Rome IV criteria. Controls were defined as asymptomatic patients presenting for surveillance of polyps, positive faecal occult blood testing or those with H. pylori infection. The 63-item questionnaire included screening tools for ARFID (NIAS, EDY-Q), orthorexia nervosa (ORTO-7), GI-symptom specific anxiety (VSI), quality of life (EQ-5D-5L VAS), depression and anxiety (PHQ-4). DE is defined according to self-reported eating disorder (ED), recorded ED diagnosis on file, or established ED screening tool cut-off scores (NIAS: item 1-3 ≥ 10, and/or item 4-6 ≥ 9, and/or item 7-9 ≥10; EDY-Q: at least one of item 2, 10, 12 ≥ 4, and item 4 ≥ 4; ORTO-7 ≤ 19).
Results: Demographics: 292 patients completed the questionnaire from 1007 invitations (41.4% male, median age 46). 239 cases had a GI disorder (81.8%) and 53 were controls (18.2%). 64.4% had organic GI disorder (58.9% IBD, 4.5% coeliac disease, 1.0% both) and 17.5% had DGBI. 193 participants (66.1%) had DE; 23.3% with features of ARFID, 12.3% with features of orthorexia, 27.1% with features of ARFID and orthorexia, and 3.8% other. Patients with DGBI had the greatest likelihood of DE (82.4%), followed by organic GI disorder (65.4%) and controls (52.8%) (p = 0.006).
Patients with GI disorders: There was higher DE severity (NIAS p = 0.010; EDY-Q p = 0.030; ORTO-7 p = 0.011), GI-specific anxiety (p < 0.001), lower QoL (p = 0.018), and more food restrictions (p = 0.006) in GI disorders compared to controls, while DGBI patients exhibited even greater DE severity, GI-specific anxiety, depression, anxiety, and lower QoL than both organic disorders and controls (all p < 0.001 for DGBI vs. controls). There was greater GI specific anxiety (p < 0.001) and more food restrictions (p = 0.042) in organic disorders compared to controls.
Patients with disordered eating (DE): There was significantly higher GI specific anxiety, depression and anxiety, GI symptom severity, lower QoL and more food restrictions in those with DE compared to those without DE (all p < 0.001), and particularly in patients with both ARFID and orthorexia compared to those without DE (all p < 0.001). Participants displaying ARFID features had significantly greater GI specific anxiety (p < 0.001), GI symptom severity (p = 0.032) and lower QoL (p < 0.001) compared to those without DE. GI symptom severity was just significantly higher in ARFID than orthorexia (p = 0.049). Participants with DE had significantly higher GI symptom frequency (p = 0.035) and lower BMI (p = 0.046) than those without DE. There was no significant association between DE and GI disease activity or whether patients attended dieticians within the clinics.
Conclusion: This study reveals a high prevalence and severity of disordered eating, among GI patients who completed an online questionnaire, particularly those with DGBI. DE severity, anxiety, QoL, and food restrictions were also significantly worse in patients with organic disorders and DGBI. These findings suggest that routine screening for DE should be integrated into GI clinics to better identify and manage these disorders. Further studies are required to explore if treatment of comorbid DE improves psychological and GI symptom outcomes for patients.
497
Haemosuccus pancreaticus: a rare cause of gastrointestinal bleeding
Niamh Buckley1, Santhi Swaroop Vege2 and Christopher Blevins2
1Royal North Shore Hospital, Sydney, Australia;2Mayo Clinic Rochester, Rochester, USA
Introduction: Overt obscure gastrointestinal bleeding is a diagnostic challenge frequently faced by clinicians for which the possible etiologies are broad. We describe a rare case of Haemosuccus Pancreaticus occurring in the setting of chronic pancreatitis which should be considered as a differential in the correct clinical context.
Case Report: We present the case of a 63-year-old man with a sixteen year history of recurrent obscure upper GI bleeding. The pattern of his episodes consisted of intense epigastric pain followed closely by melena which relieved the discomfort. This was often associated with a transient elevation of lipase. They occurred at approximately six month intervals and subsequently increased in frequency to every other month. He underwent extensive investigation which failed to uncover the source of the bleeding including multiple gastroscopies, duodenosocopies, colonoscopies, capsule endoscopies, a CT angiography and a tagged red blood cell study. CT abdomen and pelvis revealed a suspected saccular splenic artery pseudoaneurysm measuring 1.5 cm that abutted the pancreatic duct (Figure 1). There were changes observed that suggested chronic pancreatitis, the likely aetiology of the pseudoaneurysm. This clinical picture was suspicious for haemosuccus pancreaticus and was confirmed with EUS evaluation at the time of bleeding. During the same procedure, five microcoils (Nester 10 mm) were placed via EUS which completely cessated flow in one aspect of the pseudoaneurysm and significantly reduced it elsewhere (Figure 2). However, three days later the patient had melaena and features characteristic of his previous episodes. Repeat CT demonstrated enlargement of the aneurysm and embolization of the splenic artery was performed by interventional radiology. This has thus far been successful, with complete resolution of his symptoms.
References
1. Han, B, Song, ZF, Sun, B. Hemosuccus pancreaticus: a rare cause of gastrointestinal bleeding. Hepatobiliary Pancreat Dis Int.2012; 11(5): 479-488.
2. Shah, AA, Charon, JP. Haemosuccus pancreaticus, an uncommon cause of upper gastro intestinal bleeding: Case report and review of the literature. J Pak Med Assoc.2015; 65(6): 669-671.
502
Severe idiopathic secretory diarrhoea with a profound sustained response to somatostatin analogues
Geovanny Gandy1,2, Alex Prudence1,2 and Miriam Tania Levy1,2
1Gastroenterology Department, Liverpool Hospital, Sydney, Australia;2University of New South Wales, Sydney, Australia
Introduction: Vasoactive intestinal peptide (VIP) secreting tumours are rare neuroendocrine neoplasms that present with chronic secretory diarrhoea and electrolyte derangements, with an incidence of 1 in 10 million people per year.1 Raised VIP levels and radiological evidence of a lesion, most commonly pancreatic, confirm the diagnosis. However, this can prove challenging, as tumours only transiently secrete VIP and levels may not be elevated between diarrhoeal episodes.2 We present a case of chronic secretory diarrhoea clinically compatible with a VIPoma, with rapid and sustained response to somatostatin analogue therapy despite negative investigations.
Case Report: A 35-year-old Vietnamese female presented with progressively worsening non-bloody diarrhoea up to ten times daily, with hypotension and hypokalaemia requiring resuscitation in intensive care, on a background of two years of loose bowel motions. She reported no fevers, infective symptoms, sick contacts, recent antibiotic use, or recent overseas travel. Stool microscopy, extended PCR and cultures were negative; faecal calprotectin and faecal elastase were normal. Thyroid function was normal, tuberculosis gamma interferon assay and coeliac disease serology were negative. Faecal chemistry was consistent with secretory diarrhoea. Panendoscopy was unremarkable and biopsies excluded coeliac disease, microscopic colitis and inflammatory bowel disease. Neuroendocrine screening was negative, including serum VIP 16.9 pmol/L (normal <50 pmol/L). Ga-68 DOTATE PET, multiphase CT, and EUS revealed no lesions. On clinical suspicion of a VIPoma, octreotide was trialled with sustained response and patient was transitioned to lanreotide. Initial cessation of lanreotide precipitated a relapse, but it was weaned successfully after four years.
References
1. Yao, JC, Eisner, MP, Leary, C, et al. Population-based study of islet cell carcinoma. Ann Surg Oncol. Dec 2007; 14(12): 3492-500. https://doi.org/10.1245/s10434-007-9566-6
2. Ma, ZY, Gong, YF, Zhuang, HK, et al. Pancreatic neuroendocrine tumors: A review of serum biomarkers, staging, and management. World J Gastroenterol May 21 2020; 26(19): 2305-2322. https://doi.org/10.3748/wjg.v26.i19.2305
511
Decoding gastrointestinal symptoms in systemic sclerosis: a cluster analysis of a large national prospective systemic sclerosis cohort
Alexander Strathmore1, Dylan Hansen1, Kathleen Morrisroe1,2, Alannah Quinlivan1,2, Susanna Proudman4, Jennifer Walker5, Joanne Sahhar3, Gene Siew-Ngian3, Lauren Host6, Wendy Stevens1, Mandana Nikpour1,2,7, Laura Ross1,2 and Chamara Basnayake1,2
1St Vincent's Hospital Melbourne, Melbourne, Australia;2University of Melbourne, Melbourne, Australia;3Monash University, Melbourne, Australia;4Royal Adelaide Hospital, Adelaide, Australia;5Flinders Medical Centre, Adelaide, Australia;6Fiona Stanley Hospital, Perth, Australia;7Royal Prince Alfred Hospital, Sydney, Australia
Background and Aim: Gastrointestinal disease (GI) is present in over 90% of patients with systemic sclerosis (SSc). As the most common organ manifestation, it causes significant morbidity and has a negative impact on quality of life. There exists substantial heterogeneity in the presentation of GI manifestations of SSc. The aim of this study was to evaluate whether there is clustering of GI symptoms in SSc, and whether these clusters have prognostic implications.
Methods: Adult patients (age ≥18 years) enrolled in the Australian Scleroderma Cohort Study (ASCS) with at least two study visits between 2007-2023 were eligible for inclusion. All patients had definite SSc, as defined by the 2013 ACR/EULAR classification criteria. Clinical data and patient-reported outcomes (PROMs) including HAQ-DI and UCLA GIT 2.0 Score, measuring physical function and GI severity, were collected annually. Seven variables were chosen and hierarchical cluster analysis with Jaccard similarity was performed using Ward’s linkage to identify subgroups. Univariate analysis with chi-square, ANOVA and Kruskal-Wallis rank tests, as appropriate, were performed to describe the differences between each subgroup. Kaplan-Meier survival analysis was performed to compare overall survival.
Results: A total of 1,652 patients were included, 85.6% female with median follow-up of 4.47 (IQR 2.86-9.2) years. Clustering of patients based on GI symptoms identified four subgroups. We observed clustering based on frequency and severity of GI symptoms. This linked to disease duration. Longer disease duration was associated with more frequent and more severe GI involvement. More frequent GI symptoms were associated with poor physical function. There was no clustering of GI symptoms based on anatomical GI tract location. Cluster 1 (n=1116) was the largest cluster characterised by a high frequency of all GI symptoms, and was characterised by vomiting and faecal incontinence. Patients in Cluster 1 reported more severe GI disease (UCLA-SCTC GIT 2.0 score) and significantly impaired physical function (HAQ score) compared to Clusters 2-4. Cluster 3 and 4 were characterised by the absence of multiple GI manifestations. Survival analysis demonstrated better long-term survival in patients with severe GI manifestations (Cluster 1) compared to Clusters 2 and 3; perhaps accounted for by the lower prevalence of cardiopulmonary complications in Cluster 1.
Conclusion: This large SSc cohort demonstrates that GI symptoms do not cluster into discrete upper and lower GI subgroups. Subgroups exist, with clear distinctions in frequency and severity of GI symptoms. Severe GI symptoms throughout the GI tract are a feature of longer disease duration and associated with significantly impaired physical function.
524
Surgery for non-malignant polyps continues to cause avoidable morbidity: Findings from a western cohort
Anthony Whitfield1,2, Julia Gauci3, Clarence Kerrison3,2, Sunil Gupta3,2, Oliver Cronin3,2, Timothy O'Sullivan3,2, Varan Perananthan3,2, Hunter Wang3,2, Francesco V Mandarino3, Brian Lam3, Eric Lee3,2, Nicholas Burgess3,2 and Michael J Bourke3,2
1Blacktown Hospital, Sydney, Australia;2Westmead Clinical School, University of Sydney, Sydney, Australia;3Westmead Hospital, Sydney, Australia
Introduction: Most non-malignant colorectal polyps (NMCPs) can be removed endoscopically with minimal morbidity and negligible mortality. Despite this, a high rate of surgical resection still occurs in western populations resulting in avoidable cost to the patient and to the health budget. To establish better pathways for endoscopic resection of NMCPs in Australia, we sought to understand the prevalence and outcomes of surgery in a state-wide representative sample.
Methods: A linked dataset provided by the Centre for Health Record Linkage (CHeReL), which included all admissions for surgery in patients aged 18 and over in New South Wales (NSW) between July 2007 and December 2017 was analysed. Australian classification of health interventions (ACHI) codes were used to filter the data set for colorectal surgery and International classification of diseases (ICD) codes were used to identify cases with a primary diagnosis of NMCP or colorectal cancer (CRC). Emergency surgery, inflammatory bowel disease and cases of total colectomy were excluded. Trends over two time periods (2008-2012 and 2013-2017) were compared. Major adverse events including mortality were captured 30 days from index surgery. Logistical regression was used to estimate risk ratios and 95% confidence intervals.
Results: From July 2007 - December 2017, 36,257 surgeries for NMCP and CRC were performed in NSW. 4181 (11.4%) were performed for NMCP. Excluding the rectum, NMCPs accounted for 16.4% of surgery for neoplasia. 51.1% (2137/4181) were performed in private hospitals. Between 2008-2012 and 2013-2017 there was no major difference in volumes of surgery for NMCPs (2008-2012,1968 cases; 2013-2017, 1948 cases; p=0.774). No significant differences were observed (p=0.708) and this remained the case for all subgroups: teaching hospital vs non and major city vs regional. A major adverse event was encountered in 19.3% of surgery for NMCPs (808/4181). Predictors for major adverse event included age, male sex, rectal surgery, American society of anaesthesiologists physical classification system (ASA) III & IV and laparotomy. Full cover health insurance was a negative predictor (OR 0.72, p=0.05, 95% CI 0.52-0.99). Mean length of stay was 12.8 days when a major adverse event occurred compared to 6.9 days when one did not (p=<0.001).
Conclusion: Surgery for NMCPs occurs at unacceptable rates in Australian Hospitals resulting in avoidable morbidity. Endoscopic resection pathways are required within public and private hospitals to address these avoidable poor outcomes for patients with NMCPs. Streamlining these patients to endoscopic resection will reduce inpatient workloads and associated health care costs.
529
Patients with functional gastrointestinal disorders spend less time in tertiary care when managed by a single clinician: Results of a multi-centre audit in South Australia
Ryan M Mathias1,2,3, Samantha Plush1,2, Elka Fairhead4, Benjamin Ngoi2,3, Louisa Edwards3, Alice Day1,2,3 and Robert Bryant1,2,3
1Inflammatory Bowel Disease Service, The Queen Elizabeth Hospital, Adelaide, Australia;2School of Medicine, The University of Adelaide, Adelaide, Australia;3Central Adelaide Local Health Network, Adelaide, Australia;4Department of Dietetics, The Queen Elizabeth Hospital, Adelaide, Australia
Background and Aim: Functional gastrointestinal disorders (FGID) are a group of disorders that manifest with abdominal symptoms. FGiDs have a serious impact on quality of life and represent a significant global burden on healthcare services. Guidelines now recommend an early, positive diagnosis in low-risk patients to reduce the risk of over-investigation. Establishing a strong clinician-patient relationship is a cornerstone of management. This requires both confidence in management and consistent messaging. The aim of this study was to identify factors that may contribute burden on two tertiary gastroenterology services.
Methods: This multi-centre, retrospective chart review of electronic medical records evaluated adults attending general gastroenterology outpatient clinics at two teaching hospitals. Occasions of service (OOS) were characterised as being seen by either a single clinician or discontinuous care. Discontinuous care was defined as multiple clinicians of varying seniority reviewing the same patient from first encounter during their time in service. Time to diagnosis and discharge, OOS per patient and number of harmful investigations were assessed. A harmful investigation was defined as one that involved either an invasive procedure such as endoscopic assessment or ionising radiation. Statistical analysis was performed with ANOVA, Kaplan-Meier plots and multiple logistic regression analysis.
Results: 275 patients (mean age 49 (SD 18), 72% female) were seen primarily for FGID between June 2021 - June 2022. When comparing single clinicians and discontinuous care, there was a protracted time to diagnosis between (42 vs 140 days, p<0.001) and time to discharge (158 versus 356 days, p<0.0001). Patients were more likely to receive a diagnosis early (HR 1.6, 95% CI 1.25; 2.04) and be discharged sooner (HR 1.83, 95% CI: 1.44,2.33) when seen by single clinicians compared with discontinuous care. Patients who received an early diagnosis by a single clinician spent less time in service following their diagnosis (80 days [IQR 0-183]) compared to those who experienced discontinuous care (378 days [IQR 217-616]); p<0.0001. There was a trend towards less harmful investigations in the single clinician group versus discontinuous care group (p=0.08).
530
Error and underestimation: capturing psychiatric complexity in disorders of gut-brain interaction
Paris Hoey1,3, Lynne Heyes2 and Trina Kellar1,3
1Department of Gastroenterology, Royal Brisbane and Women's Hospital, Brisbane, Australia;2Department of Consultation-Liaison Psychiatry, Royal Brisbane and Women's Hospital, Brisbane, Australia;3Faculty of Medicine, University of Queensland, Brisbane, Australia
Background and Aim: Disorders of gut-brain interaction (DGBI) are common, affecting 37.7% of Australians [1]. DGBI arise from past and present psychosocial stressors, via a complex interplay of nervous system, immune dysfunction, microbiome and mucosal-barrier dysfunction [2]. Whilst the prevalence of comorbid psychiatric disorders in DGBI is well established, medical literature oversimplifies the psychiatric profile of this population. Most studies use anxiety and depression self-reported screening measures for diagnosis [1]. Further, GI-psychologists and psychiatrists are few in medical services, leaving diagnosis to the primary physician. Post-traumatic stress disorder (PTSD), complex PTSD (C-PTSD), personality disorders (PD), eating disorders and persistent pain may be missed. We hypothesised that significant psychological factors contributing to complex DGBI were undiagnosed, thus untreated, in our cohort. This study aimed to compare the psychiatric profiles of patients with DGBI, pre- and post-psychologist formulation.
Methods: Retrospective cohort study, in a metropolitan tertiary-level adult hospital, specialist multidisciplinary outpatient clinic. Inclusion criteria: consecutive patients who completed full neurogastroenterologist and gastro-psychologist assessment January 2023 to May 2024. Diagnoses were recorded using Rome IV, DSM-5 and ICD-11 diagnostic criteria.
Results: 21 consecutive patients were included, 76% female, mean age 44. This represents a complex DGBI cohort, 57% had 3+ DGBI diagnoses, most commonly chronic nausea vomiting syndrome (52%), centrally mediated abdominal pain (43%), functional dyspepsia-postprandial distress syndrome (38%), and defecation disorders (33%). Prior to gastro-psychologist assessment, based on referral documentation and patient history, the primary psychiatric diagnosis was anxiety or major depressive disorder in 71% (n=15/21). PTSD in 1/21, C-PTSD 0/21, trauma without PTSD diagnosis 6/21. Active eating disorder 1/21, and PD 0/21. Notably, no psychiatric history was reported by 24%. Vastly more psychiatric complexity was uncovered following gastro-psychologist formulation (Figure 1). All met diagnostic criteria, with 52% suffering 3+ comorbid psychiatric disorders. Importantly, C-PTSD was present in 62%, PTSD 5%. 57% met criteria for active eating disorder (n=12/21), with 11/21 restrictive. PD present in 33%. Persistent pain disorder in 76%.
533
A double-blind, placebo-controlled, adaptive dose-response study to assess the acute effects of micro-doses of gluten in adults with treated coeliac disease (Gluten Threshold Study)
A James M Daveson1,2, Emma Craig1, Anuj Sehgal1, Jennifer Schaefer1, Michelle Colgrave3,4, Utpal Bose3,4, Melinda Hardy5, Jason Tye-Din5,6 and Robert P Anderson7
1Wesley Research Institute, Brisbane, Australia;3CSIRO Agriculture & Food, Brisbane, Australia;2Coral Sea Clinical Research Institute, Mackay, Australia;7Mackay Base Hospital, Mackay, Australia;4ARC CIPPS Edith Cowan University, Perth, Australia;5Immunology Division, The Walter & Eliza Hall Institute, Melbourne, Australia;6Department of Gastroenterology, The Royal Melbourne Hospital, Melbourne, Australia
Background & Aim: Evidence supporting a lower limit of gluten consumed in a gluten free diet (GFD) for Coeliac disease (CeD) is controversial. 20 mg per kg (20 parts per million) is accepted globally as the upper limit in gluten free foods except for Australia and New Zealand where “no detectable” gluten is enforced. We recently showed patients with CeD elevate serum interleukin-2 (IL-2) 2 – 6 hours after ingesting ~6 grams of vital wheat gluten (VWG). Reasoning serum IL-2 after a single gluten ingestion could be an objective, quantitative biomarker of gluten toxicity, our aim was to define an upper limit of gluten ingestion that did not elevate IL-2.
Methods: We performed an adaptive, double-blind, placebo-controlled, dose-ranging safety study at a single site. 51 patients with CeD on a GFD were randomised in 4 sequential cohorts and dosed on three occasions each a month apart. Participants were observed for 6h post ingesting VWG or placebo in gelatin capsules. Cohort 1 received 1000mg gluten protein on 3 occasions as “positive control”. Three subsequent Cohorts were randomised to receive 3 of the 4 sequential dose levels: 610mg, 90mg, 13mg or placebo; 8mg, 5mg, 3mg or placebo; & 3mg, 2mg, 1mg of gluten or placebo. Primary endpoint was the % of IL-2 responders (defined as mean IL-2 at 2, 4 and 6 h more than two standard deviations above the upper limit of normal from the placebo group). Secondary outcomes included symptoms assessed by modified CeD PRO before and hourly post dosing. Faecal and urinary gluten immunogenic peptides (GIP) were exploratory endpoints to assess adherence to GFD.
Results: The mean age was 53 (F25/M11). IL-2 levels were significantly elevated in 94% (17/18) of CeD patients after 1000mg gluten; 83% (10/12) after 610mg; 41% (5/12) after 90mg; 38% (5/13) after 13mg; 25% (3/12) after 8mg; 16% (2/12) after 5mg; and 33% (4/12) after 3mg. There were no severe adverse events or significant correlation between dose of gluten and symptoms. All pre food challenge faecal GIPS were negative.
Conclusion: All dose levels of gluten including <20mg were well tolerated but stimulated IL-2 elevation in CeD patients on a GFD. Low dose gluten challenges with serum IL-2 assessment may be useful for immune monitoring in clinical trials and may inform food regulations and support a no detectable gluten standard. CeD patients are unlikely to be aware of minute dietary exposures to gluten that reactivate gluten-specific immunity.
537
Effect of mushroom extract on patients with gastroesophageal reflux disease
William Wu1,2, Jerry Zhou2 and Vincent Ho2
1Ryde Hospital, Sydney, Australia;2Western Sydney University - School of Medicine, Campbelltown, Australia
Background and Aim: Gastro-oesophageal reflux disease (GORD) is a common condition that significantly impacts quality of life and imposes a substantial economic burden. Conventional treatments often have adverse effects and may not fully control symptoms, leading to interest in alternative therapies. Mushrooms have demonstrated gastroprotective properties in animal models and may offer a natural adjunct treatment for GORD. The aim of this study is to investigate the effects of a mushroom extract on GORD symptoms, quality of life, and biochemical markers in a single-blinded, randomized cross-over study.
Methods: Participants with confirmed GORD on manometry and ambulatory pH monitoring will be recruited from outpatient clinics. Each participant will receive both the mushroom extract and a placebo for four weeks each, in a randomized order. Symptoms and quality of life will be assessed using validated questionnaires. Blood tests will be performed at set intervals to measure changes in biochemical markers. The study aims to recruit 50 participants which is the sample size calculated to observe a difference of 30% in the proportion of patients with GORD treated for such symptoms and cross-over group non-treated (placebo) considering α = 0.05, and β =0.80.
Results: This study will provide initial data on the efficacy of mushroom extract in reducing GORD symptoms and improving quality of life. Changes in serum biomarkers will also be evaluated to understand potential mechanisms. This is a pilot study which is currently ongoing, preliminary results should be available at the time of presentation.
554
The effects of amyloidosis on the gastrointestinal tract in an Australian population
Myo Jin Tang, Nikil Vootukuru, Jason Tjahyadi, Daniel Clayton-Chubb, Olga Motorna, Brendan Wisnioski, Stephen Ting, Stephen Bloom, Simon Gibbs, Rohit Sawhney and Ola Niewiadomski
Eastern Health, Melbourne, Australia
Background and Aim: Gastrointestinal (GI) symptoms are common in systemic amyloidosis with a significant proportion attributed to amyloid deposition in the liver and GI tract. Patients with amyloidosis are also at risk of malnutrition. The aim of this study was to describe the GI and hepatic manifestations in patients with amyloidosis at time of diagnosis and over a follow up period of two years.
Methods: This was a single centre prospective observational study of patients with newly diagnosed amyloidosis with characterisation at baseline and then follow-up assessments at 6-, 12- and 24-month intervals. Gastric involvement was identified as the key measure due to suspected high prevalence of upper GI symptoms in the amyloid population and availability of a non-invasive diagnostic test. Patients underwent a gastric emptying study (GES), serum biochemistry, micronutrient screening, liver ultrasound (US) and fibroscan at the outlined intervals. A scored patient generated subjective global assessment (PG-SGA) was completed at time of diagnosis to assess nutritional status. Patients over the age of 18 with biopsy proven systemic or localized AL amyloidosis were included. Patients with pre-existing chronic liver diseases or gastrointestinal motility disorders were excluded.
Results: 16 patients were included in our study; 13 were diagnosed with ATTR and 3 with AL amyloidosis, respectively. The median age was 75 and with 87.5% male. Two patients only had serum biochemistry and micronutrient screening performed. Liver fibrosis was assessed with Fibroscan in 14 patients. The median liver stiffness measurement (LSM) at baseline was 8.4kPa. 10 patients had LSM tracked over the follow up period. 6 patients saw improvement to LSM with treatment while 4 patients saw worsened LSM despite treatment. At baseline, 5/14 patients had normal ALTs (median LSM 7.1(3.7-36.9)kPa) while 9/14 had elevated ALTs (median LSM 9.4(5.4 – 32.9)kPa). In the 9 patients with elevated ALTs, 6/9 saw improvement post treatment, 1/9 had increased ALTs and 2/9 did not have repeat ALTs. 13 patients had liver US performed. At baseline, 9/13 patients had normal liver US (median LSM in these 7.1(3.7 – 32.9)kPa), while 4/13 had hepatic steatosis on US (median LSM in these 12.4(6.8 – 36.9)kPa). In both cohorts, the majority (75% and 71% respectively) saw improvement in LSM after amyloidosis treatment. All 14 patients had normal hepatic synthetic function throughout the follow up period. 12/14 patients had elevated BNPs (which up-trended despite treatment). Four patients (28%) had abnormal GES; two at baseline (1x AL and 1x ATTR) and two developed on follow up (1x AL and 1x ATTR). None of these patients had GI symptoms. Three of these patients had mild gastric emptying delay which did not improve with treatment for their amyloidosis. One patient with ATTR amyloidosis and type 2 diabetes had moderate gastroparesis (on follow up) and did not receive treatment for amyloidosis. An additional two patients had upper GI symptoms but normal GES. Nutritional assessment as per the PG SGA was available in 10 patients. Seven patients were moderately malnourished (Score 4 or higher, category B); three of these patients had an abnormal GES. Micronutrient deficiencies were uncommon with only one patient with iron deficiency at baseline.
Conclusion: Elevated LSM may be an early indicator of liver involvement given majority saw improvement in LSM post treatment. However, LSM has little relationship with synthetic hepatic function. Malnutrition is prevalent in amyloidosis patients, with delayed gastric emptying a possible contributing factor in some cases only.
573
Utility of mean nocturnal baseline impedance in the diagnosis of refractory gastroesophageal reflux disease
Paris Hoey1,2, Abdul Raheem Q Khan1 and Lei Lin1,2
1Department of Gastroenterology, Royal Brisbane and Women's Hospital, Brisbane, Australia;2Faculty of Medicine, University of Queensland, Brisbane, Australia
Background and Aim: The mean nocturnal baseline impedance (MNBI) is a new reflux metric, based on multichannel intraluminal impedance and pH monitoring (MII-pH) which reflects the burden of longitudinal reflux and the integrity of esophageal mucosa. MNBI may be useful in cases where the MII-pH metrics are inconclusive for pathological reflux. Our aim was to assess the diagnostic utility of MNBI in the setting of inconclusive acid exposure time (AET).
Methods: We retrospectively identified all adult patients who underwent 24-48 hours pH impedance monitoring (Laborie and Medtronic) off Proton pump inhibitors (PPI) between January 2023 to May 2024 at two Brisbane metropolitan hospitals to investigate refractory reflux symptoms that did not adequately respond to PPI. MNBI was measured at the 5-cm impedance channel from three separate nocturnal 10-minute time periods. As per Lyon Consensus 2.0, we defined MNBI as positive when <1500 ohm, as inconclusive when between 1500-2500, and as negative when >2500 ohm. We defined AET as pathologic when >6%, as physiologic when <4%, and as inconclusive when between 4%–6%. Total reflux episodes (TRE) were defined as negative when <40/day, as inconclusive when between 40–80/day, and as positive when >80/day. The primary outcome was the rate of positive MNBI in patients with inconclusive AET to determine the yield of MNBI as an adjunctive evidence of reflux metric in the setting of diagnostic uncertainty.
Results: 86 adult patients were included in the analysis, with an average age of 54 years, and female prevalence of 69%. There was moderate correlation between MNBI and AET in our cohort with R= -0.46 (linear regression, p <0.001), but the correlation between MNBI and TRE was not strong (R=0.21, p=0.05). In seven patients with inconclusive AET on pH-impedance testing, application of MNBI led to a diagnosis of pathologic acid exposure in four patients (57%). In three patients with both inclusive AET and inconclusive TRE, application of MNBI led to a diagnosis of pathologic acid exposure in 2 patients (67%).
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
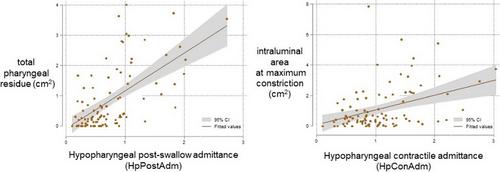
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


