Comparative analysis of chronic kidney disease risk: Inflammatory bowel disease vs. autoimmune diseases
Ming-che Chuang1, Cheng-Li Lin2, Fuu-Jen Tsai3,4 and Tsung-Yu Tsai1,4,5
1Center for Digestive Medicine, Department of Internal Medicine, China Medical University, Taichung, Taiwan (R.O.C.);2Management Office for Health Data (DryLab), Clinical Trial Center (CTC),, China Medical University, Taichung, Taiwan (R.O.C.);3Department of Medical Research, China Medical University Hospital, Taichung, Taiwan(R.O.C.);4School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan (R.O.C.);5School of Medicine, China Medical University, Taichung, Taiwan(R.O.C.)
Background and Aim: Autoimmune diseases, such as systemic lupus erythematosus, rheumatoid arthritis, and type I diabetes mellitus, increase the risk of chronic kidney disease (CKD). Similarly, inflammatory bowel disease (IBD) patients also face an elevated risk of CKD, yet this is frequently disregarded due to an assumption that the occurrence and severity of kidney dysfunction are lower compared to other autoimmune diseases. However, the comparison of CKD risk between autoimmune diseases and IBD remains unknown. In this study, we aim to evaluate the risk of CKD between patients with autoimmune disease and IBD.
Methods: Using the National Health Insurance database in Taiwan, we compared 11336 patients who were diagnosed with autoimmune disease with 2834 IBD patients during 2009-2019. Autoimmune diseases included as fellow: systemic lupus erythematosus, rheumatoid arthritis, psoriasis, systemic sclerosis, Sjogren's syndrome, Bechet’s disease, polymyositis, dermatomyositis, ankylosing spondylitis, autoimmune thyroiditis, and type 1 diabetes mellitus. We applied Cox regression analysis to estimate hazard ratios (HRs) for CKD in autoimmune disease and IBD.
Results: The mean follow-up of patients with autoimmune disease and IBD was 6.06 and 5.99 years in this study (Table 1). We found that 346 events developed in 68669 person-year in patients with autoimmune disease compared with 78 events in 16988 person-year in patients with IBD (adjusted HR [aHR]: 1.09; 95% confidence interval [95% CI]: 0.85 to 1.39, p=0.51). However, we further divided IBD patients into ulcerative colitis group and Crohn's disease group and then evaluated the CKD risk with autoimmune disease separately. 29 events developed in patients with Crohn’s disease (aHR: 1.84; 95% CI, 1.25 to 2.69, p=0.002), and 49 events developed in patients with ulcerative colitis (aHR: 0.88; 95% CI: 0.65 to 1.18, p=0.39) (Table 2). The cumulative incidence of CKD was higher in patients with Crohn’s disease compared to the autoimmune disease patients (Figure 1).
15
Vedolizumab-induced reactive arthritis: A rare adverse effect
Joel Thio
Department of Gastroenterology and Hepatology, Logan Hospital, Australia;Faculty of Medicine, University of Queensland, Brisbane, Australia
Introduction: Vedolizumab is a gut-specific humanised monoclonal antibody used in inflammatory bowel disease. It is an alpha-4 beta-7 integrin inhibitor, preventing lymphocytic adhesion to mucosal addressin cell adhesion molecule-1 in the gastrointestinal tract, reducing inflammation. Amongst the adverse effects of Vedolizumab, reactive arthritis is uncommon, only being mentioned amongst the literature in one other case report. We present a case of Vedolizumab-induced reactive arthritis in a patient known to our service.
Case Report: We describe a 71-year-old male known to our service who developed joint pains and effusions several weeks after commencing induction therapy with Vedolizumab for ulcerative pancolitis. Joint aspiration (Table 1) revealed an inflammatory arthritis and sexually transmitted infections were excluded. Faecal calprotectin was elevated but similar to levels from a year before. Furthermore, flexible sigmoidoscopy findings were similar to findings from before Vedolizumab induction therapy was initiated. A diagnosis of Vedolizumab-induced reactive arthritis was made and treatment with steroids improved joint inflammation. Due to this, he was planned for subsequent treatment of his ulcerative colitis with an anti-tumour necrosis factor alpha agent.
Conclusion: This case describes the second known report of Vedolizumab-induced reactive arthritis. In our patient, Vedolizumab-induced reactive arthritis was diagnosed after excluding septic arthritis and crystal arthropathy on the joint aspirate. The temporal relationship of four weeks from when Vedolizumab was initiated on induction to the onset of polyarthropathy made this diagnosis more likely. We recommend increased vigilance of this adverse effect of Vedolizumab, especially in patients with new onset arthropathy, even though self-limiting.
21
Comparative effectiveness of upadacitinib versus ustekinumab in patients with moderately to severely active Crohn’s disease: a matching-adjusted indirect comparison
Lena Thin1, Christopher Ma2, Marla Dubinsky3, Jordan Axelrad4, Samuel Anyanwu5, Jacinda Tran5, Ana Lacerda5, Namita Joshi5 and Jenny Griffith5
1Fiona Stanley Hospital, Perth, Australia;2Inflammatory Bowel Disease Clinic, Department of Medicine, University of Calgary, Calgary, Canada;3Division of Pediatric Gastroenterology and Nutrition, Icahn School of Medicine, Mount Sinai, New York, USA;4Department of Medicine, Division of Gastroenterology, NYU Grossman School of Medicine, USA;5AbbVie Inc, Chicago, USA
Background and Aim: Upadacitinib (UPA), an oral Janus kinase inhibitor, and ustekinumab (UST), a parenteral IL 12/23 antagonist, are effective treatments for moderately to severely active Crohn’s Disease (CD). In the absence of head-to-head data, a placebo (PBO)-anchored matching-adjusted indirect comparison (MAIC) was conducted to indirectly compare efficacy of UPA vs UST.
Methods: Individual patient (pt)-level data from phase 3 UPA trials and published data from phase 3 UST trials were used. For induction, pts received UPA 45mg daily or PBO for 12 weeks or UST ~6mg/kg IV or PBO IV at week 0 with 8-week follow-up. For maintenance, UPA clinical responders were re-randomized to UPA 15mg, 30mg, or PBO daily for 52 weeks. UST clinical responders were re-randomized to 90mg SC (every 8 or 12 weeks) or PBO SC for 44 weeks. UPA pts had baseline (BL) CD Activity Index (CDAI) 220-450; those with prior UST or vedolizumab exposure were excluded. Treatment effect modifiers, including BL mean CDAI, Simple Endoscopic Score for CD (SES-CD), median C-reactive protein, prior biologic(s) failure, and disease location, from UPA data were weighted to match the UST population. Outcomes assessed were CDAI response (≥100-point decrease or CDAI <150), CDAI remission (CDAI <150), endoscopic response (SES-CD ≥50% decrease), and SES-CD ≤2. Separate MAICs were conducted for induction and maintenance; data reported for induction clinical outcomes are stratified by prior inadequate response to tumor necrosis factor inhibitors (TNFi-IR).
Results: A greater proportion of UPA- vs UST-treated pts achieved endoscopic response (difference 26.3%, P<0.001) and SES-CD ≤2 (difference 9.9%, P<0.05) at the end of induction. In TNF-IR patients, a greater proportion of UPA- vs UST-treated pts achieved CDAI response at the end of induction (difference 18.2%, P<0.05) and at the end of Week 8 (difference 26.0%, P<0.001). CDAI remission rates were also higher at end of Week 8 for UPA- vs UST-treated pts (difference 13.3%, P<0.05). Rates of achieving CDAI response and remission were similar between UPA- and UST-treated pts at the end of induction and Week 8 among bio-naïve pts. Following maintenance treatment, similar rates of SES-CD ≤2, endoscopic response, and CDAI remission were obtained in the total population of UPA and UST-treated pts.
Conclusion: Pts with moderately to severely active CD treated with UPA achieved higher rates of endoscopic (total population) and clinical (TNFi-IR population) outcomes during induction compared to UST-treated pts. Outcomes at the end of maintenance were similar for UPA and UST, however, results should be interpreted with caution due to low sample size.
22
Upadacitinib treatment is associated with improved clinical and quality of life outcomes in patients with crohn's disease: Results from the U-ENDURE long-term extension
Nabil Siddique1, David Rubin2, Edouard Louis3, Julian Panes4, Astrid Rausch5, Luc Biedermann6, Yoichi Kakuta7, Elena Dubcenco8, Ana Lacerda8, Tian Feng8, Benjamin Duncan8, Tao Wang8, Sharanya Ford8, Samuel Anyanwu8, Namita Joshi8 and Peter Bossuyt9
1Sir Charles Gairdner Hospital, Perth, Australia;2Inflammatory Bowel Disease Center, University of Chicago Medicine, Chicago, USA;3Department of Hepato-Gastroenterology and Digestive Oncology, University Hospital CHU of Liège, Liège, Belgium;4Inflammatory Bowel Diseases Unit, Hospital Clínic Barcelona, IDIBAPS, CIBERehd, Barcelona, Spain;5Gastroenterology Department, British Hospital, Buenos Aires, Argentina;6Department of Gastroenterology and Hepatology, University Hospital Zurich, Zurich, Switzerland;7Division of Gastroenterology, Tohoku University Graduate School of Medicine, Sendai, Japan;8AbbVie Inc., Chicago, USA;9Department of Gastroenterology, Imelda General Hospital, Bonheiden, Belgium
Background and Aim: Upadacitinib (UPA), an oral Janus kinase inhibitor approved for the treatment of moderately to severely active Crohn’s disease (CD), showed notable improvements in clinical response/remission, health-related quality of life (QoL), and fatigue reduction compared to placebo (PBO) in the phase 3 induction (U-EXCEL/U-EXCEED) and maintenance (U-ENDURE) trials. This analysis reports clinical, QoL, and fatigue outcomes of the U-ENDURE long-term extension (LTE) up to wk48 and safety up to wk204.
Methods: Patients (pts) who experienced a clinical response after 12wks of UPA 45 mg (UPA45) once daily (QD) induction (U-EXCEL/U-EXCEED) were re-randomized in the 52-wk U-ENDURE maintenance study (PBO, UPA 15 mg [UPA15] QD, or UPA 30 mg [UPA30] QD), and were eligible to continue in the LTE with their previously assigned treatment (blinded until the last pt completed maintenance wk52). Efficacy data were reported up to LTE wk48 (PBO [N = 89], UPA15 [N = 107], UPA30 [N = 173]; excluding pts who received open-label UPA30 rescue therapy). Assessments included clinical response/remission per stool frequency/abdominal pain score (SF/APS) or per Crohn’s Disease Activity Index (CDAI), Inflammatory Bowel Disease Questionnaire (IBDQ), and Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F). Safety was assessed in all pts (PBO [N = 223], UPA15 [N = 221], UPA30 [N = 229]) from wk0 of the maintenance study (including those who received rescue therapy) up to LTE wk204 (cut-off date: 01 Aug 2023).
Results: At induction BL, demographics and characteristics were similar for all treatment groups. At LTE wk0, more pts receiving UPA vs PBO achieved clinical remission (SF/APS: PBO 73.0%, UPA15 78.3%, UPA30 80.3%; CDAI: PBO 75.3%, UPA15 81.3%, UPA30 80.9%; Figure 1A-B); sustained through LTE wk48. Clinical efficacy was accompanied by positive QoL outcomes, as shown by improved IBDQ and FACIT-F scores over time (Figure 1C-D). The mean [95% CI] changes from induction BL in IBDQ and FACIT-F were sustained from LTE wk0 (IBDQ: PBO 53.2 [44.7, 61.7], UPA15 60.3 [52.3, 68.3], UPA30 61.1 [55.7, 66.6]; FACIT-F: PBO 11.7 [8.8, 14.5]; UPA15 13.5 [11.0, 16.1], UPA30 15.2 [13.5, 16.9]) to LTE wk48 (Figure 1C-D). The occurrence of severe adverse events (AEs) and serious AEs was lower in pts treated with UPA vs PBO, except for numerically higher rates of AEs of special interest (herpes zoster, adjudicated gastrointestinal perforations, neutropenia, lymphopenia, creatine phosphokinase elevation, and hepatic disorders) in pts treated with UPA.
Conclusion: Long-term UPA treatment resulted in sustained clinical response/remission and improvements in QoL as measured by the IBDQ and FACIT-F compared with PBO, while maintaining an overall positive safety profile in pts with CD.
25
Effect of upadacitinib on extraintestinal manifestations in patients with moderately to severely active Crohn’s disease
Emily K Wright1,9, Jean-Frederic Colombel2, David Hudesman3, Qian Cao4, Subrata Ghosh5, Walter Reinisch6, Ana Lacerda7, Elena Dubcenco7, Chirag Doshi7, Samuel Anyanwu7, Tian Feng7 and David Rubin8
1St. Vincent's Hospital Melbourne, Melbourne, Australia;2Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, USA;3Inflammatory Bowel Disease Center, Division of Gastroenterology, NYU Langone Health, New York, USA;4Department of Gastroenterology, Inflammatory Bowel Disease Center, Sir Run Shaw Hospital, College of Medicine, Zhejiang University, Hangzhou, China;5College of Medicine and Health, University College Cork, Cork, Ireland;6Clinical Department of Gastroenterology and Hepatology, Medical University Vienna, Vienna, Austria;7AbbVie Inc., Chicago, USA;8University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago, USA;9The University of Melbourne, Melbourne, Australia
Background and Aim: Extraintestinal manifestations (EIMs) in patients with Crohn’s disease (CD) are challenging to treat and can negatively impact quality of life, with an estimated prevalence of 6–47%. The efficacy and safety of upadacitinib (UPA), an oral reversible Janus kinase inhibitor, was demonstrated in three phase 3 randomized controlled double-blind clinical trials; UPA has been approved for the treatment of moderately to severely active CD. We evaluated the effect of UPA treatment on EIMs in patients in these trials.
Methods: In two phase 3 induction studies, U-EXCEL (NCT03345849) and U-EXCEED (NCT03345836), patients with moderately to severely active CD were randomized 2:1 to receive 12 weeks of once-daily UPA 45 mg or placebo. Clinical responders to 12 weeks of UPA 45 mg were re-randomized 1:1:1 to the phase 3 maintenance study U-ENDURE (NCT03345823) for 52 weeks of once-daily treatment with UPA 15 mg, UPA 30 mg, or placebo. This analysis utilized EIM data from a form where investigators recorded the presence (yes/no) of 16 pre-specified EIMs. Baseline EIMs were assessed, as well as EIM resolution at weeks 12 of induction and 52 of maintenance therapy for patients with EIMs at induction baseline. Arthropathy EIMs (peripheral and axial arthropathy including sacroiliitis and ankylosing spondylitis), classic EIMs (arthropathy EIMs, episcleritis, uveitis, iritis, erythema nodosum, pyoderma gangrenosum, Sweet’s syndrome, and oral aphthous ulcers), anemia, and all EIMs (arthropathy and classic EIMs, anemia, primary sclerosing cholangitis, autoimmune hepatitis, venous thromboembolism, chronic obstructive pulmonary disease, bronchiectasis, and nephrolithiasis) were evaluated. Differences in EIM resolution rates with UPA vs placebo in the pooled induction and the maintenance studies were evaluated. Data were reported using non-responder imputation incorporating multiple imputation for missing data due to COVID-19.
Results: At baseline, EIMs were observed in 41.1% (420/1021) of patients included in the pooled induction studies, and 39.8% (200/502) of patients included in the maintenance study efficacy analyses (Table). At week 12 of induction, resolution rates of all EIMs, classic EIMs, and arthropathy EIMs were greater in those receiving UPA 45 mg (30.5%, 44.4%, and 44.3%, respectively) than in those receiving placebo (21.1%, 19.7%, 20.6%; P ≤ .05); resolution rates for anemia were greater with placebo vs UPA 45 mg (Table). At week 52 of maintenance, the resolution rates of all EIMs, classic EIMs, arthropathy EIMs, and anemia were higher with UPA 30 mg (35.6%, 30.6%, 31.9%, 44.4%; P ≤.05) and numerically greater with UPA 15 mg (24.6%, 19.4%, 22.6%, 27.6%) vs placebo (15.2%, 12.8%, 13.6%, 15.4%; Table).
Conclusion: Patients with CD who received UPA generally had greater EIM resolution than did patients who received placebo. Over one-third of patients had early resolution of classic and arthropathy EIMs within 12 weeks of UPA treatment. In the maintenance study, UPA 30-mg treatment resulted in a significantly greater proportion of patients achieving EIM resolution than placebo treatment.
26
Efficacy and safety of upadacitinib in patients with moderately to severely active Crohn’s disease: results from the U-ENDURE long-term extension
Nikola Mitrev1,2, Geert D'Haens3, Edouard Louis4, Edward Loftus Jr5, Miguel Regueiro6, Vipul Jairath7, Fernando Magro8,9,10, Hiroshi Nakase11, Elena Dubcenco12, Ana Lacerda12, Tian Feng12, Benjamin Duncan12, Tao Wang12, Sharanya Ford12, Samuel Anyanwu12 and Irina Blumenstein13
1Wollongong Hospital, Wollongong, Australia;2Blacktown Hospital, Blacktown, Australia;3Department of Gastroenterology and Hepatology, Amsterdam University Medical Centers, Amsterdam, The Netherlands;4Department of Hepato-Gastroenterology and Digestive Oncology, University Hospital CHU of Liege, Liege, Belgium;5Division of Gastroenterology and Hepatology, Mayo Clinic College of Medicine and Science, Rochester, USA;6Department of Gastroenterology and Hepatology, Cleveland Clinic Foundation, Cleveland, USA;7Department of Medicine, Western University, London, Canada;8Unit of Pharmacology and Therapeutics, Department of Biomedicine, Faculty of Medicine, University of Porto, Porto, Portugal;9Department of Gastroenterology, São João University Hospital Center, Porto, Portugal;10CINTESIS@RISE, Faculty of Medicine, University of Porto, Porto, Portugal;11Department of Gastroenterology and Hepatology, Sapporo Medical University School of Medicine, Sapporo, Japan;12AbbVie Inc., Chicago, USA;13Department of Internal Medicine 1, Goethe-University Hospital, Frankfurt, Germany
Background and Aim: Upadacitinib (UPA) is an oral Janus kinase inhibitor approved for the treatment of moderately to severely active Crohn’s disease (CD). The U-ENDURE (NCT03345823) maintenance study and long-term extension (LTE) evaluate the long-term efficacy and safety of UPA maintenance therapy. Here, we report the results of the U-ENDURE LTE.
Methods: Patients (pts) completing the U-ENDURE 52-week (wk) maintenance study were eligible to participate in the LTE and continue their previously assigned treatment (placebo [PBO], UPA 15 mg [UPA15] once daily [QD], or UPA 30 mg [UPA30] QD; blinded until the last pt completed maintenance wk52). Clinical response, clinical remission, endoscopic response, endoscopic remission, as well as high-sensitivity C-reactive protein (hs-CRP) and faecal calprotectin (FCP) were evaluated as-observed up to wk48 of the LTE among pts (PBO [N = 89], UPA15 [N = 107], UPA30 [N = 173]); excluding pts who received open-label UPA30 rescue therapy. Safety was assessed in all pts (PBO [N = 223], UPA15 [N = 221], UPA30 [N = 229]) from wk0 of the maintenance study up to LTE wk204 (cut-off date: 01 Aug 2023).
Results: At LTE wk0, the SF/APS clinical remission rates were 73.0%, 78.3%, and 80.3% for PBO, UPA15, and UPA30, respectively (Figure 1A). Similar rates were reported at LTE wk0 for CDAI clinical remission (PBO 75.3%, UPA15 81.3%, UPA30 80.9%; Figure 1B) and clinical response (CR-100: PBO 79.5%, UPA15 84.9%, UPA30 84.4%). Rates of clinical remission were stable through wk48 of the LTE. Endoscopic response (PBO 32.9%, UPA15 59.6%, UPA30 66.5%) and remission rates (PBO 27.8%, UPA15 42.4%, UPA30 47.3%) at LTE wk0 were sustained through wk48 with UPA while decreased with PBO (Figure 1C-D). At LTE wk0, the mean [95% CI] change from induction BL in hs-CRP was 1.8 [–0.4, 4.1], –13.2 [–17.9, –8.6], and –12.8 [–16.8, –8.9] for PBO, UPA15, and UPA30, respectively; sustained through wk48. Similar results were observed with FCP (mean [95% CI] change from induction BL: PBO 126 [–103, 356], UPA15 –2946 [–4121, –1772], UPA30 –1871 [–2577, –1165]). Severe adverse events (AEs) and serious AEs were lower with UPA treatment compared with PBO. The rates of most AEs of special interest were similar between UPA and PBO; however, numerically higher rates of herpes zoster, adjudicated gastrointestinal perforations, neutropenia, lymphopenia, creatine phosphokinase elevation, and hepatic disorders were reported in pts treated with UPA vs PBO.
Conclusion: In pts completing wk48 of the LTE, sustained efficacy was observed in clinical and endoscopic endpoints with over 2 years of UPA treatment, while maintaining an overall positive safety profile in pts with CD.
29
Crohn’s stricture resolution following treatment with high dose ustekinumab: A case report
Rachit Gupta and Emily K Wright
St Vincent's Hospital Melbourne, Melbourne, Australia
Introduction: Crohn’s disease (CD) is a chronic inflammatory bowel disease that can progress to bowel damage, defined as strictures, fistulas and abscesses. Ustekinumab, a monoclonal antibody to the p40 subunit of interleukin (IL)-12 and IL-23 is effective for induction and maintenance therapy for CD. The role of ustekinumab in patients with stricturing CD has not been defined. We describe a case of a patient with anti-TNF refractory stricturing colonic CD who achieved clinical, biochemical and endoscopic remission on ustekinumab monotherapy.
Case Report: We present a 40-year-old male with a 13-year history of stricturing colonic and perianal CD. He had previously failed anti-TNF therapy with both adalimumab [including when escalated to 40 mg weekly dosing] and IV infliximab [escalated to 10mg/kg 4 weekly dosing) used in combination with azathioprine 75 mg daily. Colonoscopy performed in the setting of active clinical [Harvey – Bradshaw index (HBI) = 4, and biochemical (CRP = 38 mg/ L, faecal calprotectin (FC) = 2300 mcg/g]) disease activity confirmed severe active inflammation with deep ulceration affecting the recto-sigmoid colon with a stricture at 35 cm preventing further passage of the colonoscope (Figure 1 top row). Histology from the stricture demonstrated inflamed granulation tissue with no granulomas or dysplasia. Treatment was changed from infliximab to ustekinumab with an IV induction dose of 390 mg and 90 mg every 4 weeks as maintenance treatment. The decision to use 4 weekly subcutaneous dosing was based on the severity of inflammation endoscopically and the fact that the patient had previously failed anti-TNF therapy increasing his risk of non-response to therapy. 12 months following commencement of ustekinumab there was evidence of clinical [HBI = 0] and biochemical improvement [CRP < 2 mg/L, FC not available]. Colonoscopy (Figure 1 bottom row) performed 24 months after commencing ustekinumab therapy demonstrated ulcer free mucosal healing with resolution of the stricture seen at earlier endoscopy. The endoscope was able passed to the terminal ileum. Histology of the distal colon and stricture demonstrated no acute inflammation.
Conclusion: This is the first known case of high dose ustekinumab therapy resulting in colonic stricture resolution in the setting of severe inflammatory CD. Prospective studies are needed to evaluate the efficacy of ustekinumab in stricturing CD.
33
Does ciprofloxacin reduce the need for surgery in perianal Crohn's disease
Sahar Pakneshan1, Zhen Hong1, Batsirai Matarise1, Mark Norrie1, Szymon Ostrowski1 and Muhammad Asif Shahzad1,2
1Logan Hospital, Brisbane, Australia;2Griffith University, Brisbane, Australia
Background and Aim: Perianal Crohn's disease affects 25%-35% of patients with Crohn's disease (CD). Treatment for perianal CD may include combination of biologic medications, immunomodulators, antibiotics or surgery. Amongst Antibiotics only two, namely metronidazole and Ciprofloxacin have been studied. To our knowledge, there is only one Randomised Controlled Trial that compared placebo with antibiotics in perianal fistulae which only included 25 patients. Despite of this sparse evidence both European society of Crohn’s Colitis (ECCO) and American Gastroenterology Association (AGA) recommend the use of Antibiotics in combination with a biologic over a biologic drug alone for the induction of fistula remission. We aim to evaluate the efficacy of ciprofloxacin with primary outcome as avoidance of surgery in perianal CD and determine optimal duration of Ciprofloxacin.
Methods: Retrospective data from hospital pharmacy database and the gastroenterology department database was evaluated to identify patients who were prescribed Ciprofloxacin for perianal fistulising CD between January 2019 and December 2023. The following data was collected: patients’ demographics, disease classification and severity, dose, duration, and adverse events of Ciprofloxacin; concurrent anti TNF agent; disease activity score before and after treatment with Ciprofloxacin; abscess development while on Ciprofloxacin and if surgery was required; the outcome of surgery.
Results: Overall, 67 encounters were identified that Ciprofloxacin was prescribed for active perianal CD. This involved 20 patients with 17 requiring multiple (2-7) courses. The starting dose for all patients was 500 mg twice daily. The duration of treatment ranged between 7 to 84 days with one patient longer than three months. The most common indication for starting the antibiotic was perianal abscess or fistula (42 encounters) which was detected either clinically or by MRI Pelvis. Fourteen encounters (4 patients) required surgical intervention while on Ciprofloxacin. Fifty-three encounters (16 patients,79%) had good clinical outcome as surgery was avoided. Significant adverse effects were noted only in one patient who developed Achilles tendinitis (total duration of treatment 215 days, 4 months of BD and 4 months of daily dose). Most common concurrent biologic agent was infliximab. Five out of twenty patients were new diagnoses of perianal CD; four of which were commenced on adalimumab and one on infliximab. The other 15 patients were already on anti-TNF therapy. Three of these fifteen patients were switched from adalimumab to infliximab and one from vedolizumab to Infliximab. Four of these 15 patients had their dose escalated whereas seven were kept on same dose. At the end of data collection period sixteen out of twenty patients were on infliximab.
Conclusion: Ciprofloxacin was able to reduce the need for surgery in 79% of encounters. It is important to start or optimise anti TNF therapy to avoid multiple courses of ciprofloxacin. It appears that optimal duration for ciprofloxacin for perianal abscess/fistula is at least 4 weeks.
34
Medium term outcomes and predictive factors of colectomy in patients with acute severe ulcerative colitis
Nicholas Wan1,2,3, Bhuwan Tandon2,3, Shahid Ullah2,3, Alex Barnes2,3 and Paul Spizzo2,3
1Gastroenterology Department, Lyell McEwin Hospital, Adelaide, Australia;2Gastroenterology Department, Flinders Medical Centre, Adelaide, Australia;3College of Medicine and Public Health, Flinders University, Adelaide, Australia
Background and Aim: Acute severe ulcerative colitis (ASUC) is a medical emergency associated with a significant mortality rate. The literature amongst medium-term outcomes of ASUC remain limited. This study aims to determine if early medical rescue therapy in patients with ASUC reduces the need for colectomy in the medium-term.
Methods: This was a retrospective cohort study conducted in an Australian quaternary IBD centre. Adult UC patients admitted between January 2015 and December 2021 that fulfilled the Truelove and Witts’ criteria for ASUC were identified and included. Demographic and clinical data was collected including date of colectomy and IBD-related readmission at 6 months. Patients who did not receive Infliximab (IFX) as rescue therapy or following discharge were excluded. Medium term was defined as within 1-3 years. The primary outcome of this study was colectomy (within 1-3 years), secondary outcomes were UC-related re-admissions at 6 months. Kaplan-Meier curves were utilised to investigate colectomy and readmission-free days from the initial flare to the commencement of biologics. Multivariate log binomial models were employed to explore significant factors related to colectomy and six-month readmission.
Results: 267 patients with UC flares were identified between the shortlisted timeframes. After exclusions, 32 patients remained (median age, 36 years (18-71); 56.3% male). The median time of admission to the commencement of IFX was 5 days (3-7.3). The overall colectomy rate was 34.4% (11/32); of these patients, 3 needed a colectomy during their index presentation and 8 within the subsequent 3 years. The median time from IFX commencement to colectomy was 9 days (5-330). 9 patients (28.1%) had a UC-related readmission within 6 months of discharge. Biochemical results (day 1 CRP, day 1 albumin) and demographics such as age and gender were analysed, however we could not find any statistically significant association with the need for colectomy or UC-related readmission. The overall trend and likelihood of undergoing colectomy and having a UC-related admission rose with longer durations between IFX initiation, however the results were not statistically significant.
35
Corticosteroid-free remission through 2 years of upadacitinib therapy in patients with moderately to severely active ulcerative colitis
Marla Dubinsky1, Raja Atreya2, Maria Abreu3, Hiroshi Nakase4, Silvio Danese5, Michelle R Kujawski6, Andrew Garrison6, Jason Eccleston6, Rebecca Smith7 and Remo Panaccione8
1Icahn School of Medicine at Mount Sinai, New York, USA;2First Department of Medicine, Friedrich-Alexander-University Erlangen-Nürnberg, Erlangen, Germany;3Department of Medicine, University of Miami Miller School of Medicine, Miami, USA;4Department of Gastroenterology and Hepatology, Sapporo Medical University School of Medicine, Sapporo, Japan;5Humanitas University and Humanitas Research Hospital, IRCCS, Milan, Italy;6AbbVie Inc., Chicago, USA;7Alfred Hospital, Melbourne, Australia;8Division of Gastroenterology and Hepatology, University of Calgary, Calgary, Canada
Background and Aim: Upadacitinib (UPA) is an oral, reversible Janus kinase (JAK) inhibitor, designed to preferentially inhibit JAK1, approved for the treatment of moderately to severely active ulcerative colitis (UC) with a positive benefit–risk profile vs placebo in the U-ACHIEVE Maintenance study.1,2 Here we assessed the achievement of symptomatic remission, corticosteroid (CS)-free symptomatic remission, and CS-free remission, through 48 weeks in the ongoing, 288-week, long-term extension (LTE) U-ACTIVATE study (NCT03006068).
Methods: Data from patients (pts) with clinical response to 8 week induction therapy,1,2 who completed the 52-week U-ACHIEVE Maintenance on once-daily UPA 15 mg (UPA15) or 30 mg (UPA30) and entered the LTE, were analyzed. Symptomatic remission (stool frequency subscore [SFS] ≤1 + rectal bleeding subscore [RBS] =0), CS-free symptomatic remission, and CS-free clinical remission (Partial Mayo Score ≤2 and no subscore >1), were evaluated through LTE Week 48 in pts who were in clinical remission (per Adapted Mayo Score) at the end of maintenance and stayed on the same dose (UPA15/15 and UPA30/30 groups), and in pts on UPA15 who were not in clinical remission and whose dose was escalated to UPA30 (UPA15/30 group) at LTE Week 0. All data are presented as observed.
Results: Of the 101 and 122 pts in the UPA15/15 and UPA30/30 groups who were in remission at LTE Week 0, 91.4% (85/93) and 90.6% (96/106), respectively, were in symptomatic remission at Week 48. Of UPA15/30 group pts, 64.3% (27/42) were in symptomatic remission at Week 48. Among pts who entered the LTE, 30.7% (31/101), 39.3% (48/122), and 37.5% (18/48) of UPA15/15, UPA30/30, and UPA15/30 group pts, respectively, had CS use at induction baseline. Most pts who entered the LTE in CS-free remission maintained this status over 48 weeks, with 89.3% (25/28) of UPA15/15 and 85.7% (36/42) of UPA30/30 group pts achieving this endpoint at Week 48. The proportion of UPA15/30 group pts achieving CS-free remission increased from 44.4% (8/18) at Week 0 to 64.7% (11/17) at Week 48. The proportion of pts with CS-free and symptomatic remission was similar between the UPA15/15 and UPA30/30 groups across timepoints; the proportion of UPA15/30 group pts achieving this endpoint increased from 38.9% (7/18) at Week 0 to 58.8% (10/17) at Week 48.
Conclusion: CS-free and symptomatic remission with continuous UPA15 or UPA30 treatment were maintained through 48 weeks of the LTE, suggesting the CS-sparing, long-term benefit of UPA therapy through ~2 years in pts with moderately to severely active UC. A subgroup of non-remitters on UPA15 were also able to achieve CS-free symptomatic remission with dose escalation to UPA30 with longer-term treatment.
References
1. Danese, S et al. Lancet2022; 399: 2113–28.
2. Vermeire, S et al. Lancet Gastroenterol Hepatol2023; 8: 976–89.
36
Efficacy and safety of retreatment with upadacitinib after treatment interruption in ulcerative colitis: Data from the phase 3 open-label extension study U-ACTIVATE
Remo Panaccione1, Jean-Frederic Colombel2, Marla Dubinsky2, Tadakazu Hisamatsu3, Valencia Remple4, Andrew Garrison4, Justin Klaff4, Michelle R Kujawski4, Brandon Baraty5 and Séverine Vermeire6
1University of Calgary, Calgary, Canada;2Icahn School of Medicine at Mount Sinai, New York, USA;3Department of Gastroenterology and Hepatology, Kyorin University School of Medicine, Tokyo, Japan;4AbbVie Inc., Chicago, USA;5Macquarie University Hospital, Sydney, Australia;6Department of Gastroenterology and Hepatology, University Hospital Leuven, Leuven, Belgium
Background and Aim: Upadacitinib (UPA) is an oral reversible Janus kinase (JAK) inhibitor designed to preferentially inhibit JAK1 approved for the treatment of moderately to severely active ulcerative colitis (UC). UPA may be temporarily discontinued for many reasons including adverse events (AEs) and lack of efficacy.1 As clinical consequences of discontinuing and restarting UPA are yet to be characterised, here, we assess the efficacy and safety of UPA retreatment in patients (pts) who lost response following UPA treatment withdrawal.
Methods: Pts with a clinical response to 8 weeks’ (wks) UPA 45 mg once daily (QD; UPA45) induction therapy in the Phase 3 U-ACHIEVE or U-ACCOMPLISH studies were re-randomised to placebo (PBO), UPA 15 mg QD (UPA15) or UPA 30 mg QD (UPA30) for the 52-wk maintenance phase of U-ACHIEVE. Pts randomised to PBO who lost response could enter the long-term extension (LTE), U-ACTIVATE, and be retreated with UPA15. Efficacy was analysed (i) at wk 4 of the LTE and (ii) at wk 48 of the LTE among pts with an inadequate response to UPA15 who dose escalated to UPA30 between wks 2 and 36. Exposure-adjusted event rates (EAERs) of treatment-emergent AE (TEAE) were assessed throughout.
Results: Of 223 pts with a clinical response to UPA45 induction randomised to PBO during maintenance, 112 (50.2%) lost response (mean [standard deviation (SD)] days to loss of response: 135.4 [84.6]) and 110 subsequently entered the LTE. Pts with loss of response vs those without were more likely to have a history of inadequate response, loss of response, or intolerance to ≥1 biologic (57.1% vs 46.8%, respectively) or corticosteroid use at baseline (42.0% vs 33.3%). After 4 wks of retreatment with UPA15, 75/108 (69.4%) and 39/108 (36.1%) pts achieved clinical response and remission, respectively (Figure A). In total, 38 (34.5%) pts dose escalated to UPA30 (mean [SD] days to escalation: 80.3 [57.8]); 30/31 (96.8%) and 22/31 (71.0%) achieved clinical response and remission at wk 48 of retreatment, respectively (Figure B). For safety during maintenance, 225 pts with 128.7 patient-years (PYs) of exposure (loss of response [n=112], 42.6 PYs; no loss of response [n=113], 86.1 PYs) were analysed. Generally, the EAERs of serious TEAEs were numerically lower in patients with vs without loss of response. However, patient years of exposure were low, restricting interpretation. During the LTE, EAERs were generally similar in pts who underwent dose escalation vs all pts.
Conclusion: In pts who experience loss of response following UPA withdrawal, efficacy can be recaptured following retreatment with UPA15 and UPA30. No new safety signals were identified.
Reference
1. Sandborn WJ, et al. Gastroenterology 2020;158:2139–2149.e14.
37
Time to relapse during upadacitinib maintenance therapy in patients with ulcerative colitis who had a clinical response to induction therapy
Marla Dubinsky1, Jordan Axelrad2, Michelle R Kujawski3, Jason Eccleston3, Xuan Yao3, Kavitha Subramaniam4,5 and Edward Loftus Jr6
1Icahn School of Medicine at Mount Sinai, New York, USA;2NYU Langone Health, New York, USA;3AbbVie Inc., Chicago, USA;4Gastroenterology and Hepatology Unit, The Canberra Hospital, Canberra, Australia;5ANU Medical School, Australian National University, Canberra, Australia;6Mayo Clinic College of Medicine and Science, Rochester, USA
Background and Aim: Upadacitinib (UPA) is approved for the treatment of ulcerative colitis (UC) based on results of a Phase 3 clinical trial program.1 This post hoc analysis evaluated time to relapse during maintenance in patients with a clinical response or remission after induction.
Methods: Patients with a clinical response (decrease in Adapted Mayo score ≥2 and ≥30% from baseline, and a decrease in rectal bleeding subscore [RBS] ≥1 or absolute RBS ≤1) after 8 weeks of UPA 45 mg once daily (QD) induction therapy (U-ACHIEVE Induction or U-ACCOMPLISH) were re-randomized 1:1:1 to placebo (PBO), UPA 15 mg QD (UPA15), or UPA 30 mg QD (UPA30) for 52-week maintenance therapy (U ACHIEVE Maintenance). The Kaplan–Meier method was used to estimate time to relapse (premature study discontinuation, treatment discontinuation owing to lack of efficacy or adverse event, or receipt of UC-related rescue therapy) in patients with a clinical response, and the subset of these in clinical remission (Adapted Mayo score ≤2, with stool frequency subscore ≤1 and not greater than baseline, RBS=0 and endoscopic subscore ≤1 without friability) after induction. Patients with initiation or dose escalation of corticosteroids during induction were considered non-responders. Hazard ratios (HRs) with 95% confidence intervals (CIs) and nominal p-values are presented.
Results: Overall, 413 (PBO, n=134; UPA15, n=135; UPA30, n=144) induction responders were analyzed, including 159 (n=54, n=47, and n=58, respectively) induction remitters. Median time to relapse with PBO was 169 days for induction responders and 224 days for remitters; the median was not estimable for UPA15 or UPA30 because <50% of responders and <25% of remitters with each dose had experienced a relapse by Week 52; Fig). In induction responders, the probability of relapse at Week 52 was lower with UPA15 (HR [95% CI]: 0.32 [0.23, 0.47]; p<0.001) and UPA30 (0.17 [0.11, 0.26]; p<0.001) vs PBO. Similar results were seen in remitters with UPA15 (0.21 [0.10, 0.44]; p<0.001) and UPA30 (0.11 [0.05, 0.26]; p<0.001) vs PBO. In both subgroups, the probability of relapse was numerically lower at most timepoints with UPA30 vs UPA15.
Conclusion: The probability of relapse during maintenance was lower with UPA15 and UPA30 vs PBO in induction responders and remitters. These results are consistent with the primary analysis, which demonstrated better efficacy with both UPA doses vs PBO across clinical, endoscopic, and histologic endpoints.1
Reference
1. Danese S, et al. Lancet 2022;399:2113–2128.
41
Terminal ileitis on imaging: how often is it Crohn's disease?
Carl Cosgrave1, Zacchary Tamsett1,2, Eliza Flanagan1,3, Irene Lu1, William Beattie1 and Neel Heerasing1,2
1Barwon Health, Geelong, Australia;2Deakin University, Geelong, Australia;3Monash University, Melbourne, Australia
Background and Aim: Terminal ileitis (TI) refers to inflammation of the distal ileum and ileocaecal valve. Although it is classically reported to be a hallmark of ileocolonic Crohn’s disease (CD), TI has an extensive differential diagnosis list1. It is a frequently reported computer tomography (CT) finding, however limited literature is available correlating radiological findings with endoscopic diagnosis of CD2,3. Given the range of differentials, it is essential to ascertain the underlying aetiology and investigate appropriately for the underlying cause of TI. This study aims to further investigate the correlation between radiological findings and diagnosis of CD, and to determine if standard biochemical markers may be able to be used to assist in correlation.
Methods: We performed a retrospective cohort study of people who underwent a CT abdomen at a single tertiary hospital between January 2018 and January 2024. We included all patients who had the phrases “terminal ileitis” or “inflammation of the terminal ileum” on their CT report. Medical records were searched for age, sex, medical history, endoscopy reports, histopathology, C-reactive protein (CRP) levels and albumin levels. Patients with a past history of CD or aged under 18 years were excluded from the study.
Results: We identified 66 patients with a new finding of terminal ileitis, after excluding those with known inflammatory bowel disease. The median age was 46 years, and 52% of the cohort were female. 30 patients (46%) underwent colonoscopy, 25 patients (83%) had successful terminal ileal intubation. Endoscopic evaluation combined with histopathology revealed a new diagnosis of Crohn’s disease in 8 patients (12%) (Figure 1). 65% of those with an “unknown diagnosis” underwent a colonoscopy. Of the people included in our study, only a minority of patients had faecal calprotectin performed as part of their work-up. 31 patients had stool cultures demonstrating infectious causes, 5 patients had acute surgical pathology (e.g. perforated diverticulitis or appendicitis). There was no statistically significant difference between the CRP (p=0.062) or albumin (p=0.081) levels amongst those with Crohn’s disease, infectious TI or surgical causes.
Conclusion: Although it is classically reported to be a hallmark of ileocolonic CD, TI has a broad range of differential diagnoses. Our investigation found that the majority of cases were infectious, with only a small minority being diagnosed with CD. The low rate of correlation between radiological findings and endoscopic confirmation of disease highlights a need for more robust assessment through laboratory investigations and potentially other imaging modalities such as intestinal ultrasound. We suggest a standardised approach and consistency in biomarkers, faecal calprotectin levels, and unless contraindicated, endoscopy with terminal ileum biopsies for patients with terminal ileitis to best understand their underlying aetiology.
References
1. Dilauro, S, Crum-Cianflone, NF. Ileitis: when it is not Crohn's disease. Curr Gastroenterol Rep.2010 Aug; 12(4): 249-58.
2. Asif, B. Shinn, B, Spataro, J, Kistler, C, Ahmed, M. CT Diagnosis of Terminal Ileitis with Clinical, Endoscopic, and Histologic Correlation - More Than Just IBD. American Journal of Gastroenterology.2018; 113:p S660-S661.
3. Pais, T, Fernandes, S, Fernandes, C, Ribeiro, I, Carvalho, J. Terminal Ileitis Found Upon Imaging: Is It Always Crohn's Disease?. American Journal of Gastroenterology.2014; 109(7):p 1089.
42
Predicting steroid failure in acute severe ulcerative colitis using the Admission Model for Intensification of Therapy in Acute Severe Colitis (ADMIT-ASC) in a regional health service
Carl Cosgrave1, Zacchary Tamsett1,2, Eliza Flanagan1,3, Sahan Withanage1, William Beattie1 and Neel Heerasing1,2
1Barwon Health, Geelong, Australia;2Deakin University, Geelong, Australia;3Monash University, Melbourne, Australia
Background and Aim: Acute severe ulcerative colitis (ASUC) is an important cause of morbidity and mortality in ulcerative colitis (UC). Intravenous corticosteroids are the mainstay of initial therapy, with assessment of clinical response at day 3 used to determine need for rescue therapy. Predicting the likelihood of steroid failure is therefore an important aspect of managing patients with ASUC, with estimated failure rates of 30-40% (1). The Oxford Group recently validated the Admission Model for Intensification of Therapy in Acute Severe Colitis (ADMIT-ASC) index for predicting steroid failure in ASUC (2). It combines C-Reactive protein (CRP), albumin and the Ulcerative Colitis Endoscopic Index of Severity (UCEIS) score to predict the likelihood of failure of steroid therapy at admission which could guide early initiation of rescue therapy (Table 1). We aimed to assess whether this index score is replicated in our cohort.
Methods: We performed a retrospective single-centre cohort study at a regional tertiary hospital amongst patients admitted with ASUC (ICD K51.90) between January 2010 and December 2020. We included those who fulfilled the Truelove and Witts criteria for ASUC(3), and excluded those under 18 years of age. Medical records were reviewed for demographics, biochemistry and endoscopy findings. UCEIS scores were calculated on the basis of endoscopy findings if not already documented. Steroid non-responsivity was determined by progression to infliximab, cyclosporine, or colectomy.
Results: 57 patients met the criteria for ASUC; 5 were excluded as their UCEIS scores were unable to be calculated. The median age was 38.5, and 43.9% were female. 40.4% of presentations with ASUC were new diagnoses (n=23), whilst 43.9% had been diagnosed more than 12 months ago (n=25). There was a positive correlation between higher ADMIT-ASC scores and failing salvage therapy (rs=0.41121, p=0.0.00246). There were higher steroid failure rates in our population rate than those reported in the initial ADMIT-ASC study population, particularly in patients with a score of 2 (Table 2). There was also a positive correlation between higher ADMIT-ASC scores and those requiring a colectomy (rs=0.40712, p=0.00274). The average time from presentation to endoscopy was 2.2 days (median 2 days), resulting in potential delays to identification of likely steroid failure. 75% of our ASUC patients (n=39) required salvage therapy 64% (n=25) receiving infliximab 5mg/kg, 23% (n=9) receiving infliximab 10mg/kg, and 13% (n=5) receiving cyclosporin. The overall colectomy rate was 35% (n=20).
Discussion: Whilst outcomes and colectomy rates in ASUC have significantly improved over the last 25 years, identification of patients likely to benefit from early escalation is essential to ongoing improvement in patient outcomes. Our study found higher steroid failure rates than that of the Oxford group which may reflect patient population, study size or a lower clinical threshold for escalation to rescue therapy. Whilst current PBS conditions in Australia restrict early escalation to rescue therapies such as infliximab, adopting established prediction criteria on admission will identify the group of patients most at risk of steroid failure, who will likely benefit from early intensification of management.
References
1. Turner, D, Walsh, CM, Steinhart, AH, Griffiths, AM. Response to Corticosteroids in Severe Ulcerative Colitis: A Systematic Review of the Literature and a Meta-Regression. Clin Gastroenterol Hepatol2007; 5: 103–110.
2. Adams, A, Gupta, V, Mohsen, W, et al. Early management of acute severe UC in the biologics era: development and international validation of a prognostic clinical index to predict steroid response. Gut2023; 72: 433-442.
Management of perianal fistulizing Crohn’s disease is not in keeping with guidelines – results from a multi-centre retrospective cohort study
Nicholas Wan1,3, Ryan Matthias2,3, Robert Bryant2,3, Barbra Andrin1, Sangwoo Han2 and Dharshan Sathananthan1,3
1Gastroenterology Department, Lyell McEwin Hospital, Elizabeth, Vale, Australia;2Inflammatory Bowel Disease Service, The Queen Elizabeth Hospital, Adelaide, Australia;3Adelaide Medical School, University of Adelaide, Adelaide, Australia
Background and Aim: Perianal fistulising Crohn’s disease (PFCD) affects up to 20% of patients with Crohn’s Disease (CD). PFCD can cause pain, purulent discharge and faecal incontinence, leading to significant morbidity and reduction in quality of life. The use of biologic therapy, antibiotics and surgical intervention remain the mainstay of management of PFCD. This study aims to review current practices in the management of PFCD across two large tertiary IBD-centres.
Methods: This retrospective cohort study assessed adult patients with PFCD between two tertiary Australian hospitals between 2006 to 2024. Patients with PFCD were identified using prescribing data. CD phenotype, therapy and fistula-related data were extracted. Biologic choice and therapeutic drug monitoring, antibiotic choice and duration, surgical intervention, and length of stay in hospital were monitored. Cross-sectional disease activity of perianal fistulizing disease was assessed at the time of data collection using clinical fistula symptom grade and radiological assessment were available. Clinical remission was defined as fistula symptom grade of 1 or less. Radiological remission was defined by healing fistula tracts or no active inflammation seen on MRI.
Results: 57 patients (median age, 40 years (31-54); 52.6% male) with PFCD were included in the study and followed over a median duration of 46.5 months (23.8-72.3). There were a total of 157 individual surgical procedures over the period, 2.75 per patient, most of which (94.2%) were examination under anaesthesia. Antibiotic therapy was dispensed for either perianal sepsis or an actively draining fistula in 26 patients, 2.65 number of courses per patient. The most common antibiotic prescribed was Metronidazole (68.1%), followed by Amoxicillin-Clavulanic acid (27.7%). The median duration of antibiotic therapy was 5 days (5-7) for Metronidazole and 5 days (5-10) for Amoxicillin-Clavulanic acid. There were 56 (98.2%) patients on biologic therapy. The most common biologic agents were Infliximab (75.4%), Adalimumab (19.3%) and Ustekinumab (3.5%). At the time of analysis, 48 patients (84.2%) were in clinical remission and 33 patients (57.8%) were in radiographical remission. In patients treated with infliximab, 37/43 (86%) had therapeutic drug monitoring performed. Amongst these, 30 (81.1%) had subtherapeutic levels (defined as Infliximab level < 10), with 12/30 (40%) of patients having active PFCD.
Conclusion: Across two tertiary IBD-centres, management of PFCD is variable and not in keeping with current guidelines. Short courses of antibiotics were used, and the majority of patients had subtherapeutic drug levels when tested. Optimising outcomes for patients with PFCD requires awareness of best practice and a multidisciplinary team approach.
59
Treatment benefits of upadacitinib based on disease severity, disease duration and number of prior biologics in patients with moderately to severely active ulcerative colitis: A post-hoc analysis of Phase 3 trial data
Edward Loftus Jr1, Joana Torres2, Gareth Parkes3, Ken Takeuchi4, Si Xuan5, James Crooks5, Justin Klaff5, Yuri Sanchez Gonzalez5, Robert Gilmore6,7 and Silvio Danese8
1Division of Gastroenterology and Hepatology, Mayo Clinic College of Medicine and Science, Rochester, USA;2Gastroenterology Division, Hospital Beatriz Angelo, Gastroenterology Division, Hospital da Luz, Gastroenterology Division, Hospital da Luz, Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal;3Barts Health NHS Trust, Barts and the London School of Medicine and Dentistry, London, UK;4Department of Gastroenterology and Hepatology, IBD Center, Tsujinaka Hospital Kashiwanoha, Kashiwa, Japan;5AbbVie Inc., North Chicago, USA;6Department of Gastroenterology, Mater Hospital, Brisbane, Australia;7Mater Research Institute, University of Queensland, South Brisbane, Australia;8University Vita-Salute San Raffaele, Milan, Italy
Background and Aim: Treatment goals in ulcerative colitis (UC) include controlling inflammation, reducing symptoms, and achieving normalization of quality of life and mucosal healing (MH). Results from Phase 3 induction and maintenance trials (U ACHIEVE [NCT02819635] and U-ACCOMPLISH [NCT03653026]) showed rapid relief of UC symptoms (abdominal pain, bowel urgency, stool frequency, rectal bleeding), normalization of fatigue, and MH with upadacitinib (UPA) treatment. Many patients in the program had been exposed to multiple biologics prior to entry and there is a need to understand UPA treatment benefits patients based on disease severity, disease duration, and number of prior biologics used.
Methods: Patients achieving a clinical response after 8-week induction treatment with UPA 45 mg QD were enrolled in the maintenance trial and re-randomized 1:1:1 to UPA 15 mg QD, UPA 30 mg QD or placebo (PBO) QD. The proportion of patients achieving efficacy outcomes were compared by disease severity (moderate vs severe based on adapted Mayo score), disease duration (by year quartiles), and prior biologic use (0, 1, or 2+) at induction week 8 and maintenance week 52. Outcomes included MH, defined as endoscopic score of 0 and Geboes histologic score <2.0, and complete symptom resolution with fatigue normalization (CSR-FN), defined as remission per partial adapted Mayo score (i.e., stool frequency subscore ≤1 and rectal bleeding subscore of 0), no bowel urgency, no abdominal pain and FACIT-Fatigue score ≥40.1.
Results: More biologic-naïve patients achieved MH normalization than biologic-experienced patients (Table 1). At week 8, 16.5% of biologic-naïve patients achieved MH with UPA 45 mg compared to 6.9%-9.1% of patients with prior experience of 1 or 2+ biologics. After 52 weeks of maintenance, 27.0% (UPA 30 mg) and 21.2% (UPA 15 mg) of biologic-naïve patients achieved MH at maintenance week 52, compared to 16.9%-18.8% (UPA 30 mg) and 12.2%-22.3% (UPA 15 mg) of biologic-experienced patients. Comparable rates of MH were observed regardless of disease severity and disease duration. Comparable rates of CSR-NF were observed regardless of disease severity, disease duration and prior biologic use. UPA 30 mg showed numerically higher efficacy rates vs UPA 15 mg at maintenance week 52.
Conclusion: UPA demonstrated benefits in MH and CSR-NF regardless of disease severity, disease duration, and prior biologic use. Higher rates of MH at the end of induction and maintenance were observed in biologic-naïve vs biologic-experienced patients, suggesting additional benefits from using UPA early in the treatment pathway as a first-line advanced therapy.
71
Upadacitinib was administered as a sequential salvage therapy for acute severe ulcerative colitis
David Huynh1,2, Myat Khaing1,2, Richard Fernandes1, Reuben Malloy2, Lei Lin2, Robert Gilmore1, Nicole Walker1, Emi Khoo1 and Jakob Begun1
1Mater Hospital Brisbane, Brisbane, Australia;2The Prince Charles Hospital, Brisbane, Australia
Introduction: Acute severe ulcerative colitis (ASUC) is a medical emergency with high mortality. Corticosteroids are the main treatment, but unresponsive cases may need infliximab or ciclosporin to avoid colectomy. JAK inhibitors show promise for moderate to severe ulcerative colitis (UC) and are being explored for ASUC. Upadacitinib, a newer JAK1 inhibitor, is effective even in refractory cases to advance therapies due to its proven rapid onset and efficacy. Our case is the first in Australia to introduce upadacitinib as sequential rescue therapy for ASUC.
Case Report: A 69-year-old woman with a family history of UC, was diagnosed with pan colonic UC in 2019 during a routine colonoscopy, which was part of surveillance for familial adenomatous polyposis syndrome. Initially, her disease was mild, and she remained asymptomatic without medical therapy, albeit having active disease biochemically and endoscopically. In early 2022, she commenced oral and rectal 5-ASA therapy, which led to biochemical and endoscopic remission within about three months. However, after a year of treatment, she experienced a severe flare, which rapidly responded to IV hydrocortisone followed by weaning oral prednisolone and was commenced on 6-mercaptopurine. Despite new treatment, she later presented with symptoms consistent with ASUC according to the Truelove and Witts criteria (Figure 1). Her CRP was elevated at 52 mg/L and experienced up to eight times bloody motions a day, alongside new-onset anaemia (Hb of 110 g/L). Following ASUC treatment guidelines, she was refractory to IV hydrocortisone and was rescued with IV infliximab 5mg/kg on day 5. There was initial partial response, however, her CRP increased to 17 mg/L despite improving symptoms. A repeat flexible sigmoidoscopy revealed persistent severe colitis with Mayo endoscopic score 3 and Ulcerative Colitis Endoscopic Index of Severity 6 (Figure 1), and therefore an escalated infliximab dose 10mg/kg was given but she still failed to respond. Colectomy was considered but deferred in favour of patient preference and decided to trial sequential medical rescue therapy with oral upadacitinib 45 mg daily alongside oral prednisolone wean. Following upadacitinib initiation, there was rapid improvement in bowel frequency, cessation of rectal bleeding, and reduction in CRP levels within seven days. Treatment progress was monitored non-invasively via intestinal ultrasound, revealing significant improvement in sigmoid bowel wall thickness from 6.6 mm to 3.6 mm by day 7. The patient was discharged on 45mg upadacitinib for sixteen weeks, gradually tapering prednisolone over six weeks. By week 12, complete remission was achieved clinically, biochemically, and sonographically, with sigmoid bowel wall thickness at 2.2 mm. Currently, the patient maintains stability on a maintenance dose of 30 mg upadacitinib orally once daily and at the 16-week mark, mucosal healing was confirmed via segmental colonic biopsies.
Conclusion: We reported a case that demonstrates the rapid effectiveness and efficacy of upadacitinib in the management of ASUC. This case serves as potentially another safe alternative therapy in not only moderate to severe UC, but also in ASUC as a sequential salvage therapy to avoid colectomy.
76
Safety of biologic therapies for the management of inflammatory bowel disease when used in combination with anti-rejection therapy in liver transplant recipients
Simone Chin1,2,3, Danny Con1, Matthew Choy1, Crispin Corte2,3, Patrick Hilley1, Adam Testro1 and Ashish Srinivasan1
1Austin Health, Heidelberg, Australia;2Royal Prince Alfred Hospital, Camperdown, Australia;3The University of Sydney, Sydney, Australia
Background and Aim: There are limited safety data on the use of biologic therapies in combination with anti-rejection therapies to manage inflammatory bowel disease (IBD) following liver transplantation (LT). Specific concerns regarding the safety of ‘gut-specific’ versus ‘systemic’ biologic therapies have been raised. This study aimed to compare the safety of these therapeutic combinations in IBD patients managed at Australia’s two largest LT centres.
Methods: This retrospective dual-centre Australian study included adult LT recipients who required biologic therapy for the management of IBD between 2004 and 2023. The primary outcome was safety events per biologic episode, defined as any documented infection, adverse event or intolerance associated with biologic therapy. Severity of safety events were categorised as mild (outpatient management with no disruption to biologic therapy), moderate (outpatient management with disruption and resumption of biologic therapy), and severe (requiring inpatient management). Safety events were stratified by ‘gut-specific’ (vedolizumab) versus ‘systemic’ (anti-TNF or ustekinumab) biologic therapies. The impact of continuing corticosteroid therapy as part of the anti-rejection regimen following biologic initiation was also evaluated.
Results: Thirty-six patients who required biologic therapy for the management for IBD following LT were identified. These patients were exposed to 59 biologic episodes, with sixteen patients sequentially exposed to more than one biologic therapy. Primary sclerosing cholangitis (88.9%) was the most frequent underlying liver condition and ulcerative colitis (72.2%) was the most common IBD subtype requiring biologic therapy. Vedolizumab was the most frequently prescribed biologic (n=27) followed by anti-TNF (n=22) and ustekinumab (n=10). The median duration of each biologic episode was 12 months (IQR 6-27). The cohort were collectively exposed to 44.5 patient years of vedolizumab, 30.3 patient-years of anti-TNF), and 14.1 patient-years of ustekinumab. Twenty-seven (45%) biologic episodes were associated with 35 safety events a median of 8 months (IQR 4.5-13.5) following biologic initiation. Safety events associated with ‘gut-specific’ vs ‘systemic’ biologic therapies were comparable (15 v 20, p=0.61), with no differences between mild, moderate, and severe events (Table 1). The incidence rates of safety events with ustekinumab (0.43 per patient-year) and vedolizumab (0.43 per patient-year) were numerically lower compared to anti-TNF therapy (0.53 per patient-year) (p=0.34 and p=0.21 respectively). Corticosteroid exposure was associated with more frequent safety events (incidence ratio 2.05 [95% CI 1.13-3.73, P=0.018]) across the entire cohort irrespective of biologic.
Conclusion: This dual-centre study is one of the largest internationally to examine the safety outcomes LT patients exposed to biologic therapies for IBD. Safety events were reassuringly comparable between LT recipients who received ‘gut specific’ and ‘systemic’ biologic therapy, with most events being mild to moderate in severity. Similar to non-transplant settings, corticosteroid exposure was associated with a higher incidence of safety events, reiterating the need to minimise exposure within this high-risk population. In view of comparable safety outcomes following exposure to ‘gut-specific’ and ‘systemic’ biologic therapies, choice of biologic therapy to manage IBD following LT should not be directly influenced by transplant status. Larger studies are awaited to confirm these findings.
84
The effect of solid food diet therapies on the induction and remission of Crohn’s disease: A systematic review
Jennifer Zhang1, Nikil Vootukuru1 and Ola Niewiadomski1,2
1Department of Gastroenterology, Eastern Health, Melbourne, Australia;2Monash University, Melbourne, Australia
Background and Aim: The efficacy of highly restrictive dietary therapies such as exclusive enteral nutrition (EEN) in the induction of remission in Crohn’s disease (CD) is well established, however, ongoing issues exist with its poor palatability, restrictions, and adherence. The aim of this review is to evaluate the current evidence for the efficacy of solid food diets exclusively, on the induction and maintenance of clinical and biochemical remission in CD. Secondary aims include impact on endoscopic healing and quality of life.
Methods: A systematic review including randomised controlled trials (RCTs), open-label randomised trials and head-to-head clinical trials was conducted. Adult and paediatric patients with clinically active and inactive disease were included. Two authors independently performed critical appraisals of studies, including study selection and risk of bias assessments.
Results: 14 studies were included for review, with several studies suggesting clinically significant findings. Clinical remission was achieved in a paediatric population undertaking the Mediterranean diet (MD) (moderate risk of bias). In adults, the Crohn’s disease exclusion diet (CDED) was comparable to the CDED with partial enteral nutrition (PEN) diet in induction of remission (moderate risk of bias). A low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet was also shown to decrease symptoms in patients with quiescent or mildly active CD (high risk of bias), however, this was not corroborated by other FODMAP diet studies.
Conclusion: There are promising outcomes for the MD and CDED in inducing remission in mild to moderate CD. The current evidence for solid food dietary therapy in CD is limited by the quality of studies and relatively high bias. Future well designed studies are needed to confirm the efficacy.
87
Hello, is it amoeba you are looking for?
Shauna Madigan1, Vanessa Chong2, Joseph Fantasia2 and Dharshan Sathananthan2
1Flinders Medical Centre;2Lyell McEwin Hospital
Introduction: Chronic colonic ulceration and inflammation can result from various causes, typically either infective or inflammatory. Often in the Australian setting this is presumed to be inflammatory bowel disease (IBD). This case demonstrates the importance of considering infective causes of colonic ulceration and mimics of IBD.
Case report: A 65y.o female presents to the emergency department with a month history of worsening abdominal pain and bloody diarrhoea. She had a history of colonic Crohn’s disease diagnosed a year prior. On presentation she met criteria for acute severe colitis and was started on intravenous corticosteroids. Her flexible sigmoidoscopy showed well demarcated, deep punched out ulcers with normal intervening mucosa, atypical for Crohn’s disease (image below). Histology showed active mucosal inflammation without inclusion bodies, architectural distortion, or granuloma. On day three of intravenous steroids, she was not making meaningful clinical improvement. Her stool sample returned positive for amoeba histolytica. Review of her initial colonoscopy one year prior showed cecal ulceration with histology showing the presence of amoebic trophozoites. Entamoeba histolytica is the fourth leading cause if parasitic death, with the common manifestation being intestinal amebiasis [1]. The prevalence in Australia is difficult to determine as it is not a notifiable disease however it has been reported in Northern Territory and return travellers [2]. Risk factors for entamoeba include contaminated food/water intake, or sexual transmission through faecal or oral contact. Our patient did not have any of these risk factors. There has been reported cases of amebiasis in QLD [3] and Sydney [4] without traditional risk factors. Intestinal amebiasis can mimic Crohn’s disease and disease course is thought to be worsened by the administration of systemic corticosteroids [5]. Our patient was treated for 7 days of high dose IV metronidazole, followed by oral paromomycin and well as steroids ongoing due to concern about dual pathology. Despite this treatment as well as intravenous infliximab she developed fulminant colitis, and she went on to have a total colectomy.
Conclusion: This case highlights the importance of considering alternative differentials for atypical colonic ulcers in patients with IBD. It also shows that amoeba histolytic can occur despite the traditional risk factors and should be considered in patients with colonic ulceration, abdominal pain, and bloody diarrhea. It re-enforces the value of an infective screen in patients being worked up for inflammatory bowel disease.
References
1. Carrero, J.C., et al., Intestinal amoebiasis: 160 years of its first detection and still remains as a health problem in developing countries. International Journal of Medical Microbiology, 2020. 310(1): p. 151358.
2. Hal, S.J., et al., Amoebiasis: current status in Australia. Medical Journal of Australia, 2007. 186(8): p. 412-416.
3. Smith, S., et al., Case Report: Endemic Amebiasis in Australia: Implications for Residents, Travelers, and Clinicians. Am J Trop Med Hyg, 2017. 97(1): p. 245-247.
4. Domazetovska, A., et al., A 12-Year Retrospective Study of Invasive Amoebiasis in Western Sydney: Evidence of Local Acquisition. Trop Med Infect Dis, 2018. 3(3).
5. Shirley, D.A. and S. Moonah, Fulminant Amebic Colitis after Corticosteroid Therapy: A Systematic Review. PLoS Negl Trop Dis, 2016. 10(7): p. e0004879.
97
Striking a balance: Patient-centric blood test monitoring guidelines for inflammatory bowel disease
Abhimati Ravikulan and James Irwin
Midcentral Dhb, Palmerston North, New Zealand
Background and Aim: Inflammatory bowel disease (IBD) therapies can cause myelosuppression and hepatitis. European Crohn's and Colitis Organisation (ECCO) recommends 3-monthly blood test monitoring, however patient adherence varies. This study aims to determine appropriate blood test monitoring frequency based on medication-related complications in IBD patients.
Methods: A retrospective analysis was conducted on the Manawatū IBD incidence cohort1 between 01/01/2011 – 31/12/2022. All medication use (5 amino-salicylic acid (5ASA), thiopurine (6-mercaptopurine, azathioprine), biologic (adalimumab, infliximab), methotrexate) and all blood testing was recorded. Hepatitis was defined as ALT >2x upper limit of normal, and myelosuppression as neutrophil count <1.0x10^9/L. Patients were observed from diagnosis until first abnormal blood test, or last follow-up. Testing duration required to identify a single hepatitis or myelosuppression event was calculated. Cox regression analysed correlation between medication use and hepatitis occurrence.
Results: Among 204 incident cases, 12 were excluded due to pre-diagnosis hepatitis or myelosuppression, leaving 192 patients. There were two myelosuppression events, and 25 hepatitis events. Testing duration for each hepatitis event is shown in Table 1. 6-mercaptopurine (Odds Ratio 39.2, p<0.001) azathioprine (OR 6.25, p=0.002), methotrexate (OR 9.94, p=0.004) and low mean cell volume (OR 0.89, p=0.001) were independently associated with hepatitis occurrence.
Conclusion: IBD treatment associated hepatitis or myelosuppression is associated with thiopurine and methotrexate use and is infrequent. Testing duration required to identify a single hepatitis event is long, particularly after medication initiation is complete. We propose, after a 6-month medication initiation period, that 6-monthly blood test monitoring is safe, and is more acceptable to patients.
Reference
1. Morton, H, Coad, J, Pedley, KC, Irwin, JR. Incidence of Inflammatory Bowel Disease in New Zealand Remains High, Findings in the Manawatū Region. Dig Dis Sci.2023 Nov; 68(11): 4230–4242. doi: https://doi.org/10.1007/s10620-023-08070-5.
101
Adalimumab originator and biosimilars in global inflammatory bowel disease treatment
Tsz Hong Yiu1, Hiroshi Nakase2, Wai Keung Leung3, Huiyu Lin4, Rupa Banerjee5, Emilia Anderson6 and Rupert Leong6
1Western Health, Melbourne, Australia;2Sapporo Medical University, Sapporo, Japan;3University of Hong Kong, Pok Fu Lam, Hong Kong SAR;4Tan Tock Seng Hospital, Singapore, Singapore;5Asian Institute of Gastroenterology and AIG Hospitals, Gachibowli, India;6Concord Repatriation General Hospital, Sydney, Australia
Background and Aim: Adalimumab has experienced a significant rise in biosimilars availability following the expiration of the patent for its originator, Humira. We conducted a global review encompassing both the originator and biosimilars of adalimumab, focusing on differences in formulations and the variety of product support systems available in different countries. The aim is to provide guidance for selecting the most appropriate product.
Methods: We collected global data on adalimumab biosimilars from medication registries such as the U.S. Food and Drug Administration in the USA and the Therapeutic Goods Administration in Australia. Product details were obtained from product information documents, with additional inquiries to manufacturers for any missing information. International authors conducted structured interviews with local pharmaceutical companies in Australia, Hong Kong SAR, India, Japan, and Singapore to gather information on the support systems available for patients, prescribers, and pharmacists regarding these products.
Results: We identified 29 Adalimumab products worldwide and gathered information for Humira and 13 biosimilars (Table 1). Humira, Xelenka, Ardalicip and Yuflyma offer high-concentration citrate-free formulations, effectively minimizing injection discomfort. Humira and Xelenka provide a wide range of dosages, including 80mg and 20mg formulations for inflammatory bowel disease induction therapy and paediatric patient management, respectively. Xelenka, Yuflyma, and Ardalicip have the longest room temperature shelf life of up to 30 days, making them suitable for frequent travellers. The level of product support services varies between countries and products. Products marketed in Australia, namely Humira, Yuflyma, Idacio, Hyrimoz, Hadlima, Abrilada, and Amgevita, as well as Exemptia in India, provide the most extensive support. Support services include patient hotlines, online portals with educational videos, and injection/script reminders for patients, along with online portals and demonstration devices for prescribers and pharmacists.
Conclusion: Adalimumab products exhibit variations in formulations and associated support programs across different countries. Among the four products offering high-concentration citrate-free formulations, Humira and Xelenka offer a wide range of dosages for different indications. Meanwhile, Xelenka, Yuflyma, and Ardalicip provide the longest room temperature shelf lives, which is favourable for travellers. Most Australian products and Exemptia in India offer comprehensive support for patients, prescribers, and pharmacists. This study enables clinicians to choose the most suitable option tailored to the specific needs of each patient and prescriber.
113
Safety, tolerance and acceptance of the recombinant zoster vaccine (Shingrix®) for patients with inflammatory bowel disease (IBD) on advanced therapies: Results from a tertiary IBD centre vaccine rollout program
Justin Baker, Oliver Post, Reeham Abu-Rgeef, Sherman Picardo and Kannan Venugopal
Royal Perth Hospital, Perth, Australia
Background and Aim: Patients with inflammatory bowel disease (IBD) on advanced medical therapies have more than a 3-fold risk of varicella zoster (Shingles) infection. The PBAC has recently recommended varicella zoster virus recombinant vaccine Shingrix® for those aged 18-64 at moderate to severe risk of infection. Shingrix® has been available on Western Australia’s State Medicines Formulary since November 2022 and is listed for use as per the Australian Immunisation Handbook. The aim was to evaluate vaccine acceptance and characterise short term tolerance and safety in an IBD population on advanced therapies.
Methods: All IBD patients commencing an advanced therapy (monoclonal antibody therapy, Janus Kinase (JAK) inhibitor, Sphingosine-1-phosphate inhibitor or an immunomodulator) were offered two doses of Shingrix® vaccine. All patients were counseled by an IBD pharmacist, prior to vaccine administration. A telephone survey of patients who received both vaccinations between November 2022 and April 2024, was conducted at least four weeks after their second dose, to capture data related to vaccine adverse events. Medical records were reviewed for baseline characteristics and immediate infusion reactions.
Results: Seventy-eight patients were offered Shingrix®, of which 4 (5.1%) declined (3 due to wishing to minimize medical therapies and 1 due to concerns over previous adverse event to pneumococcal vaccination). Seventy-four patients received both doses of the vaccine, of which 58 completed the follow-up survey (response rate 78%). Median age was 43 years (IQR 33-52). 32 patients (55.2%) had ulcerative colitis and 26 (44.8%) had Crohn’s disease. The majority were receiving a JAK inhibitor (56.9%), followed by TNFa antagonist (12.1%), TNFa antagonist/Thiopurine (10.3%), IL-12/23 inhibitor (5.2%), Thiopurine (3.4%) and Sphingosine-1-phosphate inhibitor (3.4%). Most respondents did not report any adverse events to the first (58.6%) or second (60%) dose. Injection site reactions were most common to the first and second doses (25.9% and 13.8% respectively). This was followed by fatigue (15.5%;10.3%), fever (10.3%;8.6%), headache (6.9%;6.9%), myalgia (3.4%; 1.7%) and GI symptoms (1.7%; 3.4%), Figure 1. Varicella IgG serology was positive for 93% of patients, with 82% and 48% acquiring chickenpox and shingles infections more than 3 months prior to vaccination. The median interval between first and second Shingrix® doses was 42 days (IQR 42-51). There were no reported episodes of anaphylaxis, flares in IBD activity or subsequent varicella zoster infections following Shingrix® administration.
Conclusion: Shingrix® vaccination was well tolerated with high acceptance and minimal adverse events in an IBD population on advanced therapies.
115
Evaluation of the artificial intelligence system CAD-EYE to optically characterise lesions in inflammatory bowel disease surveillance
1Royal Perth Hospital, Perth, Australia;2Curtin University, Bentley, Australia
Background and Aim: Patients with inflammatory bowel disease (IBD) have an increased risk of colorectal dysplasia and cancer. Endoscopic surveillance is recommended but is challenging due to the presence of active inflammation, flat dysplasia and inflammatory pseudopolyposis. CAD-EYE, an artificial intelligence powered endoscopic module by Fujifilm, optically characterises lesions in real time. We evaluated the accuracy of CAD-EYE in IBD surveillance.
Methods: Consecutive IBD patients undergoing surveillance at a single centre between January and December 2023 were included. Surveillance was performed with image enhanced endoscopy (withdrawal with Linked Colour Imaging and CAD-EYE). Non-magnified, still images of any lesions identified during the procedure were captured in real time followed by blue light image characterisation by CAD-EYE as neoplastic (malignant potential) or hyperplastic (non-malignant potential) prior to resection. If the operator identified a lesion considered an inflammatory pseudopolyp, image capture and characterisation was performed but the lesion was not resected, as per current clinical practice. Two independent expert IBD clinicians reviewed all still images and characterised the lesions. A maximum of five non resected inflammatory pseudopolyps per patient were included, if verified as such by the expert reviewers. The accuracy of CAD-EYE was assessed for all lesions (composite of histology for resected lesions and expert verified non-resected pseudopolyps). For the resected lesions, accuracy of CAD-EYE was compared to expert characterisation.
Results: Thirty-eight patients, 50% male with a median age of 52 years were included. The median procedure time was 27 minutes (IQR 21-36) with a median withdrawal time of 19 minutes (IQR 15-28). A total of 97 lesions were identified, of which 43 were resected (11 adenomas, 4 sessile serrated lesions, 22 hyperplastic polyps, 2 lymphoid tissue and 4 inflammatory pseudopolyps). The remaining 54 lesions were non-resected inflammatory pseudopolyps. CAD-EYE correctly characterised 92/97 lesions (94.8%) with a sensitivity 80.0% and specificity 97.6% for neoplastic lesions. For resected lesions CAD-EYE (accuracy 93.0%, sensitivity 80.0%, specificity 100%) was superior to expert characterisation (accuracy 88.0%, sensitivity 77.0%, specificity 100%) for neoplastic lesions.
Conclusion: CAD-EYE demonstrated excellent accuracy in characterisation of lesions in IBD surveillance including inflammatory pseudopolyps. It was superior to expert characterisation for resected lesions.
120
Determining the optimal radiologic disease activity scoring on magnetic resonance imaging for clinical healing of Crohn’s perianal fistulas: Analysis of a prospective imaging series
Michael De Gregorio1,2, Leon S Winata1, Corina C Behrenbruch1,2, Imogen Hartley1,2, Susan J Connor3,4, Basil D'Souza2,5, Michael J Johnston1, Michael Kamm1,2, James O Keck1, Jordi Rimola6, Tom Sutherland1,2, Rodney J Woods1, Emily K Wright1,2, William R Connell1, Alexander Thompson1,2 and John Nik Ding1,2
1St Vincent's Hospital Melbourne, Australia;2University of Melbourne, Australia;3Liverpool Hospital Sydney, Australia;4UNSW Sydney, South West Sydney Clinical Campuses, Australia;5Northern Hospital, Australia;6Hospital Clínic Barcelona, Spain
Background and Aim: Magnetic resonance imaging (MRI) is the gold-standard for evaluating disease activity and treatment response for Crohn’s perianal fistulas. Multiple indices to grade radiologic disease activity severity exist, however there is no consensus regarding which index correlates most accurately with clinical findings. We explored the relationship between established radiologic scoring indices and clinical healing and their role in assessing and predicting treatment response.
Methods: An analysis of 135 MRI from 60 patients with Crohn’s perianal fistulas enrolled in a prospective, real-world observational study was performed. The prospective study followed patients for a minimum of 12 months post commencement of a multidisciplinary care model, incorporating early and intensive optimisation of medical and surgical therapies, which included serial pelvic MRI. Each MRI had a paired physical examination, providing concurrent clinical healing outcomes; with clinical healing defined as the absence of draining perianal fistula external openings despite gentle finger compression. Radiologic disease activity severity was graded using the Van Assche Index (VAI), Magnetic Resonance Index for Assessing Fistulas in Patients with Crohn’s Disease (MAGNIFI-CD), and Fibrosis Score (FS) indices. The primary analysis evaluated the relationship between radiologic indices and concurrent clinical healing. Secondary analyses evaluated: [1] optimal index scores associated with concurrent clinical healing; [2] association between individual scoring criteria and concurrent clinical healing; [3] association between changes in index scores over serial imaging and achieving clinical healing at 12 months in those with clinically active disease; [4] the ability of baseline individual scoring criteria to predict clinical healing at 12 months in those with clinically active disease; and [5] optimal changes in index scores over serial imaging associated with achieving clinical healing at 12 months in those with clinically active disease. Relationships were assessed using logistic regression analyses and optimal indices using area under the receiver operating characteristic (AUROC) curves.
Results: All 60 patients had a baseline MRI, with 53 (88 %) and 22 patients (37 %) having serial MRI at 1 and 2 years, respectively. Intravenous contrast was used in 126 MRI (93 %), needed for scoring MAGNIFI-CD. Concurrent clinical healing significantly correlated with lower VAI (OR 0.70, 95%CI 0.59-0.83, P < 0.001) and MAGNIFI-CD (OR 0.76, 95%CI 0.65-0.88, P < 0.001) and higher FS (OR 3.14, 95%CI 1.94-5.08, P < 0.001). On ROC curve analysis, VAI, MAGNIFI-CD, and FS all exhibited similarly high AUROC for concurrent clinical healing, with AUROC of 0.91, 0.84, and 0.92, respectively. The optimal VAI, MAGNIFI-CD, and FS scores associated with concurrent clinical healing were ≤ 6 (sensitivity 82.8 %, specificity 93.5 %), ≤ 8 (sensitivity 77.8 %, specificity 73.1 %), and ≥ 5 (sensitivity 82.8 %, specificity 93.5 %), respectively. On multivariable analysis, only the degree of fibrosis on FS (OR 2.07, 95%CI 1.43-2.98, P < 0.001) and radiologic fistula tract extension on VAI (OR 0.22, 95%CI 0.08-0.60, P = 0.003) were independent positive and negative indicators of concurrent clinical healing, respectively. Of the 31 patients with clinically active disease at baseline, there were only weak associations between changes in index scores over serial imaging and achieving clinical healing at 12 months. No baseline individual scoring criteria predicted clinical healing at 12 months. The optimal changes in VAI, MAGNIFI-CD, and FS scores associated with achieving clinical healing at 12 months were a decrease of ≥ 4 (sensitivity 66.7 %, specificity 75.0 %), a decrease of ≥ 2 (sensitivity 70.0 %, specificity 69.2 %), and an increase of ≥ 1 (sensitivity 58.3 %, specificity 56.3 %), respectively.
Conclusion: Radiologic disease activity severity using VAI, MAGNIFI-CD, and FS indices have equally strong associations with concurrent clinical healing. In patients with clinically active disease, changes in indices over serial imaging post treatment did not demonstrate a strong association with achieving clinical healing. No baseline individual scoring criteria were predictive of achieving clinical healing at 12 months, with further studies needed to determine the predictive utility of individual radiologic parameters.
122
A novel and rapid faecal myeloperoxidase assay predicts endoscopic findings in patients with IBD
Belal Chami1,2, Mark Ghali1,2, Paul Witting1,2, Crispin Corte1,2, Nikola Mitrev1,2 and Viraj Kariyawasam1,2
1University of Sydney, Sydney, Australia;2Western Sydney Local Health District, Sydney, Australia
Background: Neutrophils are one of the primary infiltrative immune cell types in IBD, with neutrophil migration into the gut wall being proportional to disease severity. Myeloperoxidase (MPO) is a heme-containing peroxidase most abundantly expressed in neutrophils. Upon degranulation MPO oxidants elicit their microbiocidal effects. During chronic inflammation, MPO oxidants (chiefly HOCl) damage host tissue and may perpetuate inflammation. We previously showed that levels of intestinal MPO are correlated to UC and CD disease severity. Recently, we developed a novel and rapid method (~5 min) to detect faecal MPO activity, coined the MPO Luminol reaction (MPOLR), which catalysis the reactions of luminol in the presence of MPO-produced HOCl, via the MPO halogenation cycle.
Aim: To validate MPOLR in faecal samples and compare with established biomarkers, endoscopic and patient disease severity indices of IBD, in patients with active/inactive IBD and control patients.
Method: We recruited n=60 patients, aged 18-55 years, into 4 groups: Crohn’s disease (CD), ulcerative colitis (UC), healthy relatives of IBD patients and random colonoscopy controls with no prior or subsequent IBD diagnosis. Disease states were defined using colonoscopy, scored via UCEIS (ulcerative colitis endoscopic index of severity) and the SES-CD (Simple Endoscopic Score for CD). Faecal MPO, calprotectin and lactoferrin levels were quantified via traditional ELISA-based approaches while MPO activity was determined via MPOLR. Spearman’s correlation was employed to evaluate endoscopic SES-CD/UCEIS and Indexed Disease Severity (IDS) correlations to evaluated biomarkers. Confounders such as age, gender and drug therapy were accounted for using logistic regression.
Results: Faecal MPOLR activity was significantly correlated to endoscopic & IDS indices (Spearman r = 0.642, p = 0.009 & Spearman r = 0.616, p = 0.016), in contrast to faecal calprotectin (Spearman r = 0.46, p = 0.0858 & Spearman r = 0.19, p = 0.215). Interestingly, faecal MPOLR and calprotectin levels did not reveal a significant correlation, suggesting MPOLR is a unique biomarker of IBD (Spearman r = 0.238, p = 0.2426). Similar trends were observed in CD and UC subpopulations of IBD, however further studies are required to validate these observations.
Conclusion: These promising results suggests MPOLR is an alternative marker of disease severity to calprotectin with several advantages based on its simplicity and rapid method of detection.
128
Real world data on efficacy and safety of upadacitinib in Crohn’s disease and ulcerative colitis in a multi-centre setting
Joseph Fantasia, Vanessa Chong and Arvind Rajagopalan
Lyell McEwin Hospital, Elizabeth Vale, Australia
Background: Upadacitinib is a selective and reversible JAK-1 inhibitor with proven efficacy at inducing and maintaining remission in Crohn’s Disease (CD) and Ulcerative Colitis (UC). It has been accessible via the Pharmaceutical Benefits Scheme for moderate-severe UC and CD since 2022 and 2023 respectively.
Aim: To review treatment outcomes and safety profile of patients who have received Upadacitinib for treatment of CD and UC.
Methods: Multi-center, retrospective review of all patients who were commenced on Upadacitinib for treatment of CD and UC between Jan 2023 and March 2024. Patients were required to have had a minimum of 3 months of treatment. Demographic and disease related information was obtained from their medical record.
Results
Conclusion: Participants in this study were high risk and complex. A significant percentage achieved clinical remission or demonstrated clinical response after commencing therapy. Mean duration to response and/or remission of 3-6 months. The rate of side effects was low and only one participant required surgical intervention. In the setting of complex/difficult to treat patients, Upadacitinib appears a safe and effective biological agent for the management of both Ulcerative Colitis and Crohn’s Disease. Ongoing follow up is required to review the long-term effects.
129
Accuracy of intestinal ultrasound in assessing proximal constipation in ulcerative colitis: interim results from the SEE UCAC study
Ryan M Mathias1, Alice S Day1,2, Simon JB Prowse5, Suzanne Edwards4, Ramon Pathi6, Thomas Goodsall3,7 and Robert Bryant1,2,3
1Inflammatory Bowel Disease Service, The Queen Elizabeth Hospital, Adelaide, Australia;2Inflammatory Bowel Disease Research Group, The Basil Hetzel Institute for Translational Health Research, Adelaide, Australia;3School of Medicine, The University of Adelaide, Adelaide, Australia;4School of Public Health, The University of Adelaide, Adelaide, Australia;5Northern Adelaide Local Health Network, Adelaide, Australia;6Southern Adelaide Local Health Network, Adelaide, Australia;7Department of Gastroenterology, John Hunter Hospital, Newcastle, Australia
Background: Assessment of inflammatory bowel disease (IBD) with intestinal ultrasound (IUS) is well established but accuracy and reliability in assessing colonic contents and constipation is poorly defined despite the potential clinical utility. Ulcerative colitis (UC) associated proximal constipation (UCAC) is a frequent cause of symptoms in distal UC, potentially leading to unnecessary investigations or escalation of therapy. We aimed to determine the accuracy of IUS in the assessment of UCAC against computed tomography (CT) as the gold standard.
Methods: This prospective, single centre study included IUS performed for disease activity assessment of UC as a part of standard of care. When constipation was suspected using IUS (presence of posterior acoustic shadowing (PAS) and/or colonic diameter > 50mm), patients underwent same day low-dose CT (LDCT). Constipation on CT was defined as a modified Leech score ≥ 2, a score that defines the presence of stool and distension of the colon on x-ray, and modified for dual use in this study. IUS and CT parameters were read by a blinded second sonographer and two independent radiologists respectively. Agreement between IUS diameters and CT was via Bland-Altman plots and linear and logistic regression analysis. Correlation between categorical variables was assessed using Chi squared and McNemar’s test. Reliability was quantified using intraclass correlation coefficients (ICCs).
Results: 43 patients who underwent IUS and LDCT (median age 48.4, female 54%, E2 48%) were included in this preliminary analysis. Linear regression showed substantial correlation between colonic diameter measured on IUS and LDCT (r=0.70, p<0.001), as well as modified Leech score (r=0.72, p<0.0001, Table 1). There was no statistically significant difference between constipation diagnosed by IUS vs CT (p=0.99). There was moderate to substantial agreement between all ultrasound parameters when blind read by another sonographer (ICC 0.76-0.91), except for colonic gas which was fair (0.31).
Conclusion: Interim results support the accuracy of IUS compared with CT in assessing UCAC. Further evaluation of IUS parameters in assessing constipation is required, as well as assessment of responsiveness following cathartic therapy.
132
Measuring infliximab drug levels using spectroscopy
Saiumaeswar Yogakanthi1, Shekhar Kumta1,2, Sukhneet Shergill3, Mustafa Mohamedrashed1 and Mayur Garg1,2
1Northern Health, Epping, Australia;2University of Melbourne, Parkville, Australia;3Deakin University, Burwood, Australia
Background and Aim: Infliximab is an established agent for patients with inflammatory bowel disease. Although effective, infliximab is affected by variable pharmacokinetics, thereby requiring measurement of drug levels. At present, infliximab drug levels are measured using enzyme linked immunosorbent assays (ELISA). Fourier transform infrared spectroscopy (FTIR) is an established technique in analytical chemistry, in which, the interactions between light and the underlying molecular structure of analytes, yields information about their chemical composition. Given the prolonged turnaround times associated with ELISA, FTIR offers a possible point of care test for measuring infliximab drug levels. This study aimed to assess the feasibility of assessing infliximab drug levels in plasma using spectroscopic analysis.
Results: Analysis of the spectral signatures of infliximab and infliximab with plasma identified the spectral bands between 850 and 1750 as the region of interest. A regression model using the partial least squares regression technique was subsequently established using 10 latent variables. Autoscaling was used as pre-processing. Cross-validation was performed using the venetian blinds technique with 10 splits and a blind thickness of 1. The model’s root squared mean error of calibration, cross validation and prediction was 15.2ug/mL, 28ug/mL and 15.5ug/mL respectively, whilst the R2 of calibration, cross validation and prediction was 0.97, 0.91 and 0.98. These results suggest the model developed had a very high goodness of fit but a moderate degree of error with respect to its accuracy of infliximab level prediction.
Conclusion: In this study, we have demonstrated the ability to detect infliximab levels in plasma using spectroscopy. Whilst demonstrating a good fit, limitations at present include the mean error in prediction of 15ug/ml. These results provide the basis for further model refinement to improve predictive accuracy through additional spiked samples and testing on patient cohorts.
133
The epidemiology of hereditary pancreatitis patients in Australia and total pancreatectomy with islet autologous transplantation outcomes
Denghao Wu1,2, James Zuiani1,2, Chris Drogemuller1,2, Sunita De Sousa1,2, Richard Couper2,3 and Toby Coates1,2
1Royal Adelaide Hospital, Adelaide, Australia;2The University of Adelaide, Adelaide, Australia;3Women and Children's Hospital, Adelaide, Australia
Background and Aim: Hereditary Pancreatitis (HP) is a chronic disease caused by uncontrolled activation of trypsin in the pancreas. HP typically first presents as acute recurrent pancreatitis during infancy or early childhood and develops into chronic inflammation of the pancreas in adolescence, leading to lifelong debilitating pain, elevated risks of reduced endocrine function, diabetes, and pancreatic cancer. The condition is diagnosed by a genetic variant panel including PRSS1, SPINK1, CFTR, CTRC, CPA1, and CASR. Patients of HP are ideal candidates for total pancreatectomy with islet autologous transplantation (TPIAT). We aim to understand the effects of HP-associated genetic variants on disease risk and progression, investigate potential novel HP-associated variants and their pertinence in HP patients undergoing TPIAT.
Methods: HP patients were identified from existing hospital records. Interviews were administered to collect HP-associated data including pain management, medical prescriptions, interventions, smoking and alcohol history, and overall quality of life. Saliva samples were obtained for whole-exome-sequencing (WES). Genetic data were analysed using standard bioinformatics toolkits for variant discovery and correlation with HP phenotype. This was compared to a control sample of 2,504 patients with adult-onset chronic pancreatitis. Patients who has undergone TPIAT were longitudinally assessed at 3, 6 and repeating 12-month intervals post procedure.
Results: A total of 20 pedigrees comprising 122 HP patients were recruited for the project. The majority (57%) of the cohort were Indigenous Australians and 64% of patients reported ongoing moderate to severe pain. Bioinformatics analyses of WES genotypic data yielded a list of 33 potential novel pathogenic variants including ECE1, GJA5, and SPTBN5. 80% of patients undergone the TPIAT procedure achieved insulin independence within 6 months post-surgery with normalise C-Peptide levels. Further research on HP organoid production for research is also currently undergoing.
Conclusion: Our estimated prevalence of HP is higher than previously described and disproportionately affect Indigenous populations. The percentage of HP patients requiring lifelong analgesics is alarming. Crucially, novel genetic factors are important in predicting disease phenotypic onset and progression. Furthermore, TPIAT has been shown to be a successful treatment for patients of HP in Australia.
146
Effectiveness of exclusive enteral nutrition as an adjunct to corticosteroids in acute severe ulcerative colitis
Kate Vaughan1, Kylie Clavarino1, Desmond Patrick1,2 and Lauren White1,2
1Sunshine Coast University Hospital;2Griffith University
Background and Aim: The standard management of Acute Severe Ulcerative Colitis (ASUC) is early administration of intravenous corticosteroids (IVCS) and re-assessment on Day 3 via the Oxford criteria whether to initiate rescue therapy. Exclusive enteral nutrition (EEN), substituting a regular diet with a semi-elemental or polymeric formula, has well-supported literature in Crohn’s disease. The current literature in ASUC is conflicting1, 2. Our aim was to assess the effectiveness of EEN as an adjunctive therapy to IVCS in patients with ASUC.
Methods: All patients admitted with ASUC (meeting Truelove and Witt’s criteria) to a single tertiary centre teaching hospital between March 2022 and May 2023 were reviewed by a dietitian, educated and offered EEN or standard diet (SD). The results of those who accepted and completed 5 days of EEN were compared to those who chose SD. Patients were able to cease EEN at any stage and if did so were included in SD cohort. The primary outcome was the need for rescue therapy on Day 3. Secondary outcomes included need for colectomy at 12 weeks, tolerability of EEN and biochemical response. Furthermore, the need for rescue therapy with all-comers to EEN (any days completed) versus upfront SD was also compared to test the hypothesis that bowel frequency may increase due to a liquid diet leading to increased use of rescue therapy.
Results: 60 patients were included. 35 patients initiated EEN, 17 tolerated 5 days. Final EEN group n=17, SD n=43. There was no difference between the baseline UCEIS (EEN μ5.92, SD μ5.75), CRP (EEN μ47, SD μ57) or albumin (EEN μ31, SC μ43). 12/17 (71%) EEN patients required rescue therapy, compared to 33/43 (77%) in SD (p-value 0.619, x20.2462). 3/17 (18%) patients on EEN required a colectomy within 3 months compared to 7/43 (16%) SD patients (p-value 0.898, x20.016). 17/35 (48%) of patients tolerated 5 days of EEN. Reasons for cessation were poor tolerability (n=15), diarrhea (n=1), discharge (n=1), and unknown (n=1). There was no significant difference in the delta CRP from D1 to D5 (EEN μ34.3, SC μ43.5). There was no significant difference in the need for rescue therapy for allcomers to EEN (n=35), rescue therapy 26/35 (74%) compared with upfront SD (n=25), rescue therapy 18/25 (72%) (p-value 0.843, x2 0.039).
Conclusion: In the ASUC cohort there is no difference in the rates of rescue therapy at day 3, or colectomy within three months, in those exposed to EEN, completing 5 days of EEN or completing a SD. Half of those who start EEN cease due to poor tolerability.
References
1. Sahu P et al. 2021. Randomised clinical trial: exclusive enteral nutrition versus standard of care for acute severe ulcerative colitis. AP&T. doi: 10.1111/apt.16249.
2. Willmann L et al 2022. Effectiveness of polymeric exclusive enteral nutrition as an adjunct to standard of care in patients with acute severe ulcerative colitis. Gastroenterology. https://www.gastrojournal.org/article/S0016-5085(23)03019-6/pdf
149
Effectiveness of the adjuvanted recombinant zoster vaccine in preventing herpes zoster among patients ≥50 years of age with inflammatory bowel disease in the United States: a retrospective real-world database analysis from 2018 to 2021
1GSK, Value of Evidence Organization (VEO), Vaccine Epidemiology, Viral Non-Respiratory, Rockville, United States;2GSKDepartment of Real-World Analytics, Wavre, Belgium;3GSKVaccines Clinical Statistics, Amsterdam, The Netherlands;4Real World Data Management & Programming, GSK, Bengaluru, India;5Vaccines R&D, Clinical Sciences, GSK, Rockville, United States;6GSK, Abbotsford, Australia
Background and Aim: Patients with inflammatory bowel disease (IBD) face higher risks of herpes zoster (HZ) compared to the general population. The US Food and Drug Administration approved recombinant zoster vaccine (RZV) for adults ≥50 years of age (YOA) in 2017 and for adults ≥18 YOA who are or will be at increased risk of HZ due to immunodeficiency or immunosuppression, as patients with IBD, in 2021. This study addresses an information gap for RZV vaccine effectiveness (VE) in preventing HZ among IBD patients ≥50 YOA.
Methods: This retrospective matched cohort study used the Optum Clinformatics Data Mart healthcare administrative claims database from Jan 2018─Dec 2021. Patients ≥50 YOA with IBD who received 2 RZV doses ≥28 days apart (RZV cohort) were 1:3 matched to their unvaccinated counterparts (non-RZV cohort) by age, medication category, and other confounders (propensity score). The RZV cohort was indexed on the second dose and non-RZV cohort was indexed on vaccinated counterparts’ index date. Follow-up started from index date +30 days until earliest date of HZ occurrence, end of enrolment, death, receipt of HZ vaccine, or study end. The first HZ episode during follow-up was identified using an algorithm incorporating ICD-10 diagnosis code, inpatient or outpatient claims and/or HZ antiviral medication used within 7 days pre/post-HZ diagnosis. HZ incidence rates (IRs) were calculated overall, stratified by condition (ulcerative colitis [UC], Crohn’s disease [CD]) and age. Cox hazards models estimated overall and stratified hazard ratios (HRs). VE (%) was calculated as (1−HR)x100.
Results: We identified 6501 RZV vaccinated and 19962 matched unvaccinated IBD patients who were included in the 2-dose analysis. The IR of HZ was 2.92/1000 person-years (PY) in the RZV cohort and 10.96/1000 PY in the non-RZV cohort, resulting in a VE of 73.4% (95% confidence intervals [CIs]: 60.8-82.0) for IBD patients (Figure). VE against HZ was 63.5% (95%CIs: 43.0-76.6) and 85.7% (95%CIs: 69.5-93.3) in UC and CD 2-dose cohorts. IRs and VE stratified by condition and age are presented in Figure.
Conclusion: Our analysis provides real-world evidence that RZV vaccination effectively prevents HZ in IBD patients ≥50 YOA, reducing the burden in this high-risk population. These findings align with the available literature on RZV effectiveness in patients with IBD, suggesting that this population could greatly benefit from RZV vaccination.
Originally published as: D. Constenla et al. P986 Effectiveness of the adjuvanted recombinant zoster vaccine (RZV) in preventing herpes zoster (HZ) among patients ≥50 years of age with Inflammatory Bowel Disease in the United States: A retrospective real-world database analysis from 2018 to 2021. Journal of Crohn's and Colitis 2024, Volume 18, Issue Supplement_1, Pg i1779. Reproduced by permission of Oxford University Press on behalf of European Crohn's and Colitis Organisation.
150
Beyond the scope: utility of intestinal ultrasound for predicting clinical outcomes in ulcerative colitis in clinical remission
Rose Vaughan, Jessie Zhou, Lei Chen, Nicholas Mingos, Jonathan Segal and Britt Christensen
Royal Melbourne Hospital, Melbourne, Australia
Background and Aim: Intestinal Ultrasound (IUS) is a point-of-care tool increasingly utilised in the management of ulcerative colitis (UC) as a marker of disease activity and response to therapy. IUS has the advantage of being non-invasive, non-irradiating, well tolerated, cost-effective with good reproducibility when compared to ileo-colonoscopy and magnetic resonance enterography. There is however limited evidence that sonographic remission on IUS predicts UC disease course.
Methods: This study examined the relationship between IUS and clinical outcomes for UC patients in steroid-free clinical remission, specifically if presence of sonographic inflammation was associated with medication escalation, corticosteroid use, hospitalisation or surgery. A retrospective study at a metropolitan tertiary hospital included all UC patients who underwent IUS for IBD between 2017 and 2022 in clinical remission (Simple Colitis Clinical Activity score ≤2) at time of IUS and followed up for at 6 months. Patients with rectum-confined disease (E1), stoma, or suboptimal IUS were excluded. Sonographic healing, defined as BWT ≤3 mm without hyperaemia, inflammatory fat, or disrupted bowel wall stratification was the combined endpoint. Kaplan-Meier analysis was performed to compare medication-escalation-free survival, corticosteroid-free survival, hospitalisation-free survival and surgery-free survival in those with and without sonographic healing. Univariate and multivariate Cox proportional hazard regression analyses were performed to identify predictors of these clinical outcomes.
Results: 2,113 ultrasound reports were assessed for eligibility, with 394 patients having confirmed UC diagnosis. Of these, 149 consecutive patients in clinical remission met the inclusion criteria (43% male). Sonographic inflammation was present in 45%. During mean follow-up of 634 days, medication escalation occurred in 40%, corticosteroid use in 27%, hospitalisation in 13% and UC related surgery in 2%. Sonographic inflammation was not a predictive factor for these outcomes; the only significant predictor was the baseline Montreal classification (Table 1). Although sonographic hyperaemia was associated with worse combined outcomes, this did not reach statistical significance.
Conclusion: This study is the first to examine the predictive utility of IUS in the setting of clinical remission and interestingly demonstrates that IUS does not appear to predict clinical complications. The role of IUS in UC has been slower to be established compared to Crohn’s disease due to concerns about poor rectal views and lower sensitivity to detect mild mucosal inflammation. This study challenges utility of IUS in predicting outcomes for UC patients in clinical remission, highlighting the need for further research to establish its role in guiding real-time treatment decisions.
151
The real-world use of five aminosalicylate treatment for ulcerative colitis: Crohn's Colitis Cure (CCC) data insights program
Wai Kin Su1,2,3, William Wilson4,5, Joseph Pipicella1,3,6, Craig Haifer7, Astrid-Jane Williams2,6,8, Kate Lynch9,10, Angela Forbes11, Gareth Walker12,13,14, Michael Schultz15, Ian Lawrance16,17, Yoon-kyo An13,18, Laurel Brett19, Susan J Connor1,2,3,6 and Jane Andrews1,10,20
1Crohn's Colitis Cure, Liverpool, Australia;2Department of Gastroenterology and Hepatology, Liverpool Hospital, South Western Sydney Local Health District, Liverpool, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Institute for Applied Medical Research, Liverpool, Australia;4University of New South Wales, Medicine & Health (South Western Sydney Clinical School), Sydney, Australia;5St Vincent's Public Hospital Sydney, Sydney, Australia;6Lyell McEwen Hospital, Adelaide, Australia;7SA Health, Adelaide, Australia;8Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;9Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;10Central Adelaide Local Health Network, Adelaide, Australia;11Royal Brisbane and Women’s Hospital, Brisbane, Australia;12University of Queensland, Brisbane, Australia;13QIMR Berghofer, Brisbane, Australia;14Mater Research,Brisbane, Australia;15Department of Gastroenterology, Logan Hospital, Brisbane, Australia;16School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;17Centre for Inflammatory Bowel Diseases, Saint John of God Subiaco Hospital, Perth, Australia;18IBD centre of British Columbia, Vancouver, Canada;19Department of Medicine, University of Otago, Christchurch, New Zealand;20Department of Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand
Background: Five-aminosalicylates (5ASAs) promote and maintain remission in people with ulcerative colitis (UC). They are administered orally or rectally, with combination (oral and rectal) therapy more effective than oral monotherapy, especially when treating flares. 5ASAs may be perceived as outdated and thus neglected. With increasing UC incidence and prevalence globally, understanding real-world 5ASA use and value is vital.
Methods: Crohn’s Colitis Care (CCCare) is a cloud-based electronic medical record used in Australasia since 2018. Data feed into a de-identified clinical quality registry (CQR), which was interrogated in April 2024. All people with UC with a clinical assessment at any time point were included.
Results: Of the 3,515 eligible people, 79.8% resided in Australia and 20.2% in New Zealand (NZ). Their median age was 43 years (IQR 32 – 57), with an even gender distribution (51.1% female). Median disease duration was 9.5 years (IQR 4.8 – 17.3). Median duration of follow up within CCCare was 2.5 years (IQR 1.1 – 3.8). Treatment details are summarised in Table 1. Fewer people received rectal monotherapy in Australia than in NZ (4.6% vs 8.7%, p < 0.001), and females were more likely to receive rectal administration than males (34.6% vs 26.5%, p < 0.001). People with E1 and E2 disease were more likely to receive oral and rectal 5ASA (47.5% and 36.2% respectively) therapy than people with E3 disease (15.0%, p < 0.001). People with E3 phenotype were more likely to be on no 5ASA therapy than people with current E0/1/2 phenotypes (27.5% vs 19.4%, p < 0.001). In those who ceased 5ASA therapy, 1,140 (44.2%) had a reason documented, with the most common being medication rationalisation and/or deep remission (37.1%). Those on rectal monotherapy were more likely to self-initiate treatment cessation compared to other routes of 5ASA administration. A total of 927 (35.9%) of the people on 5ASAs (n= 2582) were recorded as already receiving additional IBD therapy at CQR entry (immunomodulators [IMs]/ biologics / small molecules). Of those receiving 5ASA alone at CQR entry (n=1655), 5ASAs were subsequently judged to have failed in 34.1% (n=564). 5ASA failure was defined as the need for additional IBD therapies (98.1%, n=349 for IMs/biologics/small molecules and n=204 for steroids); hospitalisation (n=7, 1.2%), or IBD surgery (n=3, 0.9%).
Conclusion: Despite being universally effective, the persistence of 5ASA therapy indicates they are well tolerated & perceived as beneficial by many consumers. More people in NZ received rectal monotherapy compared to Australia, and gender-specific trends in 5ASA administration, unrelated to disease phenotype, were identified, highlighting the potential need for cultural training to overcome what may be a ‘social gap’ to improve acceptance of this efficacious route of therapy when indicated.
153
Dose escalated therapy improving outcomes in inflammatory bowel disease: Crohn's Colitis Cure (CCC) data insights program
Wai Kin Su1,2,3, William Wilson4,5, Watson Ng2,6, Clair Whittaker7, Edward Giles8,9,10, Gareth Walker11,12,13, Angela Forbes14, Ian Lawrance15,16, Shoma Dutt17,18, Kate Lynch19,20, Laurel Brett21, Yoon-kyo An22,23, Susan J Connor1,2,3,6 and Jane Andrews1,20,24
1Crohn’s Colitis Cure, Sydney, Australia;2Department of Gastroenterology and Hepatology, Liverpool Hospital, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, Ingham Institute for Applied Medical Research, Sydney, Australia;4Lyell McEwin Hospital, Adelaide, Australia;5SA Health, Adelaide, Australia;6Medicine & Health (South Western Sydney Clinical School), University of New South Wales, Sydney, Australia;7St Vincent’s Public Hospital, Sydney, Australia;8Monash Children's Hospital, Clayton, Australia;9Department of Paediatrics, Monash University, Clayton, Australia;10Centre of Innate Immunity and Infectious Diseases, Hudson Institute of Medical Research, Melbourne, Australia;11University of Queensland, Brisbane, Australia;12QIMR Berghofer, Brisbane, Australia;13Royal Brisbane and Women's Hospital, Brisbane, Australia;14Department of Medicine, University of Otago, Christchurch, New Zealand;15Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Perth, Australia;16School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;17The Children’s Hospital at Westmead, Westmead, Australia;18Speciality of Child and Adolescent Health, Children's Hospital at Westmead Clinical School, Sydney School of Medicine, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;19Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;20Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;21Department of Gastroenterology, Logan Hospital, Logan, Australia;22Mater Hospital Brisbane, Brisbane, Australia;23Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia;24Central Adelaide Local Health Network, Adelaide, Australia
Background and Aim: Biologic therapies are effective medications in Inflammatory Bowel Disease (IBD), yet many people do not achieve an adequate or sustained response to standard dosing, thus requiring dose escalation (DE). We examined the need for DE and subsequent outcomes in a large real-world cohort.
Methods: Crohn’s Colitis Care (CCCare) is a cloud-based electronic medical record used in Australasia since 2018. Data feed into a de-identified clinical quality registry (CQR), which was interrogated in April 2024. People with IBD receiving adalimumab, infliximab, ustekinumab, or vedolizumab were included. DE was defined as maintenance dosing > 40 mg subcutaneous (SC) Q2 weekly for adalimumab, > 5 mg/kg intravenous (IV) Q8 weekly or >120 mg SC Q2 weekly for infliximab, > 300 mg IV Q8 weekly or > 108 mg SC Q2 weekly for vedolizumab, and > 90 mg SC Q8 weekly for ustekinumab. We examined data prior to and 12 months post DE.
Results: Of the 6,093 eligible people, 37.3% (n=2,272) were receiving DE therapy. Most of the cohort had Crohn’s disease (69.1%, n=4,208), whilst 29.0% (n=1,765) had ulcerative colitis, and 1.9% (n=115) had IBD-Unclassified. There was an even gender distribution (50.2% male), and the median age was 40 years (IQR 30 – 53). The median time to DE was 5 months (IQR 0 – 19), and 74.2% (n=1685) remained on DE therapy beyond 12 months. In those who required DE therapy, more people were currently smoking compared to those receiving standard dosing (11.3% vs 9.6%, p < 0.05). Rates of remission and healthcare utilisation (HCU) pre- and post-DE are presented in Table 1. There was a statistically significant increase in remission rates assessed by faecal calprotectin (< 250 μg/g) (28.1% increase, p < 0.001), patient-reported outcome (PRO2) (20.2% increase, p < 0.001), and endoscopic remission (5.4% increase, p < 0.001). Systemic steroid use reduced by 61% (p < 0.001). There was a reduction in HCU in the 12 months following DE. There was a reduction in the number of endoscopies performed (37% reduction, p < 0.001), radiology investigations (22.9% reduction, p < 0.001), and admissions (39% reduction, p = 0.91). People receiving DE therapy were seemingly more engaged with healthcare providers, with the number of helpline calls increased by 11.7% (p < 0.05). The number of clinical assessments was unchanged.
Conclusion: In a large real world Australasian cohort of people receiving biologic therapy, DE is associated with significantly improved rates of remission and reduction in HCU. As the cost of DE therapy is not government subsidised in Australia and New Zealand, people with IBD rely on compassionate access schemes of pharmaceutical companies, in turn delaying adequate disease control, thereby patient’s well-being and increasing the workload of healthcare providers due to the application and follow-up process. Further health economic analysis is required to further guide healthcare resource allocation.
154
Documented variation in inflammatory bowel disease care in Australasia : Crohn’s Colitis Cure (CCC) data insights program
Wai Kin Su1,2,3, Jack McNamara2, Joseph Pipicella1,3,4, William Wilson5,6, Simon Ghaly9,10, Aura Gesha Cabaero2, Gareth Walker11,12,13, Angela Forbes14, Heidi Su15, Laurel Brett21, Shoma Dutt18,19, Yoon-kyo An22,23, Ian Lawrance16,17, Kate Lynch8,20, Jane Andrews1,7,8 and Susan J Connor1,2,3,4
1Crohn’s Colitis Cure, Sydney, Australia;2Liverpool Hospital, Department of Gastroenterology and Hepatology, South Western Sydney Local Health District, Sydney, Australia;3The Ingham Institute for Applied Medical Research, Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, Sydney, Australia;4South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;5Lyell McEwin Hospital, Adelaide, Australia;6SA Health, Adelaide, Australia;7Central Adelaide Local Health Network, Adelaide, Australia;8Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;9St Vincent’s Public Hospital, Sydney, Australia;10St Vincent’s Clinical School, University of New South Wales, Sydney, Australia;11Royal Brisbane and Women's Hospital, Brisbane, Australia;12University of Queensland, Brisbane, Australia;13QIMR Berghofer, Brisbane, Australia;14Department of Medicine, University of Otago, Christchurch, New Zealand;15Department of Gastroenterology, Te Whatu Ora Health New Zealand Waitaha Canterbury, New Zealand;16Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Perth, Australia;17School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;18The Children’s Hospital at Westmead, Westmead, Australia;19Speciality of Child and Adolescent Health, Children's Hospital at Westmead Clinical School, Sydney School of Medicine, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;20Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;21Department of Gastroenterology, Logan Hospital, Logan, Australia;22Mater Hospital, Brisbane, Brisbane, Australia;23Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia
Background and Aim: Inflammatory bowel disease (IBD) is a global health issue with Australia and New Zealand having amongst the highest prevalence rates worldwide. Our study examined the quality, safety, and consistency of care amongst twelve Australasian centres over a 12-month period.
Methods: CCCare is a cloud-based IBD-specific electronic medical record (EMR) used in Australasia. Deidentified data prospectively entered by clinicians and consumers during routine clinical practice from April 2023 to April 2024 were retrospectively analysed. Only centres with over 100 people with IBD with an assessment during the last 14-month period were included.
Results: A total of 6,277 eligible people with IBD from 12 centres were included. Of those, 55.6% (n=3,488) had Crohn’s disease (CD), 41.9% (n=2,629) Ulcerative colitis (UC), and 2.5% (n=160) IBD-unclassified (IBDU). Their median age was 42 years (IQR 31 – 56) with an even gender distribution (50.1%, n=3,087, male). The number of people with IBD in CCCare in this study per centre ranged from 120 to 1,038 (median 527, IQR 248 – 687). In the total cohort, 52.6% (n=3,304) were currently on advanced IBD therapy (biologics or novel small molecules), with centre variation from 34.1% to 70.2% (p< 0.001). Of those on advanced therapy, 33% were on dose escalated therapy which also varied between centres from 17.1% to 64.2% (p < 0.001). Current steroid use ranged from 0.5% to 17.6% (median 12.1%, IQR 10.6 – 13.0, p<0.001). Ten centres documented IBD surgical rates. which varied from 0.1% to 7.5% (median 0.6%, IQR 0.2 – 2.8, p < 0.001). Ten centres documented IBD admission rates, which ranged from 0.4% to 4.2% (median 1.6%, IQR 0.7 – 2.4, p < 0.001). While the overall smoking rate across the cohort was 10.8%, the median smoking rate was 8.4%, which again varied significantly amongst sites (IQR 6.9 – 12.8, p < 0.001). Large variations were seen in documentation of healthcare maintenance items. Nine centres documented Influenza vaccination rates which varied from 0.7% to 52.1% (median 2.4%, IQR 1.9 – 18.6%, p < 0.001). Covid vaccinations documented at eleven centres varied from 0.2% to 86.9% (median 17.7%, IQR 5.8 – 49.4, p < 0.001). Seven centres documented skin care check completion rates, and these ranged from 0.5% to 30.2% (median 3.2%, IQR 1.4 – 9.1, p < 0.001). Eleven centres documented a total of 2,044 faecal calprotectin results (FCP) with an overall FCP remission rate (< 250 mg/g) of 74.9% varying from 58.9% to 100% (median 74.4%, IQR 70.4 – 81.4, p < 0.01). Over the 12 months, 1,624 lower endoscopies were performed with an observed remission rate of 55.6% varying from 6.7% to 100% between sites (median 55.2%, IQR 47.1 – 66.9, p < 0.001). Similarly, 616 radiological investigations were documented across ten sites with an observed remission rate of 19.2% to 55.6% (IQR 29.5 – 48.3, p = 0.05).
Conclusion: Despite much literature addressing care guidelines and targets, significant variation in care documentation and outcomes remains for people with IBD in Australasia. CCCare, as an IBD-specific EMR, supports scalable, continuous reporting of these measures. CCCare is thus ideally placed to develop into a national Clinical Quality Registry (CQR) to improve these deficiencies and reduce unwarranted care variation.
155
Exploring a novel score to assess the patient perceived burden of disease in Crohn’s disease and ulcerative colitis: Crohn’s Colitis Cure (CCC) data insights program
Wai Kin Su1,2,3, Bonita Gu2,4, Joseph Pipicella1,3,4, William Wilson5,6, Andrew Kim9,10, Gabrielle Wark2, Edward Giles11,12,13, Gareth Walker14,15,16, Angela Forbes17, Heidi Su18, Shoma Dutt21,22, Yoon-kyo An24,25, Ian Lawrance19,20, Kate Lynch8,23, Susan J Connor1,2,3,4 and Jane Andrews1,7,8
1Crohn’s Colitis Cure, Sydney, Australia;2Liverpool Hospital, Department of Gastroenterology and Hepatology, South Western Sydney Local Health District, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Institute for Applied Medical Research, Sydney, Australia;4South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;5Lyell McEwin Hospital, Adelaide, Australia;6SA Health, Adelaide, Australia;7Central Adelaide Local Health Network, Adelaide, Australia;8University of AdelaideFaculty of Health Sciences, Adelaide, Australia;9St Vincent’s Public Hospital, Sydney, Australia;10St Vincent’s Clinical School, University of New South Wales, Sydney, Australia;11Monash Children’s Hospital, Clayton, Australia;12Department of Paediatrics, Monash University, Clayton, Australia;13Centre of Innate Immunity and Infectious Diseases, Hudson Institute of Medical Research, Melbourne, Australia;14Royal Brisbane and Women's Hospital, Brisbane, Australia;15University of Queensland, Brisbane, Australia;16QIMR Berghofer, Brisbane, Australia;17Department of Medicine, University of Otago, New Zealand;18Department of Gastroenterology, Te Whatu Ora Health New Zealand Waitaha Canterbury, New Zealand;19Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Perth, Australia;20School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;21The Children’s Hospital at Westmead, Westmead, Australia;22Speciality of Child and Adolescent Health, Children's Hospital at Westmead Clinical School, Sydney School of Medicine, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;23Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;24Mater Hospital, Brisbane, Australia;25Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia
Background and Aim: The prevalence and burden of inflammatory bowel diseases (IBD) including Crohn’s disease (CD) and ulcerative colitis (UC) is rising globally. We propose here a novel score to capture and quantify the patient-perceived burden of disease (PPBoD) in IBD, in a large real-world Australasian cohort.
Methods: The Crohn’s Colitis Care (CCCare) de-identified Clinical Quality Registry was interrogated in April 2024. Adults with CD and UC across 19 IBD centres with an outpatient encounter in the last 14 months were included. A novel PPBoD score was designed for CD and UC. PPBoD for CD included patient reported components from the Harvey-Bradshaw Index (abdominal pain and patient-rated general wellbeing) as well as nocturnal bowel frequency, defecation urgency and stool frequency. PPBoD for UC included patient-reported components from the Mayo Score (stool frequency and rectal bleeding) as well as general wellbeing, urgency, and nocturnal bowel frequency. A PPBoD score required both defection urgency and patient rated general wellbeing to be documented. A total score of 0 was defined as no PPBoD, 1-2 as mild, 3-4 as moderate and ≥5 as significant. Possible relationships amongst PPBoD, demographics, disease and treatment factors were explored.
Results: A total of 6,211 people with IBD (57.2%, n=3551 CD and 42.8%, n=2660 UC) were identified with a clinical assessment in the last 14 months. Of whom, 69.4% (n=4,308) had sufficient data to calculate PPBoD. In this cohort, 82.5% had either no or only mild PPBoD (Table 1). The cohort was geographically dispersed across Australia (73.6%, n=3171) and New Zealand (26.4%, n=1137). People living in New Zealand had higher PPBoD. Females, active smokers and those who had used corticosteroids in the last 14 months reported a higher PPBoD. The utilisation of advanced therapies (biologic or novel small molecules) and aminosalicylates did not differ across PPBoD categories. In the subset of 1,530 (24.6%) with a recent faecal calprotectin, people with no PPBoD were more likely to have biochemical remission (faecal calprotectin < 100 mg/g). Data for endoscopic and radiological remission were available in 1391 (22.4%) people; those with no PPBoD were more likely to be in remission. In people with no PPBoD, 1.2% had any days out of role due to IBD, whereas those with higher PPBoD had more days out of role (Table 1).
Conclusion: We present a novel consumer-focused score to quantify PPBoD in IBD. Within this geographically dispersed cohort, the majority had either no or mild PPBoD. Smoking, steroid therapy and days out of role were all indicators associated with significant PPBoD. Further studies are required to validate this novel score to assess PPBoD in IBD.
156
Healthcare utilisation in people with inflammatory bowel disease: Crohn’s Colitis Cure (CCC) data insights program
Wai Kin Su1,2,3, Joseph Pipicella1,3,4, William Wilson5,6, Andrew Kim9,10, Chloe Davidson2, Edward Giles11,12,13, Gareth Walker14,15,16, Angela Forbes17, Heidi Su18, Ian Lawrance19,20, Shoma Dutt21,22, Kate Lynch8,23, Laurel Brett24, Jakob Begun25,26, Susan J Connor1,2,3,4 and Jane Andrews1,7,8
1Crohn’s Colitis Cure, Sydney, Australia;2Liverpool Hospital, Department of Gastroenterology and Hepatology, South Western Sydney Local Health District, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Institute for Applied Medical Research, Sydney, Australia;4South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;5Lyell McEwin Hospital, Adelaide, Australia;6SA Health, Adelaide, Australia;7Central Adelaide Local Health Network, Adelaide, Australia;8Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;9St Vincent’s Public Hospital, Sydney, Australia;10St Vincent’s Clinical School, University of New South Wales, Sydney, Australia;11Monash Children’s Hospital, Clayton, Australia;12Department of Paediatrics, Monash University, Clayton, Australia;13Centre of Innate Immunity and Infectious Diseases, Hudson Institute of Medical Research, Melbourne, Australia;14Royal Brisbane and Women's Hospital, Brisbane, Australia;15University of Queensland, Brisbane, Australia;16QIMR Berghofer, Brisbane, Australia;17Department of Medicine, University of Otago, New Zealand;18Department of Gastroenterology, Te Whatu Ora Health New Zealand Waitaha Canterbury, Christchurch, New Zealand;19Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Perth, Australia;20School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;21The Children’s Hospital at Westmead, Sydney, Australia;22Speciality of Child and Adolescent Health, Children's Hospital at Westmead Clinical School, Sydney School of Medicine, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;23Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;24Department of Gastroenterology, Logan Hospital, Logan, Australia;25Mater Hospital, Brisbane, Australia;26Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia
Background and Aim: Inflammatory bowel disease (IBD) is a lifelong illness, increasing in prevalence, with Australia and New Zealand amongst the highest in the world. Long-term management poses significant economic burden on people with IBD and the healthcare system. We aim to describe the healthcare utilisation (HCU) across 19 sites using Crohn’s Colitis Care (CCCare) as their IBD electronic management record (EMR).
Methods: CCCare is a cloud based EMR used in Australasia. Data are prospectively entered by clinicians and consumers during routine care and deidentified data flow through to the clinical quality registry (CQR). The CQR was interrogated in May 2024 to examine HCU over a 12-month period (April 2023 - April 2024). Only records of people with a clinical assessment during the last 14 months were included.
Results: There was 6,259 eligible people, with a median age of 41 years (IQR 31 – 56). There was an even gender distribution (50.2%, n=3145, male) and more than half had Crohn’s Disease (56.1%, n=3510), 41.4% ulcerative colitis (n=2591) and 2.5% IBD-Unclassified (n=158). Median disease duration was 10.7 years (IQR 5.1 – 18.8). Most resided in Australia (76.4%, n=4782) with 23.6% (n=1477) in New Zealand. The majority resided in a metropolitan area (77.7%, n=4085) with 11.3% in remote areas (n=593). Patient demographics are presented in Table 1. Ambulatory HCU is presented in Table 1. The consumer helpline accounted for 8,754 contacts: 1.4 per person. In-person clinic assessments was half of this activity (0.7 per person), with notably fewer endoscopic and radiology events. Kruskal-Wallis multivariate analysis revealed that age (p < 0.001 to < 0.01), medical centre (p < 0.001), region p < 0.001 to 0.012), country (p< 0.001), and duration of disease (p < 0.001) significantly affected most healthcare utilisation metrics, while gender (p = 0.07 to 0.41) was not a significant factor. Current advanced therapy (biologic or novel small molecule) significantly influenced helpline, radiology, and endoscopy utilisation (p < 0.001) but had no significant impact on clinical assessments (p = 0.45).
Conclusion: The long-term management of people with IBD requires the comprehensive input of expert multidisciplinary teams reflected in the number of in-person clinic visits and helpline contacts and supplemented by endoscopic and radiologic investigations. The utilisation of healthcare resources is demonstrated here, and further analysis will help identify unwarranted variation in care between IBD centres.
157
Inflammatory bowel disease nurse helpline contact trends in a large real-world Australasian cohort: Crohn’s Colitis Cure (CCC) data insights program
Wai Kin Su1,2,3, Patrick Chan4, Joseph Pipicella1,3,5, William Wilson6,7, Sally Antoniades10, Aura Gesha Cabaero2, Angela Forbes11, Kirsten Arnold12,13, Rachel Grafton8,14, Jane Andrews1,8,9 and Susan J Connor1,2,3,5
1Crohn’s Colitis Cure, Sydney, Australia;2Liverpool Hospital, Department of Gastroenterology and Hepatology, South Western Sydney Local Health District, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Institute for Applied Medical Research, Liverpool, Australia;4Department of Gastroenterology and Hepatology, Fiona Stanley Hospital, Murdoch, Australia;5South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;6Lyell McEwin Hospital, Adelaide, Australia;7SA Health, Adelaide, Australia;8Central Adelaide Local Health Network, Adelaide, Australia;9Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;10St Vincent’s Public Hospital Sydney, Sydney, Australia;11Department of Medicine, University of Otago, New Zealand;12Health New Zealand Te Whatu Ora Canterbury, New Zealand;13Co-chair IBD Nurses Group NZ, NZ Gastroenterology Nurses College committee member, Crohn’s Colitis NZ committee member, Wellington, New Zealand;14Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia
Background and Aim: Achieving optimal outcomes for people with Inflammatory Bowel Disease (IBD) requires lifelong engagement in care. Specialised-IBD-nurse-led helplines improve access to care and reduce healthcare costs. Despite this, IBD nurses and helplines receive variable funding, and little is known about their use across care sites. We therefore analysed real world IBD-helpline usage across 10 sites in Australasia.
Methods: Crohn’s Colitis Care (CCCare) is a cloud-based IBD-specific electronic medical record used in Australia and New Zealand. It includes a “Helpline” tab to enable specific helpline encounter documentation. De-identified data feed into an associated, clinical quality registry (CQR). Helpline-associated data prospectively entered during clinical practice from April 2023 to April 2024 were retrospectively analysed. Data from people with IBD with an assessment during the last 14-month period were included.
Results: In the eligible cohort (n=6,259), 56.1% (n=3,510) had Crohn’s Disease (CD), 41.4% (n=2,591) had Ulcerative colitis (UC) and 2.5% (n=158) had IBD-Unclassified (IBDU). Their median age was 41 years (IQR 31 – 56), with an even gender distribution (50.2%, n=3,145 male). The majority resided in Australia (76.4%, n=4782; 23.6%, n=1477 in New Zealand). A total of 8,754 helpline encounters were documented, 75.3% (n=6593) by email and 24.7%, (n=2161) by phone. The most common reasons for contact were related to medications (26.8%, n=2341), administrative issues (24.9%, n=2172), investigations (21.2%, n=1848) and clinical concerns (17.4%, n=1516). Across the cohort, there were a mean of 1.4 helpline contacts per person (cpp). People aged between 18-39 years and >89 years had the highest number of contacts per person (1.8 – 2.2), see table 1. Those aged 18-39 used email more than phone for contacts. People residing in large regional areas had the highest utilisation (2.0 cpp), with metropolitan and small regional both at 1.7 cpp. Just over half (53.2%, n=3328) were currently receiving an advanced therapy (biologic or novel small molecule) yet this half accounted for 76.2% (n=6674 contacts) of helpline utilisation compared to those not receiving an advanced therapy (23.8%, n=2080 contacts), perhaps reflective of the complexity of their healthcare or of ensuring supply of these agents.
Conclusion: IBD helplines are well used and play an integral role in healthcare delivery to people with IBD. The preference for digital forms of contact aligns with the shift towards digital communication and highlights the importance of providing a streamlined digital platform to engage with people with IBD, improve satisfaction and healthcare outcomes. Digital platforms have the potential to empower individuals in managing their healthcare by offering on-demand educational resources and solutions to frequently asked questions.
162
Biological agent drug holiday impairs treatment persistence in Crohn’s Disease: Data from the Persistence Australian National IBD Cohort (PANIC5)
Rupert Leong1,2,3, John Chetwood1,2, Aviv Pudipeddi1,2, Thanaboon Chaemsupaphan1,2, Ryan Chang-ho Choi1,2, Yanna Ko1,2, Viraj Kariyawasam1,3 and Sudarshan Paramsothy1,2,3
1Concord Repatriation General Hospital, Sydney, Australia;2Concord Repatriation Hospital, University of Sydney, Australia;3Department of Gastroenterology, Macquarie University Hospital, Australia
Background and Aim: Patients with Crohn’s disease (CD) on monoclonal antibody (mAB) biological agents may occasionally pause treatment to take drug holidays. Upon recommencing the mAB, however, it is unknown if treatment persistence remains the same as their initial trajectory or if loss of persistence occurs. Whether persistence loss differs between mABs, is mitigated by immunomodulators or shorter drug holidays, is also unknown. We evaluated the mAB persistence of CD subjects taking drug holidays versus those who did not as controls.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC) 5 registry of CD subjects up until Dec 2021. The PANIC registry includes 100% of all mAB prescribing data in Australia. Drug holiday was defined as stopping mAB therapy and recommencing the same mAB after a dispensing gap. Non-persistence was defined as failure to dispense advanced therapy prescriptions for >6-months. Kaplan Meier survival curves were generated for persistence and compared using the log-rank test. Cox proportional hazards regression models were employed to calculate hazard ratios (HR) and 95% confidence intervals (CI) with P<0.05 deemed statistically significant SPSS (IBM, USA).
Results: A total of 19,087 unselected CD patients (46.3% male, median 45.7 months follow up) were recruited, contributing 79,677 patient-years of prospective follow-up. There were 3,392 episodes of drug holiday for a median duration of 245 days (IQR: 184-247) compared against 25,866 controls who did not take a drug holiday. Patients who resumed mAB therapy following a drug holiday had a significantly lower median persistence of 23 months versus 49 months in controls (HR: 0.63, 95% CI: 0.60-0.66, P<0.001). Drug holidays <6mth significantly mitigated persistence loss (HR: 1.17, 95%CI: 1.03-1.32, P=0.017) but combination immunomodulator-use did not. TNFi (P<0.001), vedolizumab (P=0.006) and ustekinumab (P<0.001) all demonstrated persistence loss after a drug holiday (Figure).
Conclusions: In Crohn’s disease, upon recommencing monoclonal antibody biological agent after a drug holiday, persistence is significantly reduced irrespective of the biological agent or use of combination immunomodulators. Following a treatment break, especially if longer than 6-months, switching to another advanced therapy may need to be considered.
163
A cross section of inflammatory bowel disease management in older persons in Australasia: Crohn’s Colitis Cure (CCC) data insights program
Crystal Seng1,2, Wai Kin Su3,4,5, William Wilson6,7, Craig Haifer8,9, Astrid-Jane Williams3,10,11, Angela Forbes17, Ian Lawrance12,18, Kate Lynch13,19, Laurel Brett20, Jakob Begun14,21, Susan J Connor3,4,5,11, Jane Andrews4,13,15 and Gareth Walker1,2,16
1The Royal Brisbane and Women's Hospital, Brisbane, Australia;2The University of Queensland, Brisbane, Australia;3Department of Gastroenterology and Hepatology, South Western Sydney Local Health District, Liverpool Hospital, Sydney, Australia;4Crohn’s Colitis Cure, Sydney, Australia;5Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, Liverpool, The Ingham Institute for Applied Medical Research, Australia;6Lyell McEwin Hospital, Adelaide, Australia;7SA Health, Adelaide, Australia;8St Vincent’s Public Hospital Sydney, Sydney, Australia;9St Vincent’s Clinical School, University of New South Wales, Sydney, Australia;10IBD Centre of British Columbia, Canada;11South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;12School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;13Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;14Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia;15Central Adelaide Local Health Network, Adelaide, Australia;16QIMR Berghofer, Brisbane, Australia;17Department of Medicine, University of Otago, Christchurch, New Zealand;18Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Australia;19Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Australia;20Department of Gastroenterology, Logan Hospital, Logan, Australia;21Mater Hospital, Brisbane, Australia
Background and Aim: There is an increasing population of older people living with inflammatory bowel disease (IBD) owing to both increasing incidence after age 70 and longer survival of those with earlier onset disease. Management of this older cohort of people with IBD is challenging given higher average rates of comorbidity, polypharmacy, frailty, infection risk and malignancy. Furthermore, this cohort is often excluded from registry clinical trials which limits the applicability of study findings. Here, we aimed to characterize the real-world state of older persons’ IBD diagnosis and management across Australasia.
Methods: Crohn’s Colitis Care (CCCare) is a cloud-based electronic medical record used in Australasia since 2018. Data feed into a de-identified clinical quality registry (CQR), which was interrogated in April 2024. People with IBD under active care (encounter within 14 months) were included. The cohort was divided into three age groups: <40 years, 40–69 years and ≥70 years.
Results: Of 6388 eligible people, the median age was 42 years (IQR 31–56). Those ≥70 years comprised 8.3% (n=531). Median duration of disease was the longest in those ≥70 years (16.3 years, IQR 7.4–30.8). Time out of daily role was lowest in those ≥70 years, with 97.9% indicating IBD had no impact on their daily activities. Comorbidity analysis found cardiovascular related diseases to be the most common amongst those ≥70 years. In this older cohort, hypertension was the most common (26.7%, n=142) followed by hyperlipidemia (15.1%, n=80), gastroesophageal reflux disease (13.0%, n=69), ischaemic heart disease (10.9%, n=58) and type 2 diabetes mellitus (9.8%, n=52). In comparison, for those aged <40, the most common comorbidities were anxiety (3.7%, n=108), asthma (3.5%, n=102), iron deficiency (3.0%, n=88), depression and anxiety (2.8%, n=80). Medical management characteristics are summarized in Table 1. While we observed similar rates of steroid therapy use in those ≥70 years compared with 40–69 years, we found lower use of immunomodulator (IMM) and advanced therapies (AT) in older patients. There was a lower proportion of those aged ≥70 years receiving infliximab (32.5%) and adalimumab (16.3%) and a greater proportion of this cohort prescribed ustekinumab (24%) or vedolizumab (36.1%). We found the highest proportion of patients with composite endoscopic and radiological remission among those ≥70 years (54%, n=67).
Conclusion: These data show that advanced therapies are commonly used in patients ≥70 years and suggest that clinicians are successfully achieving long term disease control in older patients by preferencing the use of gut-selective and IL12/23 agents. The inclusion of older patients in registry studies and large real-World cohorts, such as CCCare, will help guide optimal therapy in older people with IBD.
164
Mortality in inflammatory bowel disease: Crohn’s Colitis Cure (CCC) data insights program
Owen Alsulaibi1,8, Wai Kin Su1,2,3, William Wilson5,6, Hiu Ching Letisia Sin7,20, Watson Ng2,4, Gareth Walker9,10,11, Angela Forbes12, Ian Lawrance13,14, Kate Lynch15,19, Jakob Begun17,18, Susan J Connor1,2,3,4 and Jane Andrews1,16,19
1Crohn’s Colitis Cure, Sydney, Australia;2Department of Gastroenterology and Hepatology, Liverpool Hospital, Liverpool, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Institute for Applied Medical Research, Liverpool, Australia;4South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;5Lyell McEwin Hospital, Adelaide, Australia;6SA Health, Adelaide, Australia;7St Vincent’s Public Hospital, Sydney, Australia;8Orange Health Service, Orange, Australia;9Royal Brisbane and Women's Hospital, Brisbane, Australia;10University of Queensland, Brisbane, Australia;11QIMR Berghofer, Brisbane, Australia;12Department of Medicine, University of Otago, Christchurch, New Zealand;13Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Subiaco, Australia;14School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;15Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;16Central Adelaide Local Health Network, Adelaide, Australia;17Mater Hospital, Brisbane, Australia;18Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia;19Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;20St Vincent’s Clinical School, University of New South Wales, Sydney, Australia
Background and Aim: The prevalence of Inflammatory Bowel Disease (IBD) has increased worldwide with Australia and New Zealand amongst the highest prevalence rates. Prior literature suggested that people with IBD experienced higher mortality rates than the general population. Advances in therapeutic options have reduced mortality such that IBD may no longer be a life limiting disease. We therefore examined mortality and demographics in a large cohort of people with IBD receiving care in Australasian centres using Crohn’s Colitis Care (CCCare) as their IBD electronic management record (EMR).
Methods: CCCare is a cloud-based EMR used in Australasia since 2018. Data feed into a de-identified clinical quality registry (CQR), which was interrogated in April 2024. People with IBD who have ever been clinically assessed since August 2018 were included.
Results: Of the 8,528 eligible people, 0.6% (n = 54) are documented as deceased. Patient demographics are presented in table 1. Comparing the deceased cohort with the non-deceased, there were a statistically significant difference in median age (71.5 years vs 42 years respectively) and duration of disease (20.3 years vs 10.8 years). In those deceased, a higher proportion of people had Crohn’s disease (74.1%, n=40) compared to the remainder of the cohort. Half of the deceased were aged between 70 – 89 years (50%, n=27). There was no difference between groups in gender, country of residence, or the likelihood of combined endoscopic and radiological remission (based on their last documented investigation results). However, the deceased were more likely to be receiving an advanced therapy (biologic or novel small molecule) at their last clinical assessment. Hypertension was the most common comorbidity documented in both groups (6.8%, n=10 vs 5.9%, n=490). Amongst people with IBD who were deceased ischaemic heart disease (6.1%, n=9), Type 2 diabetes mellitus (5.4%, n=8), and chronic obstructive pulmonary disease (COPD) (3.4%, n=5) were the most common comorbidities. Most of the deceased cohort were active or previous smokers (71.8%, n=22 vs 41.7%, n=2326, p < 0.001).
Conclusion: Although the median age of death amongst people with IBD in CCCare is lower than the median age of 82 in the general Australian population, the most frequently documented comorbidities in this group are reflective of the chronic diseases associated with known causes of death in Australia (Diabetes, Coronary heart disease, COPD, and Asthma). This study would suggest that the advances in IBD therapy have made IBD less likely to be a life limiting disease; rather mortality appears more linked to comorbidities associated with known high mortality rates. Further analysis is required to characterise significant contributors to mortality in people with IBD.
166
Ustekinumab and vedolizumab exhibit superior persistence versus tumour necrosis factor inhibitors in Crohn’s disease: Data from the Persistence Australian National IBD Cohort (PANIC5)
Rupert Leong1,2,3, John Chetwood1,2, Yunki Yau1,2, Fei Pan3, Melissa Kermeen1, Thanaboon Chaemsupaphan1,2, Aviv Pudipeddi1,2, Sudarshan Paramsothy1,2,3 and Viraj Kariyawasam1,3
1Concord Repatriation General Hospital, Concord Repatriation Hospital, Australia;2University of Sydney, Concord, Australia;3Macquarie University Hospital, Macquarie University, Australia
Background and Aim: Persistence serves as an indicator of sustained real-world therapeutic effectiveness of advanced therapies (AT) in the treatment of Crohn’s disease (CD). To date there has been no prospective population-based comparative effectiveness data utilizing a real-world 100% sample dataset. Vedolizumab, traditionally, has not been deemed effective in treating CD. We, therefore, aimed to determine the persistence of tumour necrosis factor alpha inhibitors (TNFi) versus non-TNFi in CD.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC) 5 registry of CD subjects up until Dec 2021. The PANIC registry includes 100% of all AT prescribing data in Australia. Non-persistence was defined as failure to dispense AT prescriptions for >6-months. Kaplan-Meier survival curves were generated for AT persistence and compared using the log-rank test. Cox proportional hazards regression models were employed to calculate hazard ratios (HR) and 95% confidence intervals (CI) with P<0.05 deemed statistically significant SPSS (IBM, USA).
Results: A total of 19,087 unselected CD patients (46.3% male, median 45.7 months follow up) were recruited, contributing 79,677 patient-years of prospective follow-up. The cohort comprised 31,967 treatment lines: 10,218 infliximab (IFX), 12,916 adalimumab (ADA), 2,974 vedolizumab (VED), and 5,859 ustekinumab (UST). In AT-naïve CD subjects, UST persistence (HR: 1.82, 95%CI: 1.65-2.01, P<0.001) and VED persistence (HR: 1.28, 95%CI: 1.15-1.42) were significantly higher than TNFi. In AT-exposed CD subjects, however, only UST persistence (HR: 1.60, 95%CI: 1.49-1.72) was significantly higher than TNFi but not VED (HR: 1.04, 95%CI: 0.97-1.12). IFX persistence was significantly higher than ADA in AT-naïve (HR: 1.08, 95%CI: 1.04-1.12) and in AT-exposed CD subjects (HR: 1.19, 95%CI: 1.11-1.28). Each line failure from 1st to 4th+ line reduced persistence significantly (P<0.001).
Conclusions: In one of the largest direct comparative studies using prospective national population-based registry data, ustekinumab and vedolizumab were significantly more persistent than TNFi in AT-naïve subjects, and ustekinumab had a significantly higher persistence than TNFi in AT-exposed subjects with Crohn’s disease. Vedolizumab effectiveness is highest in AT-naïve subjects.
169
Physical activity is associated with a decreased risk of developing inflammatory bowel disease: a systemic review and meta-analysis
Ho Tuan Tiong1, Dali Fan1, Chris Frampton2, Ho Nam Lee1, Ashwin N Ananthakrishnan3 and Richard Gearry1,2
1Department of Gastroenterology, Christchurch Hospital, Christchurch, New Zealand;2Department of Medicine, University of Otago, Christchurch, Christchurch, New Zealand;3Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School, Boston, USA
Background and Aim: Modifiable risk factors in Inflammatory Bowel Disease (IBD), such as physical activity, may be utilised as prevention strategies. However, the findings of previous studies on the association between physical activity and IBD risk have been inconsistent. We aimed to perform a systematic review and meta-analysis to estimate the effect of physical activity on IBD risk.
Methods: A search was conducted for relevant studies published before April 2023 that assessed the effect of pre-IBD diagnosis levels of physical activity on IBD incidence. Individual summary statistics (relative risks; RR), and confidence intervals (CI) were extracted with forest plots generated. We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to assess the quality of evidence.
Results: 10 observational studies were included (Figs. 1,2). For cohort studies, there were 1,182 Crohn’s disease (CD) and 2,361 ulcerative colitis (UC) patients, with 860,992 participants without IBD. For case-control studies, there were 781 CD to 2,636 controls, and 1,127 UC to 3,752 controls. Compared to individuals with low physical activity levels, the RRs of CD in individuals with high physical activity levels for cohort and case-control studies were 0.78 (95% CI 0.68-0.88, P = 0.0001) and 0.87 (95% CI 0.79-0.95, P = 0.003), respectively. For UC, the RRs were 0.62 (95% CI 0.43-0.88, P = 0.008) and 0.74 (95% CI 0.51-1.07, P = 0.11).
Conclusion: This meta-analysis suggests that physical activity is inversely associated with the risk of developing IBD, more so in CD than in UC.
185
Improved outcomes in long-term follow up of IBD transitions clinic
Alysia Bastas1, Melissa Barbarich1, Taha Mollah2 and Edward Giles3,4
1Monash Health, Monash Children's Hospital, Clayton, Australia;2Department of General Surgery, St Vincent’s Hospital Melbourne, Fitzroy, Australia;3Department of Paediatrics, Monash University, Clayton, Australia;4Centre for Innate Immunity and Infectious Disease, Hudson Institute of Medical Research, Clayton, Australia
Background and Aim: Transitional healthcare is the co-ordinated movement of paediatric patients with chronic conditions to adult care systems. However, this period if often disjointed resulting in disengagement and poor health outcomes. Approximately 10% of IBD cases are diagnosed in childhood, often with more severe symptoms and accelerated progression than adult-onset disease. In November 2016, our tertiary gastroenterology department established a Young Adult IBD Transition Clinic (YAC) for patients aged 16-25. A study published in 2022 demonstrated reduced emergency department attendance and high rates of patient/carer satisfaction in the first two years of this service. (1) The present study aims to evaluate whether enduring positive effects persist across clinical outcomes and patient satisfaction eight years after the establishment of the YAC.
Methods: All patients who visited the YAC between November 2022 and November 2023 were identified (current YAC cohort, n=147). Patients who attended the clinic during its inception phase from November 2016 to June 2018 were used as the control group (initial YAC cohort, n=61). Clinical outcome data were retrospectively collected from electronic medical records. Among the participants, a sub-group completed the IBD-PSQ questionnaire (initial YAC cohort n=34, current YAC cohort n=16), which quantifies participants' level of clinic satisfaction. Data analysis was performed using IBM SPSS Statistics software. The Shapiro-Wilk test assessed normality. For normal data, an independent sample t-test compared means; for non-normal data, the Wilcoxon Rank Sum Test compared medians.
Results: In the initial YAC cohort there were 17 IBD related ED presentations over 22,265 days, while the current YAC cohort had a reduced rate of 26 presentations over 47,414 days (p=0.072). Findings from the IBD-PSQ survey revealed that the mean total score for the current YAC cohort was significantly higher than the initial YAC cohort (77.8750 vs 71.5588, p= 0.031), indicating higher levels of satisfaction. Assessing individual items, 9 of 19 questions (47.3%) had a higher median response in the current YAC cohort, however, only one of these was statistically significant.
Conclusion: This study highlights that in the eight years since its establishment, the YAC clinic has both maintained and demonstrated further improvements in patient outcomes and satisfaction. Studies with extended follow-up periods and increased sample sizes will be required to precisely determine the impact of specialised transitional clinics and focus on components of the service that drive improved outcomes.
Reference
1. Mollah, T, Lee, D, Giles, E. Impact of a new young adult inflammatory bowel disease transition clinic on patient satisfaction and clinical outcomes. Journal of Paediatrics and Child Health.2022; 58(6): 1053–9.
193
The psycho-social impact of fistulising perianal Crohn’s disease in Australasia: Crohn’s Colitis Cure (CCC) data insights program
Dominique Nano2, Wai Kin Su1,2,3, Jack McNamara2, William Wilson7,8, Arteen Arzivian9,10, Astrid-Jane Williams2,4,11, Gareth Walker12,13,14, Angela Forbes15, Heidi Su16, Edward Giles17,18,19, Ian Lawrance20,21, Shoma Dutt22,23, Kate Lynch6,24, Laurel Brett25, Jakob Begun26,27, Jane Andrews1,5,6 and Susan J Connor1,2,3,4
1Crohn’s Colitis Cure, Sydney, Australia;2Department of Gastroenterology and Hepatology, South Western Sydney Local Health District, Liverpool Hospital, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Institute for Applied Medical ResearchLiverpool, Australia;4South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;5Central Adelaide Local Health Network, Adelaide, Australia;6Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;7Lyell McEwin Hospital, Adelaide, Australia;8SA Health, Adelaide, Australia;9St Vincent’s Public Hospital Sydney, Sydney, Australia;10St Vincent’s Clinical School, University of New South Wales, Sydney, Australia;11IBD Centre of British Columbia, Vancouver, Canada;12Royal Brisbane and Women's Hospital, Brisbane, Australia;13University of Queensland, Brisbane, Australia;14QIMR Berghofer, Brisbane, Australia;15Department of Medicine, University of Otago, Christchurch, New Zealand;16Department of Gastroenterology, Te Whatu Ora Health, Christchurch, New Zealand;17Monash Children’s Hospital, Clayton, Australia;18Department of Paediatrics, Monash University, Clayton, Australia;19Centre of innate immunity and infectious diseases, Hudson Institute of Medical Research, Clayton, Australia;20Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Perth, Australia;21School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;22The Children’s Hospital at Westmead, Westmead, Australia;23Speciality of Child and Adolescent Health, Children's Hospital at Westmead Clinical School, Sydney School of Medicine, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;24Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;25Department of Gastroenterology, Logan Hospital, Logan, Australia;26Mater Hospital, Brisbane, Australia;27Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia
Background and Aim: Fistulising perianal Crohn’s disease (fpCD) poses a significant burden for people with Crohn’s disease (CD). FpCD causes pain, incontinence, and increases the risk of sepsis. This impairs several psycho-social factors and quality of life (QoL). We aim to describe the effect fpCD has on QoL as indicated by opioid use, time out of role (TooR), and mental health indicators.
Methods: Crohn’s Colitis Care is a cloud-based electronic medical record used in Australasia since 2018. Data feed into a de-identified clinical quality registry (CQR), which was interrogated in April 2024. All people with CD with a clinical assessment at any time point were included.
Results: Of 4713 people with CD, 83.6% (n=3941) never had fpCD documented, 9.8% (n=461) previously had fpCD, and 6.6% (n=311) currently have active fpCD. The overall median age was 41 years (IQR 30 – 55) with an even gender distribution (50.4% female); most resided in Australia (76.7%, n=3616) with 23.3% in New Zealand (n=1097). More people with current fpCD used opioid analgesia related to their inflammatory bowel disease (IBD), compared to those with previous or never fpCD (2.3% vs 0.9% & 0.6% respectively, p < 0.001). People with current fpCD more commonly had TooR (> 1 day) compared to those with previous or never fpCD (14.0% [n=32] vs 7.5% [n=29] & 6.5% [n=196], p < 0.001). For those with TooR, more people with current fpCD had >10 days (7.0% [n=16] vs 3.1% [n=12] &1.6% [n=47], p < 0.001). Mental health was assessed using Kessler Psychological Distress Scale (K10) and the Depression Anxiety and Stress Scale (DASS-21) - see Table 1. People with current fpCD had higher median scores across all mental health indices compared to those with previous or never fpCD. A higher proportion of people with current fpCD reported moderate to extreme anxiety (37%, n=17) compared to those with previous or never fpCD (26.1%, n=23 and 26.3%, n=117 respectively, p=0.55). There were higher scores for depression (mild to extreme) amongst people with current fpCD (50%, n=23) compared to those with previous (39.8%, n=35) and never fCD (31.9%, n=142, p < 0.05).
Conclusion: People with current fCD have higher rates of opioid use, more TooR, and higher scores in K10 and DASS-21 compared to those who have never had fpCD. This highlights the additional psycho-social impact of fpCD on QoL and the need for proactive management of both their fpCD and resultant psycho-social issues to address this burden holistically.
199
Changing trends in healthcare utilisation in inflammatory bowel disease over the past six years
Caroline Miller1, Kerrie Goldsmith1 and Abhinav Vasudevan1,2
1Eastern Health, Box Hill, Australia;2Monash University, Clayton, Australia
Background and Aim: Rates of inflammatory bowel disease (IBD) are increasing in Australia. IBD nurses and the helplines they run are essential in ensuring the appropriate care of patients with this increasingly complex medical condition. With new treatments becoming available over the last few years, we investigated the changing trends in healthcare utilisation of IBD patients at an Australian hospital network.
Methods: We retrospectively reviewed data from the IBD helpline at a tertiary IBD service over 6 years. Records were kept from regular phone and email contacts, as well as number of patients prescribed biologic therapy within our unit. Overall IBD patient numbers were identified through the hospital’s electronic medical records. Linear regression was used to examine rates over time.
Results: IBD patient numbers have significantly increased by a median of 9% per annum from 1059 patients in 2018 to 1523 in 2023 (p=0.01). The number of patients on advanced therapies increased by 71% during this period, from 329 in 2018 to 563 in 2024, with those requiring escalated dosing growing by 90% in the previous 3 years alone. Despite this increase in number of patients and associated complexity of patients requiring advanced therapeutics, the number of inpatients significantly decreased by a median 8% per year from 153 in 2018 to 96 in 2023 (p=0.02). IBD helpline contacts increased by 265% from 1040 in 2018 to 3795 in 2023, at a median increase of 22% per year (p<0.001). The proportion of patients requiring an ileocolic resection with Crohn’s disease also stayed stable over the duration of analysis.
Conclusion: Despite increased numbers and associated complexity of patients with IBD at our institution, the rate of inpatient admissions has significantly decreased. It is likely that improved therapeutics have reduced hospitalisations, but much of the burden of care has transitioned to outpatient management, with Helpline services and outpatient reviews substantially increasing. Resourcing for IBD services should focus on the increasing need for outpatient services, particularly IBD Helpline services and outpatient reviews, given the changing nature of IBD management.
201
Development and validation of a convolutional neural network model in the detection of Crohn’s disease erosions and ulcers by pan-enteric wireless capsule endoscopy
1Royal Prince Alfred Hospital, Camperdown, Australia;2University of Sydney, Camperdown, Australia;3St Vincents Hospital, Darlinghurst, Australia;4Macquarie University Hospital, Macquarie, Australia;5Concord Repatriation General Hospital, Concord, Australia
Background and Aim: PillCam Crohn’s is a pan-enteric wireless capsule endoscope that directly evaluates both the small bowel and colon. Artificial intelligence (AI) algorithms have shown promise in the endoscopic detection of mucosal inflammation in inflammatory bowel diseases (IBD) with pooled diagnostic sensitivity of 95% and specificity of 94% for detecting intestinal ulcers from capsule endoscopy images(1). We developed and validated an AI algorithm using a convolutional neural network (CNN) for Crohn’s disease (CD) evaluation. This study aimed to determine the accuracy and efficiency in the interpretation of still frames and video input.
Methods: A total of 2846 Pillcam Crohn’s capsule endoscopy still images and short capsule endoscopy video segments (equating to 84,696 images) from the small bowel were captured from 16 CD patients (divided into 80% training and 20% validation datasets). Data inputs were categorised as either normal or abnormal mucosa, stratified by presence of erosions, ulcers, or inflammation. A CNN model (ResNet18, PyTorch) was trained, using labelled data with additional augmentation (image flip, gaussian blur, and colour jitter), to differentiate normal from ulcerated mucosa. The model was assessed in its ability to detect any abnormality in the validation dataset (measured against human reporting), and then evaluated on its ability to determine inflammatory phenotype. Area under curves (AUC) and standard diagnostic accuracy values (sensitivity, specificity, negative-, positive predictive values [NPV/PPV]) were calculated for the CNN model’s ability to detect active small bowel CD.
Results: The CNN model achieved excellent accuracy in the validation phase of 97.8% (sensitivity 98.1%, specificity 97.3%, PPV 98.1%, NPV 97.3%, AUC 0.99; Figure 1). The CNN model detected ulcers with a sensitivity of 94.9%, a specificity of 85.6%, and AUC of 0.95, and detected erosions with a sensitivity of 77.6%, a specificity of 88.5%, and AUC of 0.86. Image review of the false negative erosions demonstrated most were trivial. After training the model with video input, the model’s accuracy in the analysis of video validation data was excellent at 98.2% (sensitivity 89.0%, specificity 99.2%, PPV 93.2%, NPV 98.7%, AUC 0.98), and retained high specificity at the cost of sensitivity in discriminating between ulcers (sensitivity 43.3%, specificity 99.8%, AUC 0.97), erosions (sensitivity 56.2%, specificity 99.2%, AUC 0.96) and inflammation (sensitivity 48.0%, specificity 99.9%, AUC 0.99). The CNN model was able to achieve these results in under 3 minutes, representing a significant time saving when compared to human analysis and reporting.
Conclusion: The CNN model was highly accurate and efficient in the detection of CD mucosal abnormalities when encountering still frames or video input data. The ability to distinguish normal from abnormal mucosa was highly precise. The model’s sensitivity in differentiating ulcers, erosions or inflammation was less accurate. The high accuracy in detecting abnormalities does lend this algorithm to being incorporated into capsule endoscopy reporting software as an adjunct to promptly draw attention to abnormalities, and reduce fatigue and human error- much in the way polyp detection algorithms are incorporated into colonoscopy processing software.
Reference
1. Soffer, S, Klang, E, Shimon, O, Nachmias, N, Eliakim, R, Ben-Horin, S, et al. Deep learning for wireless capsule endoscopy: a systematic review and meta-analysis. Gastrointestinal Endoscopy. 2020: 92; 831-839.e8.
202
Transmural healing is associated with a reduced risk of clinical relapse in Crohn’s disease
Aravind Gokul Tamilarasan1,2, Dina Bestawros3, Chris Chiu3, Stephen Oborn1, Jessica Yang3,4, Sudarshan Paramsothy3,4 and Rupert Leong3,4
1Royal Prince Alfred Hospital, Camperdown, Australia;2University of Sydney, Camperdown, Australia;3Concord Repatriation General Hospital, Concord, Australia;4Macquarie University Hospital, Macquarie, Australia
Background and Aim: Transmural healing is listed as a potential measure of depth of Crohn’s disease (CD) remission in the latest consensus guidelines from the International Organisation for the Study of Inflammatory Bowel Diseases (IOIBD). Whether transmural healing is associated with clinical remission or protective against longitudinal clinical relapse in uncertain. We aimed to determine the relevance of endoscopic, histologic, and radiologic assessment of ileal CD on longitudinal outcomes.
Methods: Consecutive patients with ileocolonic CD were recruited if they had magnetic resonance enterography (MRE) and colonoscopy with ileal biopsies within a 6-month period. Collected data included patient demographics, baseline clinical, endoscopic, histologic and radiologic disease status, medical therapy, and rates of clinical relapse in the subsequent 18 months. The composite endpoint of clinical relapse was defined as the presence of one of: need for corticosteroids or exclusive enteral nutrition or Crohn’s disease exclusion diet, Crohn’s disease-related hospitalisation or surgery, or an elevated faecal calprotectin (FCP≥100). Histologic assessment with modified Global Histologic Disease Activity Score (GHAS) was calculated by an independent, blinded expert gastrointestinal pathologist with a score >4 defining active inflammation. Blinded central radiologists determined the simplified MaRIA score with ≥2 defining active disease. Categorical predictive factors were assessed using Fisher’s exact test. Multiple logistic regression was used to perform multi-variate analysis. For those in clinical remission at baseline, log-rank analysis was used to assess the time to clinical relapse and displayed using the Kaplan Meier method. Statistical analysis was performed using SPSS.
Results: In total, 122 patients were identified (January 2017-June 2021) of whom 51 patients were excluded due to inadequate clinical information, duplication of records, or due to the colonoscopy/MRE not occurring within 6 months. Therefore, 71 patients were included in the final analysis. Univariate analysis determined that the odds of longitudinal clinical relapse were far lower for patients in remission, compared with disease activity, for each respective modality. Odds ratio for clinical relapse amongst those in endoscopic (ER), histologic (HR), radiologic (RR) or clinical remission (CR) at baseline are listed in Table 1. Multivariate analysis determined that the only factor independently associated with avoidance of clinical relapse was radiologic remission (OR 0.18, p=0.008). Correspondingly, only radiologic remission (compared with radiologic disease activity) at baseline demonstrated significantly longer relapse-free survival (491 days vs 342 days, p=0.009, Figure 1). Histologic (509 vs 421 days, p=0.086) and endoscopic remission (503 vs 407 days, p=0.374) showed numerically longer relapse-free survival compared with disease activity, but this did not reach statistical significance.
Conclusion: Baseline disease remission (endoscopic, histologic, radiologic, and clinical) was associated with avoidance of clinical relapse at 18 months. However, upon multivariable analysis only radiologic remission was independently associated with prevention of clinical relapse, and also showed significantly longer relapse-free survival. This adds to the current literature demonstrating the myriad benefits of transmural healing in CD. We would advocate for clinicians including transmural healing as a therapeutic target in the management of CD patients.
203
The burden of mental health issues in people with inflammatory bowel disease in Australasia: Crohn’s Colitis Cure (CCC) data insights program
Taryn Lores1,6, Sabina Iliescu2, Wai Kin Su2,3, William Wilson4, Kirsty Leray5, Gordana Kuzet2, Kate Lynch1,6, Jane Andrews1,6 and Susan J Connor2,3,7
1CALHN, Adelaide, Australia;2Liverpool HospitalDepartment of Gastroenterology and Hepatology, South Western Sydney Local Health District, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Institute for Applied Medical Research, Liverpool, Australia;4SA Health, Adelaide, Australia;5St Vincent's Clinical School, University of New South Wales, Sydney, Australia;6The University of Adelaide, Adelaide, Australia;7South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia
Background and Aim: The burden of mental health issues (MHIs) in people with Inflammatory bowel diseases (IBD) is high. To facilitate their recognition and management, brief psychological screening measures the Depression, Anxiety and Stress Scale (DASS-21) and the Kessler Psychological Distress Scale (K10) are available Crohn’s Colitis Care (CCCare). CCCare is a cloud-based electronic medical record that has been used in Australasia since 2018. CCCare data feed into a de-identified clinical quality registry (CQR) for research and auditing purposes. The CQR was analysed to determine frequency of survey use and prevalence of psychological distress.
Methods: The CQR was interrogated in April 2024. CCCare consumers were included in the analysis if they ever had 1) a clinical assessment, and 2) at least one of the psychological screening measures completed. Respondents were classified as being at risk for clinically relevant psychological distress (CRPD) if they scored in the moderate-to-extremely severe ranges on any of the DASS-21 scales and/or moderate-to-severe ranges on the K10. Consumers may have been sent assessments multiple times; only their most recent scores were used in this analysis.
Results: Of the 8,504 IBD consumers who had ever had a clinical assessment on CCCare, 2,221 (26.1%) were sent the DASS-21 and 1,815 (21.3%) were sent the K10; completion rates were 41.4% and 39.3%, respectively. A total of 1,015 (11.9%) had at least one scale score available for analysis. Screening scores are presented in Table 1. Median age of respondents was 41 years (IQR=31-53) and median disease duration was 10.6 years (IQR=6-18). Women were more likely to complete the questionnaires than men (DASS-21: 46% vs 37%; K10: 43% vs 36%). A substantial proportion of respondents scored at risk for CRPD, including 22% for depression, 27% for anxiety, 17% for stress and 24% for general distress. There was no difference between subtypes of IBD. For consumers with CD, a higher proportion of those with current fistulising disease (fCD) scored in the mild range for depression, compared to those who never had or had fCD previously (50% [n=23] vs 31.9% [n=142] vs 39.8% [n=35], respectively, p<.05). Amongst the broader CCCare cohort (n=8,504), anxiety was the fifth most reported comorbidity (3.5%, n=296), depression the sixth (3.2%, n=273) and depression with anxiety the tenth (2.4%, n=206).
Conclusion: In this large cohort of people with IBD on CCCare, only a quarter had been invited to complete psychological screening. Of these, up to one-in-four screened at risk of CRPD. Much of this distress is likely under-recognised and under-managed in routine IBD care due to resource limitations and funding constraints. Increased use of the screening module is likely to improve the recognition of mental health needs in the IBD population.
205
The prevalence and impact of obesity in an ANZ cohort of people with inflammatory bowel disease: Crohn’s Colitis Cure (CCC) data insights program
Patricia Kaazan1,2, Wai Kin Su3,4, Christopher Rayner1, Gareth Walker5,11, William Wilson7, Elaine Dinoy8, Gabrielle Wark3, Angela Forbes9, Michael Schultz9, Jia Yap9, Ian Lawrance10, Shoma Dutt11, Kate Lynch1, Laurel Brett15, Jakob Begun12, Jane Andrews1,13 and Susan J Connor4,14
1Faculty of Health Sciences, The University of Adelaide, Adelaide, Australia;2Flinders Medical centre, department of Gastroenterology and Hepatology, Adelaide, Australia;3Liverpool Hospital, Department of Gastroenterology and Hepatology, South Western Sydney Local Health District, Liverpool, Australia;4The Ingham Institute for Applied Medical Research, Liverpool, Australia;5University of Queensland, Brisbane, Australia;6QIMR Berghofer, Brisbane, Australia;7SA health, Adelaide, Australia;8St Vincent's public Hospital, Sydney, Australia;9University of Otago, Dunedin, New Zealand;10School of Medicine and Pharmacology, Perth, Australia;11Speciality of Child and Adolescent Health, Children's Hospital at Westmead Clinical School, Sydney, Australia;12Mater Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia;13Central Adelaide Local Health Network, Adelaide, Australia;14South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia
Background: Obesity is one of the main threats to global health. An estimated 31% of Australians live with obesity, a proportion that has almost doubled since 1995. Between 15-40% of patients with inflammatory bowel disease (IBD) are reportedly obese (Body Mass Index (BMI) ≥30 kg/m2), but Australian data are lacking. Visceral adiposity represents a chronic inflammatory state, and previous data suggest deleterious effects of obesity on both IBD pathogenesis and course1.
Methods: Crohn’s Colitis Care is an IBD cloud-based electronic medical record used by multiple Australasian IBD centres. Data are fed into a de-identified clinical quality registry (CQR), which was interrogated in April 2024. Patients with IBD under active care (encounter within 14 months) with sufficient data to calculate BMI were included. We assessed the prevalence and severity of obesity (using BMI as a surrogate) and explored whether it influenced dosing of advanced therapies (biologics and novel small molecules). Dose escalated is defined as daily dose equivalence > standard daily dose equivalence. Similarly, dose reduced is defined as daily dose equivalence < standard daily dose equivalence. Daily dose equivalence (mg/day) calculated as dose (mg) divided by frequency in days.
Results: Of 4763 eligible patients, 87.1% (n=4147) resided in Australia and 12.9% (n=616) in New Zealand. In total 2404 patients were prescribed an advanced therapy. The median BMI and BMI classification were similar across both countries and largely across IBD treatment sites. Patient characteristics are presented in table 1. There was a statistically significant difference in dosing variations of advanced therapies across different BMI groups (χ2 = 23.5, P<0.05). In the underweight group, more patients received dose escalation and less patients received standard dosing. In the morbidly obese group, less patients received standard dosing of advanced therapy. Waist circumference (a more accurate indicator of visceral adiposity) was only available in 218 patients (4.5%). Median waist circumference for males was 98 cm (87-107) and for females 86 (76-98.3), both in the high-risk category.
Conclusion: In the largest Australasian study assessing obesity in IBD, the prevalence of obesity and overweight was 56%, in line with global reports. Extreme BMI values were significantly associated with different dosing of advanced therapies. Obesity is an important issue that warrants proactive management and further examination. Waist circumference should routinely be documented as an easily obtained surrogate for visceral adiposity to facilitate clinical research in this area.
Reference
1.
Kaazan, P, Seow, W, Yong, S, Heilbronn, LK, Segal, JP. The Impact of Obesity on Inflammatory Bowel Disease. Biomedicines. 2023 Dec 8; 11(12): 3256. doi: https://doi.org/10.3390/biomedicines11123256.
Table 1
225
Iron deficiency with or without anaemia continues to be an issue in inflammatory bowel disease: Crohn's Colitis Cure (CCC) data insights program
Brigid Pinnuck1, Wai Kin Su2,3,4, William Wilson5,6, Joseph Pipicella3,4,7, Watson Ng2,8, Sally Antoniades9, Gareth Walker10,11,12, Angela Forbes13, Shoma Dutt14,15, Kate Lynch1,16, Susan J Connor2,3,4,8 and Jane Andrews4,16,17
1Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;2Department of Gastroenterology and Hepatology, Liverpool Hospital, South Western Sydney Local Health District, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Medical Institute for Applied Medical Research, Liverpool, Australia;4Crohn's Colitis Cure, Sydney, Australia;5Lyell McEwin Hospital, Adelaide, Australia;6SA Health, Adelaide, Australia;7Medicine and Health, South West Sydney Clinical School, University of New South Wales, Sydney, Australia;8South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia;9St Vincent's Hospital Sydney, Sydney, Australia;10Royal Brisbane and Women's Hospital, Brisbane, Australia;11University of Queensland, Brisbane, Australia;12QIMR Berghofer, Brisbane, Australia;13University of Otago, Christchurch, New Zealand;14The Children's Hospital at Westmead, Sydney, Australia;15Specialty of Child and Adolescent Health, Children's Hospital Westmead Clinical School, Sydney School of Medicine, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;16Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;17Central Adelaide Local Health Network, Adelaide, Australia
Background: Inflammatory bowel disease (IBD) increases the risk of nutritional deficiencies, particularly iron deficiency (ID), which is due to chronic blood loss from ulceration and intestinal inflammation causing increased iron demand and malabsorption. Reported rates of ID in IBD cohorts largely vary from 23-90% worldwide, influenced by age, gender, nutritional status and comorbidities. ID can occur without anaemia and anaemia is not universally caused by ID.
Method: Crohn’s Colitis Care is a cloud-based electronic medical record used in Australasia. Data feed into a de-identified clinical quality registry (CQR), which was interrogated in April 2024. People with IBD under active care (encounter within 14 months) were included to explore the prevalence of ID in this cohort. ID was defined as a serum ferritin level of <30mcg/L or a serum ferritin level 30-100mcg/L and serum transferrin saturation <16%. Anaemia was defined as a haemoglobin (Hb) of <130 g/L in males and <120 g/L in females.
Results: The cohort under active care included 6,259 people, of whom 37.3% (n=2,335), had iron studies (IS) (serum ferritin and transferrin saturation) and a Hb recorded. Their median age was 41 years (IQR 30-56) with an even gender distribution (50.4% female); 87.2% (n=2,037) resided in Australia and 12.8% (n=298) in New Zealand. Crohn’s disease (CD) affected 60.8% (n=1,419) of the cohort, ulcerative colitis (UC), 37.0% (n=864) and IBD unspecified (IBDU), 2% (n=52). ID was found in 21.5% (n=502) of those with IS, with an equal rate amongst IBD subtypes; 20.9% in CD, 22.2% in UC and 26.9 % in IBDU. Of those with ID, 26.7% (n=134) had concurrent anaemia (28% (n=84) in CD, 24% (n=46) in UC, and 4%, (n=4) in IBDU). In those with ID, the most common form of iron replacement was ferric carboxymaltose (n=45, 74%), yet overall, 60/502 (12%) with ID were documented to have been given iron replacement. A subgroup analysis in those with ID at a single site showed that 45% (n=18/40) were prescribed iron replacement. The median C-reactive protein for those with IS was 2.3 (IQR 0.9-4.5).
Conclusion: ID is more common than ID with anaemia in this large ANZ IBD cohort. While rates of ID with anaemia are low, it is likely to be impairing quality of life. Our data suggest either variation in iron repletion practice between sites or in its documentation; with one site having a repletion rate of 45% compared to an average of 12% overall. Despite the ease of diagnosis and the importance of managing ID, it remains an area with significant opportunity to improve practice and outcomes. Protocolised screening and repletion may be needed to ensure consistency.
227
Is there a link between inflammatory bowel disease and oral cancer: Case series
1Darwin Hospital, Department of Gastroenterology, Royal;2School of Medicine, Flinders University;3Department of Gastroenterology, Royal Melbourne Hospital
Crohn’s disease (CD) and Ulcerative Colitis (UC), make up the large majority of inflammatory bowel diseases (IBD), and affect different sites along the length of the gastrointestinal tract. Their initial presentation leading up to the diagnosis of IBD may include symptoms of diarrhoea, rectal bleeding, abdominal pain and weight loss. There is no clear established etiology for IBD, however it is thought to be driven by genetic, environmental, immunological and infectious factors. Increasing incidences of IBD have been observed worldwide (including Australia), with more than 100,000 people in Australia living with a variant of IBD. Oral cancers are historically linked to well-known behavioural risk factors such as tobacco smoking and alcohol consumption, however its association with IBD are scarcely reported and reviewed. However, it appears that there may be a causal link between diagnosis of IBD, and the development of carcinoma of the oral cavity based on current available literature. In our case series, we review two patients with IBD on a biologic treatment, whom after initially presenting with oral ulcers was confirmed to have oral carcinomas on subsequent further investigations.
228
Disseminated melioidosis in inflammatory bowel disease: A case report
Yu Sung Kim1,2, Tessa Cubilo1, Robyn West1, Metthananda Nawarathne1, Guru Iyngkaran1,3 and Kirsty Campbell1,2
1Darwin Hospital, Department of Gastroenterology, Royal;2School of Medicine, Flinders University;3Department of Gastroenterology, Royal Melbourne Hospital
Inflammatory Bowel Diseases (IBD), including Crohn’s Disease (CD) and Ulcerative Colitis (UC), are inflammatory diseases of the gastrointestinal tract. Immunosuppressive therapy and biologic agents are commonly used treatments for the management of IBD. However, these therapies are associated with an increased risk of infection. As a result, screening for certain infections are pre-requisites prior to commencing these therapies in patients.
Meliodosis, an infection caused by the bacterium Burkholderia pseudomallei (B. pseudomallei), is commonly seen in the tropics and the sub-tropic regions of the world. The Northern Territory has a higher prevalence of melioidosis and other diseases such as strongyloides, compared to the rest of Australia. This raises the question of whether pre-biologic screening in patients who have travelled or lived in the Northern Territory should be standardised to include these diseases. We explore a case of the devastating effects of disseminated melioidosis on a CD patient who had been managed on biologic therapy, and the following management challenges it presents.
231
The introduction of an intestinal ultrasound service significantly reduces diagnostic endoscopy usage in an inflammatory bowel disease service
Grace Feng1,2, Robert Little1,2, Zaid Ardalan1,2, Anthony B Friedman1,2, Rebecca Smith1,2, Kirstin M Taylor1,2 and Miles P Sparrow1,2
1Department of Gastroenterology Alfred Health, Melbourne, Australia;2Monash University, Melbourne, Australia
Background and Aim: Endoscopic assessment is the gold standard for monitoring of inflammatory bowel disease (IBD) activity. Increasingly, intestinal ultrasound (IUS) is utilised as a non-invasive alternative disease monitoring strategy. Our aim was to quantify and compare endoscopy usage for evaluation of IBD disease activity before and after the introduction of an IUS service.
Methods: A retrospective single-centre study was performed. Total numbers of lower GI endoscopies (ileocolonoscopy or flexible sigmoidoscopy) performed for luminal Crohn’s disease (CD) or ulcerative colitis (UC) disease evaluation were collected across two 5-year time periods: the pre IUS era (2010-2014) and the IUS era (2015-2019). Endoscopies for dysplasia surveillance were excluded. The primary endpoint was a comparison of the cumulative number of endoscopies for IBD activity evaluation annually relative to the annual number of patients seen in clinic in the pre-IUS and IUS eras. Secondary endpoints included evaluating the number of endoscopies by individual year within each time period, endoscopies according to diagnosis (CD vs UC), and the number of IUS performed within the IUS era. Categorical variables were compared using a Chi-squared test.
Results: The number of endoscopies performed for IBD disease evaluation decreased from 576 in the pre-IUS era to 474 in the IUS era despite an increase in cumulative annual patient reviews (1985 vs 3337 patient reviews, respectively). The annual number of endoscopies for disease evaluation per patient in the pre-IUS and IUS eras is illustrated in Figure 1. The proportion of cumulative annual endoscopies relative to patients reviewed across the 5-years reduced from 29 per 100 patients in the pre-IUS era to 14 per 100 patients in the IUS era (OR 2.47, 95% CI 2.15-2.84; p < 0.001). There was a reduction in total endoscopies for CD evaluation from 325 to 264 and for UC evaluation from 251 to 210. The proportion of cumulative annual endoscopies relative to patients reviewed reduced from 30 to 14 per 100 patients in CD (OR 2.60, 95% CI 2.16-3.12; p < 0.001), and 37 to 17 per 100 patients in UC (OR 2.90, 95% CI 2.33-3.59, p<0.001). In the IUS era, a total of 3319 IUS were performed (2673 CD, 646 UC). This included 1467 IUS for assessment of suspected activity (44 per 100 patients/year) and 1852 IUS for objective confirmation of clinical remission (55 per 100 patients/year).
Conclusion: In the 5 years following introduction of an IUS service, the number of endoscopies performed for evaluation of IBD activity per patient review was halved. With IUS being performed for both assessment of disease activity and objective confirmation of clinical remission, the potential workflow and cost savings of reducing endoscopies for IBD disease activity evaluation are significant.
237
Corticosteroid and opiate use in inflammatory bowel disease, 25 years after the TREAT Registry was established
Brigid Pinnuck1, Wai Kin Su2,3,4, William Wilson5,6, Joseph Pipicella3,4,7, Gabrielle Wark2, Michele Arcidiacono8, Gareth Walker9,10,11, Angela Forbes12, Heidi Su13, Michael Schultz14, Ian Lawrance15,16, Shoma Dutt17,18, Laurel Brett19, Kate Lynch1,20, Jane Andrews4,20,21 and Susan J Connor2,3,4,22
1Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;2Department of Gastroenterology and Hepatology, Liverpool Hospital, South Western Sydney Local Health District, Sydney, Australia;3Gastroenterology, Hepatology and Inflammatory Bowel Disease Research Group, The Ingham Medical Institute for Applied Medical Research, Sydney, Australia;4Crohn's Colitis Cure, Sydney, Australia;5Lyell McEwin Hospital, Adelaide, Australia;6SA Health, Adelaide, Australia;7Medicine and Health, South West Sydney Clinical School, University of New South Wales, Sydney, Australia;8St Vincent's Hospital Sydney, Sydney, Australia;9Royal Brisbane and Women's Hospital, Brisbane, Australia;10University of Queensland, Brisbane, Australia;11QIMR Berghofer, Brisbane, Australia;12Department of Medicine, University of Otago, Christchurch, New Zealand;13Department of Gastroeneterology, Te Whatu Ora Health, Christchurch, New Zealand;14Department of Meidcine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand;15Centre for Inflammatory Bowel Disease, Saint John of God Subiaco Hospital, Perth, Australia;16School of Medicine and Pharmacology, University of Western Australia, Perth, Australia;17The Children's Hospital at Westmead, Sydney, Australia;18Specialty of Child and Adolescent Health, Children's Hospital Westmead Clinical School, Sydney School of Medicine, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;19Department of Gastroenterology, Logan Hospital, Logan, Australia;20Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;21Central Adelaide Local Health Network, Adelaide, Australia;22South West Sydney Clinical Campuses, University of New South Wales, Sydney, Australia
Background and Aim: Despite data from the TREAT (Crohn’s Therapy, Resource, Evaluation, and Assessment Tool) registry, corticosteroids and opiates are still frequently used in inflammatory bowel disease (IBD). During an IBD flare, corticosteroids are a common first line option, and opiates are often prescribed for associated abdominal pain. However, longer term use of both agents increases the risk of complications, other adverse IBD outcomes and can impair quality of life. We aimed to describe the current real-world prescribing practices of corticosteroids and opiates for people with IBD across Australia and New Zealand (NZ).
Method: Crohn’s Colitis Care is a cloud-based electronic medical record used in Australasia. Data feed into a de-identified clinical quality registry, which was interrogated in April 2024. People with IBD under active care (encounter within 14 months) were included.
Results: Of 6382 eligible people, 76.9% (n=4,907) resided in Australia and 23.1% (n=1,475) in NZ. There was an even gender distribution (50.2% male). The median age was 42 years (IQR 31–56) and median disease duration was 10.7 years (IQR 5.1-18.8). In the preceding year, 9.3% (n=591) of the cohort were prescribed a course of corticosteroids, of those, 57.9% (n=342) were also prescribed an advanced therapy (biologic or novel small molecule). The most common reasons for discontinuing steroids were “rationalisation and/or deep remission” (30.6%, n=166), “inadequate efficacy” (29.0%, n=157) and “course completed” (20.3%, n=110). There were no differences in the rate of steroid use between IBD subtypes (8.7% in Crohn’s disease (CD) vs 11.2% in IBD unclassified (IBDU) vs 9.8% in ulcerative colitis (UC), p=0.22). Opiates were prescribed in 8.1% (n=519). However, opiates were only prescribed for an IBD indication in 27 people (0.4% of the cohort), with others receiving opiates for non-IBD indications. People with CD were more likely to have been prescribed an opiate than those with IBDU and UC (p<0.001).
Conclusion: Globally, reported corticosteroid used in IBD is variable (13-57%), with our reported use at the lower end of this, however much of the comparative data were explored over longer time periods. Pleasingly, local use appears to be short term with “deep remission” and “course completed” being common reasons for cessation. Opiate use within this large Australian and NZ cohort is comparable to international data. Interestingly, while corticosteroids are predominately used for IBD, opiate use appears related to other comorbidities. These comorbidities, including mental health, are important to examine to identify further opportunities to optimise care.
241
Development and validation of a simplified scoring system that predicts two-year clinical remission in patients with ulcerative colitis on vedolizumab
1Department of Gastroenterology and Liver Services, Concord Hospital, Sydney, Australia;2Division of Gastroenterology, Department of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand;3Faculty of Medicine and Health, University of Sydney, Sydney, Australia;4Department of Gastroenterology, Tan Tock Seng Hospital, Singapore;5Faculty of Medicine and Health Sciences, Macquarie University, Australia;6Department of Gastroenterology and Hepatology, Blacktown and Mount Druitt Hospital, Australia
Background and Aims: Vedolizumab is the gut-selective advanced therapy which is safe and efficacious for treatment of ulcerative colitis (UC). Once patients achieve successful induction, there is a risk of loss of response leading to eventual flare. We aimed to identify these predictive factors and develop a practical scoring system to determine ongoing efficacy of vedolizumab.
Methods: We performed logistic regression on prospectively recruited UC subjects from the Vedolizumab Immunomodulator Enforced Withdrawal Study (VIEWS). All patients were in corticosteroid-free clinical and endoscopic improvement at baseline and continued vedolizumab. Predictive factors of two-year corticosteroid-free clinical remission were determined and modelled into the VIEWS score, then validated in another UC cohort.
Results: Of 62 patients in derivation cohort, 48 (77.4%) maintained clinical remission over two years. The predictive factors of remission were female (OR:6.0), anti-tumor necrosis factor naive (OR:3.8), baseline histological remission (OR:10.8), thiopurine combination (OR:3.6), and fecal calprotectin level ≤250 μg/g (OR:6.3). These factors were incorporated into VIEWS Score, yielded an AUROC curve of 0.89 (95%CI:0.81-0.98) in prediction of two-year clinical remission (Figure A: derivation cohort, B: validation cohort). Of 64 UC patients in the validation cohort, 40 (62.5%) remained in clinical remission at two years with AUROC of 0.77 (95%CI:0.60-0.94). At a cut-off threshold of 4, VIEWS score identified two-year clinical remission with sensitivity of 88.4% and specificity of 63.6%.
Conclusion: This is the first study to determine predictive factors and propose scoring system of ongoing clinical remission in UC patients on maintenance vedolizumab. In patients at high risk of relapse, combination therapy with thiopurine may be beneficial.
243
Knowledges and perspectives of gastroenterologists across the Asia-Pacific region towards the use of histology in inflammatory bowel disease
1Department of Gastroenterology and Liver Services, Concord Repatriation General Hospital, Sydney, Australia;2Division of Gastroenterology, Department of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand;3Faculty of Medicine and Health, University of Sydney, Sydney, Australia;4Department of Gastroenterology, Tan Tock Seng Hospital, Singapore;5Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital Jinshan branch, New Taipei, Taiwan;6Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan;7Faculty of Medicine and Health Sciences, Macquarie University, Sydney, Australia
Introduction: Recently, histological outcomes have gained significant attention as a potential new treatment target for patients with inflammatory bowel disease. However, it remains unclear whether gastroenterologists in the Asia-Pacific region possess adequate knowledge and hold positive attitude towards utilizing histology in this context. This study aimed to evaluate their knowledge and attitudes through a comprehensive survey.
Methods: A cross-sectional survey was conducted from May to September 2023 among gastroenterologists in the Asia-Pacific region, incorporating data from a previous Australian survey conducted in 2022. The questionnaire assessed knowledge and attitude towards the role and the application of histology in IBD practice. Statistical analyses were employed to compare knowledge scores and identify predictors. Ethical approval was obtained, and participation was voluntary with implied consent.
Results: A total of 221 Gastroenterologists from 12 Asia-Pacific countries, including 77 (34.8%) from Australia, responded to questionnaire, with 185 (83.7%) completed the survey. The mean knowledge score was 9.8 ± 3.3 out of 19 (51.6%). There was no significant difference in the average score among countries (P=0.53). In univariable analysis, IBD specialist, PhD degree, and regular participation in IBD multidisciplinary teams were associated with higher knowledge scores (P<0.001, 0.02, and 0.01, respectively) (Figure). Most respondents (90.7%) agreed on the importance of histology in IBD. While 54.6% of Australian gastroenterologist perceived the role of histology as established, only 37.0% of Asian respondents from Asia considered this similarly (P=0.02). Histological activity alone minimally influences treatment escalation for patients with endoscopic remission, but achieving combined histo-endoscopic remission often leads to therapy de-escalation.
Conclusion: Although majority of gastroenterologists in Asia-Pacific region are aware of the use of histology in IBD, they have limited histological knowledge and do not routinely apply in clinical practice. There is a need to enhance this knowledge to gastroenterologists and promote routine use of standard histological evaluations in IBD practice.
247
Inflammatory bowel disease acute clinic – the Canterbury, New Zealand experience
Catherine Wall1,2, Samantha Benson-Pope1,2, Kirsten Arnold1,2, Richard Gearry1,2 and Heidi Su1
1Christchurch Hospital, Christchurch, New Zealand;2University of Otago Christchurch, Christchurch, New Zealand
Background and Aim: The prevalence of inflammatory bowel disease (IBD) is increasing. It is essential that patients with IBD have timely access to specialist follow-up to avoid unplanned care. We aimed to describe the outcomes of a recently introduced IBD Acute Clinic.
Methods: The IBD Acute Clinic is run weekly, with patients reviewed by the IBD Fellow or IBD Clinical Nurse Specialist. Referral criteria include acutely unwell patients, patients with a new diagnosis of IBD, and patients recently discharged from hospital requiring short-term follow-up. An IBD dietitian is available fortnightly to see acute clinic patients, and referral is at the discretion of the IBD Fellow or Clinical Nurse Specialist or based on the Crohn’s Colitis Care (CCCare) IBD nutrition self-screening tool (IBD-NST) score of >2. Data were collected on indication for referral, time from referral to review, referral for imaging and endoscopy, changes to treatment, admissions to hospital post-review, and referral to IBD dietitian. During the first three months of the clinic, patients were emailed a brief survey following the appointment to assess their clinic format experience.
Results: In the first 12 months of the clinic. 237 patients were reviewed in 48 clinics, 7 (2.9%) patients did not attend and 4 (1.6%) were admitted to hospital prior to review. Most referrals were for flare of IBD symptoms (69.6%) or follow up post hospital discharge (13.5%). Patients were assessed within an average of 5 working days of referral and 19% had a phone assessment. Imaging and endoscopy were requested for 21.1% and 24.9% of patients respectively and 62.9% had escalation of treatment. A sixth of patients received dietitian care which included management of malnutrition, nutritional treatments for active disease and healthy eating education. Pre-clinic nutrition screening was possible via CCCare. The patient experience survey was emailed to and completed by 28/59 patients. Most (96%) reported that being seen in the clinic was of benefit to them, and 17% reported that they would have presented to the emergency department or after-hours general practice service if this short-interval review were not available.
Conclusion: The IBD Acute Clinic has been successful at reviewing IBD patients at short notice and has likely led to a reduction in unplanned care. Routine implementation of a nutrition screening tool with patients attending the IBD acute clinic may improve patient access to nutrition care. Early assessment and treatment is likely to lead to improved outcomes for patients with IBD.
256
Disease clearance after 16 weeks of treatment with vedolizumab in patients with moderate to severe ulcerative colitis: An interim analysis from the VERDICT trial
Vipul Jairath1,2,3, Guangyong Zou2,3,4, Shashi Adsul5, Jean-Frederic Colombel6, Geert R D'Haens7, Marcelo Freire5, Gordon W Moran8,9, Laurent Peyrin-Biroulet10,11,12,13,14, William J Sandborn15, Shaji Sebastian16, Simon Travis17, Séverine Vermeire18, Jurij Hanžel3,19, Christopher Ma3,20,21, Rocio Sedano1,2,3, Patrick Sheridan3, Naveen Arya22, Melanie Beaton1, Peter Bossuyt23, Silvio Danese24, Daniel Green25, William Harlan III26, Marek Horynski27, Jaroslaw Kierkus28, Adam Kopoń29, Maria Klopocka30,31, Remo Petroniene32, Mark S Silverberg33, Lukasz Wlanski34, Brian G Feagan1,2,3 and Donna Abercrombie35
1Department of Medicine, Division of Gastroenterology, University of Western Ontario, London, ON, Canada;2Department of Epidemiology and Biostatistics, University of Western Ontario, London, ON, Canada;3Alimentiv Inc., London, ON, Canada;4Robarts Research Institute, Schulich School of Medicine and Dentistry, University of Western Ontario, London, ON, Canada;5Takeda Pharmaceuticals, Cambridge, MA, USA;6Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA;7Department of Gastroenterology and Hepatology, Amsterdam University Medical Centers, Amsterdam, the Netherlands;8Nottingham Digestive Diseases Biomedical Research Centre, University of Nottingham, Nottingham, UK;9NIHR Nottingham Biomedical Research Centre, Nottingham University Hospitals NHS Trust, Nottingham, UK;10Department of Gastroenterology, Nancy University Hospital, F-54500, Vandœuvre-lès-Nancy, France;11INSERM, NGERE, University of Lorraine, F-54000, Nancy, France;12INFINY Institute, Nancy University Hospital, F-54500, Vandœuvre-lès-Nancy, France;13FHU-CURE, Nancy University Hospital, Nancy, France;14Groupe Hospitalier Privé Ambroise Paré – Hartmann, Paris IBD Center, Neuilly sur Seine, Paris, France;15Division of Gastroenterology, University of California San Diego, La Jolla, USA;16IBD Unit, Hull University Teaching Hospitals, Hull, UK;17Kennedy Institute and Biomedical Research Centre, University of Oxford, Oxford, UK;18Department of Gastroenterology and Hepatology, University Hospitals Leuven, KU Leuven, Leuven, Belgium;19Department of Gastroenterology, Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia;20Division of Gastroenterology & Hepatology, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada;21Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada;22ABP Research Services Corp., Oakville, Canada;23Imelda GI Clinical Research Center, Imelda General Hospital, Bonheiden, Belgium;24Gastroenterology and Gastrointestinal Endoscopy Unit, IRCCS San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy;25Department of Gastroenterology, Taunton Surgical Centre, Oshawa, Canada;26Asheville Gastroenterology Associates, Asheville, USA;27Endoskopia Sp. z.o.o., Sopot, Poland;28The Children’s Memorial Health Institute, Warsaw, Poland;29Department of Gastroenterology, Toruńskie Centrum Gastrologiczne Gastromed, Toruń, Poland;30Department of Gastroenterology and Nutritional Disorders, Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, Poland;31Gastroenterology Clinic, Dr. Jana Biziel University Hospital n 2 in Bydgoszcz, Bydgoszcz, Poland;32Barrie GI Associates Inc., Barrie, Canada;33Toronto Immune and Digestive Health Institute, Toronto, Canada;34Gastroenterological Department, Samodzielny Publiczny Zakład Opieki Zdrowotnej w Łęcznej, Łęcznej, Poland;35Takeda Pharmaceuticals Australia, Sydney, Australia
Background and Aim: Disease clearance in ulcerative colitis (UC) is defined as concurrent achievement of clinical, endoscopic, and histologic remission. Regardless of the drug used in clinical trials, no more than 20% of patients reach disease clearance after 1 year; thus, it is a high bar to achieve with a potential for disease modification. VERDICT is a continuing, randomised, controlled trial (NCT04259138) with a primary objective of determining the optimal treatment target in moderately-to-severely active UC, by comparing target Group 1 (corticosteroid-free [CSF] symptomatic remission), target Group 2 (CSF symptomatic remission + endoscopic improvement), and target Group 3 (CSF symptomatic remission + endoscopic improvement + histologic remission). Patients follow treatment algorithms that feature early introduction of vedolizumab (VDZ) with no dose escalation before week 16 and no week 10 dosing. Here we report the achievement of CSF disease clearance at week 16 in Group 3.
Methods: CSF disease clearance was defined as achievement of a CSF Mayo rectal bleeding subscore=0 + endoscopic improvement (Mayo Endoscopic Score [MES] ≤1) + histologic remission (Geboes score <2B.0). VDZ 300 mg was administered intravenously following a treatment algorithm based upon baseline UC treatment until assigned treatment target was reached at week 16. Results are summarized overall and by bio-exposure status.
Results: As of 18 Aug 2023, 553 patients were enrolled in VERDICT with 253 assigned to target Group 3. The group had a mean age of 41.2 years (standard deviation [SD] 14.3), mean disease duration of 7.3 years (SD 7.8), and 42% were female (Table). In total, 216 (85%) were bionaïve, 159 (63%) had a baseline MES of 3, and 129 (51%) were receiving concomitant corticosteroids. Figure 1 shows the breakdown of the 253 patients. At time of analysis, remission target status was unavailable for 30 bionaïve and 11 bio-exposed patients. Among the 212 patients with observed data, 86 (41%) achieved CSF remission, including 77 (41%) of the 186 bionaïve patients with data and 9 (35%) of the 26 bio-exposed patients with data. Corresponding values of achieving CSF disease clearance in the intention-to-treat population were 34% (86/253), 36% (77/216), and 24% (9/37), respectively. All patients with disease clearance were receiving VDZ treatment from baseline.
257
Preferences towards treatment attributes among patients with Crohn’s disease and ulcerative colitis in Argentina, Australia, Brazil, Saudi Arabia and Taiwan: a discrete choice experiment
Yoon-kyo An1, Marjorie Argollo2, Domingo C Balderramo3, Azzam Nahla4, Chia-Jung Kuo5, Olga Fadeeva6 and Elenor Uy6
1Mater Hospital, Brisbane, Australia;2Department of Gastroenterology, Federal University of São Paulo, São Paulo, Brazil;3Servicio de Gastroenterología y Endoscopia Digestiva, Hospital Privado Universitario de Córdoba, Instituto Universitario de Ciencias Biomédicas de Córdoba, Córdoba, Argentina;4Division of Gastroenterology, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia;5Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taiwan;6Takeda Pharmaceuticals International AG, Singapore
Background: Advanced therapies (ATs) with different mechanisms of action and routes of administration (RoA) are used for inflammatory bowel disease (IBD: Crohn’s disease [CD] and ulcerative colitis [UC]), and patients (pts) play an increasing role in the decision-making process. Pts’ preferences for treatment attributes from 7 European countries have been reported previously; however, evidence from non-European countries is lacking.
Methods: Adult pts with CD or UC on treatment for ≥6 months from Argentina, Australia, Brazil, Saudi Arabia and Taiwan were enrolled in this cross-sectional, self-administered online survey (Oct 2022 to May 2023). Pts’ preferences for IBD treatment attributes are described. In a discrete choice experiment, the relative importance of treatment attributes was estimated using conditional logit models.
Results: Overall, 706 pts with CD and UC (n=353 each) completed the survey. Mean (standard deviation [SD]) ages (years [y]) were 36.8 (9.9) and 37.7 (10.2), 47.9% and 47.6% were female, and mean (SD) disease durations (y) were 4.5 (6.0) and 4.6 (6.7) for CD and UC, respectively; 58.1% (CD) and 56.1% (UC) were exposed to ATs. For pts with CD, the rate of long-term remission on maintenance therapy (MT) was the most important attribute for treatment choice (32.5%), followed by the rate of 1-y remission (25.7%), RoA (24.6%) and risk of serious adverse events (AEs, 11.5%) and mild AEs (5.8%). For pts with UC, the rate of corticosteroid-free remission after 1 y was the most important attribute (30.8%), followed by RoA (27.4%), rate of mucosal healing after 1 y (16.1%), long-term remission on MT (14.9%) and risk of serious AEs (10.0%) and mild AEs (0.8%). Country-specific results are shown in the Table. Compared with intravenous administration every 4–8 weeks, pts with CD preferred subcutaneous (SC) administration every 1–2 weeks (odds ratio [95% confidence interval]: 1.41 [1.27–1.56] P<0.001) or every 4–12 weeks (1.22 [1.08–1.39, P=0.002]), and pts with UC preferred taking a tablet (1.41 [1.25–1.59], P<0.001) or SC administration every 4–12 weeks (1.30 [1.14–1.48], P<0.001) or every 1–2 weeks (1.20 [1.07–1.35], P=0.002). Pts exposed to ATs ranked the importance of RoA lower than that of effectiveness compared with AT-naïve pts, and 49.3% of pts with CD and 50.5% with UC indicated that they wanted ATs to start earlier.
263
Insights into patient perspectives: acute severe ulcerative colitis inpatient experience survey
Mustafa Mohamedrashed, Saiumaeswar Yogakanthi, Ayushi Chauhan, Sarah Lucas, Soleiman Kashkooli and Mayur Garg
Northern Health, Melbourne, Australia
Background and Aim: Acute severe ulcerative colitis (ASUC) represent a severe manifestation of inflammatory bowel disease (IBD) that requires close monitoring and aggressive treatment. This study aimed to evaluate the experience of patients admitted to a single tertiary service with ASUC, focusing on perception of the received therapy, and preferences regarding location of care.
Methods: Patients admitted with ASUC between May 2022 and October 2023 were invited to participate in a retrospective qualitative and descriptive study by completing a short online survey in February 2024. Patients were identified through retrospective review of the unit’s existing inflammatory bowel disease database, with 35 patients randomly selected for participation. Data regarding disease characteristics, management and outcomes were obtained through retrospective review of electronic medical records. Statistical analysis was performed using Prism 10 (GraphPad Software Inc., La Jolla, USA).
Results: Of the 35 patients invited, 27 (77%) responded. Only patients fulfilling Truelove and Witt’s criteria for ASUC were included in this study (20/27, 74%). 13 (65%) were female with a median age of 34 (IQR 29-50) years. The median disease duration was 2.25 (IQR 1.6-6.5) years, and the median length of stay was 5 (IQR 4.37-6.62) days. The majority of study participants were exposed to 5ASA therapy prior to their index admission at 14/20 (70%), and 7/20 (35%) had received prior immunomodulator or biological therapy. Most study participants reported they received excellent overall inpatient care (75%) and strongly agreed with feeling safe when being managed as an inpatient (85%). Furthermore, 15/20 (75%) of participants felt their individual needs and questions were met during their hospitalisation and 16 (80%) strongly agreed with that their management plan and disease was well explained during hospitalisation. A preference for inpatient rather than ambulatory settings was noted by the majority (14/20, 70%) for management of their episode of ASUC.
Conclusion: In this single retrospective descriptive study, patients admitted with ASUC experienced a high degree of satisfaction with their care, with a preference towards inpatient care. Most patients preferred inpatient intravenous based management. Larger studies are required to elucidate the additional factors that drive this preference and those that would increase patient comfort with ambulatory care of this condition.
265
Is there a “weekend effect” on clinical outcome of acute severe ulcerative colitis? A single centre retrospective analysis
Mustafa Mohamedrashed1, Saiumaeswar Yogakanthi1, Diana Lewis1, Ryan Bartlett1, Leya Nedumannil1, Melissa Chew1, Rebecca Pearce1, Soleiman Kashkooli1 and Mayur Garg1,2
1Northern Health, Melbourne, Australia;2The University of Melbourne, Melbourne, Australia
Background and Aim: Acute severe ulcerative colitis (ASUC) represents a medical emergency that requires hospitalisation, close monitoring and intensive medical therapy. The “weekend effect” refers to the observed phenomenon of poorer patient outcomes when admitted over the weekend compared to weekdays. The aim of this study is to examine the effects of this phenomenon on multiple clinical outcomes in patients admitted with ASUC.
Methods: Patients admitted with ASUC between January 2016 to May 2023 were identified retrospectively using our centre coding discharge data. Patient characteristics and clinical outcomes were accessed from the electronic medical records (EMR). The primary outcome was length of initial hospitalisation, with secondary outcomes being time to first endoscopic assessment, requirement for rescue therapy, time to rescue therapy, rate of colectomy, and 12-month readmission rate. Weekday admissions were defined as Monday-Thursday, with weekend admissions Friday-Sunday.
Results: 95 patients (53% male; median age 35 [IQR 28.5-49] y) fulfilling Truelove and Witts’ criteria were included in this study. 67 (70.5%) were admitted on weekdays, and 28 (29.5%) on weekends. Baseline characteristics of both groups are outlined in Table 1. The median length of initial hospitalisation was 6.5 (IQR 5-11) days in patients admitted on weekdays compared with 6 (IQR 4-9) days in those admitted on weekends (p = 0.15). The time to first endoscopic assessment was one day vs three days (p = 0.10) in those admitted on weekdays vs weekends, respectively. Rescue therapy with infliximab was required in 30 (31.5%) vs 18 (19%) patients (p = 1.0), respectively. The median time for infliximab therapy was 4 (IQR: 3-6) days in weekday group vs 3 (IQR: 2-5) days in weekend group (p = 0.07). There was no significant difference in requirement for colectomy (3 vs 1 patients, p = 1.0). Twelve-month all-cause readmission rates were similar for both weekday and weekend admission groups (33/67 [49%] vs 10/28 [35.7%], p = 0.32). UC-related readmissions were similar (weekday 13/67 [19.4%] vs. weekend 7/28 [25%], p = 0.73), as were non-UC-related admissions (weekday 20 [29.8%] vs. weekend 3 [10.7%], p = 0.08).
Conclusion: Patients admitted to hospital with ASUC on weekends had a trend towards delayed endoscopy, but no statistically significant differences across other measured parameters. Weekend admission did not negatively influence clinical outcomes.
267
Unique faecal microbial profiles in first degree relatives of inflammatory bowel disease patients
Sabrina Koentgen1, Fan Zhang1, Nan Wu1, Thisun Jayawardana1, Robert Little2, Paris Tavakoli3, Simon Ghaly3, Susan J Connor4 and Georgina Hold1
1Micobiome Research Centre, UNSW, Sydney, Australia;2Department of Gastroenterology, Alfred Hospital, Melbourne, Australia;3St Vincents Hospital, Sydney, Australia;4Liverpool Hospital, Sydney, Australia
Background and Aim: Inflammatory bowel disease (IBD) is a chronic, relapsing and remitting condition comprising both ulcerative colitis (UC) and Crohn’s disease (CD). While the aetiology of IBD is unknown, a range of genetic and environmental risk factors have been described. First-degree relatives (FDRs; siblings, parents and children) of IBD patients share many of these factors and are known to have a 2-20-fold increased risk of IBD development. To better understand the interplay between environmental and genetic risk factors, we evaluated the gut microbial profiles of an FDR cohort, their IBD probands and healthy controls (HC). The aim was to identify whether FDRs of IBD patients have healthy or IBD-like microbial features.
Methods: All participants were recruited as part of the Australian IBD Microbiome (AIM) study; a longitudinal observational cohort with 3-monthly clinical sampling (faecal and oral) over a two-year period. Participants were selected based on self-reported first-degree relative status (n=68) and, where possible, affected IBD relatives (n=24) were included for comparison. All participants were antibiotic free for 3-months prior to baseline sample submission. FDR case-control matching (~1:3; n=203) was performed using the MatchIt package in R-studio, based on age, sex, BMI, ethnicity, smoking status, education and ‘Index of relative socio-economic advantage and disadvantage’ (IRSAD) decile. Baseline oral and faecal samples underwent DNA extraction and 16S rRNA sequencing (Ramaciotti Centre for Genomics, UNSW). The Microbiome Research Centre 16S analysis pipeline and R studio were used for statistical analysis and data visualisation.
Results: The FDR group was predominantly female (63%) with a mean age of 49.7 years and BMI of 25.5 kg/m2. Case-control matching resulted in a balanced cohort with standard mean difference falling below 0.2 for all variables. The IBD cohort was significantly different in age to FDR (mean 36.7 vs. 49.7 years, respectively; p < 0.05) but not controls (mean 40.4 years) and BMI was comparable between groups. Both ethnicity and smoking status were consistent between groups. European Australians were the most represented ethnic group (47.6%) and 98.6% of participants across the cohort were non-smokers. Education and IRSAD decile were high among all groups (university educated; 81.2% IRAD decile 8-10) and alcohol consumption was not significantly different. Oral microbiota profiles showed no significant difference in alpha diversity across FDR, IBD and HC groups. When comparing participants within the IBD group, patients with CD had lower alpha diversity than those with UC (p=0.016). Differential abundance analysis of the oral microbiota revealed FDRs had increased abundance of Oribacterium, Granulicatella, Lachnoanaerobaculum and Rothia compared to HC, and increased levels of Capnocytophaga, Tannerella and Abiotrophia compared to the IBD group. Faecal microbial profiles between groups had greater differences than oral signatures. In agreement with other studies, the IBD group had significantly reduced alpha diversity compared to both FDR and HC groups. All groups were compositionally different by Bray-Curtis beta dissimilarity analysis (p<0.018). FDRs had higher abundance of Akkermansia, Alistipes and Monoglobus compared to both IBD and HC groups. FDRs and IBD shared similar abundance of Butyricicoccus which was lower than that observed in the HC group.
Conclusion: Despite limited differences in oral microbiome profiles between FDRs and healthy controls had greater variance at the genus level than the IBD patients compared to either group. Faecal microbial analysis showed distinct differences with enrichment of key beneficial genera in the FDR group. FDR profiles however still shared significant gut microbial features with the IBD group and remained distinct from healthy controls. These oral and faecal signatures may indicate a higher risk microbial profile in FDRs. Future analyses of longitudinal samples, incorporating evaluation of microbial functional activity may determine the significance of the distinct microbial signature observed in FDRs of IBD.
269
Longitudinal microbial dynamics in an Australian adult inflammatory bowel disease cohort
Yashar Houshyar1, Fan Zhang1, Nan Wu1, Paris Tavakoli1,2, Michael C Grimm1, Susan J Connor1,3,4, Simon Ghaly2 and Georgina Hold1
1UNSW, Sydney, Australia;2St Vincents Hospital, Sydney, Australia;3Gastroenterology Department, Liverpool Hospital, Sydney, Australia;4Ingham Institute, Sydney, Australia
Background and Aim: The aetiology of inflammatory bowel disease (IBD) has been proposed to include an inappropriate host immune response to environmental triggers including the gut microbiota particularly in genetically susceptible individuals. Reduced microbial diversity and altered populations of commensal and pathogenic microbes are commonly seen in IBD. However, comprehensive analysis of microbiome changes in an Australian IBD cohort has not been undertaken. The Australian IBD Microbiome (AIM) Study was established in 2019 to define microbiota signatures in a longitudinal Australian IBD cohort. The aim of this current study was to investigate FCP and microbial analysis in AIM study participants over 12 months.
Methods: Of 144 AIM participants (49 Crohn’s disease (CD), 47 ulcerative colitis (UC) and 48 healthy controls (HC)) were included for this study. Clinical information, patient-reported data, and biological samples were collected every three months over the 12-month period. Microbiome structure/function of stool samples was undertaken using shotgun metagenomic sequencing (MGS; Illumina at Ramaciotti Centre for Genomics, UNSW). Alpha diversity was measured using Shannon’s index and beta diversity assessed through Bray-Curtis similarity. Taxonomic variations were analysed using the Wilcoxon rank-sum test, while the DESeq2 method was used to identify differentially abundant functional pathways. FCP levels were quantitatively measured using the Calprotectin ELISA ALP kit (CALPROLAB, Norway). Statistical analysis was performed using R studio.
Results: Median age at recruitment was 44 years for CD and UC and 39.5 years for HCs (p = 0.009) with 57%, 55% and 42% respectively being female (p = 0.34). The average disease duration for CD was 147.8 months and 162.4 months for UC (p = 0.64). The most common phenotype in CD was L2 (colonic; 39%) followed by L1 (Ileal; 37%) and L3 (Ileocolonic; 22%). 32% of UC patients had proctitis followed by pancolitis (23%) and left-sided colitis (28%). 7 CD and 6 UC patients had documented flares of disease activity during the 12-month period. FCP values were significantly higher in both CD and UC compared to HC (median for CD = 36.5 (0 - 2574) vs HC = 5.49 (0 - 172.5; p < 0.0001)) and UC = 41.2 (0-2926) vs HC = 5.49 (0-172.5; p < 0.0001)); However, there were no significant differences between CD and UC. CD showed a significant reduction in microbial alpha diversity at both the phylum and genus levels compared to both HC and UC (p = 0.002, p < 0.001). UC showed a significant reduction at the genus level compared to HC (p = 0.01) but was not significantly different at phylum level. Beta diversity indicated that CD had high variability and distinct microbial patterns compared to HC and UC (p = 0.001). UC also showed significant difference with HC (p = 0.001); however, the variability was less compared to CD. CD showed an increased abundance of Proteobacteria (p = 0.029), Bacteroidota (p = 0.0003), and decreased Firmicutes (p < 0.0001), with higher Escherichia (p < 0.0001) and Bacteroides (p = 0.002) compared to HC. UC had decreased Desulfobacterota, Verrucomicrobiota (p < 0.0001), and increased Alistipes (p = 0.02), and Lachnospira (p < 0.01) compared to HC. Interestingly, functional analysis demonstrated that CD exhibited more severe and widespread metabolic disruptions compared to UC and HC with an upregulation in pathways related to cell proliferation, oxidative stress, and microbial metabolism, while UC was characterised by disruptions in nitrogen metabolism and decreased carbohydrate and vitamin K2 metabolism.
Conclusion: Our findings reveal that similar to other study cohorts, Australian IBD patients exhibit elevated FCP levels together with alterations in microbiome signatures mainly in CD indicating higher levels of intestinal inflammation and severe microbial disruptions in IBD compared to HC. Functional analysis indicates that there is an upregulation of various inflammatory pathways in IBD. These findings highlight unique microbial dynamics and metabolic disruptions in CD and UC, providing valuable insights into the pathophysiology of IBD.
270
Completion rates when collecting detailed dietary information from adults and children in a longitudinal IBD cohort study
Kelly Lambert2, Denelle Cosier1,2, Thisun Jayawardana1, Paris Tavakoli1 and Georgina Hold1
1UNSW, Sydney, Australia;2School of Medical, Indigenous and Health Sciences, University of Wollongong, Wollongong, Australia
Background and Aim: The Australian Inflammatory Bowel Disease Microbiome (AIM) Study is an ongoing longitudinal cohort examining 500 adults and children with IBD and 500 healthy controls. Given the key role that diet plays in driving the profile of the microbiome, it is critical to collect detailed dietary information from study participants. Few studies exist that provide comprehensive information on how to achieve this on a widespread scale. The aim of this paper is to describe completion rates and feasibility of techniques used for collecting detailed dietary data from adults and children in a prospective cohort study.
Methods: Participants recruited to the AIM Study complete 24 detailed data collection instruments at three time points (baseline, 12 and 24 months). To collect information on potential changes in nutrient intake and dietary patterns over time, study participants complete detailed dietary information. Of the three dietary instruments, a 3-day food diary is recorded in the Easy Diet Diary smartphone app developed by Xyris™ and electronically emailed to the research team. Participants unable to access or complete via the app complete a paper 3-day food diary. A validated 80-item food frequency questionnaire (Cancer Council Victoria) was separately administered using unique links. A validated food avoidance and restriction questionnaire is completed via REDCAP to evaluate the prevalence and patterns of food restriction and avoidance.
Results: Details on the completion rates for the first 1000 participants recruited are shown in Table 2. Although 658 food records were returned at baseline, 606 of these contained ≥3 days of dietary data and were considered complete. Hard copies were returned by 14.8 % of participants at baseline (13.5% adults and 23% children). Healthy controls were significantly more likely to complete food diaries than people with IBD (p<0.0001). Adults with IBD were more likely to submit completed food diaries than children (63.2% vs 45.5%, p = 0.03). Completion of food diaries did not differ according to IBD type (p=0.21). Completion rates for 12 and 24 months were higher in part due to non-continuance of participants who did not complete the previous milestone.
Conclusion: Given the strong interaction between diet and the gut microbiota, it is essential that good quality detailed dietary information is collected in future studies. The collection of detailed dietary information is time and resource intensive. This study gives insight into the completion rate of detailed dietary information tools and may be used to inform the design of future studies.
287
A non-invasive inflammatory bowel disease severity index can help predict a complicated course of illness
Akhilesh Swaminathan1,2, Grace Borichevsky1, Chris Frampton1, Mark Hampton1, Anthony Kettle1, Laurent Peyrin-Biroulet3,4, Corey Siegel5, Andrew Day1 and Richard Gearry1
1University of Otago, Christchurch, New Zealand;2Alfred Health, Melbourne, Australia;3Department of Gastroenterology, Nancy University Hospital, Nancy, France;4INSERM, NGERE, University of Lorraine, Nancy, France;5Section of Gastroenterology and Hepatology, Dartmouth Hitchcock Centre, Lebanon, USA
Background and Aim: The disease severity index (DSI) for inflammatory bowel disease (IBD) is a novel tool that encapsulates the burden of illness but requires endoscopic assessment. This study developed non-invasive DSIs using faecal calprotectin (DSI-fCal) and faecal myeloperoxidase (DSI-fMPO) instead of colonoscopy and investigated whether these indices were associated with the burden of disease.
Methods: Adults with Crohn’s disease (CD) and ulcerative colitis (UC) were recruited prospectively and followed for 24 months. Baseline biomarker concentrations were used to develop DSI-fCal and DSI-fMPO, and these were correlated with the original DSI, baseline IBD symptoms (Harvey-Bradshaw index for CD and simple clinical colitis activity index for UC), endoscopic activity (simple endoscopic score for CD and UC endoscopic index of severity), symptoms of stress (perceived stress scale-10), depression (patient health questionnaire-9), anxiety (generalised anxiety disorder scale), and quality-of-life (QoL; IBD questionnaire 32). Area under the receiver-operating-characteristics curves (AUROC) assessed baseline DSI-fCal/DSI-fMPO as predictors of incident clinical and biochemical remission at six months (symptom remission and fCal <150 μg/g), and a complicated IBD course at 24 months (disease relapse needing escalation of biologicals/immunomodulators/recurrent corticosteroids, IBD-hospitalisations/surgeries). Multivariable binary logistic regression assessed the utility of DSI-fCal/DSI-fMPO in predicting a complicated IBD course.
Results: In total, 171 patients were included (CD=99, female=90, median age=46y (IQR 36-59)). DSI-fCal and DSI-fMPO correlated with the original DSI (r>0.9, p<0.001), endoscopic indices (r=0.45-0.49, p<0.001), IBD-symptoms (r=0.53-0.58, p<0.001), stress (r=0.25-0.30, p<0.1), depression (r=0.32-0.35, p<0.001), anxiety (r=0.16-0.19, p<0.05), and QoL (r=-0.57—0.58, p<0.001). Baseline DSI-fCal (AUROC=0.79, 95% CI 0.65-0.92) and DSI-fMPO (AUROC=0.80, 95% CI 0.67-0.93) were associated with six month clinical and biochemical remission. DSI-fCal (AUROC=0.83, 95% CI 0.77-0.89) and DSI-fMPO (AUROC=0.80, 95% CI 0.73-0.87) performed similarly in predicting a complicated IBD-course to the original DSI (pdifference>0.05, Figure 1). The non-invasive DSIs were independently associated with a complicated IBD-course on multivariable analyses (DSI-fCal28, aOR=6.04, 95% CI 2.42-15.08; DSI-fMPO25, aOR=7.84, 95% CI 2.96-20.73).
291
The role of bound anti-drug antibodies to infliximab in predicting future immunogenic failure when de-escalating from combination therapy with an immunomodulator to anti-TNF monotherapy: The Risk Assessment of drug-bound anti-drug-antibodies for Predicting immunogenicity during Immunomodulator De-escalation to Infliximab Monotherapy (RAPID-IM) Study
Karla Cameron1, Melissa Sam2,3,4,7, Nithya Thennakoon11, Bonita Gu7,10, Arteen Arzivian8, Thomas Skinner8, Edward Shelton11, Craig Haifer8,9, Susan J Connor7,10, Catherine Toong3,5,6,12, Peter Gibson1, David Gibson1, Alex Boussioutas1, Miles P Sparrow1 and Mark Ward1
1Department of Gastroenterology, School of Translational Medicine, Monash University and Alfred Health, Melbourne, Australia;2Immunology Laboratory, Department of Haematology, NSW Health Pathology, Liverpool, Australia;3Immunology Research Group, Ingham Institute for Applied Medical Research, Liverpool, Australia;4School of Chemistry, University of NSW, Sydney, Australia;5Department of Immunology, Liverpool Hospital, Liverpool, Australia;6Immunology, NSW Health Pathology, Sydney, Australia;7South-West Sydney Clinical School, University of NSW, Sydney, Australia;8Department of Gastroenterology, St Vincent's Hospital, Sydney, Australia;9School of Clinical Medicine, University of NSW, Sydney, Australia;10Department of Gastroenterology, Liverpool Hospital, Liverpool, Australia;11Department of Gastroenterology, Monash Health, Melbourne, Australia;12University NSW, Sydney, Australia
Background and Aim: Withdrawing immunomodulators (IM) from combination therapy with infliximab (IFX) can lead to immunogenic failure due to development of antibodies to IFX (ATI). Conventional drug sensitive ELISAs detect ATI only when IFX drug levels are undetectable. We investigated whether bound ATIs detected using a novel drug tolerant ELISA taken at time of de-escalation to IFX monotherapy, predicted subsequent loss of response and unfavourable IFX pharmacokinetics in IBD patients on combination therapy.
Methods: Multicentre case-control retrospective study of IBD patients treated with combination IV IFX and IM. Patients had > 6 months steroid-free clinical (Harvey Bradshaw Index ≤ 4/Partial Mayo Score ≤ 2) and biochemical remission (C-reactive protein (CRP) <5 mg/L or faecal calprotectin (FCP) <150 μg/g). Cases (withdrew IM and continued IFX monotherapy) were compared to controls (continued combination therapy). The primary endpoint was relapse (clinically active disease with elevated FCP or CRP) over 24 months follow-up; secondary endpoints included changes in therapy and IFX drug levels. Therapeutic drug monitoring with a drug-tolerant ELISA was collected within 3 months of IM withdrawal.
Results: Bound-ATI were detected in 7/45 (15.6%) cases and 5/37 (13.5%) of controls, none of which tested positive for ATI using drug sensitive ELISA. The groups were well matched, although median duration of combination therapy was longer in cases than controls (41 vs. 20 months, p=0.045) (Table 1). Median duration of follow-up was 17 months. No patients with bound ATI at baseline met the primary endpoint of disease relapse. Higher rates of biochemical disease activity and treatment escalation in the withdrawal group were noted, however ATI status was not associated with these outcomes. When considering changes in IFX levels over subsequent 12 months, there was no significant difference between cases and controls (-0.99 and -0.84 mg/L respectively, p = 0.20). A trend was observed for greater decreases in IFX drug levels in those with ATI at baseline, and in all IM withdrawal patients with ATI, infliximab levels reduced from baseline.
294
Long-term follow up of patients with inflammatory bowel disease treated for cytomegalovirus colitis
Gurtej Singh1, William Beattie1, Britt Christensen1,2, Finlay Macrae1,2 and Jonathan Segal1,2
1Department of Gastroenterology, The Royal Melbourne Hospital, Melbourne, Australia;2Melbourne Medical School, The University of Melbourne, Melbourne, Australia
Background and Aim: Cytomegalovirus (CMV) is a virus commonly found latent in all humans which may be pathologically reactivated by inflammation and immunosuppression; both present in the pathogenesis and treatment of Inflammatory Bowel Disease respectively. Whether CMV colitis is associated with escalating medical therapy, further hospital admissions, and worse clinical outcomes such as toxic megacolon or colectomy when compared to non-CMV associated flare-ups remains controversial. This study’s aims were to follow up IBD patients following CMV colitis and assess disease progression and clinical outcomes.
Methods: A retrospective study of patients treated at Royal Melbourne Hospital between 2018-2023 was completed. Included patients had a diagnosis of IBD, positive immunohistochemistry for CMV on biopsy, and were treated with Ganciclovir or Valganciclovir for CMV colitis. Data collected included demographic details and laboratory investigations at time of first episode of CMV colitis. Data regarding treatment for IBD and CMV colitis at time of CMV colitis was also collected. Outcome results were collected at 6-month and 12-month time points after first episode of CMV colitis.
Results: Fourteen patients were included in this study; 13 with UC and 1 with CD. Recurrence of CMV colitis occurred in 21% of cases at 6 months and 29% at 12 months. Additional courses of corticosteroids remained constant at 21% of cases at 6 and 12 months. Forty-three percent of patients had changed their biologic at 6 months and this stayed constant at 12 months. Similarly, 29% of patients had escalated their biologic dose at 6 months which was the same at 12 months. At 6 months, 43% of patients had been re-hospitalised due to IBD or CMV including 2 colectomies. At 12 months, these figures increased to 36% and 3 respectively. Disease remission was only achieved by 7% of patients at 6 months, increasing to 29% at 12 months.
Conclusion: While a descriptive study, our results compared with previous studies suggest that CMV colitis is a negative prognostic marker in patients with IBD. Patients had higher rates of hospitalisation, failed medical therapies, and one in five patients proceeded to colectomy. These risks may be greater at <6 months from index episode of CMV colitis. High rates of CMV recurrence suggest that clinical practice may also need to be changed, such as longer durations of anti-viral treatment following CMV colitis episodes. Further research regarding effective management of CMV colitis is needed to minimise poor outcomes in these patients.
304
Trends in length of stay and steroid use in patients admitted with acute severe ulcerative colitis: impact of escalated and intensified infliximab dosing
Ryan Bartlett1, Mustafa Mohamedrashed1, Saiumaeswar Yogakanthi1, Melissa Chew1, Leya Nedumannil1, Rebecca Pearce1, Sarah Lucas1, Ayushi Chauhan1, Diana Lewis1, Soleiman Kashkooli1 and Mayur Garg1,2
1Northern Health, Melbourne, Australia;2The University of Melbourne, Melbourne, Australia
Background and Aim: Acute Severe Ulcerative Colitis (ASUC) represents a medical emergency necessitating prompt management with intravenous steroids. Between 30-50% of patients require rescue therapy, with modern strategies transitioning toward escalated or intensified infliximab dosing. This project evaluated the association between evolving strategies with length of stay and 12-month cumulative steroid burden.
Methods: Patients admitted with ASUC between January 2016 and December 2023 were identified retrospectively using discharge codes and patient records. Patient characteristics and clinical outcomes were accessed from electronic medical records with index admissions being analysed. Infliximab rescue therapy was defined as standard dose if up to 5mg/kg was administered in the first 14 days of admission or escalated/intensified if ≥10mg/kg was administered. Outcomes assessed included length of hospitalisation, 12-month cumulative steroid exposure (in prednisolone mg equivalent) and readmission rates. Statistical analysis was performed using Mann-Whitney U and Pearson’s Chi-Square tests.
Results: 111 patients (47 [42.3%] female, median age 38 [range 19-93] years) met Truelove and Witts criteria for ASUC. 55 (49.5%) patients required infliximab rescue therapy, with 25 (45.5%) patients receiving infliximab standard dose and 30 (54.5%) patients receiving intensified infliximab dosing. There was an increasing trend in the proportion of patients receiving escalated/intensified infliximab from 2016-2019 (20.8%) to 2020-2023 (40.9%) (p=0.08). Length of stay was similar in patients who received standard or escalated/intensified infliximab (median 6 vs 8.5 days, p=0.128). Readmission rates were similar with 12% in patients receiving escalated/intensified dose vs standard dose (12% vs 28% p=0.278). 12-month cumulative steroid usage was similar in patients who received standard (median 1850mg [IQR=1625-2465]mg) and escalated/intensified (median 1650mg [IQR=1452.5-1880]mg) infliximab (p=0.163). Median length of stay did not significantly change (p=0.193) between 2016-2019 (6 days) and 2020-2023 (6 days). Median 12-month cumulative steroid exposure remained stable when comparing 2016-2020 and 2020-2023 (1705mg vs 1667.5mg, p=0.981). ASUC readmission rates remained stable when comparing 2016-2020 (18.2%) and 2020-2023 (25.6%).
305
Rise in admissions for acute severe ulcerative colitis at a metropolitan health service with a culturally and linguistically diverse population: implications for health resource planning
Ryan Bartlett1, Mustafa Mohamedrashed1, Saiumaeswar Yogakanthi1, Melissa Chew1, Leya Nedumannil1, Rebecca Pearce1, Sarah Lucas1, Ayushi Chauhan1, Diana Lewis1, Soleiman Kashkooli1 and Mayur Garg1,2
1Northern Health, Melbourne, Australia;2The University of Melbourne, Melbourne, Australia
Background and Aim: Australia has an increasingly multicultural population with a rising migrant profile. Epidemiological data suggests greater risk of inflammatory bowel disease in first- and second-generation migrants from a low to high prevalence country, with risk of Ulcerative Colitis (UC) preceding Crohn’s disease. Little is known about the effect of this on hospitalisations for UC, including acute severe ulcerative colitis (ASUC). This study evaluated demographic trends of ASUC admissions in a metropolitan healthcare setting with an expanding culturally and linguistically diverse (CALD) population, with admission outcomes compared.
Methods: Demographic and disease characteristics of patients admitted with ASUC at a single tertiary metropolitan centre from January 2016 to December 2023 were recorded. Trends in presentation and outcomes in ASUC patients of Caucasian/European and non-Caucasian/European background were compared. Statistical significance between groups was determined using Mann-Whitney U tests and Pearson Chi-Square tests.
Results: During this 8-year period, 167 patients (70 [41.9%] female, median age 39 [range 19-93] years) were admitted for a total of 209 admissions. Of index admissions, 113 (67.7%) met Truelove and Witts criteria for ASUC. Admissions increased over time, from 8 patients in 2016 to 41 patients in 2021, and stabilisation to 34 patients in 2023. The ethnicity of patients with severe UC admissions was 48.5% Caucasian/European, 16.1% South Asian, and 14.4% Middle Eastern; ethnicity information was not available for 13.2% of patients. Of patients with recorded ethnicity, when comparing presentations in 2016-2019 to 2020-2023, there was a statistically significant increase in the proportion of non-Caucasian/European patients, increasing from 35.6% to 52.1% (p=0.046). In ASUC patients, 55.4% of Caucasian/European patients required infliximab rescue therapy, compared with 41.0% of non-Caucasian/European (p=0.169). Median length of stay was 6 days (IQR=3-11) in Caucasian/European patients compared with 5 days (IQR=4-7) (p=0.363) in non-Caucasian/European patients. 9.8% patients of Caucasian/European background required inpatient colectomy, compared with 5.4% of non-Caucasian/European background (p=0.486).
313
Intestinal ultrasound in immune checkpoint inhibitor-related colitis
Hiu Ching Letisia Sin1,2,5, Brandon Baraty1,2,3,4,5, Victoria Li2, Simon Ghaly1,2,5 and Craig Haifer1,2,5
1St Vincent's Hospital, Sydney, Australia;2University of New South Wales, Sydney, Australia;3Ryde Hospital, Sydney, Australia;4Macquarie University Hospital, Sydney, Australia;5Australian Gastroenterology Network of Intestinal Ultrasound (GENIUS), Sydney, Australia
Background and Aim: Immune checkpoint inhibitors (ICIs) have revolutionised cancer therapy. However, associated immune-related adverse events (irAEs) including ICI-colitis have posed a unique diagnostic and management challenge. Investigation and management of ICI-colitis requires repeated endoscopic evaluation, posing a significant burden on already comorbid patients. As the incidence of this condition grows, there is an increasing need for readily available, non-invasive assessments. Intestinal ultrasound (IUS) represents an excellent point-of-care option that is already well-validated in inflammatory bowel disease management. Our study aims to evaluate IUS in the investigation and monitoring of ICI-colitis, compared with clinical, endoscopic, and histologic findings, and other non-invasive biomarkers (faecal calprotectin (FCP) and serum C-reactive protein (CRP)).
Methods: We performed a retrospective review of patients with ICI-colitis referred to a tertiary care gastroenterology unit, between February 2023 and May 2024, that had undergone at least 1 IUS. Clinical data including disease severity (Common Terminology Criteria for Adverse Events (CTCAE) v5.0 criteria), biomarkers including CRP and FCP, and endoscopic data were analysed where available. All ultrasounds were undertaken by accredited gastroenterologists, and central reading was performed.
Results: A total of 32 scans were performed across 13 patients. 25 scans had corresponding FCP, and 30 had corresponding CRP levels. Only 9 scans had corresponding endoscopic investigations. 50% of patients were on steroids at the time of IUS, and 22% were on biologics. BWT ≥3mm was identified in 87% of scans that were performed whilst patients were symptomatic (CTCAE ≥1), and 100% of patients with more severe clinical phenotypes (CTCAE 3-4) demonstrated BWT ≥3mm. colour Doppler activity was appreciated in 80% of patients with the most severe phenotype (CTCAE 4). Amongst patients who had symptom resolution, follow-up scans demonstrated improvement of BWT to <3mm in 60% of patients, and 100% had resolution in colour Doppler activity. A moderately positive correlation was found between BWT and CRP (r=0.53, p=0.01) as well as a positive trend between BWT and FCP that did not meet statistical significance (r=0.47, p=0.07). For patients that had endoscopic procedures, BWT strongly correlated with the degree of endoscopic inflammation (Ulcerative Colitis Endoscopic Index of Severity (UCEIS) score; r=0.77, p=0.03).
Conclusions: In patients with clinically active ICI-colitis, significant IUS changes of increased BWT and/or colour Doppler signal were commonly seen, which normalised with symptom resolution. BWT was positively correlated with endoscopic activity and CRP, with a trend towards positive correlation with FCP. Our findings suggest that IUS may be a useful investigative and monitoring modality for management of ICI-colitis. This study will form the basis of a larger prospective study assessing the utility of IUS in the investigation and management of patients with ICI-colitis.
315
Granulomatous cholecystitis in Crohn’s disease with primary sclerosing cholangitis: A case report
Mohamed Reffai Syed Mohamed1, Babak Sarraf1, Peter Kanowski2 and Christine Welch1
1Townsville University Hospital, Townsville, Australia;2Sullivan Nicolaides Pathology, Townsville, Australia
Introduction: Crohn’s Disease (CD) is a chronic inflammatory condition, which predominantly affects the small and large bowel though not limited to it. CD related gallbladder complications commonly include gallstone formation and cholecystitis. Direct CD-related gallbladder inflammation is very rare and histological features of CD in the gallbladder is similarly uncommon. We present a case of 82-year-old female, who presents with unusual presentation of CD and primary sclerosing cholangitis (PSC) without established inflammatory bowel disease.
Case Report: An asymptomatic 82-year-old female was referred for investigation of anaemia (initially referred as iron deficiency). No cause was found on endoscopic evaluation. Anaemia persisted despite replete iron stores. Subsequent haematological investigations including bone marrow aspirate suggested anaemia of chronic disease. Liver enzymes were mildly cholestatic and ultrasound showed thickened gallbladder wall (Figure 1). Magnetic resonance cholangiopancreatography (MRCP) showed cholelithiasis, gallbladder thickening and possible changes of cholangitis/biliopathy. A cholecystectomy was performed, intra-operative findings showing a thickened gallbladder with fibrosis. Histopathology of the gallbladder showed active inflammation with granulomatous changes and focal surface ulceration resembling CD. IgG4 stains were negative. Serum Anti-Saccharomyces Cerevisiae Antibodies (ASCA) IgG was significantly elevated (117 U/mL, normal <10). The anaemia improved post cholecystectomy, however, liver enzymes became increasingly cholestatic. MRCP two years later showed progressive biliary beading and stricturing, with a diagnosis of likely PSC (Figure 2).
Conclusion: Isolated involvement of the gallbladder in CD as seen in this case is rare with a retrospective study of gallbladder histology in patients with CD finding little difference from the general population. It is well established that PSC and IBD are commonly seen together, with 60-80% of patients with PSC having coexistent IBD. Our patient was initially diagnosed with CD (the only manifestation of which was in the GB) and subsequently developed PSC. To our knowledge, this is the first reported case of PSC presenting in a patient with Crohn’s Cholecystitis.
319
Microbial signatures associated with inflammatory bowel disease in Australia: baseline sequencing from the Australian IBD Microbiome study
Thisun Jayawardana1, Robert Little2,3, Fan Zhang1, Sabrina Koentgen1, Nan Wu1, Paris Tavakoli1,4, Andrew Chung1, Anson Ho1, Alex Boussioutas2,3, Mark Ward2,3, Miles P Sparrow2,3, Peter Gibson3, Simon Ghaly1,4, Crispin Corte5, Nick J Talley6,12, Steven Leach1,7, Shoma Dutt8, Avi Lemberg1,7, Sudarshan Paramsothy9, Rupert Leong9, Susan J Connor1,10 and Georgina Hold1,11
1UNSW, Sydney, Australia;2Alfred Health, Melbourne, Australia;3Monash University, Melbourne, Australia;4St Vincents Hospital Network, Sydney, Australia;5Royal Prince Alfred Hospital, Sydney, Australia;6University of Newcastle, Newcastle, Australia;7Sydney Children's Hospital Randwick, Sydney, Australia;8Westmead Children's Hospital, Sydney, Australia;9Concord Repatriation General Hospital, Sydney, Australia;10Liverpool Hospital, Sydney, Australia;11Ingham Institute, Sydney, Australia;12John Hunter Hospital, Newcastle, Australia
Background and Aim: Microbial dysbiosis is associated with Crohn’s disease (CD) and ulcerative colitis (UC) onset and disease activity, however, large-scale data pertaining to Australian patients are limited. Characterising the gut microbial composition in an Australian population is important to understand the impact of a unique combination of environmental exposures. This study aimed to describe the differences in gut microbiota composition between patients with IBD and healthy controls within the Australian IBD Microbiome (AIM) study.
Methods: Paired faecal and oral samples alongside participant demographic and disease characteristics were collected at baseline from the first 1000 participants enrolled in the AIM study from June 2019 to November 2023. Participants were divided into three groups: CD, UC, healthy controls (HC). Faecal and oral samples were self-collected in DNA stabilising buffer, aliquoted and stored at -80oC until extraction. Samples underwent 16S rRNA sequencing with annotation of DNA sequences to operational taxonomic units at the genus level. Differences in alpha diversity (Shannon index) and relative abundance of identified genera between the three groups were assessed using Kruskal-Wallis or Mann-Whitney U tests. Beta diversity (Bray-Curtis dissimilarity) between bacterial communities were shown using the Principal Coordinate Analysis (PCoA), and the significance of variance was tested using ADONIS within R.
Results: 908 participants (302 CD, 261 UC, 345 HC) returned baseline faecal (n = 703) and/or oral samples (n = 743) and were included in the analysis. Mean age was 43 years (SD 15), mean BMI 26 kg/m2 (SD 5.3), 59% were female and the median faecal calprotectin (FCP) was 20 ug/g (IQR 15-56) across the entire cohort. In the CD cohort, median CDAI was 79 (IQR 36-159) and FCP 37.1 ug/mg (IQR 20-149). In the UC cohort, the median partial Mayo was 1 (IQR 0-2) and FCP 35.9 (IQR 20-182). CD and UC patients had comparable and lower alpha diversity than the HC group (p <0.0001; Figure 1A). Beta diversity was different between CD, UC and HC groups (p < 0.001; Figure 1B). There were five phyla with significantly different relative abundances between the three groups with broad depletion of ‘healthy’ commensals and expansion of traditionally pro-inflammatory taxa (p <0.05, Figure 1C). No significant inter-group differences were seen with oral microbial analysis.
320
Impaired health-related quality of life is associated with alterations in gut microbiota in patients with inflammatory bowel disease: baseline sequencing from the Australian IBD Microbiome study
Thisun Jayawardana1, Robert Little2,3, Fan Zhang1, Sabrina Koentgen1, Nan Wu1, Paris Tavakoli1,4, Andrew Chung1, Anson Ho1, Alex Boussioutas2,3, Mark Ward2,3, Miles P Sparrow2,3, Peter Gibson3, Simon Ghaly1,4, Crispin Corte5, Nick J Talley6,7, Steven Leach1,8, Shoma Dutt9, Avi Lemberg1,8, Sudarshan Paramsothy10, Susan J Connor1,11,12, Rupert Leong10 and Georgina Hold1
1UNSW, Sydney, Australia;2Alfred Health, Melbourne, Australia;3Monash University, Melbourne, Australia;4St Vincent's Hospital, Sydney, Australia;5Royal Prince Alfred Hospital, Sydney, Australia;6University of Newcastle, Newcastle, Australia;7John Hunter Hospital, Newcastle, Australia;8Sydney Children's Hospital at Randwick, Sydney, Australia;9Westmead Children's Hospital, Sydney, Australia;10Concord Repatriation General Hospital, Sydney, Australia;11Liverpool Hospital, Sydney, Australia;12Ingham Institute, Sydney, Australia
Background and Aim: Inflammatory Bowel Disease (IBD) activity as well as disease monitoring and intervention have a substantial impact on the quality of life (QoL) of IBD patients. In addition to luminal and extra-intestinal manifestations, patients frequently report adverse social, employment and psychological outcomes. Changes in the gut microbiota are associated with IBD onset and activity and have also been implicated in modifying health-related QoL (HRQoL) across a range of conditions. This study aimed to investigate the association between HRQoL and gut microbial composition in IBD patients using the 32-item Inflammatory Bowel Disease Questionnaire (IBDQ-32).
Methods: Paired faecal and oral samples alongside participant demographics, disease characteristics and the IBDQ-32 survey were collected at baseline from all patients with IBD enrolled in the Australian IBD Microbiome (AIM) study from June 2019 to November 2023. IBDQ-32 scores range from 32 to 224, with a higher score indicating better HRQoL. Patients were divided into two groups: impaired HRQoL (cumulative score <170) and preserved HRQoL (>170). Faecal and oral samples were self-collected in DNA stabilising buffer, aliquoted and stored at -80oC until extraction. Samples underwent 16S rRNA sequencing with annotation of DNA sequences to operational taxonomic units at the genus level. Differences in alpha diversity (Chao1, ACE, Shannon index) and relative abundance of identified genera between groups were assessed using Kruskal-Wallis or Mann-Whitney U tests. Beta diversity (Bray-Curtis dissimilarity) in bacterial communities were shown using Principal Coordinate Analysis (PCoA), and significance of variance tested using R.Results: 563 participants (302 CD, 261 UC) returned baseline faecal (n = 407) and/or oral samples (n = 436) and were included in the analysis. Mean age was 43 years (SD 15), mean disease duration 11 years (SD 11), mean BMI 26 kg/m2 (SD 5.4), 58% were female, 14% were smokers, 349/555 (63%) were in clinical remission and the median FCP was 37 ug/mg (IQR 20-167). The median cumulative IBDQ-32 score was 180 (IQR 150-197). 191/483 (40%) of patients were defined as having impaired HRQoL with no difference between CD and UC patients and 47% of these patients were in clinical remission. Patients with impaired HRQoL had lower faecal microbial alpha diversity on two of three measured indices (Figure 1A-C) but comparable beta diversity to patients with preserved HRQoL. There were no differences in alpha or beta diversity in oral samples and no significant differences in relative abundance of phyla according to HRQoL status in either faecal or oral samples. However, on analysis at the genus level, there were 38 and 11 genera with significantly different relative abundances between HRQoL groups in the faecal and oral samples, respectively.
329
Monocyte distribution width: a biomarker that differentiates bacterial gastroenteritis from acute severe ulcerative colitis in patients presenting with diarrhoea
Christopher Li Wai Suen1,2,4, Shipraa Kaul1, Ethan Tan1, Danny Con1,2, Michelle Taylor3, Joanne Wiid3, Chris Hogan3, Matthew Choy1,2, Kumar Visvanathan2,4 and Peter De Cruz1,2
1Department of Gastroenterology, Austin Health, Melbourne, Australia;2Department of Medicine, University of Melbourne, Melbourne, Australia;3Department of Laboratory Haematology, Austin Health, Melbourne, Australia;4Immunology Research Centre, St Vincent’s Hospital Melbourne, Melbourne, Australia
Background and Aims: Monocyte distribution width (MDW) is a haematological parameter that can be generated by newer generation blood analysers on routine full blood examination. It reflects the variation in the size of monocytes and is elevated in the setting of infection. The utility of MDW in inflammatory disorders is however unknown. We aimed to assess whether MDW can help differentiate bacterial gastroenteritis from Acute Severe Ulcerative Colitis (ASUC) among patients presenting to the Emergency Department (ED) with diarrhoea. We further aimed to assess whether MDW correlated with disease activity and clinical outcomes in ASUC.
Methods: We conducted a retrospective cohort study comprising three patient groups: (1) ASUC, (2) bacterial gastroenteritis and (3) a control group of patients without active inflammation. The control group consisted of outpatients with chronic hepatitis B in immune control phase with normal liver transaminases and suppressed viral load < 2000 IU/mL. Clinical outcomes, routine biomarkers and MDW were recorded.
Results: A total of 176 patients were identified (53 ASUC, 70 bacterial gastroenteritis and 53 controls). At time of ED presentation, patients with bacterial gastroenteritis had the highest MDW (median 23.6, interquartile range [IQR] 20.7-25.8) compared to ASUC (19.0, IQR 17.9-21.2) and controls (16.8, IQR 15.9-18.0; P<0.001). On receiver operator characteristic curve analysis, MDW discriminated bacterial gastroenteritis from ASUC with an area under the curve (AUC) of 0.78 (95% confidence interval [CI] 0.70-0.87, P<0.001). Using Youden’s index, a MDW threshold ≥ 22.3 had 64.3% sensitivity, 84.6% specificity, 63.8% negative predictive value and 84.9% positive predictive value for bacterial gastroenteritis. Of the 53 patients with ASUC, 25 responded to intravenous hydrocortisone while 28 were steroid non-responders and required infliximab (IFX). 24 patients responded to IFX rescue, while the 4 IFX non-responders received tofacitinib sequential therapy. In ASUC, MDW correlated positively with established markers of disease activity including CRP (Spearman rank correlation, rho=0.54, P<0.001), platelet count (rho=0.36, P=0.009) and faecal calprotectin (rho=0.35, P=0.02). A lower MDW on the day of IFX administration appeared to predict IFX response (AUC 0.80, 95% CI 0.61-1.00, P=0.002). At follow-up (median 85 days), MDW was predictive of biochemical remission with a faecal calprotectin < 100 μg/g (AUC 0.80, 95% CI 0.64-0.95, P<0.001).
Conclusion: MDW is a novel biomarker that may help distinguish ASUC from bacterial gastroenteritis at time of ED presentation in patients with diarrhoea. In ASUC, MDW correlates with existing markers of activity and may help predict response to IFX.
331
Real world population-based effectiveness of tofacitinib versus monoclonal antibodies in ulcerative colitis: Data from the Persistence Australian National IBD Cohort (PANIC5)
Rupert Leong1,2,3, Yunki Yau1,2, John Chetwood1,2, Thanaboon Chaemsupaphan1,2, Viraj Kariyawasam3, Sudarshan Paramsothy1,2,3 and Aviv Pudipeddi1,2
1Concord Repatriation General Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3Macquarie University Hospital, Sydney, Australia
Background and Aim: Janus kinase inhibitors (JAKi) exhibit distinct performance characteristics versus monoclonal antibody (mABs) biological agents in the management of ulcerative colitis (UC). Treatment persistence serves as an indicator of sustained real-world therapeutic effectiveness. Currently, there is a lack of direct comparative effectiveness data of JAKi small molecules versus mABs. We, therefore, aimed to determine the persistence of tofacitinib (TOF) versus vedolizumab and tumour necrosis factor inhibitor (TNFi) mABs in advanced therapy (AT)-naïve and AT-exposed real-world UC subjects.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC5) registry of all UC subjects on PBS AT up until Dec 2021. PANIC5 collected 100% of all AT prescribing data at a population-level. Non-persistence was defined as failure to continue AT prescriptions for >6-months. Kaplan-Meier survival curves were generated for AT persistence and compared using the log-rank test. Cox proportional hazards regression models were employed to calculate hazard ratios (HR) and 95% confidence intervals (CI) with P<0.05 deemed statistically significant SPSS (IBM, USA).
Results: A total of 9,671 consecutive UC patients (52.9% male) were recruited, providing 23,220 patient-years of prospective follow-up. The cohort comprised 14,798 treatment lines: 6,047 infliximab (IFX), 1,982 adalimumab (ADA), 5,481 vedolizumab (VED), 750 golimumab (GOL) and 538 tofacitinib (TOF). TOF exhibited superior persistence versus mABs overall (HR: 1.70, 95%CI: 1.22-2.37, P=0.002), especially in AT-exposed subjects (HR: 2.54, 95%CI: 1.76-3.68, P<0.001) but not AT-naïve subjects (HR: 1.23, 95%CI: 0.55-2.74, P=0.62). TOF exhibited superior persistence versus VED in AT-exposed subjects (HR: 2.01, 95%CI: 1.38-2.94, P<0.001) but not in AT-naïve subjects (HR: 0.67, 95%CI: 0.30-1.50, P=0.33). TOF exhibited superior persistence versus TNFi in AT-exposed subjects (HR: 3.02, 95%CI: 2.08-4.38, P<0.001) but not in AT-naïve subjects (HR: 1.53, 95%CI: 0.69-3.42, P=0.30). The persistence of TOF (P=0.78) did not significantly decline from AT-naive- to AT-exposed treatment status, unlike TNFi and VED (both P<0.001; Figure).
333
Upadacitinib maintains hidradenitis suppurativa remission in patient with ulcerative colitis
Introduction: Hidradenitis suppurativa (HS) is a chronic inflammatory disease of skin follicles thought to have a significant overlap with inflammatory bowel disease (IBD). Upadacitinib, a selective Janus kinase 1 inhibitor, is a small-molecule advanced therapy approved for use in ulcerative colitis (UC). While it is well documented that HS responds to anti-tumour necrosis factor blocker (anti-TNF) adalimumab, a monoclonal antibody used to manage IBD, there is limited clinical evidence that upadacitinib may treat HS. HS clinical response rate (HiSCR), a commonly utilised endpoint in management of HS, is defined as a ≥50% reduction in inflammatory lesion count and no increase in abscesses or draining fistulas. We report a case of a patient with UC and concomitant HS, who failed to respond to multiple advanced therapies and then completely responded to upadacitinib, achieving both UC remission and maintaining HiSCR.
Case report: A 29-year-old woman was diagnosed with UC in early 2020. Her comorbidities include HS, acne, obesity (BMI 40), and polycystic ovarian syndrome. The patient was initially managed with oral and topical mesalazine, tapering corticosteroids, and azathioprine. Acute severe flare in December 2020 necessitated rescue and maintenance infliximab, which was discontinued after 6 months due to antibody development and side effects. Vedolizumab was commenced and discontinued 13 months later due to loss of response. The patient initially responded to adalimumab in September 2022 until an acute flare in July 2023. Finally, upadacitinib was initiated, leading to excellent clinical, biochemical, and endoscopic response. During these tumultuous 3 years the patient was also followed in a dermatology clinic for a facial rash, rosacea and HS. HS was initially classified as a Hurley stage 3 (severe). Several therapies, including spironolactone were attempted with limited effect. HS improved significantly when the patient had been commenced on adalimumab, achieving HiSCR. After initiation of upadacitinib, it was noted that HS initially aggravated with a single nodule appearing at the right breast, however this was linked to a commencement of isotretinoin for acne and rapidly improved afterwards. At present, 44 weeks into the upadacitinib treatment, the patient’s HS remains in clinical remission.
Conclusion: This case highlights the potential use of upadacitinib in maintaining remission of HS in a patient with ulcerative colitis. As the evidence on the upadacitinib effect on extraintestinal and dermatological manifestations of IBD is still limited, this case may inform the choice of a biologic therapy for IBD management in patients with concomitant HS.
334
Switching to ustekinumab versus vedolizumab following first-line treatment failure of tumour necrosis factor inhibitors in Crohn’s disease: Data from the Persistence Australian National IBD Cohort (PANIC5)
Rupert Leong1,2,3, John Chetwood1,2, Thanaboon Chaemsupaphan1,2, Fei Pan3, Aviv Pudipeddi1,2, Sudarshan Paramsothy1,2,3 and Viraj Kariyawasam3
1Concord Repatriation General Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3Macquarie University Hospital, Sydney, Australia
Background and Aim: Tumour necrosis factor inhibitors (TNFi) are the most prescribed advanced therapy (AT) class in Crohn’s disease (CD). Prescribers face uncertainty, however, when TNFi fails whether to switch to ustekinumab (UST), vedolizumab (VED), or to another TNFi. Persistence serves as an indicator of sustained real-world therapeutic effectiveness and may guide the selection of the second-line AT. We, therefore, aimed to determine the persistence of second-line AT following TNFi, UST, and VED first-line non-persistence in CD patients.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC5) registry of CD subjects up until Dec 2021. The PANIC5 registry includes 100% of all AT prescribing data in Australia. Non-persistence was defined as failure to dispense AT prescriptions for >6-months. Kaplan-Meier survival curves were generated for AT persistence and compared using the log-rank test. Cox proportional hazards regression models were employed to calculate hazard ratios (HR) and 95% confidence intervals (CI) with P<0.05 deemed statistically significant SPSS (IBM, USA).
Results: Of the 19,087 unselected CD patients, 15,708 commenced first-line TNFi. Among these, 5,851 (37.2%) switched to another drug after a median time of 14 months (IQR: 6-33) to UST (n=1,872), VED (n=893) or another TNFi (n=3,086). Median persistence of second-line AT was 11 months (IQR: 4-25). Second-line UST had significantly higher persistence versus second-line VED (HR: 1.73, 95%CI: 1.51-1.97, P<0.001), and second-line TNFi (HR: 1.87, 95%CI: 1.68-2.07, P<0.001). Second-line TNFi versus VED revealed no statistically significant difference in persistence (HR: 0.93, 95%CI: 0.83-1.03, P=0.15). Of the 2,209 CD subjects that commenced first-line UST, 206 (9.3%) switched to a second-line AT after a median of 8 months (IQR: 4-15). There was no significant difference in persistence to second-line VED (n=44) versus TNFi (n=162) after first-line UST non-persistence (P=0.98). Of the 1,159 CD subjects that commenced first-line VED, 249 (21.5%) switched to a second-line AT after a median of 10 months (IQR: 6-18.5). There was no significant difference in persistence to second-line UST (n=112) versus TNFi (n=137) after first-line VED non-persistence (P=0.16).
335
Video vision transformer for quantification of ulcerative colitis endoscopic and histologic disease activity
Savannah Morrison1,2, Chris Chiu3, Rena Cao1, Crispin Corte1,3, Peter Lim1,3, Joo Shin1, Catriona Mckenzie1, James Kench1 and Aravind Gokul Tamilarasan1,3
1Royal Prince Alfred Hospital, Sydney, Australia;2University of Newcastle, Newcastle, Australia;3University of Sydney, Sydney, Australia
Background and Aim: There is considerable inter-user variability in endoscopic and histologic scoring of the severity of ulcerative colitis (UC)1. The aim of this study was to create and train an artificial intelligence algorithm to predict the severity of UC using endoscopic videos.
Methods: This prospective cohort study recruited UC patients undergoing flexible sigmoidoscopy or colonoscopy between October 2023 and May 2024. The endoscopic examination was recorded from the splenic flexure to the anus, with IBD-experienced readers determining unique endoscopic Mayo Scores (eMS) of the left colon and rectum. Biopsies were given histological Nancy scores2 by gastrointestinal histopathologists. The videos were segmented into 3 second tubelets, and poor quality videos excluded. The dataset was divided into a training/test dataset (90/10), grouped by patient and stratified by disease class. Two video vision transformer models were trained to recognise Mayo and Nancy Scores respectively, and their performance in predicting disease activity, and accuracy in determining severity scores was evaluated. Standard diagnostic accuracy measures were used to calculate the models’ ability to detect and quantitate UC disease activity and included area under the receiver-operator curve, accuracy, sensitivity, specificity, and precision.
Results: 29 patients were recruited; 3 patients were excluded due to poor bowel preparation, or failure of recording. 15 patients had histological activity, and the resultant Mayo and Nancy scores showed moderate correlation (R=0.66). 2408 video tubelets were derived from the patient dataset after filtering. The mean time taken for end-to-end prediction of disease activity was 0.77s. For Mayo scoring, the model had an AUROC of 0.943 in identifying disease activity, with accuracy, sensitivity, specificity, and precision at 88.5%, 86.3%, 92.2%, 93.6% respectively. Multiclass performance accuracy was at 87.0%, with a macro F1 score of 0.87. For Nancy scoring, the resultant model was less robust but retained moderate to high accuracy and sensitivity at the cost of specificity: AUROC of 0.917 in identifying disease activity (Nancy score ≥1), and accuracy, sensitivity, specificity, precision at 89.4%, 92.2%, 78.6%, 96.4% respectively. Multiclass performance was at 88.4%, with a macro F1 score of 0.83.
Conclusion: Our results demonstrated the ability of video models to quantify ulcerative colitis endoscopic and histologic disease activity with high levels of accuracy. Our small sample size limited the model performance, and further refining of the training videos will see further improvements in diagnostic accuracy, with potential for future real-world application as an adjunct to human interpretation, with cost and time saving capacity.
References
1. Hashash JG, et al. Inter- and Intraobserver Variability on Endoscopic Scoring Systems in Crohn's Disease and Ulcerative Colitis: A Systematic Review and Meta-Analysis. Inflamm Bowel Dis. 2024:izae051. doi: 10.1093/ibd/izae051.
2. Marchal-Bressenot A, et al. Development and validation of the Nancy histological index for UC. Gut 2017;66:43–49.
343
Student led interdisciplinary clinics can provide comprehensive nutrition, sarcopenia and mental health risk screening for patients with inflammatory bowel disease
Samantha Plush1,2,3, Robert Bryant1,2,3, Saravana Kumar4 and Alice Day1,2,3
1The Department of Gastroenterology and Hepatology, The Queen Elizabeth Hospital, Adelaide, Australia;2The School of Medicine, University of Adelaide, Adelaide, Australia;3The Basil Hetzel Institute, Adelaide, Australia;4Allied Health and Health Services, University of South Australia, Adelaide, Australia
Background and Aim: Undernutrition, sarcopenia, and poor mental health are common in inflammatory bowel disease (IBD) affecting quality of life. Despite high prevalence, these co-morbidities are under-recognised due to lack of service capacity. Students may enable workforce capacity providing valuable interdisciplinary screening and care planning for patients, whilst also developing the students’ interdisciplinary practice skills. This study aimed to determine benefit of a student led interdisciplinary screening clinic to diagnose patient risk whilst meeting student learning objectives.
Methods: Eighteen final year dietetic, physiotherapy or exercise physiology students conducted 5-10 weekly half day interdisciplinary outpatient clinics within a tertiary IBD service between July and October 2023. Following training, students completed all aspects of the interdisciplinary consult under supervision. Risk screening assessments comprised of anthropometrics, depression anxiety and stress scale-21 (DASS-21), subjective global assessment (SGA), short physical performance battery (SPPB), handgrip strength (HGS) and inflammatory bowel disease-nutrition screening tool (IBD-NST). Consecutive patients attending a tertiary IBD outpatient gastroenterology appointment were contacted to participate in the clinic. Descriptive statistics were completed, and prevalence is presented as number (n) and percentage.
Conclusion: A student-led interdisciplinary screening clinic ensures timely identification of patient risk for undernutrition, sarcopenia, and poor mental health, improving access to early intervention opportunities. Students can act as a valuable enabler for workforce capacity whilst developing valuable skills in interdisciplinary practice.
348
Dietary emulsifiers might improve rather than be detrimental to outcomes in patients with active Crohn’s disease: a pilot randomised, double-blind feeding study
Jessica Fitzpatrick1,2, Peter Gibson1, Kirstin M Taylor1 and Emma Halmos1
1Department of Gastroenterology, School of Translational Medicine, Monash University, Melbourne, Australia;2Alfred Health, Melbourne, Australia
Background: Specific dietary emulsifiers have been implicated in the pathogenesis of Crohn’s disease (CD) on the basis of: (1) Preclinical studies, where high doses of specific emulsifiers reduce intestinal mucus thickness, increase bacterial expression of flagellin, impair intestinal barrier function and drive gastrointestinal inflammation in genetically susceptible mice; (2) Prospective cohort studies, where high intake of ultra-processed foods (usually high in emulsifier content) is associated with increased risk of developing CD; (3) Dietary intake studies, where Australian patients with CD eat more emulsifiers than do healthy controls; and (4) Intervention study in healthy adults, where high emulsifier intake reduced unstressed, but increased stress-induced intestinal permeability.
Aim: To perform a pilot proof-of-concept study to determine whether these data translate into detrimental effects of high intake of emulsifiers in patients with CD by comparing diets differing only in emulsifier content on clinical and inflammatory disease activity and intestinal permeability in patients with active CD in a double-blinded randomised controlled feeding trial.
Methods: Patients, who had active disease and were on stable medical therapy for at least 2 months prior with no exposure to steroids and antibiotics in the preceding 4 and 2 weeks, respectively, were recruited from public and private healthcare settings in Victoria. Patients who had active disease on the basis of endoscopy, imaging and/or faecal calprotectin >250 μg/g, an abnormal Harvey Bradshaw Index (HBI) (≥5), ileal involvement and sonographically visible disease were randomised to receive 4 weeks of previously characterised high emulsifier (HED) or low emulsifier (LED) diets. All food was provided. Measures taken at day 0 and day 28 included bowel wall thickness (BWT) and hyperaemia of the worst affected segment on intestinal ultrasound (IUS), HBI, biochemistry and intestinal permeability assessed by a dual-sugar test providing a 2-h urinary lactulose:rhamnose ratio (LRR). Sonographic response was defined as: ≥2 mm reduction in BWT, or ≥1 mm reduction with reduction in hyperaemia, or BWT reduction by ≥25%. Dietary adherence (% consumption of provided food) was assessed via food diaries. Data were analysed per protocol. Data presented as mean (95% confidence interval), or median (interquartile range), depending on distribution.
Results: 24 patients, mean 37 (32-42) years old, 54% female, were randomised and 19 completed (9 HED, 10 LED) the interventions. The 5 who withdrew prematurely (3 HED, 2 LED) due to worsening gastrointestinal symptoms (one requiring a hospital admission) had baseline highly sensitive C-reactive protein (hCRP) mean 10.2 (0 – 21.0) mg/L compared with 2.3 (1.4-3.3) mg/L in those completing the diet (p=0.001). Adherence to both diets was excellent. At day 0, sonographic findings were similar between cohorts (BWT; p=0.84; Figure 1). As shown in Figure 1, BWT decreased on both diets, but was lower on day 28 following HED compared with LED (p=0.044). Sonographic response in LED was seen in 50% (5/10) and in HED in 89% (8/9) (p=0.149). There were no differences in hCRP between diets at baseline or at the end of the study, and no change during the diet. From baseline, HBI reduced on LED [median 6 (IQR 5-7) to 3 (0-6) p=0.012] and HED [6 (5-7) to 1 (1-3) p=0.004], with no differences between diets. Intestinal permeability was similar between the groups at baseline, but, at the end of study, was mean 0.029 (0.013 – 0.045) with HED, which was lower than 0.066(0.036 – 0.097) with LED (p=0.029).
Conclusion: Both diets were associated with improvement of intestinal inflammation, but the HED was associated with a greater improvement in some indices of intestinal inflammation and in small intestinal permeability (as previously shown in healthy subjects). A detrimental effect of a diet high in emulsifiers as predicted from preclinical studies was not observed, questioning the demonisation of dietary emulsifiers in patients CD. Large scale studies are warranted.
355
Tofacitinib demonstrates preliminary efficacy in induction of remission in chronic pouchitis
Emi Khoo1,2,3, Anna Amiss4, Niamh Lindsay2, Richard Fernandes1,2,3, Robert Gilmore1,2, John Nik Ding5, Susan J Connor6, Robert Bryant7, Lauren White8, Waled Mohsen9, Rupert Leong10, Zaid Ardalan11, Anthony Croft12, Peter De Cruz13, Kate Lynch14, Yoon-kyo An1,2,3, Gerald Holtmann15 and Jakob Begun1,2,3
1Mater Hospital Brisbane, Brisbane, Australia;2Mater Research Institute, Brisbane, Australia;3University of Queensland, Brisbane, Australia;4Translational Research Institute, Brisbane, Australia;5St Vincent's Hospital Melbourne, Melbourne, Australia;6Liverpool Hospital, Liverpool, Sydney, Australia;7Queen Elizabeth Hospital, Adelaide, Australia;8Sunshine Coast University Hospital, Birtinya, Australia;9Gold Coast University Hospital, SouthPort, Australia;10Macquarie University Hospital, Macquarie University, Australia;11Alfred Hospital, Melbourne, Australia;12Royal Brisbane and Women's Hospital, Brisbane, Australia;13Austin Hospital, Melbourne, Australia;14Royal Adelaide Hospital, Adelaide, Australia;15Princess Alexandra Hospital, Brisbane, Australia
Background: Pouchitis is common following total proctocolectomy for ulcerative colitis (UC) and ileal pouch-anal anastomosis (IPAA) and generally responds to antibiotics. However, up to 20% of patients develop either antibiotic-dependent or antibiotic-refractory pouchitis, collectively referred to as chronic pouchitis.
Methods: We report our preliminary induction results from a multi-center open label induction with randomized withdrawal trial to assess the efficacy of tofacitinib in chronic pouchitis. All eligible participants received 10 mg tofacitinib twice daily for 8 weeks, with an additional 8 weeks of therapy given to patients with an inadequate initial clinical response. The primary endpoint was clinical response (a reduction of clinical PDAI≥2 points) at week 8. Secondary endpoints included endoscopic response (a reduction of endoscopic PDAI≥2), mPDAI remission (modified pouchitis disease activity index (mPDAI)≤4 and a reduction of mPDAI≥2), mPDAI response (a reduction of mPDAI≥2) and improvement in health-related quality of life (HRQoL) using the short inflammatory bowel disease questionnaire (SIBDQ). Serum cytokine levels were analyzed using LEGENDplex human inflammation panel 1. Univariate analysis was performed to identify clinical and biochemical predictors of response to tofacitinib.
Results: A total of 42 patients with chronic pouchitis (Table 1) were included in the preliminary analysis. The clinical and endoscopic response rates at week 8 were 50% and 55% respectively (Figure 1a). The mPDAI remission rate was 41% at week 8 with an mPDAI response rate of 69% (Figure 1b). There was no significant difference in the response rates between vedolizumab exposed and vedolizumab naïve patients. There was significant improvement in HRQoL, with the median SIBDQ score increasing from 36 at baseline to 53 at week 8 (p<0.05) (Figure 1c). Nineteen patients received a further 8 weeks of therapy with a clinical response rate of 29%, yielding an overall response rate including extended induction of 64%. Univariate analysis did not reveal significant differences in baseline characteristics, clinical, or biochemical markers between responders and non-responders. However, antibiotic refractory disease, endoscopic friability, and mucous exudate on endoscopy were assocaited with treatment response (p<0.05). Elevated baseline serum levels of IL-1β, IFN-α and IL-33 were associated with endoscopic response at week 8 (p<0.05) (Figure 1d).
Conclusion: Tofacitinib demonstrated efficacy in inducing both clinical and endoscopic response in patients with chronic pouchitis who have undergone IPAA for UC. Tofacitinib was effective in patients previously exposed to vedolizumab for treatment of chronic pouchitis.
373
No relationship between positive anti-neutrophilic cytoplasmic antibody and small vessel vasculitis in children with inflammatory bowel disease
Fadia Alghzawi1,2, Rachel Horn1, Jason Yap1, Stephanie Richardson1, Colleen D’Arcy1, Jonathan Akikusa1 and Anson Ho1
1The Royal Children's Hospital, Melbourne, Australia;2The Hashemite University, Zarqa, Jordan
Background and Aim: Anti-neutrophilic cytoplasmic antibody (ANCA)-associated vasculitis (AAV), including granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis and microscopic polyangiitis are rare autoimmune conditions involving inflammation of blood vessels. AAV collectively formed the most common type of primary small-size vessel vasculitis (SVV). The development of SVV as an extra-intestinal manifestation in patients with inflammatory bowel disease (IBD), especially those with positive ANCA is not well described. This study aims to ascertain whether children with IBD, in particular those with positive ANCA developed SVV or AAV with their IBD diagnosis.
Methods: Children diagnosed with IBD between January 2016 and December 2021 in a tertiary hospital were retrospectively reviewed. The development of SSV before or after IBD diagnosis was identified from medical records until their most recent or last visit. A paediatric rheumatologist determined the final SVV/AAV diagnosis. The IBD diagnosis was made based on the European Society of Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) revised porto criteria.
Results: Two hundred and seventy-two patients with IBD (41.9% Crohn’s disease (CD), 33.1% ulcerative colitis (UC) and 25% IBD-Unclassified (IBD-U)) with a mean (± SD) age of 11.7 ± 3.6 years, 166 (61%) males and mean follow-up (± SD) of 40.1 ± 19.7 months were included. Among those with IBD-U, the treating physicians further classified this group into either favouring CD (15.8%) or UC (9.2%) phenotype. Of the 272 patients, 98 (36%) had ANCA positive (56.1% were perinuclear-ANCA, 28.6% cytoplasmic-ANCA and 15.3% atypical ANCA). The rest were 54 (19.9%) with indeterminate ANCA, 94 (34.6%) with ANCA negative and 26 (9.6%) were unknown. Among those with ANCA positive, 75 (76.5%) patients had UC, including those with IBD-U favouring UC and 23 (23.5%) patients had CD, including those with IBD-U favouring CD. Table 1 shows IBD disease location based on ANCA positive. Two patients (0.74%) with UC and ANCA positive (one cytoplasmic-ANCA and the other perinuclear-ANCA) were found to have cutaneous vasculitis and neither developed AAV during follow-up.
374
Predictors of long-term anti-TNF failure: A validation analysis via the prospective Persistence Australian National IBD Cohort (PANIC) Registry
John Chetwood1,2,3, Sudarshan Paramsothy1,2,4,5 and Rupert Leong1,2,4,5
1Concord Repatriation General Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3St Vincent's Hospital Melbourne, Melbourne, Australia;4Macquarie University Hospital, Sydney, Australia;5Macquarie University, Sydney, Australia
Background and Aim: There are limited data on factors that predict long-term anti-TNF treatment failure. A recent UK study (PANTS-E) of 1164 patients recently suggested female gender, thiopurine commencement before biological agent, and thiopurine dose quartile predicted failure with infliximab but not adalimumab in bio-naïve Crohn’s disease (BN CD). We sought to validate these findings in the Australian population.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC) registry for all patients on their 1st-line advanced therapy (AT) for IBD until Dec 2021, with a luminal CD indication. The PBS prospectively collects AT population-based prescribing data. Non-persistence was defined as failure to dispense AT prescriptions for >6 months. Corticosteroid-free persistence was defined as non-persistence or corticosteroid use after 3 months of initiation, whichever came first. Kaplan–Meier survival curves were generated for AT persistence and compared using the log-rank test.
Results: The study population comprised 15,672 patients with a median age of 36.9 years (IQR: 26.5-50.1), and 8,475 (54.1%) females, with 50,897 patient-years of follow-up. Female gender was adversely associated with overall persistence (OP) and corticosteroid-free persistence (CFP) persistence with both infliximab and adalimumab (all P<0.0001) in follow-up >10 years. Thiopurine co-use was protective for OP and CFP with adalimumab (P<0.0001 & P=0.0017), and OP but not CFP with infliximab (P=0.018 & P=0.26 respectively). Higher thiopurine dispensing quartile improved adalimumab persistence (P<0.0001 & P=0.0035 for OP and CFP respectively), and thiopurine commencement prior to biological agent induction compared to co-induction improved OP for adalimumab (P=0.0017) though not CFP (P=0.20). Conversely in the PANIC registry, neither affected infliximab outcomes (thiopurine dispensing quartile: P=0.93 and P=0.82 for OP and CFP respectively, thiopurine initiation timing: P=0.14 & P=0.96 for OP and CFP respectively). Independent predictors of both adalimumab and infliximab persistence were: age, gender, use of corticosteroids and immunomodulator co-therapy at induction (all P<0.05).
375
Ustekinumab and endoscopic balloon dilation is effective for stricturing Crohn’s disease: A dual-centre retrospective cohort study
John Chetwood1,2,3, Sri Selvaratnam4, Arteen Arzivian4, Pranita Dhanji1, Sudarshan Paramsothy1,2,4,5 and Rupert Leong1,2,4,5
1Concord Repatriation General Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3St Vincents Hospital Melbourne, Melbourne, Australia;4Macquarie University Hospital, Sydney, Australia;5Macquarie University, Sydney, Australia
Background and Aim: Symptomatic stricturing Crohn’s disease (CD) represents a challenging treatment cohort with a high proportion requiring surgery. Endoscopic balloon dilation (EBD) has shown promise in surgery-free management. There are limited data evaluating the performance of different medications combined with EBD, particularly for newer agents such as ustekinumab (UST).
Methods: We performed a dual-centre retrospective cohort study of all adult patients who underwent CD stricture dilation 2015-2023. Strictures were subclassified according to concomitant use of biological agent. Primary outcome was clinical success (1-year of surgery-free medication persistence without a requirement for repeat EBD). Secondary outcomes included short-term success (1-year of surgery-free medication persistence after the first (index) EBD), surgery-free medication persistence, and adverse events. Propensity-score matching was used to address baseline cohort imbalance.
Results: 525 dilations were performed on 199 strictures in 94 patients. Per intention-to-treat per stricture, medical therapies were: immunomodulator monotherapy (IMM) in 54/199 (27.1%), UST in 58/199 (29.1%), vedolizumab (VED) in 33/199 (16.6%) and tumour necrosis factor inhibitor (TNFi) in 54/199 (27.1%). UST was associated with a greater long-term and short-term clinical success rate versus TNFi (both P=0.03) and versus IMM (P=0.016 & P<0.001 respectively) and with greater longterm clinical success than VED (P=0.002) though equivalent short-term success (P=0.32). UST retained greatest long-term success vs TNFi and IMM in the subgroup of ileal strictures. UST was associated with greater surgery-free medication persistence compared to TNFi & IMM (P=0.0036 and P=0.0003 respectively), though was similar to VED (P=0.14). A persistence difference was significant at 7 months between UST versus TNFi (92.0% vs 75.6%, P=0.029), and at 19 months between UST versus TNFi (80.5% vs 59.5%, P=0.037). Independent predictors of medication failure were: stricture length >4cm, perianal disease phenotype and use of a non-ustekinumab agent. After propensity score matching for stricture type, stricture location, stricture length, fistulising and perianal behaviour, and bioexperienced status, UST showed both superior long-term clinical success and surgery-free persistence than TNFi (P=0.026 and P=0.021 respectively).
376
Effect of IL17A inhibitors on inflammatory bowel disease progress: real-world registry data from the Persistence Australian National IBD Cohort (PANIC6) study
John Chetwood1,2,3, Sudarshan Paramsothy1,2,4,5 and Rupert Leong1,2,4,5
1Concord Repatriation General Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3St Vincent's Hospital Melbourne, Melbourne, Australia;4Macquarie University Hospital, Sydney, Australia;5Macquarie University, Sydney, Australia
Background and Aim: Few real-world studies have demonstrated a clear association between interleukin (IL)-17 inhibitors and inflammatory bowel disease (IBD) onset and severity.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC) registry for all patients with inflammatory bowel disease (IBD) on an advanced therapy (AT) up until Dec 2021. The PBS prospectively collects AT population-based prescribing data. Patients who had received an IL17 inhibitor prior to IBD AT were identified. Non-persistence was defined as failure to dispense AT prescriptions for >6 months. Corticosteroid-free persistence was defined as non-persistence or corticosteroid use after 3 months of initiation, whichever came first. Kaplan–Meier survival curves were generated for AT persistence and compared using the log-rank test.
Results: There were 106 cases of IL17 inhibitor use (87 with secukinumab, 19 with ixekizumab), for the indications of ankylosing spondylitis (24/106, 22.64%), chronic plaque psoriasis (35/106, 33.0%) and psoriatic arthritis (47/106, 44.3%). IL17 use was associated with a shorter time to start an AT agent for an IBD indication vs etantercept (P<0.0001). Prior IL17 use was also associated with a shorter persistence of the 1st IBD related biological agent (P<0.0001), including with tumour necrosis alpha inhibitors (TNFi) & ustekinumab (both P<0.0001), and vedolizumab (P=0.030) and tofacitinib (P=0.0018) vs no prior use. In secondary analysis, IL17 was associated with poorer corticosteroid-free persistence in a 1st line IBD biological agent (P<0.0001), including with TNFi (P<0.0001), ustekinumab (both P=0.0083), tofacitinib (P=0.010) though not vedolizumab (P=0.080) vs no prior use. Similarly for all IBD lines of therapy, prior IL17 exposure was associated with poorer overall and corticosteroid-free persistence (both P<0.0001), and with individual ATs (all P<0.05) except overall persistence with vedolizumab (P=0.16), though corticosteroid-free persistence was poorer (P=0.023). Overall persistence after IL17 inhibitor was poorer versus non-us, in both ulcerative colitis and Crohn’s disease (P=0.0055 & P=0.0088 respectively) with a non-significant trend in fistulising CD (P=0.053). Stratified by indication, prior IL17 use was associated with poorer IBD AT overall and corticosteroid-free persistence in patients with prior psoriatic arthritis indication for AT (P=0.033 & P=0.040 respectively), but not with a prior chronic plaque psoriasis nor ankylosing spondylitis indication (both P>0.05).
377
Infliximab and adalimumab in the treatment of fistulising Crohn’s disease: a propensity score-matched analysis from the prospective Persistence Australian National IBD Cohort (PANIC4) study
John Chetwood1,2,3, Sudarshan Paramsothy1,2,4,5 and Rupert Leong1,2,4,5
1Concord Repatriation General Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3St Vincents Hospital Melbourne, Melbourne, Australia;4Macquarie University Hospital, Sydney, Australia;5Macquarie University, Sydney, Australia
Background and Aim: There are extremely spare data on comparative medication efficacy in fistulising Crohn's disease (FCD). AGA/ECCO guidelines deem current evidence on immunomodulator co-therapy use in FCD insufficient to make recommendations. Persistence is a unique way to assess real-world outcomes.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC) registry for all patients with inflammatory bowel disease (IBD) on an advanced therapy (AT) for fistulising Crohn’s disease indication via the pharmaceutical benefits scheme (PBS) up until Dec 2021. The PBS prospectively collects AT population-based prescribing data. Non-persistence was defined as failure to dispense AT prescriptions for >6 months. Corticosteroid-free persistence was defined as nonpersistence or corticosteroid use after 3 months of initiation, whichever came first. Kaplan-Meier survival curves were generated for AT persistence and compared using the log-rank test. Propensity score matching was performed to account for baseline cohort imbalance.
Results: There were 5,739 lines of therapy in 4,466 patients over the 16-year period with 17,144 patient-years of follow-up; via therapy 2,605/5,739 (45.4%) used adalimumab and 3,134/5,739 (54.6%) used infliximab; 1,697/5,739 (29.6%) used thiopurine co-therapy at induction, whilst 242/5,739 (4.2%) used methotrexate. As a first-line biologic (biologic-naïve), infliximab showed superior overall- and corticosteroid-free persistence to adalimumab (P=0.0002 & P=0.0021 respectively). Used after first-line (biologic-exposed), there was no difference between agents for overall persistence (P=0.064) though infliximab showed greater corticosteroid-free persistence (P=0.030). Co-induction with thiopurine was associated with improved overall- and corticosteroid-free persistence (P=0.0002 & P=0.045 respectively). After propensity score matching, infliximab showed superior overall and corticosteroid-free persistence compared to adalimumab in bio-naïve (P<0.0001 and P=0.0016 respectively), not in bio-exposed patients (P=0.12 & P=0.074 respectively). Thiopurine co-use was associated with superior overall- and corticosteroid-free persistence (P=0.0014 & P=0.021 respectively), though no difference was seen with methotrexate co-use (both P>0.05).
378
Combined immunosuppressive therapies in inflammatory bowel disease: real-world registry data from the Persistence Australian National IBD Cohort (PANIC6) study
John Chetwood1,2,3, Sudarshan Paramsothy1,2,4,5 and Rupert Leong1,2,4,5
1Concord Repatriation General Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3St Vincent's Hospital Melbourne, Melbourne, Australia;4Macquarie University Hospital, Sydney, Australia;5Macquarie University, Sydney
Background: Combinations of immunosuppressive medications are used for refractory disease, multi-organ manifestations and multiple concurrent autoimmune diseases. However there are extremely limited data on prescribing data and outcomes.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC) registry for all patients with inflammatory bowel disease (IBD) on an advanced therapy (AT) receiving another immunosuppressive AT via the pharmaceutical benefits scheme (PBS) up until Dec 2021, with an overlap ≥1 month, lines were censored if overlap medications were in the same medication class. The PBS prospectively collects AT population-based prescribing data. Non-persistence was defined as failure to dispense AT prescriptions for >6 months. Kaplan–Meier survival curves were generated for AT persistence and compared using the log-rank test.
Results: 65 combinations in 64 patients were identified. Via combination, 50/65 (76.9%) contained a tumour necrosis alpha inhibitor (TNFi), 29/65 (44.6%) contained vedolizumab (VED), 17/65 (26.1%) contained ustekinumab (UST), and 9/65 (13.9%) contained a Janus kinase inhibitor (JAK). Via class, the commonest combinations were: vedolizumab/TNFi (16/65, 24.6%), ustekinumab/TNFi (15/65, 23.0%) and vedolizumab/dupilumab (5/65 (7.7%). Commonest IBD indications were luminal Crohn’s disease (CD) (34/65, 52.3%) and ulcerative colitis (UC) (20/65, 30.8%). Commonest co-indications were rheumatoid arthritis and ankylosing spondylitis (both 16/65, 24.6%), followed by psoriatic arthritis (12/65, 18.5%) and chronic plaque psoriasis (13/65, 20.0%). Median medication overlap was 6.1 months (interquartile range (IQR): 1.0-11.2 months). There was no difference between luminal CD vs UC for medication overlap duration (P=0.93), nor between non-IBD indications (all P>0.05). For IBD indications UST and VED had the longest persistence, and JAK had the poorest (overall P=0.019). For non-IBD indications, p19 inhibitors were associated with the longest overlap duration (16.0 months, IQR:0.98- 21.3), whereas dupilumab was associated with the shortest (3.0 months, IQR: 1.0-7.1). When using TNFi for an IBD indication, ustekinumab co-therapy was associated with the greatest persistence and tocilizumab with the poorest (P=0.12). For vedolizumab, there was no persistence difference according to co-therapy agent (all P>0.05).
384
Crohn's disease strictures respond to adalimumab drug treatment: Long term (4.5 years) results of the STRIDENT randomised controlled trial
Grace Lovett
St Vincent's Hospital Melbourne, Melbourne, Australia
Background and Aim: The randomised STRIDENT (Stricture Definition and Treatment) trial showed a majority of patients with symptomatic Crohn’s disease strictures clinically responded to anti-TNF therapy following 12 months of adalimumab +/- thiopurine.1 We present here 4.5 year follow up to assess risk of surgery, predictors of surgery, and long term durability of treatment response.
Methods: Patients with symptomatic inflammatory Crohn’s disease strictures (elevated faecal calprotectin and CRP) were assessed with intestinal ultrasound, MRI and ileo-colonoscopy. Patients were randomised 2:1 to high dose adalimumab induction (160mg weekly for 4 weeks) followed by 40mg fortnightly plus thiopurine, with adalimumab dose increase at 4 and/or 8 months if evidence of ongoing inflammation, versus standard dose adalimumab monotherapy. The primary endpoint (clinical response) was improved Obstructive Symptom Score by 1 point at 12 months. An MRI risk score was calculated based on a combination of pre-treatment factors: pre-stenotic dilatation ≥30mm, stricture length >50mm or bowel wall thickness ≥10mm (each factor being assigned a score of 1). Patient interview was conducted at 4 years.
Results: In the initial 12 month study, 52 (67.5%) patients were randomised to the intensive and 25 (32.5%) to the standard treatment arm. 64 of 77 (83%) patients completed at least 12 months of adalimumab therapy as part of the study while 13 (17%) withdrew: 8 surgery, 5 other. The 77 participants were assessed for outcomes at a minimum of 4 years after study entry (median 57 (IQR 51.7-59.5) months). At follow up, 44/77 (57.1%) remained on adalimumab; 24/77 (31.2%) had changed to another biologic (6 infliximab, 15 ustekinumab, 1 vedolizumab, 1 guselkumab and 1 upadacitinib) and 7/77 (9.1%) had ceased biologic therapy. Of those taking a thiopurine at 12 months, 12/28 (42.9%) remained on thiopurine treatment. Since study completion at 12 months 15/77 (19.5%) patients had required endoscopic dilation and 33/77 (42.9%) had been hospitalised, with no difference between standard or intensive treatment groups (8/18 [44.4%] standard vs 15/46 [32.6%] intensive, P=0.40; 4/18 [21.9%] standard vs 10/46 [21.7%] intensive, P>0.99). A total of 22/77 (28.6%) patients required surgery, 8 in the first year, 6 in the second year and a further 8 in the last 2.5 years, with no difference between standard or intensive treatment groups (8/22 [36.4%] standard vs 14/22 [63.6%] intensive, P=0.37). Clinical responders had higher surgery-free survival at the end of the follow up period compared to non-responders (80.4% vs 35%, P < 0.001). Median time to resection was 21.6 months (IQR 10.5-27.6) with no difference between treatment group (25.3 months [IQR 11.8-32.1] standard vs 20 months [IQR 9.2-27.2] intensive; P=0.60) or clinical response (11.8 months [IQR 6.9-27.9] non-responders vs 24 months [IQR 20-27.2] responders; P=0.06). The MRI risk score predicted surgery free survival: 100% of patients with an MRI risk score of 0 were surgery free at 4.5 years, 66.7% with a score of 1, 69.6% with a score of 2 and 46.2% with a score of 3 (P=0.008).
390
Tumour necrosis factor inhibitors have significantly poorer persistence in ulcerative colitis (UC) compared with Crohn’s disease (CD), while vedolizumab persistence is poorer in advanced therapy (AT) exposed, but not AT-naïve CD patients compared with UC: data from persistence Australian national inflammatory bowel disease cohort (PANIC 5)
Ryan Chang-ho Choi1, John Chetwood1, Aviv Pudipeddi1, Yanna Ko1, Thanaboon Chaemsupaphan1, Fei Yang Pan2, Viraj Kariyawasam3, Sudarshan Paramsothy1 and Rupert Leong1
1Department of Gastroenterology and Hepatology, Concord Repatriation General Hospital, Sydney, Australia;2Department of Gastroenterology and Hepatology, Macquarie University Hospital, Sydney, Australia;3Department of Gastroenterology and Hepatology, Blacktown and Mount Druitt Hospital, Sydney, Australia
Background and Aim: Whilst tumour necrosis factor inhibitors (TNFi) and anti-integrin α4β7 (vedolizumab) are both effective treatments for Crohn’s disease (CD) and ulcerative colitis (UC), the persistence of these advanced therapies (AT) in CD compared with UC is unknown. This study aims to determine the persistence of ATs in CD compared with UC in both AT-naïve and AT-exposed patients.
Methods: We analysed the Persistence in Australian National IBD Cohort (PANIC), the largest, prospectively collected national registry database that contains 100% of all AT data in Australia via PBS. Non-persistence was defined as failure to dispense prescriptions ≥6 months from the preceding treatment or changing to an alternate AT for an IBD indication. Kaplan-Meier curve and Cox regression were used to compare the persistence of each disease for respective AT. The variables with P<0.1 in the univariate model were included in multivariate analysis to calculate adjusted hazard ratios (aHR) with 95% confidence intervals (CI), with P-value <0.05 deemed statistically significant.
Results: From Jan 2007 to Dec 2021, 28,758 patients (CD; 19,087; 66.3%) underwent 39,618 lines of ATs (infliximab (IFX; 16,265), adalimumab (ADA; 14,898) and vedolizumab (VED; 8,455)), totaling 102,897 patient-years of follow-up (median follow-up, 41 months; interquartile range, 17-76). The time to 50% loss of steroid-free persistence was 36 months (95% CI, 35-37 months). Multivariate analysis (adjusted for age, sex and immunomodulator co-therapy) revealed that the TNFi had significantly poorer persistence in AT-naïve patients with UC compared with CD (aHR, 0.72; 95% CI, 0.68-0.75, P<0.001 for infliximab (IFX; Figure 1A) and aHR, 0.70; 95% CI, 0.64-0.77; P<0.001 for adalimumab (ADA; Figure 1B). Similarly, in AT-exposed patients, TNFi had significantly poorer persistence in UC compared with CD (aHR, 0.75; 95% CI, 0.67-0.84, P<0.001 for IFX and aHR, 0.75; 95% CI, 0.66-0.85; P<0.001 for ADA, respectively). Furthermore, TNFi persistence was markedly poorer in older patients (age ≥ 60) with UC who were AT-naïve (IFX; aHR, 0.66; 95% CI, 0.57-0.75; P<0.001 and ADA; aHR, 0.53; 95% CI, 0.43-0.67; P<0.001) or AT-exposed (IFX; aHR, 0.72; 95% CI, 0.56-0.94; P=0.014 and ADA; aHR, 0.54; 95% CI, 0.39-0.74; P<0.001), compared with CD. The time of TNFi commencement (i.e., before or after 2017 when other non-TNFi ATs became widely available) did not affect these outcomes. Contrary to TNFi, vedolizumab (VED) persistence was similar between AT-naïve patients with UC compared with CD (aHR, 0.98; 95% CI, 0.86-1.11, P=0.71; Figure 1C). In contrast, VED had poorer persistence in AT-exposed patients with CD (aHR, 0.88; 95% CI, 0.80-0.98; P=0.021) compared with UC. In older patients (age ≥60) the persistence of VED in CD was similar compared with UC in both AT-naïve (aHR for CD, 0.86; 95% CI, 0.69-1.06; P=0.2) and AT-exposed (aHR, 0.98; 95% CI, 0.78-1.23; P=0.9) patients.
394
Inequity in IBD advanced therapy prescribing across Australia reflects regional and state based variation in quality of IBD care delivery
Gregory Moore1,2, Kathryn Gazelakis2, Simon Knowles3 and Charlotte Keung1,2
1Monash Health and Monash University, Melbourne, Australia;2Monash Health, Melbourne, Australia;3Swinburne University, Melbourne, Australia
Background and Aim: Quality of care in Inflammatory Bowel Disease (IBD) can be measured by assessing variability of care delivery. Local access to advanced IBD therapies (AIBDT) is critical for the best outcome for IBD patients however barriers to their uptake remain. We assessed variability in prescribing and dispensing of AIBDT in Australia for Crohn’s Disease (CD) and Ulcerative Colitis (UC) by state and regional area.
Methods: Analysis of PBS prescription postcodes and dispensing area of AIBDT (infliximab (IFX), adalimumab (ADA), ustekinumab (UST), vedolizumab (VED) and tofacitinib (TFC)) from Services Australia from October 2017 to August 2022 was undertaken with comparisons by population, Modified Monash Model rurality (1 urban – 7 remote), clinical indication and number of Gastroenterologists per state. Statistics are expressed as Chi squared analyses. Local ethics approval was obtained.
Results: There were 169,058 prescriptions for AIBDT issued per annum over this period. ADA (45.3%) was the most frequently prescribed AIBDT compared with IFX (29.7%), VED (14.5%), UST (9.6%) and TFC (0.9%). This order was similar across all regions except for NT which used more infliximab. ADA was the most used AIBDT for luminal CD (ADA 52.2%, IFX 24.6%, UST 15.6%, VED 7.6%), and fistulising CD (ADA 59.7%, IFX 40.2%). For UC, the most prescribed was VEDO (39.3%) then IFX (36.8%), ADA (20.3%) then TFC (3.6%). Highest prescribing per 1000 population per annum was Tasmania, ACT, Victoria and SA (8.5, 8.5, 7.9 and 7.2 respectively) all significantly higher than WA, NSW and Queensland (6.3, 5.8 and 5.7) and Northern Territory (2.3). When compared with the number of gastroenterologists in each state, biologics prescribed per practitioner per annum were TAS (287), WA (189), VIC (177), SA (175) ACT (161), NSW (147), QLD (140) and NT (98). When looking at rurality, there were markedly fewer patients prescribed AIBDT in MMM3 (-70.6%), MMM4 (-57.0%), MMM5 (-81.7%). Local delivery of care (concordant prescriber-patient MMM) was 81% for MMM1, 23% for MMM2 and less than 5% for MMM4-5. More remote MMM6 and very remote MMM7 patients saw prescribers in large regional centres (MMM2, 63% & 45% respectively). There were no major differences for self-administered versus infusion AIBDT across the MMM scores of rurality.
397
Flow of advanced therapy pathways and variations over time in Crohn’s disease and ulcerative colitis: Data from the Persistence Australian National IBD Cohort (PANIC5)
Fei Yang Pan1, Aviv Pudipeddi2, Ryan Chang-Ho Choi2, John Chetwood2 and Rupert Leong1,2
1Macquarie University Hospital, Macquarie, Australia;2Concord Repatriation General Hospital, Concord, Australia
Background and Aim: Choice of advanced therapy (AT) in Crohn's disease (CD) and ulcerative colitis (UC) have increased, however the optimal positioning and sequencing of agents are unknown. We present the first national data on sequencing for all AT treatments in Australia with Sankey diagrams.
Methods: We analysed the Persistence Australian National IBD Cohort (PANIC) 5 registry, including all UC and CD patients on AT via the Pharmaceutical Benefits Scheme up to December 2021. Sankey diagrams were created using Plotly, a Python-based tool. Each AT was coded as a node along the x-axis, and the y-axis represented patients' treatment pathways, including sequential switches and stops from first to fifth-line treatments. Patients were divided into tertiles based on first AT commencement date (T1, T2, and T3) for both UC and CD data, and trends across these periods were compared. Statistical analyses were performed using SPSS.
Results: In 9,671 UC patients (23,220 patient years), VED patients were significantly more likely to stay on treatment compared to tumour necrosis factor inhibitors (TNFi) (P<0.001) from first to second line treatment. TOF was less likely to be used in bio-naïve patients and more commonly used in bio-exposed patients. Comparing first to fifth line AT in UC, TOF was the only treatment which showed an increase in patients from 85 to 397, a 366% increase. UC patients were 13.1 (CI 12.85, 13.42) P<0.001) more likely to stop treatment in T1 compared to T3. In 19,087 CD patients (79,677 patient years), VED patients were significantly more likely to stay on treatment compared to TNFi (P<0.001). UST was 2.5 times more likely to be used in bio-exposed patients compared to ADA, the second most common choice in bio-exposed patients in T3. CD patients were 13.6 times (CI 13.52, 13.84) P<0.001) more likely to stop treatment in T1 compared to T3. Comparing first to fifth line AT, UST increased from 2231 to 4294 patients (92%), and VED from 1171 to 1690 patients (44%).
402
Gut microbiota are associated with disease activity in patients with Crohn’s disease and ulcerative colitis: baseline sequencing from the Australian IBD Microbiome study
Robert Little1,2, Thisun Jayawardana3,7, Fan Zhang3, Sabrina Koentgen3,7, Nan Wu3, Paris Tavakoli3, Andrew Chung3,7, Anson Ho3,7, Alex Boussioutas1,2, Mark Ward1,2, Miles P Sparrow1,2, Peter Gibson2, Simon Ghaly4, Crispin Corte5, Nick J Talley6, Steven Leach7, Daniel Lemberg7,8, Shoma Dutt9, Sudarshan Paramsothy10, Rupert Leong10, Susan J Connor11,7 and Georgina Hold3,7
1Alfred Health, Melbourne, Australia;2Monash University, Clayton, Australia;3Microbiome Research Centre, Sydney, Australia;4St Vincent’s Hospital, Sydney, Australia;5Royal Prince Alfred Hospital, Sydney, Australia;6University of Newcastle, Newcastle, Australia;7University of New South Wales, Sydney, Australia;8Sydney Children's Hospital, Sydney, Australia;9The Children's Hospital at Westmead, Sydney, Australia;10Concord Repatriation General Hospital, Sydney, Australia;11Liverpool Hospital, Sydney, Australia
Background and Aim: Identifying microbial changes associated with active inflammation in IBD may provide a greater understanding of upstream drivers of disease activity. This study aimed to characterise differences in gut microbial signatures according to inflammatory activity amongst patients enrolled in the Australian IBD Microbiome (AIM) study.
Methods: Paired faecal and oral samples alongside participant demographic and disease characteristics were collected at baseline from all patients with IBD enrolled in the AIM study from June 2019 to November 2023. Clinically active disease was defined as Crohn’s disease activity index (CDAI) score >150 or partial Mayo (pMayo) score >1 for patients with CD and UC, respectively. Biochemical activity was defined as faecal calprotectin (FCP) >150 ug/g assessed by ELISA. Faecal and oral microbial samples were collected in DNA stabilising buffer, aliquoted and stored at -80oC. Samples underwent 16S rRNA sequencing with annotation of DNA sequences to operational taxonomic units at the genus level. Differences in alpha diversity (Shannon index) and relative abundance of identified genera between the groups were assessed using Kruskal-Wallis or Mann-Whitney U tests. Beta diversity (Bray-Curtis dissimilarity) between bacterial communities were shown using the Principal Coordinate Analysis (PCoA), and significance of variance tested using ADONIS within R.
Results: 563 participants (302 CD, 261 UC) returned baseline faecal (n = 407) and/or oral samples (n = 436) and were included in the analysis. Mean age was 43 years (SD 15), mean disease duration 11 years (SD 11), mean BMI 26 kg/m2 (SD 5.4), 58% were female, 14% were smokers and median FCP was 37 ug/mg (IQR 20-167). 118/302 (39%) of the CD group and 88/253 (35%) of the UC group had clinically active disease and 22/90 (24%) of CD and 35/120 (29%) in the UC group had FCP activity. Oral and faecal microbial analyses showed no statistical differences in alpha or beta diversity between CD and UC patients with clinical or biochemical activity vs. those in remission and no difference according to Montreal disease location or phenotype for CD or disease extent for UC. At the phyla level, there was depletion of Bacteroidota (B) and increased Firmicutes (F) abundance in faecal samples of CD patients with clinically active disease vs. those in remission - with a subsequent increase in F:B ratio. There were no differences in relative abundance of phyla in UC patients according to pMayo activity or in either group according to FCP activity vs. FCP remission. However, on analysis at the genus level, there were 15 and 8 genera with significantly different relative abundances between FCP activity vs. remission in CD (Fig 1A) and UC (Fig 1B) patients, respectively.
404
Assessing advanced trainees' perspectives on inflammatory bowel disease education: a survey study
Fei Yang Pan1 and Rupert Leong1,2,3
1Macquarie University Hospital, Macquarie, Australia;2Concord Repatriation General Hospital, Concord, Australia;3University of Sydney, Concord, Australia
Background and Aim: For advanced gastroenterology trainees (ATs), mastering IBD management is crucial. Despite its importance, there's a gap in understanding ATs' perspectives on their IBD education and needs. Variability in IBD training, with many patients seen in private rooms, limits teaching opportunities. This survey explores ATs' views on IBD education, assesses their knowledge and confidence in managing IBD patients, and identifies factors influencing their confidence.
Methods: A cross-sectional survey via Google Forms targeted NSW gastroenterology ATs, evaluating their IBD education and training. Questions covered training year, access to specialized IBD resources (clinics, nurses, dietitians, psychologists, trials coordinators), exposure to IBD patient management, and engagement with PBS paperwork. Participants rated their confidence in managing outpatient IBD patients, de-prescribing medications, prescribing advanced therapy, and completing Pharmaceutical Benefits Scheme (PBS) criteria. The survey also assessed the adequacy of teaching from consultant gastroenterologists. Data were collected using QR codes, with reminders to boost responses. Descriptive statistics summarized demographics, training experiences, confidence levels, and perceptions of teaching adequacy. Spearman correlations examined relationships between training year, supervision adequacy, teaching sufficiency, and confidence levels.
Results: Participants included 7 in AT 1, 5 in AT 2, and 4 in AT 3. Sixteen had specialized IBD clinics and nurses, while 8 did not. Thirteen had IBD dietitians, and 6 had IBD psychologists and trials coordinators, with 18 lacking these resources. Seven observed consultations with IBD gastroenterologists, while 17 did not. Supervision adequacy ratings were: 12 (1–3), 5 (4–6), 2 (7–9), and 5 (10+). Observations of IBD clinics were: 11 (1–10), 6 (11–20), and 1 (30+). Confidence in managing outpatient IBD patients was moderate (Mean = 3.3, SD = 1.4; median = 3, range 1–5). Confidence in de-prescribing medications was lower (Mean = 2.7, SD = 1.4; median = 3, range 1–5). Confidence in prescribing advanced therapy was higher (Mean = 3.5, SD = 1.3; median = 4, range 1–5). Spearman correlations showed no significant relationships between training year, supervision adequacy, teaching sufficiency, and confidence levels in managing IBD patients, de-prescribing medications, prescribing advanced therapy, and completing PBS paperwork (P > 0.05).
415
Colesevelam is effective and well-tolerated for bile acid diarrhoea in Australia
Cassandra Monitto1,2, Akhilesh Swaminathan1,3, Jacoba Van Wees1, John Coutsouvelis2,4, Alex Boussioutas1,4,5,6, Miles P Sparrow1,4, Michael Dooley2,4 and Mark Ward1,4
1Department of Gastroenterology, Alfred Health, Melbourne, Australia;2Department of Pharmacy, Alfred Health, Melbourne, Australia;3Department of Medicine, University of Otago, Christchurch, New Zealand;4Monash University, Australia;5University of Melbourne, Australia;6Peter MacCallum Cancer Centre, Melbourne, Australia
Background and Aim: Bile acid diarrhea (BAD) can result in detrimental effects to quality-of-life. Commercially available bile-acid sequestrants such as colestyramine have, in recent times, been difficult to access and have high rates of intolerance. Colesevelam is an oral, bile-acid sequestrant approved for use in BAD but not widely available in Australia. This study assessed the efficacy and tolerability of colesevelam in a cohort of Australian patients with BAD.
Methods: This retrospective, single centre study assessed adult outpatients commenced on colesevelam for clinically diagnosed BAD after intolerance/lack of efficacy to conventional treatment with colestyramine between November 2019-January 2024. Primary study endpoints included treatment efficacy (≤3 bowel motions a day and reduction in number of stools per day) and tolerability as assessed at the first clinic follow-up. The midpoint of stool frequency was used in instances where a range was reported. Treatment persistence was a secondary endpoint. The wilcoxon signed-rank test assessed differences in bowel frequency before and after treatment, and Kaplan Meier analyses evaluated treatment persistence.
Results: A total of 21 patients (previous colestyramine intolerance, n=16) were included (7 female; median age 54 years (IQR, 45-60); median follow-up 239 days (range, 98-391)). Underlying diagnoses included Crohn’s disease (CD, n=18), irritable bowel syndrome (n=2), collagenous colitis (n=1). Previous small bowel resection was reported in 15 patients with CD, 9 of which were extensive (≥50cm or multiple resections). The median treatment duration was 378 days, median dose was 6 tablets/day (3750mg) and 12/21 (57.1%) patients remained on colesevelam throughout the study period (Figure 1). All patients (19/19) with recorded stool frequency had ≥5 bowel motions a day at baseline. Median stool frequency reduced from baseline to first clinic appointment (baseline=5/day vs. first clinic=3/day, p<0.01) and 10/21 patients had ≤3 bowel motions at first follow-up (median time to follow-up of 76 days (IQR 47-98)). In those who did not have intolerance to colesevelam at first clinic follow up (n=16), median stool frequency reduced from 5/day (baseline) to 1/day (p<0.01, Figure 1). Rates of intolerance to colesevelam were similar between those with CD (4/17; abdominal pain, n=2, nausea, n=1, bloating, n=1) and those without (1/3; nausea, n=1; p=1.00).
418
Predictors of medication non-adherence in inflammatory bowel disease
Winnie Chuck, Alex Barnes and Reme Mountifield
Department of Gastroenterology and Hepatology, Flinders Medical Centre, Bedford Park, Australia
Background and Aim: Poor adherence to medications in the inflammatory bowel disease (IBD) cohort has a direct negative impact on clinical outcome. However, the self-reported medication non-adherence in the Australian IBD population ranged from 24-45%, with predictive factors including patients' psychological distress and their believe about medications. Therefore, this study aimed to examine the self-reported medication non-adherence rate and its associated factors.
Methods: A prospective cohort study is conducted via online surveys, including both Ulcerative Colitis (UC) and Crohn's Disease (CD) patients who attended a tertiary IBD centre. Adherence to medications was assessed using Medication Adherence Rating Scale-5 (MARS-5), with the score of ≤20 signifying non-adherence. Univariate and multivariable regression analysis were used to study the association of medication non-adherence and its predicting factors, by including Generalised Anxiety Disorder Questionnaire (GAD-7), Body Image Scale and Beliefs about Medications (BMQ), and activity scores by Harvey Bradshaw Index (HBI).
Results: A total of 210 responses were gathered prior to the census date [(132 females (63%); 78 males (37%); mean age 44.2 (SD 17.8 years)]. More patients had CD than UC (60.5% vs 34.9%, 6.9% indeterminate colitis), with total mean duration of diagnosis being 12.7 years (SD 12.2 years). 56 patients (26.7%) had IBD-related surgery. The mean Body Mass Index (BMI) was 28.0 (SD 7.2). Most patients were non active smokers (178, 84.5%). The prevalence of non-adherence was 25.3% [(mean MARS-5 score 22.1 (SD 3.75)]. Univariate analysis demonstrated that anxiety and depression [Odds ratio (OR) 2.9; 95% CI, 5.8-10.3; P = 0.003); OR 3.0; 95% CI, 8.4-13.2; P = 0.001) respectively] were statistically significant in its association to medication non-adherence. The other statistically significant factor was patients’ perceived medication overuse (BMQ overuse) (95% CI 8.9-10.8; P = 0.029), with sub-analysis demonstrating BMQ-12 being the only score (out of 4) for BMQ overuse that was associated with non-adherence (OR 2.34; P = 0.0023). In relation disease activity, HBI was a statistically significant predictor to medication non-adherence with OR 2.36 (95% CI 2.7-4.7; P = 0.029). After accounting for BMI, age, sex, BIS, GAD7, PHQ9 and BMQ scores, SCCAI and HBI, multivariable regression analysis demonstrated that anxiety, depression, BMQ overuse and high HBI were statistically significant medication non-adherence predictors.
Conclusion: Anxiety, depression, perceived overuse of medications by doctors and high disease activities were demonstrated to be significant in predicting medication non-adherence. These findings highlighted the complexed interplay of individual and psychosocial factors in medication non-adherence among IBD patients.
420
Infliximab induced pericardial fat necrosis
Reuben Malloy1, Denis Rubtsov1, Ayesha Chapagain1, Ruth Ducommun1, Rebecca Cohen1, David Huynh2 and Myat Khaing1,2,3
1The Prince Charles Hospital, Brisbane, Australia;2Mater Adult Public Hospital, Brisbane, Australia;3University of Queensland, Brisbane, Australia
Introduction: Infliximab, a monoclonal antibody used for inflammatory bowel disease, is typically well tolerated but with several, albeit rare, complications. Cardiac complications, such as pericarditis and pericardial effusion, are well recognised. However, there are no published cases documenting infliximab use complicated by pericardial fat necrosis (PFN); a condition arising from an inflammatory process in the mediastinal fat surrounding the heart. Here, we present the first case of infliximab induced PFN.
Case report: A 28-year-old woman presented with 3-days of severe central non-radiating sharp chest pain, worse with inspiration and lying supine, and better leaning forwards. Her medical history included first-degree heart block, psoriasis and ulcerative proctitis in histologic remission. Her ulcerative proctitis was diagnosed 1 year prior to this presentation. Her medication included 8 weekly 5mg/kg infliximab infusions commenced by her dermatologist for psoriasis 2 years prior. She had no ulcerative proctitis symptoms. Electrocardiography showed sinus rhythm with first-degree heart block. Cardiac troponin-I was 3ng/L, haemoglobin was 147g/L, and biochemistry was within normal range. C-reactive protein (CRP) and faecal calprotectin were not performed. 24-hour Holter monitor had no concerning arrythmias. Echocardiogram demonstrated normal valvular, LV and RV size and function with LVEF 69%, and RVSP of 25mmHg. CT chest and pulmonary angiogram excluded pulmonary emboli and identified a 32mm encapsulated fat soft tissue density in the left paracardiac region, consistent with PFN (Figure 1A). She was prescribed 25mg of diclofenac three times a day for one week. 4-weeks later, cardiac magnetic resonance imaging (MRI) showed disease progression with increased area of inflammation (Figure 1B). The chest pain took 6 weeks to resolve. The patient had slow improvement on serial imaging with reduced inflammation on MRI 4 months after diagnosis and complete resolution 10 months after diagnosis. A multidisciplinary decision involving gastroenterology, dermatology, rheumatology, and cardiology was then made to cease infliximab and commence Ustekinumab to prevent recurrence of PFN. 6-months after commencing Ustekinumab, the patient remained in clinical, endoscopic and histologic remission on colonoscopy with CRP <2mg/L and calprotectin of 32μg/m.
424
Screening for depression and anxiety in IBD is worth the effort
Luke Betts, Reme Mountifield and Alex Barnes
Southern Adelaide Local Health Network, Bedford Park, Australia
Background and Aim: Depression and anxiety are common in patients living with Inflammatory Bowel Disease (IBD). Symptoms impact on quality of life and psychological considerations and management in this population can be complex. Consideration has been given to screening for mental health conditions as a routine part of IBD Clinical care. The study aimed to identify the proportion of IBD clinic patients with clinically significant anxiety, depression or self-harm.
Methods: A cross-sectional survey was completed by people with IBD attending an IBD clinic at a large tertiary hospital. Clinically significant depression (Patient Health Questionnaire-9 - PHQ-9>15) and clinically significant anxiety (General Anxiety Disorder-7 - GAD-7 >10) were defined using screening questionnaires. The PHQ-9 incorporates a question on thoughts of self-harm.
Results: In a cohort of 210 respondents, the median age was 44 years (31-59) (Table 1). The majority were female (63.3%) and had Crohn’s disease (50.5%). 204 respondents completed screening questionnaires. Over a third (35.8%) of participants had clinically significant depression with PHQ-9 mean 11.6 (8.2). 17.2% of participants had clinically significant anxiety GAD-7 mean 5.9 (6.3). Thoughts of self-harm were present in 17.2% (1 in 6) of survey responses with 25.7% of these reporting thoughts of self-harm nearly every day (4.2% of survey respondents). From March to May 2024 clinical follow-up of 23 participants with clinically significant depression or anxiety identified 47.8% had existing community support in place. Mental Health Care Plan (MHCP) were or had been active in 21.7% of participants. Of those seen in rapid access IBD clinics none had formal community mental health support. One participant was deemed high risk and referred to a mental health triage service.
425
Early serum and faecal cytokines predict treatment response and colectomy in acute severe ulcerative colitis
Christopher Li Wai Suen1,2,3, Matthew Choy1,2, Kaylene Cheng3, Danny Con1,2, Julie Nigro3, Neil Wilson3, Kerry Breheney3, Peter De Cruz1,2 and Kumar Visvanathan2,3
1Austin Health, Melbourne, Australia;2Department of Medicine, University of Melbourne, Melbourne, Australia;3Immunology Research Centre, St Vincent's Hospital Melbourne, Melbourne, Australia
Background and Aim: Acute severe ulcerative colitis (ASUC) is a medical emergency with variable outcomes. We aimed to evaluate whether early serum and faecal cytokine levels predict treatment response.
Methods: Serum and stool were collected from patients with ASUC. Steroid-refractory patients received infliximab (IFX) as part of a randomised controlled trial that evaluated escalated infliximab (IFX) dosing. Specimens were collected at screening, and if steroid-refractory at days 1 and 3 post-IFX. Response to first IFX dose was assessed by day 7. IL-6 and TNF levels were quantified using ELISA after clinical study conclusion.
Results: Within the cohort of 190 patients, 54 were steroid-responsive and 136 steroid-refractory and received IFX. Of the steroid-refractory patients, 85 (62.5%) were IFX responders and 51 (37.5%) were IFX non-responders. 17/136 (12.5%) patients underwent colectomy by 3 months.
Steroid response: At screening, serum IL-6 was higher in steroid non-responders compared to responders (10.5 pg/mL vs 3.5 pg/mL, P<0.001), whereas faecal IL-6 was similar in both groups (154.7 pg/mL vs 138 pg/mL, P=0.09). Faecal TNF at screening was higher in non-responders compared to responders (48.6 pg/mL vs 14.6 pg/mL, P=0.032).
IFX response: Serum IL-6 at was higher in IFX non-responders compared to responders at all timepoints (P<0.005); however, this finding was not observed with faecal IL-6. Whilst faecal TNF at screening, days 0 and 1 did not differ between IFX responders and non-responders, median day 3 faecal TNF was suppressed below detection limits (<1.56 pg/mL) in IFX responders compared to 4.4 pg/mL in non-responders (P=0.006, AUC=0.65).
Colectomy by month 3: Higher serum IL-6 at screening (P=0.009, AUC=0.71) and day 1 (P=0.002, AUC=0.75) were associated with month 3 colectomy. Similarly, day 3 faecal IL-6 was higher in patients who required colectomy versus those who did not (159.0 pg/mL vs 110.7 pg/mL, P=0.02, AUC 0.69). Median faecal TNF at day 3 post-IFX was 6.3 pg/mL in patients who required colectomy but dropped below detection limit in those who avoided colectomy (P=0.004). Day 3 faecal TNF predicted colectomy (AUC=0.72) with a threshold of ≥7.07 pg/mL on Youden’s index having 50% sensitivity, 89.8% specificity, 43.8% PPV and 91.9% NPV.
Conclusion: Early serum and faecal cytokines predict outcomes in ASUC. Faecal TNF persistence 3 days after IFX is associated with non-response and colectomy, and might help identify patients who benefit from early IFX re-dosing. IL-6 elevation in non-responders suggests activation of an alternate immune pathway that may benefit from non-TNF-targeted therapy.
429
Unveiling the enigma: A challenging diagnostic odyssey from a patient with ulcerative colitis presented with sclerosing mesenteritis to small bowel follicular lymphoma
Introduction: Sclerosing Mesenteritis (SM) is a rare, fibrotic, non-neoplastic condition affecting the mesentery. SM presents most commonly in the 5th or 6th decade of life and may mimic an Inflammatory Bowel disease (IBD) flare, thereby delaying the diagnosis of SM. Literature has proposed previous surgery, autoimmune and paraneoplastic as potential pre-disposing factors. Non-Hodgkins Lymphoma (NHL) is the most common associated neoplasm in SM. This case study highlights the journey of a patient with Ulcerative Colitis (UC) and SM, and later diagnosed with NHL, Subtype Follicular Lymphoma (FL).
Case report: A 55-year-old man, was referred to our Tertiary Centre with abdominal pain and a computer tomography (CT) abdomen demonstrating mesenteric and retroperitoneal lymphadenopathy concerning for lymphoma. He had a background of Rectosigmoid UC (Montreal Classification E2) diagnosed in 2013 and in complete remission on Mesalazine therapy. He was extensively investigated, initially with a Fluorodeoxyglucose (FDG) positron emission tomography (PET) demonstrating retroperitoneal thickening, mesenteric lymphadenopathy and an FDG-avid foci in the small bowel (SB) (Figure 1.A). Magnetic Resonance (MR) bowel reported extensive infiltrating confluent soft tissue centred in the mesenteric root and altered signal in the proximal ileum, overall suggesting lymphoma with secondary retroperitoneal fibrosis. An endoscopic ultrasound demonstrated an extraluminal mass in the mesentery. A fine-needle aspirate was performed via transduodenal approach. Histopathology suggested SM. A CT-guided biopsy of the mesenteric mass was inconclusive. A laparoscopic biopsy of the mesenteric node confirmed SM. Multidisciplinary team (MDT) input concluded a diagnosis of SM and excluded lymphoma. A Rheumatologist commenced him on Prednisolone 60mg and a steroid-sparing agent, Azathioprine 50mg orally. Following this he clinically improved with minimal abdominal pain and had gained weight. He underwent an upper endoscopy and colonoscopy for iron-deficiency anaemia (IDA) which were non-contributory. A capsule endoscopy was organised demonstrating a small bowel ulcerative lesion. Following this, a double balloon enteroscopy (Figure 1.B) revealed a 30mm jejunal lesion with histopathology confirming Classic FL, low grade, Ki67 low and no high-grade transformation. A further PET demonstrated FDG-avid circumferential mucosal thickening in SB and mesenteric and retroperitoneal nodes. The Prednisone and Azathioprine was ceased. A haematologist has subsequently commenced Bendamustine/Obinutuzumab-Chemotherapy for FL.
432
Intensified versus standard dose infliximab induction therapy for steroid-refractory acute severe ulcerative colitis (PREDICT-UC): an open-label, multicentre, randomised controlled trial
Christopher Li Wai Suen1,2, Matthew Choy1,2, Danny Con1,2, Kristy Boyd1, Raquel Pena1, Kathryn Burrell1, Ourania Rosella1, David Proud1, Richard Brouwer1, Alexandra Gorelik3, Danny Liew4, William R Connell5, Emily K Wright5, Kirstin M Taylor6, Aviv Pudipeddi7, Michelle Sawers8, Britt Christensen9, Watson Ng10, Jakob Begun11, Graham Radford-Smith12, Mayur Garg13, Neal Martin14, Daniel van Langenberg15, John Nik Ding5, Lauren Beswick8, Rupert Leong7, Miles P Sparrow6 and Peter De Cruz1,2
1Austin Health, Heidelberg, Australia;2Department of Medicine (Austin Health), The University of Melbourne, Heidelberg, Australia;3Department of Medicine (Royal Melbourne Hospital), The University of Melbourne, Parkville, Australia;4Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia;5St Vincent's Hospital Melbourne, Fitzroy, Australia;6Alfred Health, Melbourne, Australia;7Concord Repatriation General Hospital, Concord, Australia;8Barwon Health, Geelong, Australia;9Royal Melbourne Hospital, Parkville, Australia;10Liverpool Hospital, Liverpool, Australia;11Mater Hospital, Brisbane, Australia;12Royal Brisbane and Women's Hospital, Herston, Australia;13Northern Hospital, Epping, Australia;14Princess Alexandra Hospital, Woolloongabba, Australia;15Box Hill Hospital, Box Hill, Australia
Background and Aim: The optimal dosing strategy of infliximab in acute severe ulcerative colitis (ASUC) is unknown. We compared intensified and standard dose infliximab rescue strategies and explored maintenance therapies following ASUC induction.
Methods: In this open-label randomised trial, patients from 13 Australian centres with steroid-refractory ASUC were randomised to a first dose of 10mg/kg or 5mg/kg infliximab in a 1:2 ratio. Patients receiving 10mg/kg (intensified strategy [IIS]) received a second dose at day 7 or earlier at time of non-response; all 5mg/kg patients were re-randomised 1:1 to standard (SIS) or accelerated strategies (AIS). SIS patients received 5mg/kg at week 0/2/6, with an extra 5mg/kg dose before day 7 if non-response. AIS patients received 5mg/kg at week 0/1/3, with the week 1 dose increased to 10mg/kg and given earlier if non-response. Primary outcome was clinical response by day 7 (Lichtiger score<10, with ≥3-point reduction and improvement in rectal bleeding and stool frequency ≤4/day). Maintenance phase compared thiopurine monotherapy, combination infliximab/thiopurine, and, infliximab monotherapy.
Results: 138 patients were randomised; 46 received a first dose of 10mg/kg and 92 received 5mg/kg. There was no difference in day 7 clinical response between the 10mg/kg and 5mg/kg groups (65% [30/46] vs 61% [56/92]; RR=1.06, 95%CI 0.94–1.20, P=0.62). There was no difference in time to clinical response or change in CRP from baseline to day 7. Day 7 response rate was 43% higher in the 10mg/kg vs 5mg/kg group in patients with baseline albumin <25 g/L (RR=1.43, 95%CI 0.86-2.39), and 39% higher in patients with CRP ≥50mg/L (RR=1.39, 95%CI 0.71-2.74), although not statistically significant. AIS and IIS groups achieved higher rates of combined clinical and biochemical remission at weeks 2 and 6, though outcomes were similar at month 3. Month 3 colectomy rates were IIS 3/45 (7%), AIS 9/47 (19%), SIS 5/43 (12%), P=0.20. Month 12 combined clinical and endoscopic remission rates were numerically higher in the infliximab/thiopurine group compared to thiopurine and infliximab monotherapy groups. Maintenance infliximab was associated with combined clinical and endoscopic remission at month 12 (RR=1.95, 95%CI 1.29-2.93, P=0.0014).
Conclusion: In steroid-refractory ASUC, a first dose of 10mg/kg or 5mg/kg infliximab achieved similar clinical response rates by day 7. Intensified or accelerated induction achieved earlier clinical and biochemical remission compared to standard induction; however, outcomes at three months were similar. Patients with albumin <25g/L and CRP ≥50mg/L may benefit from intensified dosing. Infliximab maintenance improved clinical outcomes at month 12.
436
Drug holiday may impair treatment persistence of monoclonal antibodies but not tofacitinib in ulcerative colitis: Data from the Persistence Australian National IBD Cohort (PANIC5)
Rupert Leong1,2,3, Viraj Kariyawasam3, Sudarshan Paramsothy1,2,3, Aviv Pudipeddi1,2 and John Chetwood1,2
1Concord Repatriation General Hospital, Concord, Australia;2University of Sydney, Concord, Australia;3Macquarie University Hospital, Macquarie University, Australia
Background and Aim: Patients with ulcerative colitis (UC) on advanced therapies (AT) may occasionally pause treatment to take drug holidays. Upon recommencing the AT, however, it is unknown if treatment persistence remains the same as their initial trajectory or if loss of persistence occurs. Whether persistence loss differs between AT or is mitigated by immunomodulators is also unknown. We evaluated AT persistence of UC subjects who took drug holidays versus those who did not.
Methods: We interrogated the Persistence Australian National IBD Cohort (PANIC5) registry of UC subjects up until Dec 2021. The PANIC5 registry includes 100% of all AT prescribing data in Australia. Drug holiday was defined as stopping AT therapy and recommencing the same AT after a dispensing gap. Non-persistence was defined as failure to continue to prescribe an AT for >6-months. Kaplan Meier survival curves were generated for persistence and compared using the log-rank test. Cox proportional hazards regression models were employed to calculate hazard ratios (HR) and 95% confidence intervals (CI) with P<0.05 deemed statistically significant SPSS (IBM, USA).
Results: A total of 9,671 unselected UC patients (52.9% male) were recruited, providing 23,220 patient-years of prospective follow-up. There were 916 episodes of drug holiday for a median duration of 212 days (IQR: 90-335) compared against 13,287 control lines without drug holiday. Resumption of AT following a drug holiday was associated with significantly reduced median persistence of 9 months (IQR: 3-21) versus 12.5 months (IQR: 5-29) in controls (HR: 0.82, 95% CI: 0.74-0.91, P<0.001). Shorter drug holidays (<180 days) did not impact non-persistence rates versus longer drug holidays (P=0.41) nor did recent immunomodulator exposure (P=0.057). Tofacitinib persistence was not impacted by drug holiday (P=0.69) as opposed to monoclonal antibodies (P=0.001, Figure).
439
Concern for ocrelizumab-induced inflammatory bowel disease: a regional experience
Thomas Skinner1,2,3 and Nishmi Gunasingam2
1St Vincent's Hospital, Sydney Darlinghurst, Australia;2Wagga Wagga Base Hospital, Wagga Wagga, Australia;3University of New South Wales, Darlinghurst, Australia
Introduction: Ocrelizumab is an intravenous anti-CD20 monoclonal antibody therapy currently licensed as a first line treatment for clinically definite relapsing-remitting multiple sclerosis (R-R MS). The increasing use of Ocrelizumab, have highlighted its unique adverse effects, with some concern for an ocrelizumab-induced inflammatory bowel disease-like pathogenicity. We present a case series of two patients at a regional secondary hospital that highlight the difficulties in assessing for and managing these seemingly rare adverse outcomes.
Conclusion: This series iterate the importance of rare but significant adverse outcomes of new treatments in its informing of a drug’s safe use, monitoring and possible role for surveillance in the future.
458
Sequential rescue therapy with Janus kinase-inhibitors in corticosteroid and infliximab-refractory acute severe ulcerative colitis
Amirah Etchegaray1, George Tambakis1,2, Anthony Croft1,2, Graham Radford-Smith1,2 and Gareth Walker1,2
1Royal Brisbane and Women's Hospital, Brisbane, Australia;2The University of Queensland, Brisbane, Australia
Background and Aims: Acute severe ulcerative colitis (ASUC) is a life-threatening medical emergency affecting over 20% of patients with ulcerative colitis (UC). 30-40% of patients are refractory to intravenous corticosteroids (IVCS) and require rescue medical therapy or immediate colectomy. The potent Janus kinase-inhibitors, upadacitinib and tofacitinib, have proven efficacy for moderate-to-severe, but not ASUC. JAK-inhibitors have theoretical advantages over current rescue therapies due to high oral availability, rapid washout and long-term treatment durability. We describe the novel use of JAK-inhibitors as sequential rescue therapy following failure of dose-intensified infliximab in IVCS-refractory ASUC.
Methods: A retrospective study of adult (>17 years old) patients receiving second-line, sequential rescue therapy with a JAK-inhibitor following failure of IVCS and dose-intensified infliximab at a tertiary IBD centre between October 2023 and April 2024. Following infliximab failure and multidisciplinary team discussion, select patients were given the option of proceeding to colectomy as per standard of care, or, in the absence of emergent indication for surgery, a trial of a JAK-inhibitor ([upadacitinib 45mg daily] or [tofacitinib 10mg TDS]). Demographic and clinical data were captured during admission and 90-days post discharge. Co-primary outcomes included inpatient clinical response and 90-day colectomy-free survival. Secondary outcomes included adverse events and 90-day clinical (PRO-2<1) and biochemical (C-Reactive Protein [CRP]<5mg/L and faecal calprotectin [FCP]<150 ug/g) corticosteroid-free remission.
Results: Six patients received sequential rescue therapy with a JAK-inhibitor (upadacitinib n=5, tofacitinib n=1) following failure of IVCS and dose-intensified infliximab. Median age was 32 years (IQR 23-39), 67% were first and diagnostic presentations of ASUC, and 50% had extensive disease (Montreal E3) endoscopically on admission. Median CRP on admission was 100 mg/L (IQR 58-105), with a median FCP of 3400 μg/g (IQR 910-4950) and median Mayo Endoscopic Score (MES) of 3 (Table 1). 90-day colectomy-free survival was 67% (2 inpatient colectomies for refractory disease) and inpatient clinical response was 67%. Among four JAK-responders, 100% and 75% achieved clinical and biochemical corticosteroid-free remission at 90-days, respectively (Figure 1). We observed one complication with post-operative peritonitis necessitating laparoscopic washout. No other adverse events were recorded.
459
A real-world study describing the management and outcomes of perianal fistulising Crohn’s disease and predictors of fistula healing in the biologic era
Moshe Loebenstein1, Bowen Xia1, Gregory Moore1,2 and Charlotte Keung1,2
1Department of Gastroenterology, Monash Health, Melbourne, Australia;2School of Clinical Sciences, Monash University, Melbourne, Australia
Background and Aim: Perianal fistulae in Crohn’s disease (pCD) are particularly challenging to treat. Optimal management requires collaboration between inflammatory bowel disease (IBD) specialists and colorectal surgeons with the mainstay of medical therapy including anti-tumour necrosis factor alpha (anti-TNF) biologic drugs together with antibiotics, immunomodulators, surgical intervention and more recently, stem cells. Studies investigating prognostic factors which predict fistula healing have been predominantly retrospective and heterogenous, increasing the challenge of drawing robust conclusions [1]. The aim of this study was to describe real-world pCD management and outcomes in the biologic era and to identify factors which may affect fistula healing.
Methods: A retrospective cohort study including all patients with pCD treated at a large tertiary centre between January 2010 and December 2021 was undertaken by merging databases identified from ICD-10 diagnosis codes for Crohn’s disease, procedure codes for perianal surgery and biologic prescriptions. Demographic and clinical data including age, biologic sex, disease phenotype, smoking status, medications and adherence and MRI reports were extracted from the medical records. For descriptive statistics, continuous variables were expressed as median and interquartile range (IQR) and categorical variables as absolute frequencies. Analysis of predictors of fistula healing was undertaken using univariate logistic regression.
Results: Our preliminary analysis included 104 patients with pCD (52.9% male) with a median age at Crohn’s diagnosis of 24.4 years (IQR 18. 0 – 33.5 years) who were followed up for a median of 83.0 months (IQR 44.0 – 119.3 months). The majority (n = 75) were diagnosed with Crohn’s prior to the onset of pCD. Most of the pCD (84.3%) was classified as complex fistulas as per the American Gastroenterological Association classification and was complicated by abscess at diagnosis (71.8%). The median time to biologic from fistula diagnosis was 11.0 months (IQR 4.0 – 36.0 months) with most receiving infliximab (68.9%), followed by adalimumab (29.1%) and ustekinumab (3.9%) as the initial biologic drug. 11 patients developed a fistula while on biologic therapy. A 50% reduction in fistula drainage was achieved in 90.4% of patients, however only 62.6% had sustained clinical or radiological healing. Increasing number of fistulae at diagnosis (OR 0.440, 95% CI 0.341 – 0.852, p = 0.008), and increased number of abscesses (OR 0.625, 95% CI 0.421 – 0.930, p = 0.02) were associated with reduced fistula healing (see figure 1). There was a trend towards reduced fistula healing with active smoking (OR 0.395, 95% CI 0.132 – 1.188, p = 0.098) but this was not significant.
Reference
1. Braithwaite, G.C., et al., Prognostic factors affecting outcomes in fistulating perianal Crohn's disease: a systematic review. Tech Coloproctol, 2017. 21(7): p. 501-519.
466
Efficacy of combination vedolizumab and upadacitinib treatment in refractory inflammatory bowel disease: a case series
Ei Phyu Phyu Swe1, Robert Gilmore1,2, Amrutha Murali1, Amirah Etchegaray1, Richard Fernandes1,2, Yoon-kyo An1,2 and Jakob Begun1,2
1Department of Gastroenterology, Mater Hospital, Brisbane, Australia;2Mater Research Institute, University of Queensland, South Brisbane, Australia
Background and Aim: Inflammatory bowel disease (IBD) is characterized by chronic inflammation of the gastrointestinal tract and encompasses both Ulcerative Colitis (UC) and Crohn’s disease (CD). Refractory cases, where available medical therapy fails, often necessitate surgical intervention. In cases where therapy with a single advanced drug therapy (ADT) fails, a combination of ADTs may be required to obtain maximal efficacy. We describe the use of a novel combination therapy involving upadacitinib and vedolizumab for the management of IBD refractory to ADT.
Methods: Twelve IBD patients who received upadacitinib in combination with vedolizumab were identified at an Australian tertiary IBD Centre. Clinical data for the 6 months following initiation of therapy was collected including patient reported outcomes, biochemical data, intestinal ultrasound (IUS) results, and endoscopic disease activities.
Results: Our study included 12 patients, 5 having UC and 7 having CD. The mean age was 41, with a male predominance (10 patients). Patient had been previously exposed to a median of 3 ADTs (range 2-5), with 9 out of 12 (75%) patients experiencing failure to at least 2 previous ADTs. Before initiating combination therapy, patients had objective evidence of disease activity including elevated inflammatory markers (C reactive protein, faecal calprotectin), as well as disease activity on IUS. 3 patients were on concomitant steroids at the time of dual ADT initiation. After 8 weeks of combination therapy, 5 patients (42%) achieved clinical remission (3 UC and 2 CD), and 4 patients (33%) achieved biochemical remission (1 UC, 3 CD). Eight patients continued combination therapy; 2 patients continued upadacitinib monotherapy, one patient continued vedolizumab monotherapy, and one patient switched to Infliximab. No adverse events were reported. After 16 weeks, 10 patients (83%) achieved clinical remission (4 UC and 6 CD), and 8 patients (66%) achieved biochemical and IUS remission (2 UC and 6 CD). One patient with UC underwent colectomy. Two patients continued combination therapy beyond 16 weeks, with 4 patients continuing vedolizumab monotherapy and 4 continuing upadacitinib monotherapy (Table). After 6 months follow-up, among 5 UC patients, 1 underwent colectomy, and 2 transitioned to Infliximab monotherapy. One patient initially achieved remission after 16 weeks of combination therapy but experienced symptom flare on vedolizumab monotherapy, necessitating upadacitinib re-initiation. One UC patient maintained clinical, biochemical, and intestinal ultrasound remission on upadacitinib monotherapy at 6 months. Among the 7 CD patients, 6 were in comprehensive remission at 6 months, while one patient had ongoing active disease despite 6 months of combination therapy. Of those achieving remission - 2 patients had 8 weeks of combination therapy, 3 had 16 weeks, with one experiencing flare on upadacitinib monotherapy necessitating vedolizumab re-initiation, and one patient required 6 months of combination therapy. Two patients reported adverse events (acne and shingles).
467
The impact of female sex in persistence of advanced therapies in Crohn’s disease and ulcerative colitis: Real-world data from Persistence Australian National Inflammatory bowel disease Cohort (PANIC) registry
Ryan Chang-ho Choi2,3, John Chetwood2,3, Aviv Pudipeddi2,3, Yanna Ko2,3, Thanaboon Chaemsupaphan2,3, Fei Yang Pan1, Viraj Kariyawasam4, Sudarshan Paramsothy2,3 and Rupert Leong1,2,3
1Macquarie University Hospital, Macquarie University, Sydney, Australia;2Concord Repatriation General Hospital, Sydney, Australia;3University of Sydney, Concord, Australia;4Blacktown and Mount Druitt Hospital, Sydney, Australia
Background and Aim: The impact of sex on the persistence of advanced therapies (ATs) in inflammatory bowel disease (IBD) is not well understood. This study aimed to examine the association between female sex and the persistence of ATs in AT-naïve and AT-exposed patients with Crohn’s disease (CD) and ulcerative colitis (UC).
Methods: We analysed the Persistence in Australian National IBD Cohort (PANIC), the largest, prospectively collected national registry database that contains 100% of all AT data in Australia from the only public funder, the Pharmaceutical Benefits Scheme (PBS). Non-persistence was defined as failure to dispense prescriptions ≥6 months from the preceding treatment or changing to an alternate AT for an IBD indication. Kaplan-Meier curve and Cox regression were used to calculate hazard ratios (HR) with 95% confidence intervals (CI), with P-value <0.05 deemed statically significant.
Results: From Jan 2007 to Dec 2021, 28,758 patients (13,951 males, 48.6%) underwent 46,765 lines of ATs, totaling 102,897 patient-years of follow-up. The time to 50% loss of steroid-free persistence was 36 months (95% confidence interval (CI), 35-37 months). In AT-naïve CD, younger females (age <45 years) had significantly poorer infliximab (IFX; HR, 0.70; 95% CI, 0.64-0.76; P<0.001) or adalimumab (ADA; HR, 0.77; 95% CI, 0.71-0.83; P=0.001; Table 1) persistence, compared with males. Similarly, AT-naïve older females (age ≥45 years) with CD had poorer IFX (HR, 0.83; 95% CI, 0.74-0.92; P<0.001) and ADA persistence (HR, 0.91; 95% CI, 0.83-0.99; P=0.033) compared with males. In AT-exposed CD patients however, female sex had no significant impact on TNFi persistence compared with males, regardless of the age (Table 1). Interestingly, younger females (age <45) had significantly lower ustekinumab (UST) persistence in both AT-naïve (HR, 0.64; 95% CI, 0.47-0.88; P=0.006) and AT-exposed CD (HR, 0.79; 95% CI, 0.65-0.95; P=0.014), compared with males. In contrast, older females (age ≥45) with CD had similar UST persistence compared with males, regardless of the AT-exposure status (Table 1). Female sex did not influence the persistence of vedolizumab (VED) in CD regardless of AT-exposure status (Table 1). Lastly, in both AT-naïve and AT-exposed patients with UC, female sex had no significant impact on the persistence of TNFi or VED (Table 1).
Conclusion: In the largest prospective population-based registry with all PBS-dispensed ATs for IBD, female sex was a risk factor for poorer TNFi persistence in AT-naïve CD and UST persistence in younger patients (age <45), regardless of the AT-exposure status. Female sex did not influence the persistence of VED in CD or any ATs in UC. Whilst further studies are required to understand the reasons behind these observations, gender-based persistence outcomes are a key area to further explore.
470
Assessment of adherence to postoperative ileocolonic resection guidelines and impact on early endoscopic recurrence in Crohn's disease: A multicenter Australian retrospective study
Adam Haig2,5, Pradeep Kakkadasam Ramaswamy2, Crystal Seng3, Deloshaan Subhaharan2, Lei Lin3, Zhen Hong4, Gareth Walker4, Lauren White1, Desmond Patrick1, Asif Shahzad4, David Clark3 and Waled Mohsen2
1Sunshine Coast University Hospital, Birtinya, Australia;2Gold Coast University Hospital, Southport, Australia;3Royal Brisbane and Women's Hospital, Brisbane, Australia;4Logan Hospital, Meadowbrook, Australia;5Griffith University, Southport, Australia
Background and Aim: Recent studies have demonstrated the efficacy of ileocolonic resection in the treatment of ileal Crohn’s disease (CD). Stratification based on risk of recurrence is current standard of care, with international guidelines recommending prophylaxis to high-risk patients. Existing data indicate suboptimal adherence to these guidelines, potentially leading to increased healthcare costs. This study aimed to evaluate (1) guideline adherence in the postoperative setting, and (2) the impact of guideline driven prophylaxis on post-operative endoscopic recurrence (POR).
Methods: We performed a retrospective cohort study of patients who underwent ileal or ileocolonic resection and anastomosis for CD between 2017 and 2021 in four Australian centres. Adherence to three specific guideline aspects was assessed: (1) colonoscopy within 12 months, (2) documentation of a Rutgeert’s score at colonoscopy, and (3) prophylactic therapy prescription in high-risk patients. High-risk patients were defined as those with one or more of the following risk factors for recurrence: postoperative smoking, prior CD-related intestinal resection, presence of penetrating or perianal disease, or presence of granulomas in the resection specimen. Early POR (defined as a Rutgeert’s score of ≥ i2 within 12 months of surgery) was assessed; if this was not documented, it was inferred from the report text and available images.
Results: A total of 180 patients were analysed, with a median age of 46 years, and of whom 55% were female. Disease was confined to the ileum in 59% of patients, and 18% had additional perianal involvement. Disease behaviour was stricturing in 66% and penetrating in 30%. 32% of the cohort had undergone prior ileocolonic resection, and 25% were smokers.122 (68%) underwent colonoscopy within 12 months, and 162 (90%) had a colonoscopy during the follow-up period (median 240 days, IQR: 174 – 402 days). A Rutgeert’s score was documented in 89/162 (55%). Of the 142 (79%) patients with at least one risk factor for recurrence, 98 (69%) received prophylactic therapy. Early POR occurred in 54 of 122 patients (44%) who underwent timely colonoscopy (high-risk group 43/94, 46%; low-risk group 11/28, 39%, p = 0.55). Prophylactic therapy in the high-risk group did not reduce early POR (28/62, 45% vs 15/32, 47%, p = 0.87).
Conclusion: Adherence to guidelines in the management of postoperative Crohn’s is suboptimal, particularly in the documentation of a Rutgeert’s score. Irrespective of prophylactic therapy prescription in our cohort, early POR remains high, and guideline driven prophylaxis did not significantly reduce this rate. Additionally, recurrence was still high in patients without traditional risk factors for recurrence. This invites further investigation into alternative risk-stratification and treatment strategies to reduce POR in Crohn’s disease.
477
Platelet albumin ratio predicts inflammatory bowel disease over infection in patients presenting with acute diarrhoea
Kathryn Gazelakis1, Kyle Williams2,3, Isabel Chu1,3, Alex Boussioutas1,3, Sally Bell2,3, David Gibson1, Peter Gibson1,3, Gregory Moore2,3, Miles P Sparrow1,3 and Mark Ward1,3
1Department of Gastroenterology, Alfred Health, Melbourne, Australia;2Department of Gastroenterology, Monash Health, Melbourne, Australia;3Monash University, Melbourne, Australia
Background and Aim: Differentiating between infectious gastroenteritis and a flare of inflammatory bowel disease (IBD) in patients admitted with diarrhoea can be challenging, and is important, as the management differs significantly. We previously described a model, based on the platelet count, serum albumin, duration of diarrhoea and the presence of blood in faeces: 1.42 (platelet:albumin ratio) + 1.28 (duration diarrhoea in days) + 6.54 (blood in faeces=1, no blood=0). The performance of the model that predicted IBD flare is shown in Figure 1. The aim of the present study was to validate this model in an external cohort.
Methods: We included patients admitted with acute diarrhoea at a single tertiary centre (not involved with the inception cohort) between January 2000 and December 2018. Inclusion criteria were infective gastroenteritis or IBD flare, using hospital coding. Our model was tested on the validation cohort by calculating its performance using sensitivity, specificity, positive and negative predictive value.
Results: The validation cohort comprised 851 cases, median age 44 [IQR 29-66], 56% female). 486 (56%) had IBD (188 Crohn’s Disease, 291 Ulcerative Colitis, 7 IBD-unclassified) and 365 (43%) infection (pathogen proven in 51%). The inception cohort was younger (median age 35 vs 44 years) and a pathogen was identified less often (16%), but other characteristics were similar. Rates of thrombocytosis (17 vs 15%) and median platelet counts were similar (278 vs 277x109/L) between the cohorts. Applying the previously determined cut-off value of 21.4 above which IBD was diagnosed, the model on the validation cohort yielded a sensitivity of 95%, specificity of 88%, with a positive predictive value of 91% and negative predictive value of 93%.
Conclusion: We have demonstrated that a simple model incorporating four easy-to-obtain data points (platelet count, albumin, number of days of diarrhoea and presence/absence of blood in faeces) can accurately differentiate a flare of IBD from infectious diarrhoea in patients presenting to hospital with acute diarrhoea.
478
Introduction of a multidisciplinary inflammatory bowel disease service in regional Australia: Evaluating the impact of the 2016 Crohn's and Colitis Australia inflammatory bowel disease audit on service provision and patient care in a regional centre
Daniel Saitta1, Daniel Yee Lee Ng1,2, James Lopez1,2, Chloda Sainsbury1, Jaycen Cruickshank1, Jong Chin1, Maree Pekin1, Sharon Wallace1, Paul Riley1, Carolyn Vasey1, James Ross1, Mathew Jacob1,2, Sarah Ryan1, Bruce Stewart1, Sajith Kattiparambil Gangadharan1 and Timothy Elliott1
1Grampians Health Ballarat, Ballarat, Australia;2Deakin University, Burwood, 3125
Background and Aim: Inflammatory bowel disease (IBD) is increasing in prevalence in Australian and patients with IBD benefit from multidisciplinary care. The 2016 Crohns’ & Colitis Australia IBD audit report (1) identified shortcomings in provision of IBD services across Australia. The audit noted only 1% of all hospitals had a full IBD service and 24% had a partial IBD service as detailed in the 2016 Crohn’s and Colitis Australia IBD standards of care (2). No regional or rural site met either partial or full IBD service criteria (1). The report provided 13 priority recommendations for improving IBD service provision, 12 of which are relevant to local sites. The aim of this study was to report on the development of an IBD service in a regional centre, with reference to the previously mentioned IBD audit recommendations and standards.
Methods: We undertook a review of our regional IBD service in 2017 against the 2016 IBD standards. After evaluating where our service fell short of these standards, we planned and implemented key elements of an IBD service as guided by the National IBD audit recommendations over the subsequent 5 years.
Results: Prior to the 2016 IBD audit recommendations, our regional centre only had partial compliance with 50% of the 2016 IBD standards. Since the audit, we have implemented 10/12 of national IBD audit recommendations. There was an improvement seen at our site in 18/26 (69%) of these standards. This increased our compliance with 2015 Australian IBD standards to partially meet 80% of standards. Over the 6 years since the audit, a multidisciplinary IBD service has been developed which includes a lead gastroenterologist with IBD expertise, 3 other gastroenterologists, 2 colorectal surgeons, 2 surgeons with an interest in IBD, a 1.0 FTE dedicated IBD nurse, IBD dietitian, stoma nurse and nominated radiologists and pathologists servicing both public and private patients in the region. Four weekly IBD multidisciplinary meetings incorporating these clinicians was established to discuss complex cases and review emerging literature. Over this period, our specialised radiologists have established an intestinal ultrasound service, occurring monthly and on an ad hoc basis in the private sector. A Monday- Friday nurse lead IBD phone and email help line was also established to provide patients a point of contact with the service as required. As of June 2024, this regional IBD service cares for 131 patients on biologic therapy including 28 on escalated/compassionate doses. 185 patients have had their management discussed in the IBD MDM since the establishment of the service in Sept 2020 until June 2024. An audit of a database of the first 12 months of calls to the IBD service help line demonstrated there was a minimum of 109 individual patient contacts. A review of the documentation surrounding those patient contacts, demonstrates assistance with a large range of patient issues including ensuring valid prescriptions and timely access to investigations, to recognition of disease flares and facilitating timely medical advice for peripartum counselling.
Conclusion: To our knowledge, our site represents the first regional IBD service to meet requirements for a partial IBD service. The 2016 Australian IBD audit recommendations provided the stimulus for this positive change.
References
1. Final report of the first audit of the organisation and provision of IBD services in Australia 2016. Crohn’s & Colitis Australia; 2016.
2. Australian IBD standards: standards of healthcare for people with inflammatory bowel disease in Australia. Crohn’s & Colitis Australia; 2016.
479
Co-existence of ulcerative colitis and Crohn’s phenotype with non-healing perianal fistula: a case report
Introduction: Inflammatory Bowel Diseases (IBD) are chronic intestinal disorder characterised by an abnormal immune response. The two main types of IBD are Ulcerative colitis (UC) and Crohn’s disease (CD). UC is typically restricted to colonic mucosa in a continuous and circumferential pattern. CD can form skip lesions, affecting any part of the gastrointestinal tract, and often lead to transmural inflammation and fistula formation. The presence of a fistula in a UC patient contradicts our current understanding of IBD. Here we present a case of UC that developed a non-healing perianal fistula.
Case report: A 42-year-old man presented with a new diagnosis of acute severe UC in June 2019. He failed to respond to intravenous corticosteroids and required an emergency subtotal colectomy. Histopathology analysis confirmed the diagnosis of UC. The patient initially had an ileostomy formed with subsequent reversal and J-Pouch formation. This was complicated by an anastomotic leak and the development of new perianal fistulising disease, managed with surgical drainage and seton placement. From 2020 to 2023, his perianal fistula (Figure 1A) required multiple drainage and surgical interventions. Despite extensive efforts by the surgical team, his perianal fistula persisted. Clinical suspicion for a CD diagnosis arose during evaluation under anaesthesia (EUA) when the internal opening was found just above the sphincter. Further restaging with MR Bowel imaging illustrated a short tract with the internal location in the same location (Figure 1B), suggesting a CD-related aetiology. The patient began Infliximab therapy, resulting in decreased fistula discharge, further supporting the Crohn’s phenotype diagnosis. However, the non-healing perianal fistula persisted. This consensus from a multidisciplinary team involving Colorectal and Gastroenterology specialists was to continue infliximab ensuring good therapeutic levels for six months. Given the focus on his quality of life, the patient is considering ileostomy and pouch excision. His therapy was switched to subcutaneous infliximab 120mg fortnightly due to poor intravenous access, with a review scheduled to discuss pouch excision and permanent end ileostomy for the aforementioned reasons.
492
Post operative recurrence and surgical outcomes following Crohn’s ileocolic resections in Australia (PORSCIA study)
Hugh Giddings1,2,3,4, Kheng-Seong Ng1,2,4,5, Michael Solomon1,2,3,4, Arteen Arzivian6, Craig Haifer6, Huiyu Lin5,7, Christian Pappas8, David Clark8,9,10, Anthony Deacon10,11, Graham Radford-Smith10,11, Nargus Ebrahimi1, Ann Wu12, Mark Lewis12, Roscoe Lim6, Jennifer Zhang13, Abhinav Vasudevan13, Kathryn Demase14, Jadon Karp14, Miles P Sparrow14, Richard Fernandes15, Yoon-kyo An15, Zi Qin Ng16, Scott Mackenzie16, Lena Thin17, Tessa Greeve18, Gregory Moore18 and Simon Ghaly6 and Australia and New Zealand Inflammatory Bowel Disease Consortium, Crohn’s Colitis Cure (CCCure)
1Department of Colorectal Surgery, Royal Prince Alfred Hospital, Camperdown, Sydney, Australia;2Surgical Outcomes Research Centre (SOuRCe), Royal Prince Alfred Hospital, Camperdown, Sydney, Australia;3Institute of Academic Surgery (IAS), Royal Prince Alfred Hospital, Camperdown, Sydney, Australia;4Faculty of Medicine and Health, The University of Sydney, Sydney, Australia;5Department of Colorectal Surgery, Concord Repatriation General Hospital, Sydney, Australia;6Department of Gastroenterology and Hepatology, St Vincent's Hospital, Darlinghurst, Sydney, Australia;7Department of Gastroenterology and Hepatology, Tan Hock Seng Hospital, Singapore;8Department of Surgery, St Vincent's Private Hospital Northside, Brisbane, Australia;9Department of Surgery, Royal Brisbane and Women's Hospital, Brisbane, Australia;10Faculty of Medicine and Health, University of Queensland, Brisbane, Australia;11Department of Gastroenterology and Hepatology, Royal Brisbane and Women's Hospital, Brisbane, Australia;12Department of Colorectal Surgery, Royal Adelaide Hospital, Adelaide, Australia;13Department of Gastroenterology, Eastern Health, Box Hill, Australia;14Department of Gastroenterology, Alfred Health, Melbourne, Australia;15Department of Gastroenterology, Mater Hospital, Brisbane, Australia;16Department of Colorectal Surgery, Liverpool Hospital, Sydney, Australia;17Department of Gastroenterology, Fiona Stanley Hospital, Australia;18Department of Gastroenterology, Monash Health, Australia
Background and Aim: Ileocolic resections (ICR) are the most commonly performed resections for Crohn’s disease (CD). There is ongoing debate about the impact of anastomotic technique on the risk of post operative recurrence (POR). Historical control groups have often been used for statistical comparison, usually with temporal bias. The aims of this study were to: (i) report contemporary rates of POR secondary to CD requiring repeat surgery (surgical recurrence at anastomosis [SR-ICR], or at any site [SR-any]) and the rates of endoscopic recurrence (ER) in the ‘biologic era’; and (ii) determine risk factors for SR.
Methods: A retrospective multicentre study involving twelve tertiary Australian centres was performed. Patients were identified from local databases or the Crohn’s Colitis Care Clinical Quality Registry (CQR), and included if they had undergone an ICR for CD from 2007 onwards. Demographic, medical and surgical data were collected by chart review. Endoscopic images were centrally read and scored using the modified Rutgeerts score. Cox proportional hazards modelling was used to evaluate clinico-pathological risk factors for SR-ICR. Accepted risk factors for POR (smoking, penetrating disease [B3], or previous resection), and other variables with P<0.10 on univariable analyses, were included in the multivariable model.
Results: A total of 911 patients underwent an ICR between 2007 and 2023 (mean 39.1yrs [SD 15.3], 52% F, 59.6% </=40 years [A1/2], 53.9% stricturing [B2], 60.4% ileal [L1], 18.9% perianal disease, 28.9% smokers, 26.0% had previous intestinal surgery for CD). The median follow-up duration was 63.7 months (IQR 24.5-107.0). A stapled side-to-side anti-peristaltic anastomosis was performed in 439 (56.1%), handsewn end-to-end in 169 (21.6%), other stapled in 121 (15.5%), other handsewn in 30 (3.8%), and Kono-S in 24 (3.1%). In patients with at least 2-years of follow up medication data, immunomodulator monotherapy was used in 31.6%, and biologic/advanced therapy in 55.2%. At least one endoscopy was captured during follow up in 690 patients (75.7%) and 91.5% of these had sufficient data for central reading. Early (i.e. within 18 months) ER (mRutgeerts score >/=i2b) occurred in 23.5%. This increased to 31.7% at any stage during follow up. Rates of SR-ICR in patients with restoration of GIT continuity (n=875) were 4.5% (95%CI 2.8-6.1) and 12.8% (95%CI 8.8-16.5) at 5- and 10-years, respectively. Rates of SR-any were 5.9% (95%CI 4.1-7.7) and 15.5% (95%CI 11.4-19.3) at 5- and 10-years, respectively. On multivariable analysis, smoking (aHR 3.49 [95%CI 1.93-6.29] was the only factor significantly associated with SR-ICR. Anastomotic technique was not associated with surgical recurrence. Prophylactic immunomodulator or biologic/advanced therapy use (within 3 months of ICR), or use of biologic/advanced therapy at any time beyond 3 months, did not significantly influence the hazards of SR-ICR.
Conclusion: The overall rate of surgical recurrence at the ileocolic anastomosis in this large Australian cohort was low, recorded to be one in twenty at 5 years. Smoking, rather than anastomotic technique, remains the strongest risk factor. This data will help inform patients and clinicians about the risk of recurrence and aid in providing a clear reference point for comparison in future studies.
507
Tracking bile acids and the impact of split dosing thiopurine on severity of intrahepatic cholestasis of pregnancy in a patient with Crohn’s colitis
Daniel Saitta1, David Langsford1,2, Timothy Elliott1 and Sajith Kattiparambil Gangadharan1
1Grampians Health Ballarat, Ballarat, Australia;2University of Melbourne, Parkville, Australia
Introduction: Inflammatory bowel disease impacts a younger demographic of patients with a slight female predominance. Ensuring reproductive health of this cohort of patients is essential for both foetal and maternal health. Severe Intrahepatic cholestasis of pregnancy (ICP) characterised by total serum bile acid (TSBA) > 100umol/L is associated with an increased stillbirth risk, foetal defects and meconium aspiration (1). Despite being listed as safe in pregnancy, emerging data suggests patients exposed to thiopurines may be at increased risk of ICP (1,2). Unique features of this case is the timeline of azathioprine dosing demonstrating a correlation with fall in TSBA and improvement in liver function tests supporting theory that thiopurines may directly impact TSBA metabolism / excretion. This also adds to the limited literature about the use of a split dosing strategy to mitigate the impact of thiopurine shunting in IBD and ICP.
Case report: A 34 year old female G1P0 27+3/40 was found to have a 7 week history of pruritus and jaundice at follow up with her gastroenterologist. She has a background of colonic crohns with disease in remission on azathioprine 200mg daily at time of presentation. Her bilirubin was 162umol/L, AST 65U/L, ALT 54U/L, GGT 24U/L at initial presentation. Coagulation, viral, autoimmune liver, urine and liver and foetal ultrasound studies were normal. She was diagnosed with severe ICP after noting significantly elevated TSBA (117umol/L). Her pregnancy was further complicated by gestational diabetes mellitus. Ursodeoxycholic acid was inefficacious in improving clinical (itch) or biochemical parameters. Thiopurine metabolites ratio (6 MMP:TGN) was 34 at 12/40, and 21 at 27/40. Cessation of azathioprine precipitated a TSBA fall to 31umol/L within 7 days. Recommencement of azathioprine with a split dosing strategy (50mg BD) at 29/40 led to increase in TSBA to 89umol/L. Azathioprine was again ceased at 30/40 and TSBA, bilirubin and symptoms resolved without any additional intervention. Her crohn’s disease remained in clinically and biochemically in remission. A plan has been made for delivery between 35 and 36 weeks and data on outcomes will be available at time of presentation.
Discussion: A retrospective UK cohort (n = 386 pregnancies) demonstrated an increased incidence of ICP (3.9%) in patients with IBD accounted for by thiopurine exposure (2). This has been reinforced by a 2024 Australian prospective cohort (n= 131) demonstrating thiopurine shunting (MMP:TGN > 11) being associated with ICP. Furthermore, this Australian cohort also demonstrated a trend of increasing thiopurine shunting as pregnancy progressed (1). Split dosing has been suggested as potential strategy to mitigate this effect, however only a few cases have been recorded with mixed results (1).
Conclusion: Thiopurine use may increase risk of ICP development, however their use for patients with inflammatory bowel disease is common in pregnancy and currently generally deemed safe by majority of guidelines. Spilt dosing is an appealing strategy given ease of implementation, however unfortunately our case does not support its efficacy. Prospective research is warranted to understand how best to manage IBD and ICP in context of thiopurine use.
References
1. Prentice, R, Flanagan, E, Wright, E, Prideaux, L, Connell, W, Sparrow, M, et al. Thiopurine metabolite shunting in late pregnancy increases the risk of intrahepatic cholestasis of pregnancy in women with inflammatory bowel disease, and can be managed with split-dosing. Journal of Crohn’s and Colitis. 2024; jjae023.
2. Selinger, CP, Rosiou, K, Broglio, G, Lever, G, Chiu, CM, Stocker, LJ, et al. Antenatal thiopurine exposure in women with IBD is associated with intrahepatic cholestasis of pregnancy. Expert Opinion on Drug Safety.2023Nov 2; 22(11): 1091–7.
510
Evaluating the impact of anti-tumour necrosis factor and small molecules therapy on depression and anxiety for inflammatory bowel disease patients
Irwin Kashani, Reme Mountifield, Alex Barnes and Arduino Mangoni
Flinders Hospital, Adelaide, Bedford Park, Australia
Background and Aim: Depression and anxiety are common in patients with inflammatory bowel disease (IBD). There has been investigation into the influence of anti-tumour necrosis factor (TNF) biologics on depression and anxiety in patients with and without IBD, with longitudinal studies and small randomized controlled trials showing conflicting results. We performed an analysis of the relationship between anti-TNF biologics and small molecule therapies on depression and anxiety in patients with IBD.
Methods: An online questionnaire was administered through IBD clinics at Flinders Medical Centre, South Australia. Data on IBD activity (Simple Clinical Colitis Activity Index and Harvey–Bradshaw Index), IBD, Medical history including previous mental illness, smoking history, surgical history, family history, demographics, and IBD medication were recorded. Depression was assessed with Patient Health Questionnaire 9 (PHQ9), with clinically significant depression defined as PHQ9 score >15. Anxiety was assessed with the General Anxiety Disorder-7 (GAD-7) Questionnaire, with definition of mild anxiety (5-9), moderate anxiety (10-14) and severe anxiety (15-21). Inadequate completion of any score or index led to that result not being included.
Results: Our preliminary data included 220 responses to the online questionnaire, with 106 from patients with Crohn's disease, 56 from patients with ulcerative colitis, 12 from patients with indeterminate colitis. The median age of respondents was 44 years (IQR), 63% female, and median duration of IBD) was 12 years (IQR). Of the participants, 65 reported having previous depression or anxiety as a past medical history diagnosis. Clinically significant depression was observed in 20.8% of the cohort, with 17.6% experiencing moderate to severe anxiety and 21.4% reporting mild anxiety. Anti-TNF therapy was used by 34.3% (n=72) of participants, while small molecule therapy (Tofacitinib or Upadacitinib) was used by 10.5% (n=22). Table 1 gives a breakdown of the results of our preliminary analysis. Neither the IBD type nor the active disease variable ( p=0.28) was a significant predictor of clinical severe depression in this dataset. In addition neither the IBD type nor the active disease variable was a significant predictor of mild anxiety or moderate-severe anxiety in this dataset. In patients with Crohn's disease, 34.3% had active disease (defined as a value of 5 or greater), compared to 20.0% of patients with indeterminate colitis and 25.9% of patients with ulcerative colitis. Notably, among patients with Crohn's disease, the rate of clinically significant depression in those using small molecule therapies was 57% (n=4/7) compared to 18% (n=17/92) in non-users (OR: 5.88 (P=0.016)). The rate of moderate to severe anxiety among small molecule therapy users was 19% (n=4/21) compared to 21% (n=31/145) in non-users (P=0.807), and the rate of mild anxiety was 42% (n=9/21) compared to 23% (n=34/145) in non-users (OR: 2.45 (P=0.058)). In ulcerative colitis, the rate of mild anxiety among small molecule therapy users was 50% (n=7/14) compared to 20% (n=8/40) in non-users OR: 4.00 (P=0.031). Clinically significant depression and moderate-severe anxiety were associated with female sex (P=0.036 and P=0.009, respectively), but not with previous surgery for IBD (P=0.338). There was no difference in the anti-TNF/small molecule and non-anti-TNF/small molecule groups for any of these variables.
Conclusion: Our study indicates a trend towards higher rates of mild anxiety among anti-TNF users but no significant association with depression or anxiety. However, small molecule therapy, particularly in Crohn's disease, was linked to a higher prevalence of clinically significant depression and mild anxiety. We acknowledge that the numbers in our preliminary are small for each therapy and that disease activity information would be very important to address as a confounder which we will address and reanalysis in our larger data set. Further research is warranted to elucidate the mechanisms underlying these associations and guide clinical management.
512
Immune-mediated colitis treated with tofacitinib
Lloyd Cresswell, James Lavender and Lay Theng Gan
Hunter New England Health, Newcastle, Australia
Introduction: Immune-mediated colitis is a challenging complication in patients receiving immunotherapy. Effective management is crucial, particularly when standard treatments fail, and surgery is the only option. Tofacitinib, a Janus kinase (JAK) inhibitor, is not currently listed in the treatment of immune-mediated colitis, though case studies have shown some efficacy. This study evaluates the efficacy of tofacitinib in treating immune-mediated colitis secondary to ipilimumab and nivolumab, for treatment of metastatic melanoma, in a patient refractory to infliximab who was not suitable for operative management.
Case report: A case study of a melanoma patient on immunotherapy who developed severe immune-mediated colitis. The patient failed infliximab rescue therapy and subsequently was administered tofacitinib at a dosage of 10 mg three times daily (TDS). The patient showed significant clinical improvement following the initiation of tofacitinib therapy. Symptoms of colitis, including abdominal pain and diarrhea, were markedly reduced, leading to an overall enhancement in disease control quality of life. No adverse effects related to tofacitinib were observed during the treatment period.
Conclusion: Tofacitinib at 10 mg TDS demonstrated effectiveness in treating immune-mediated colitis in a patient who did not respond to infliximab and was not eligible for surgical intervention. These findings suggest that tofacitinib may be a viable alternative treatment for similar cases, providing a new therapeutic avenue for managing this severe condition in melanoma patients undergoing immunotherapy.
513
An Australian cost-utility analysis of ferric derisomaltose versus ferric carboxymaltose in patients with inflammatory bowel disease: implications of incorporating fracture incidence
Alhossain Khalafallah1, Sean Abel2 and Richard Pollock3
1Specialist Care Australia, Launceston, Australia;2A. Menarini Australia Pty Ltd, Chatswood, Australia;3Covalence Research Ltd, Harpenden, United Kingdom
Background and Aim: Anaemia is a common extraintestinal manifestation of inflammatory bowel disease (IBD), most commonly caused by iron deficiency. Intravenous (IV) iron is the preferred treatment in patients with IBD and iron deficiency anaemia (IDA) unresponsive to or intolerant of oral iron, and in patients with ongoing significant bleeding, malabsorption due to gastrointestinal disease. A recent randomised controlled trial (RCT) showed that ferric carboxymaltose (FCM), a high-dose, rapid-infusion IV iron, is associated with significantly elevated risk and severity of hypophosphataemia versus ferric derisomaltose (FDI) in patients with IBD and IDA. Emerging data suggest that FCM-treated patients are also at elevated risk of fractures. The aim was to evaluate the cost-utility of FDI versus FCM in Australia, capturing differences in posology and safety.
Methods: Parametric models of fracture-free survival were derived from 110 patients treated with FDI and 179 patients treated with FCM. The best-fitting model was incorporated into a published patient-level simulation model, and the model was adapted to the Australian setting with costs of iron and iron administration, fracture treatment, and IV phosphate from the AR-DRG system. Disease-related quality of life (QoL) was modelled based on the PHOSPHARE-IBD RCT, and disutilities associated with IV iron administration and fractures were obtained from the literature. Analyses were conducted over 10 years and future costs and effects were discounted at 5% annually.
Results: Over 10 years, total costs with FCM were AUD 15,007 versus AUD 10,526 with FDI (Figure 1A). The difference in the IV iron administrations required was the largest driver of cost differences at AUD 13,275 with FCM (14.2 infusions/patient) versus AUD 10,402 with FDI (11.1 infusions/patient), followed by hypophosphataemia management costs. Fracture treatment contributed AUD 451 to total FCM costs versus AUD 124 with FDI. Quality-adjusted life expectancy (QALE) was 0.148 quality-adjusted life years (QALYs) higher with FDI than FCM (4.572 QALYs versus 4.424 QALYs), with 77.8% of the difference attributable to disease-related QoL, 13.7% to differences in fracture incidence, and 8.5% to IV iron administration (Figure 1B).
514
Intestinal ultrasound supports safety in a clinic for functional gastrointestinal disorders
Damjana Bogatic1,2,3, Ryan M Mathias2,3, Robert Bryant1,3, Alice Day1,3 and Samantha Plush2,3
1Inflammatory Bowel Disease Service, The Queen Elizabeth Hospital, Woodville South, Australia;2Faculty of Health Sciences, School of Medicine, University of Adelaide, Adelaide, Australia;3Basil Hetzel Institute for Translational Research, Woodville South, Australia
Introduction: The increasing burden of functional gastrointestinal disorders (FGID) has led to the development of specialised FGID clinics around Australia. Intestinal ultrasound (IUS) is a validated tool to assess inflammatory bowel disease and is gaining momentum in the assessment of FGID, to non-invasively and cost-effectively exclude organic pathology. IUS has been shown to increase patient engagement and awareness of their medical condition and this can be applied to patients with FGID. A multidisciplinary FGID clinic was established in South Australia to facilitate rapid review of low-risk patients with likely FGID. Risk reduction was accomplished with point of care IUS (POCUS) performed by a gastroenterologist.
Case report: A twenty-four-year-old female was referred to the FGID clinic for abdominal symptoms. She reported two years of alternating diarrhoea and constipation associated with abdominal pain without per rectal blood or red flag symptoms. Review was expedited from a gastroenterology waitlist to a dietitian-led FGID clinic integrated with a gastroenterologist and POCUS. Despite a provisional label of FGID in primary care, POCUS revealed active inflammation over a long segment of the terminal ileum (15cm) with long stretches of increased colour doppler signal that extended to the mesentery, absent wall stratification, and bowel wall thickness of 6.4mm; colonic segments were normal. Further investigations revealed markedly elevated inflammatory markers and deficiencies in iron and vitamin D. The patient proceeded to colonoscopy which showed moderate diffuse inflammation in the terminal ileum (8cm), characterised by linear ulcers, cobblestoning, oedema and loss of vascularity, with a skip lesion (SES-CD score 6) (Image 1). The ileocaecal valve was ulcerated and congested, and the colon was normal. Histology was consistent with chronic active ileitis. The patient was commenced on azathioprine and a weaning course of budesonide, with management initiated within three weeks of initial contact. Based on symptoms and risk factors documented in the referral, without a dedicated FGID clinic, the patient would have fallen into a category 2 triage with a protracted wait time for review.
516
Renal granulomatosis in Crohn's disease: A rare case report and discussion
Leshni Pillay, Weilun Gao, Jonathan Segal and Britt Christensen and Finlay Macrae
Royal Melbourne Hospital, Melbourne, Australia
Introduction: Crohn’s disease (CD) is a complex immune-mediated inflammatory disorder affecting the gastrointestinal tract (GIT). Although CD-associated granulomas are most commonly found within the GIT, they may also manifest in extra intestinal locations. We illustrate a case of a rare instance of renal granuloma secondary to CD and discuss an effective treatment approach as well as present a summary of previously reported case studies.
Case report: An 18-year-old male presented to his GP with a one-year history of abdominal pain. Medical history included treated gastrointestinal helminthiasis, giardiasis, and lactose intolerance, with no significant family history. Physical examination was unremarkable. Laboratory findings revealed elevated white cell count, increased erythrocyte sedimentation rate, and renal dysfunction. He was referred to a nephrologist, who noted additional symptoms of diarrhoea and occasional rectal bleeding. There was no significant improvement in symptoms or renal function following the cessation of a non-steroidal anti-inflammatory drug. Renal biopsy confirmed acute interstitial nephritis with a single granuloma, prompting referral to a gastroenterologist to rule out CD or sarcoidosis. Colonoscopy and biopsies confirmed CD. Fecal calprotectin levels were elevated. Further investigations excluded autoimmune disease, tuberculosis, and sarcoidosis as causes of renal impairment. Treatment involved steroid tapering followed by intravenous infliximab induction and maintenance therapy with subcutaneous injections fortnightly. Renal function and gastrointestinal symptoms improved with infliximab monotherapy, although dose escalation to weekly infliximab injections was required at seven months due to loss of response from subcutaneous infliximab. At one year, colonoscopy showed endoscopic remission, with ongoing improvement in renal function (creatinine decreased from 194 to 154 μmol/L) and resolution of pyuria. Table 1 shows a summary of previously reported case studies of renal granulomatosis in CD.
517
Systematic review and meta-analysis: impact of anti-tumor necrosis factor and small molecule therapy on depression and anxiety in inflammatory bowel disease patients
Irwin Kashani, Reme Mountifield, Alex Barnes and Arduino Mangoni
Flinders Hospital, Adelaide, Bedford Park, Australia
Background: Depression and anxiety are common comorbidities in patients with inflammatory bowel disease (IBD). Anti-tumor necrosis factor (TNF) biologics and small molecule therapies have been used to manage IBD, but their impact on depression and anxiety remains unclear.
Aims: This systematic review and meta-analysis aim to evaluate the impact of anti-TNF biologics and small molecule therapies on depression and anxiety in patients with IBD.
Methods: A comprehensive literature search will be conducted in PubMed, EMBASE, and Cochrane Library to identify relevant studies using JBI system. Studies reporting on the impact of anti-TNF biologics and small molecule therapies on depression and anxiety in IBD patients will be included. Data will be extracted, and a meta-analysis will be performed using random-effects models to estimate pooled effect sizes.
Results: Preliminary results will be presented, including the number of studies identified, study characteristics, and summary estimates of the impact of anti-TNF biologics and small molecule therapies on depression and anxiety in IBD patients. Subgroup analyses will be conducted based on type of therapy, IBD subtype, and other relevant factors.
Conclusion: This systematic review and meta-analysis will provide a comprehensive evaluation of the impact of anti-TNF biologics and small molecule therapies on depression and anxiety in patients with IBD. The findings will help guide clinical practice and future research in this area. Full analysis will be presented at congress.
518
Quality of bowel preparation in pouchoscopies
Cheng-Yu (Lina) Chen1, Waled Mohsen1, ShuYan Edwin Wong1 and Mark Jones2
1Gold Coast University Hospital, Southport, Australia;2Bond University, Robina, Australia
Background: Pouchoscopy is a minimally invasive endoscopic procedure used to examine the ileal-anal pouch for patients who have previously undergone total proctocolectomy (TPC) with ileal pouch-anal anastomosis (IPAA). This has become the surgical procedure of choice for ulcerative colitis (UC) and familial adenomatous polyposis (FAP). Pouchoscopies are routinely used to aid in the diagnosis of pouch disorders such as chronic pouchitis. Whilst there are well established society guidelines in optimizing bowel preparation for colonoscopies, unfortunately there remains a paucity of data and guidance with regards to pouchoscopies. The quality of the bowel preparation is an essential factor in the safety, diagnostic accuracy, difficulty, and speed of the examination.
Aim: The aim of this retrospective study is to review the quality of bowel preparation for patients who have undergone pouchoscopies based on administration of oral preparation, rectal preparation, both or none.
Methods: Retrospective data was collected from pouchoscopy reports at the Gold Coast University Hospital during 3-year period between 2020 to 2022. Patients included in this cohort are all above the age of 18 and would have undergone previous total proctocolectomy and J-pouch formation with history of either inflammatory bowel disease or familial adenomatous polyposis. Bowel preparation was graded using a quality score, scaled from 1 to 4, where 1 = poor, 2 = adequate, 3 = good and 4 = excellent. “Poor” refers to solid or semisolid debris that cannot be cleared effectively. “Fair” refers to collections of semisolid debris that are cleared with difficulty. “Good” was used to describe no or minimal solid stool with large amounts of clear fluid that require suctioning. “Excellent” defined as no or minimal solid stool and only small amounts of clear fluid that require suctioning. Patients were administered oral preparation (PO), rectal preparation (PR), both or none. The main confounding variable identified was mucosal inflammation and consequently coded as either yes or no based on presence or absence of inflammation. Linear regression was conducted to investigate the relationship between type of bowel preparation (exposure) and quality of preparation (outcome) after adjusting for inflammation status (confounder). To check the validity of the linear regression method, residuals were assessed for normal distribution and outliers. Analysis was conducted in SAS On Demand for Academics.
Results: Data from 189 pouchoscopies were collected; 52 of which the quality of bowel preparation was not reported and thus not included in the statistical analysis. Only one patient received both oral and rectal preparation and was also excluded from the study. Of the remaining 136 pouchoscopies, total of 49 patients received no bowel preparation, 11 received oral preparation, and 76 received rectal preparation. Results from the linear regression analysis show that after adjusting for inflammation, the average quality score is 1.9 for patients with no bowel preparation, meaning they had “adequate” bowel preparation quality. The quality score is higher for patients who received oral preparation by 0.65 on average (p value <0.05), and patients who received rectal preparation by 0.51 on average (p value <0.05), implicating they had “good” bowel preparation quality upon examination.
Conclusion: Patients who received bowel preparation had higher quality scores compared to those who received no bowel prep. In addition, those who received oral preparation had better quality scores than those who received rectal preparation. Larger and prospective studies are needed to establish guidelines on the type and volume of preparation that would result in optimising the highest quality preparation for pouchoscopies in the future.
521
A case of progressive multifocal leukoencephalopathy in a patient receiving infliximab and methotrexate for Crohn’s disease
Bassem Ibrahim
Nepean Blue Mountains Local Health District, Kingswood, Australia
Introduction: Progressive multifocal leukoencephalopathy (PML) is a rare demyelinating disorder of the central nervous system characterised by the reactivation of the JC virus (JCV). It is often associated with significant immunocompromised states and caries a poor prognosis. PML has been described in patients with underlying malignancies, HIV infection, autoimmune disorders, immunosuppression following organ transplantation and those on various immunomodulatory and monoclonal antibody therapies. The association between PML and therapies like natalizumab (anti-integrin inhibitor) have been well documented. Only a handful of case reports have noted PML in patients on infliximab and in all these cases the patient was concurrently on methotrexate and the underlying condition was rheumatoid arthritis. Here we report a case of progressive multifocal leukoencephalopathy in a patient receiving infliximab and methotrexate for Crohn’s disease. To date there appears to be no published cases of PML in patients receiving infliximab for inflammatory bowel disease.
Case Report: A 73-year-old female with a long-standing history of complex fistulising Crohn’s disease, on infliximab, methotrexate and sulfasalazine, presented to emergency department with a 3-day subacute onset of dysarthria and left-sided facial droop. A CT of the brain showed a hypodense area in the right posterior parietal white matter. An MRI was arranged as an outpatient which showed an abnormal high T2/FLAIR signal in the right frontotemporal white matter crossing the midline through the corpus callosum with some possible regions of enhancement. Outpatient neurology and neurosurgery reviews were arranged. Over the subsequent two to three weeks the patient developed progressive neurological deficits including left upper limb weakness, visual and sensory neglect, ataxic gait and headaches. The patient represented to ED three weeks following the first presentation and was admitted for further workup. A repeat MRI brain was performed during the admission which showed stable appearance of the confluent T2/FLAIR hyperintensity in the right frontoparietal white matter with extension to the splenium and left parietal white matter. There was no abnormal enhancement and no evidence of diffusion restriction. Overall picture was suggestive of leukoencephalopathy rather than glial neoplasm and given the history of anti-TNF therapy the possibility of PML was raised. A lumber puncture was subsequently performed, and PCR for JC virus was positive on CSF. A diagnosis of PML was made. Immunomodulatory therapies, which had been withheld since the admission, were ceased. Referral to palliative care services were made and the patient was subsequently discharged into residential aged care.
Conclusion: Here we present the only PML is a rare but serious complication of immunosuppression. While rarely seen in the inflammatory bowel disease population, it is important to consider in patients who are receiving concurrent immunomodulators or in those who have other risk factors for JC virus reactivation.
526
Safety and efficacy of thioguanine as an alternative to traditional thiopurines in maintaining remission in inflammatory bowel disease: a single-centre retrospective study
Gurtej Singh, Leshni Pillay, Stephanie Dimovski and Jonathan Segal
Royal Melbourne Hospital, Melbourne, Australia
Background and Aim: Traditional thiopurines demonstrate efficacy in maintaining remission in both Crohn’s disease and ulcerative colitis. Nevertheless, approximately half of patients exhibit intolerance or lack of response to these treatments. Thioguanine (TG) is an alternative thiopurine which is effective in inflammatory bowel diseases (IBD) as well offers a valuable option for managing specific side effects commonly linked with conventional thiopurines, such as pancreatitis. We aim to demonstrate the safety data on thioguanine in this retrospective, single centre, cohort study.
Methods: A retrospective, single centre study was performed in IBD patients who failed prior treatment with conventional thiopurines (irrespective of being of advanced therapies such as biologics) and were subsequently treated with TG. Clinical response to TG as well as TG failure and adverse events were recorded.
Results: A total of 13 patients were included (Females 54 %, Males 46%). Nine patients had Crohn’s disease (CD) and 4 patients had ulcerative colitis (UC). Median follow up was 16.2 months. The median dose of TG was 20 mg a day (range: 20 mg- 40 mg/day). Ten patients were on concurrent biologic therapy (Infliximab = 10, Adalimumab = 1). Seven patients (53%) were in clinical remission (3 on monotherapy and 4 on biologics). Three patients had adverse events on TG and TG was ceased in these cases [photosensitivity (1), skin cancer (1), headache and fevers (1)]. There was no recurrent pancreatitis in patients who had previous azathioprine related pancreatitis. Five patients had a mild transaminitis while one had a clinically significant increase > 2 ULN that normalised on repeat testing.
Conclusion: Overall TG was well tolerated in majority of patients either as monotherapy or as combination therapy with biologics. There was no recurrence of pancreatitis in patients with previous episodes of pancreatitis with Azathioprine. TG can be considered as an alternate option in patients with previous azathioprine related side effects either as monotherapy or combination therapy with biologics. Larger studies are needed to completely assess the adverse event profile of thioguanine.
532
Ustekinumab as salvage therapy for a flare of chronic ulcerative colitis in pregnancy: A case report
Alexander Connell1, Yadhavan Upendran1,2, Daniel Lightowler1,3, Sean Griffin1,2 and Crispin Corte1,2
1Royal Prince Alfred Hospital, Sydney, Australia;2Central Clinical School, University of Sydney, Sydney, Australia;3Medical School, University of Western Australia, Perth, Australia
Introduction: Acute severe ulcerative colitis presents a challenge of medical management during pregnancy. Typically, infliximab, cyclosporine and more recently JAK-inhibitors are used as rescue therapy for steroid-refractory severe colitis. We present a patient with a flare of chronic UC during pregnancy where ustekinumab was used as salvage therapy.
Case Report: A 30-year-old pregnant G1P0 woman was admitted to hospital at 25+4 weeks with bloody diarrhoea on a background of left-sided ulcerative colitis. She had been diagnosed at age 16 and was initially managed on mesalazine and azathioprine. She had her first episode of ASUC in 2019 when she failed to respond to cyclosporine and was subsequently salvaged with infliximab. She continued infliximab 8 weekly infusions for 18 months, before transitioning to infliximab fortnightly subcutaneous injections, which maintained her in clinical remission. At the time of conception, she was also in endoscopic and histologic remission. At 8 weeks gestation, she showed the first signs of relapse with blood in her stools. This progressed to a hospital admission at 13 weeks for moderate severity colitis. She responded to IV corticosteroids and her infliximab was dose escalated to 4 weekly 5mg/kg infusions. At 25+4 weeks, she was readmitted with > 10 episodes of bloody diarrhoea per day. Biochemistry showed albumin 27g/L, CRP 29.5, faecal calprotectin 8020 ug/g and supratherapeutic infliximab trough levels (20.90 ug/mL). Flexible sigmoidoscopy demonstrated Mayo 3 colitis (UCEIS 7) to the descending colon. C.difficile and CMV infection were excluded. There was early MDT involvement comprising Gastroenterology, Colorectal Surgery, O&G and Neonatology. She received IV corticosteroids and was given off-label IV ustekinumab at an induction dose of 520mg on day 2. Her condition improved and she was transitioned to oral steroids a week later. She subsequently had worsening symptoms and was recommenced on IV corticosteroids. She tolerated a step down to oral steroids 2 weeks later and has remained stable on a weaning regimen since. She was discharged with an elective caesarean section planned for 34 weeks gestation. Non-invasive monitoring ensured foetal health throughout, and the latest ultrasound at 32 weeks has demonstrated a healthy 1.8kg foetus.
Conclusion: Ulcerative colitis flares during pregnancy presents a complex medical scenario and early MDT involvement is essential. This case was particularly difficult as traditional salvage medical therapies had been previously exhausted. Ustekinumab was able to avoid emergent colectomy and ultimately delay delivery to improve foetal outcomes.
535
Systematic review of primary endpoint changes in phase 3 randomised control trials of advanced treatments in ulcerative colitis
Gurtej Singh, Leshni Pillay, Christine Lu, Jonathan Segal, Britt Christensen and Finlay Macrae
Royal Melbourne Hospital, Melbourne, Australia
Background and Aim: Endpoints in ulcerative colitis (UC) randomized controlled trials (RCTs) have been changing in published manuscripts. We performed a systematic review to capture the evolution of endpoint reporting in UC trials over time.
Methods: We searched the ClinicalTrials.gov through to 2024 for phase three RCTs of adult patients with UC on biologics and oral small molecules. We recorded all the endpoints for RCTs recorded in the trials. Primary endpoint (PEP) changes were defined as: (1) PEP reported as a secondary end point (SEP), (2) PEP omitted, (3) new PEP introduced, (4) change in the definition of the PEP. Endpoints were examined by two independent reviewers. The main outcome measured was change between the initially defined PEP and the PEP reported. This was assessed with: (1) tracking changes on ClinicalTrials.gov, (2) authors self-reporting changes in the manuscript, and (3) reported changes in the protocol. Baseline data was reported as the number (%) of mean ± SD or median (IQR). Categorical variables were summarised as frequencies with percentages.
Results: Analysis included a total of 3144 patients over 8 (100%) RCTs (4 induction, 7 maintenance trials). The most common endpoint reported in UC was Mayo Clinical score (3) and adopted Mayo score (3). Endoscopic endpoints were reported in 8 (100%) studies and were defined using mayo endoscopic score. Six studies (75%) reported histological healing using: Geoboes histology score, Nancy histology score, Laminal propria neutrophils and epithelial neutrophils subscore. Biomarkers were reported in 4 (50%) studies. Safety outcome was reported in 6 (75%) studies. Of the total 8 trials, no studies had PEP changes.
Conclusion: There is a concern with RCTs that changing PEP can be associated with trial positivity and hence has implications for validity of RCTs. However, our analysis of phase 3 trials searched on clinicaltrials.gov to date did not reveal any discrepancy between proposed and subsequently reported PEPs. Further larger metanalyses are needed to confirm this finding.
536
Immune checkpoint inhibitors and gastrointestinal complications: A case of granulomatous enteritis and bowel obstruction
William Wu and Brandon Baraty
Ryde Hospital, Eastwood, Australia
Introduction: Immune checkpoint inhibitors (ICIs) are increasingly used in the treatment of metastatic melanoma but can be associated with significant immune-related adverse events. This case highlights an unusual presentation of bowel obstruction potentially related to ICI-induced enteritis with granulomas, with differential diagnoses including Crohn's disease, sarcoidosis, tuberculosis, and granulomatous vasculitis.
Case Report: A 71-year-old female with a history of metastatic melanoma, previously treated with immune checkpoint inhibitors (nivolumab and ipilimumab), presented with symptoms of an acute small bowel obstruction. Treatment with ICIs had been discontinued several months earlier due to suspected ICI-related hepatitis for which she was treated with corticosteroids. Computed tomography demonstrated a transition point at the terminal ileum/ileocecal junction. She underwent emergency bowel resection with primary anastomosis. Histopathological examination of the resected bowel revealed cobblestoning of the ileum, an enterocolonic fistula, stricturing within the terminal ileum, mucosal ulceration, and a granuloma. The patient had experienced constipation in the months preceding her presentation which were attributed to opioid use for post-herpetic neuralgia. She reported no history of recurrent bowel symptoms prior to this and had never undergone endoscopic investigations. A CT scan of her abdomen 5 months prior had not shown any pathological activity at the ileum. Tuberculosis, vasculitidies and sarcoidosis tests have been normal.
Conclusion: This report features sequalae of ICI related granulomatous enteritis as the suspected aetiology underlying small bowel obstruction. This underscores the importance of considering ICI-induced granulomatous enteritis in patients with a history of immunotherapy for metastatic melanoma. The unusual presentation highlights the need for heightened clinical awareness and further research into the gastrointestinal sequelae of immune checkpoint inhibitors.
546
Systematic review of primary endpoint changes in phase 3 randomised controlled trials in advanced treatments in Crohn’s Disease
Leshni Pillay, Gurtej Singh, Christine Lu, Jonathan Segal, Britt Christensen and Finlay Macrae
Royal Melbourne Hospital, Melbourne, Australia
Background and Aim: Endpoints in Crohn’s disease (CD) randomized controlled trials (RCTs) have been changing. We performed a systematic review to capture the evolution of endpoint reporting in CD trials over time.
Methods: We searched the ClinicalTrials.gov through to May 2024 for phase three RCTs of adult patients with CD on biologics and oral small molecules. We recorded all the endpoints for RCTs recorded in the trials. Primary endpoint (PEP) changes were defined as: (1) PEP reported as a secondary end point (SEP), (2) PEP omitted, (3) new PEP introduced, (4) change in the definition of the PEP. Endpoints were examined by two independent reviewers. The main outcome measured was change between the initially defined PEP and the PEP reported. This was assessed with: (1) tracking changes on ClinicalTrials.gov, (2) authors self-reporting changes in the manuscript, and (3) reported changes in the protocol. Baseline data was reported as the number (%) of mean ± SD or median (IQR). Categorical variables were summarised as frequencies with percentages.
Results: Analysis included a total of 9197 patients over 18 RCTs (1 induction, 17 maintenance trials). The most common endpoint report in CD was CDAI (72%). Endoscopic endpoints were reported in 15 studies (83.3%) and were defined using SES-CD. Biomarkers were reported in 5 studies (27.8%). Safety outcome was reported in 15 studies (83.3%). Of the total 18 trials, 3 studies (16.7 %) had PEP changes. The PEP changes included: new PEP change (1 study), definition of PEP changes (1 study), > 1 PEP omitted (1 study). The statistical significance of this is uncertain due to the smaller cohort of studies assessed.
Conclusion: Changing PEP in CD can be associated with trial positivity and hence has implications for validity of RCTs. More extensive systematic review is needed to deduce the impact of PEP changes on CD RCTs.
551
Crohn's disease versus ileal tuberculosis in a patient with high risk epidemiology: a case report
Debapama Basu1,2, Kevin O'Callaghan1, Anna Brischetto1 and Adrian Swaine2
1Department of Infectious Diseases, Redcliffe Hospital, Redcliffe, Australia;2Department of Gastroenterology, Redcliffe Hospital, Redcliffe, Australia
Introduction: Distinguishing intestinal tuberculosis (ITB) from Crohn’s disease (CD) is often considered to be a diagnostic dilemma, due to their similar clinical presentations, endoscopic features, and histopathology. Australia has a low prevalence of tuberculosis (TB), but with global travel and immigration, there is a significant cohort with relevant epidemiology for TB exposure. Furthermore, there is increasing rates of CD in TB-endemic countries such as India and China. There is no established diagnostic criteria to definitively differentiate the two diseases at the index evaluation, in a patient with epidemiologic risk factors for TB. We report a case where trial of empiric anti-tuberculin therapy (ATT) was used to successfully differentiate ITB from CD.
Case Report: A 19-year-old Indian male presented with a four week history of nocturnal fevers, diarrhea and weight loss of 17 kg. He had immigrated to Australia 7 months prior, with unremarkable TB immigration screening. Laboratory results revealed microcytic anaemia, elevated C-reactive protein and a negative QuantiFERON Gold study. Faecal studies were positive for Giardia, with an elevated faecal calprotectin of 1600.
The patient remained febrile for seven days with ongoing abdominal pain and diarrhoea, despite treatment for Giardia. He developed aphthous ulcers and bilateral erythema nodosum during hospital admission, which further complicated the clinical differentiation. He proceeded to colonoscopy, which revealed diffuse severe inflammation in the distal ileum, characterised by granulomatous erosions and serpentine ulceration. Extensive laboratory testing for TB returned negative. In conjunction with the patient and his family, he was commenced on empiric four drug ATT. Within 48 hours of this, the patient’s fevers and frequency of bowel movements had resolved. Interval colonoscopy performed six weeks after initiation of ATT revealed mucosal healing. Based on this response to ATT, the clinical diagnosis was ITB. He subsequently completed six months of ATT and is now cured of ITB.
556
Janus kinase inhibitors for the management of acute severe ulcerative colitis: An Australian multicentre study
Robert Gilmore1,2, Richard Fernandes1,2, Deloshaan Subhaharan3, Waled Mohsen3, Lena Thin4, Simone Chin5, Danny Con5, Peter De Cruz5, Kathryn Demase6, Miles P Sparrow6, Sarah Lucas7, Mayur Garg7, Robert Bryant8, Jonathan Segal9, Britt Christensen9, Jakob Begun1,2 and Yoon-kyo An1,2
1Department of Gastroenterology, Mater Health, Brisbane, Australia;2Mater Research Institute, University of Queensland, Brisbane, Australia;3Department of Gastroenterology, Gold Coast University Hospital, Gold Coast, Australia;4Department of Gastroenterology, Fiona Stanley Hospital, Perth, Australia;5Department of Gastroenterology, Austin Health, Melbourne, Australia;6Department of Gastroenterology, Alfred Health, Melbourne, Australia;7Department of Gastroenterology, Northern Health, Melbourne, Australia;8Department of Gastroenterology, The Queen Elizabeth Hospital, Adelaide, Australia;9Department of Gastroenterology, The Royal Melbourne Hospital, Melbourne, Australia
Background: Acute Severe Ulcerative Colitis (ASUC) is a medical emergency, with limited therapeutic options available for medical management. Tofacitinib and Upadacitinib are novel Janus Kinase (JAK) inhibitors, with proven efficacy for ulcerative colitis (UC) in both clinical trial and real-world settings. This study aimed to examine the outcomes of patients treated with JAK inhibitors for ASUC in an Australian real-world population.
Methods: A retrospective multi-centre study was conducted including adult (≥17 years) patients with ASUC commenced on Tofacitinib or Upadacitinib from April 2022 to April 2024. ASUC was defined according to Truelove and Witt’s criteria. Demographic and clinical data were recorded at admission, JAK induction, discharge, week 8, week 16 and 1 year post-induction. The primary outcome was need for colectomy during inpatient admission, or at any time in the follow-up period. Secondary endpoints included clinical response to inpatient salvage therapy using modified Oxford criteria for ASUC (bowel opening <4/day and CRP <15) by day 3 of JAK induction, clinical remission, corticosteroid free clinical remission (CFCR), biochemical remission and rate of mucosal healing. ASUC was defined according to Truelove and Witt’s criteria. Clinical remission was defined using PRO2 definitions (STRIDE II guidelines). Biochemical remission was defined as CRP ≤5mg/dL and faecal calprotectin (FCP) result ≤150 μg/g. We further evaluated adverse events and drug-specific response.
Results: A total of 60 patients (50% female, median age 37 [range 16-69]) were included from 8 Australian Inflammatory Bowel Disease (IBD) centers. The majority were previously exposed to advanced drug therapy (ADT) (62%: IFX n=33, VDZ n=17, ADA n=5, UST n=4). 42% had prior admission with ASUC. Median baseline Mayo endoscopic subscore was 3 and UCEIS endoscopic score was 7. Tofacitinib salvage therapy was administered to 49% (29/60) of patients at a dose of 10mg TDS (25/29) or 10mg BD (4/29), while Upadacitnib salvage was given to 51% (31/60) at a dose of 45mg OD. 58% (35/60) of patients received JAK as first line medical salvage therapy, while 42% (25/60) received JAK salvage sequentially after failure of first line infliximab therapy during the same admission. The rate of colectomy during admission was 17% (10/60), 23% (14/60) by week 8, 28% (17/60) by week 16 and 40% (18/45) by 1 year. There was no significant difference between rate of colectomy during index admission (17% vs 16%, p=0.38), or up to 1 year post induction (42% vs 38%, p=0.24) between Tofacitinib and Upadacitinib salvage. There was a significantly increased risk of inpatient colectomy for those receiving sequential salvage therapy compared to initial JAK salvage (28% vs 9%, p=<0.01). However, there is no significant difference in the rate of colectomy in either cohort up to 1 year post induction (41% vs 38%, p=0.19). Clinical response was observed in 45% (27/60) of patients by day 3 of induction and 72% (43/60) by day 7. Clinical remission rates were 40% (24/60) by week 8 and 65% (39/60) by week 16. Biochemical remission was achieved in 51% (23/45) by week 16. Mucosal healing was achieved in 47% (14/30) of patients who underwent repeat endoscopy within 16 weeks of induction. Upon discharge, 88% (53/60) of patients were prescribed a weaning course of oral prednisolone. At week 8, 28% (15/53) remained on corticosteroid, which reduced to 2% (1/53) by week 16. CFCR was observed in 30% (16/53) of patients at week 8, and 61% (32/53) by week 16. Upon discharge, 13% of patients received a short course of enoxaparin for venous thromboembolism (VTE) prophylaxis. During their inpatient admission, 30% of patients were prescribed co-trimoxazole for pneumocystis jiroveci pneumonia (PJP) prophylaxis, with the majority continuing until their corticosteroid dose dropped below 20mg/day. Adverse events (excluding hospitalisation for subsequent colectomy) occurred in 11 patients (16%), all of which were minor and did not require hospitalisation. The most common events noted were acne (7%) and nasopharyngitis (6%). No venous thromboembolism, malignancy, systemic infection or cardiovascular events were observed.
Conclusion: This is the largest Australian study exploring the utilisation and outcomes of JAK inhibitors for ASUC. In a real-world setting, both Tofacitinib and Upadacitinib demonstrate effectiveness and safety in managing ASUC, with colectomy rates consistent with published Australian outcomes. There was no significant difference in the inpatient colectomy rate between Tofacitinib and Upadacitinib. There was a significantly higher rate of inpatient colectomy for patients requiring sequential salvage therapy, but no significance when patients were followed up to 1 year. There is variability in prescribing practice between dosage of Tofacitinib and Upadacitinib, duration and dosage of corticosteroid wean, and the use of prophylactic PJP and VTE prophylaxis.
558
The use of faecal calprotectin testing to inform management of patients with inflammatory bowel disease
Moshe Loebenstein1, Atul Shrestha1, Bowen Xia1, Georgia Sun1, Gregory Moore1,2 and Ray Boyapati1
1Department of Gastroenterology, Monash Health Melbourne, Australia;2School of Clinical Sciences, Monash University, Melbourne, Australia
Background and Aim: Faecal calprotectin (FC) serves as a sensitive biomarker of gastrointestinal inflammation. It has the benefits of being non-invasive, inexpensive and without risk of ionising radiation, allowing for routine monitoring and tight control of inflammation in patients with inflammatory bowel disease (IBD). The aim of this study was to describe the real-world use of FC and lower endoscopy for monitoring of IBD disease activity in a tertiary IBD centre where FC incurs no out-of-pocket cost to the patient.
Methods: All FC tests performed at our tertiary centre in the six-month period between 01/09/2022 and 30/03/2022 were identified and filtered to only consider those tests being performed for patients seen at least once in the IBD outpatient clinic. FC tests performed as an inpatient or in those without an established diagnosis of IBD were excluded. Demographic and clinical data were extracted from the medical record including age, gender, IBD subtype, duration and extent of disease, FC result and HBI or Partial Mayo score. Changes to patient’s management and subsequent investigations performed for monitoring of disease activity within 6 months of the FC result were identified. The data were analysed using Microsoft Excel and GraphPad Prism.
Results: A total of 240 unique patients with 367 FC results were available for analysis. 124 patients were female (51.7%), 196 tests (53%) were from patients with Crohn’s disease and 46% from those with ulcerative colitis. 55.3% of the FC results were <100, 19.3% between 100 and 250 and 25.3% >250. In asymptomatic patients (HBI=0 or Partial Mayo=0), the proportion of those having a lower endoscopy over the following 6 months was 3.5% (FC<100μg/g), 8.3% (FC 100μg/g - 250μg/g) and 28.6% (FC > 250μg/g); in symptomatic patients (HBI>0 or Partial Mayo>0), the proportions were 18.0% (FC<100μg/g), 24.4% (FC100μg/g -250μg/g) and 18.9% (FC>250μg/g). Asymptomatic patients were less likely to have a lower endoscopy compared to symptomatic patients in the following six months when the FC<100 μg/g (OR 0.17, p=0.0019) but not 100-250μg/g (OR 0.28, p=0.12), or FC>250μg/g. (OR 1.71, p=0.29). Of the FC results >250 μg/g where the patient did not have a lower endoscopy in the following 6 months, 13/25 (52.0%) asymptomatic patients and 23/47 (48.9%) symptomatic patients had an escalation in their IBD therapy during this period.
Conclusion: Colonoscopy was performed in a minority of patients following a FC test, irrespective of result. Escalation in IBD medical therapy based on FC results was common in both asymptomatic and symptomatic patients without the need for lower endoscopy. FC monitoring in IBD offers a safe, convenient and accurate means of disease monitoring with significant potential cost savings.
568
The utilisation of colonoscopy in IBD patients and the rates of macroscopic inflammation by indication
Kee Fong Loo1,2, Tejaspreet Ghataura2, Geraldine Laven-law2, Alex Barnes1,2, Erin Symonds1,2 and Reme Mountifield1,2
1Department of Gastroenterology, Flinders Medical Centre, Adelaide, Australia;2College of Medicine and Public Health, Flinders University, Adelaide, Australia
Background and Aim: Australia has one of the highest prevalences of inflammatory bowel disease (IBD) in the world which represents a significant burden on the healthcare system. The presence of inflammation not only impacts patient quality of life, but also affects the quality of surveillance colonoscopy which is conducted for colorectal cancer prevention. Our study aimed to evaluate the utilisation and compare the rates of macroscopic inflammation at colonoscopy in IBD patients by indication.
Methods: A retrospective audit of colonoscopies performed over a 12-month period in 2021 for IBD patients in a tertiary hospital was conducted. Data was extracted on patient baseline characteristics, indication for colonoscopy, referral source and presence of macroscopic inflammation for analysis. Statistical analysis was performed using Wilcoxon rank-sum, Pearson Chi-square tests and Fisher’s exact test.
Results: 180 patients were eligible for the study [median age 49 (IQR 37-60) years, 51% female, 53% Crohn’s disease (CD), 47% ulcerative colitis (UC)]. The majority of the patients were on no therapy/ drug holiday (42%), whereas 22%, 14%, 17%, 5% were taking 5-ASA, immunomodulator (IM), biologics therapy, and combination therapy (biologics + IM) respectively. The indications for colonoscopy were categorised into three groups- clinician suspected active disease/ symptoms (52%), raised fecal calprotectin (FCP) (5%), and colorectal cancer surveillance in IBD (43%). Referral sources were available in 136/180 patients. The IBD clinic was the primary referral source (70%), followed by general gastroenterology clinic (22%), South Australian ‘SCOOP’ surveillance program (5%), and surgeon (2%). FCP tests was performed in only 28% of the entire cohort. Macroscopic inflammation was identified in 78% (raised FCP group), 47% (clinician suspected active disease/ symptoms group), and 43% (surveillance group). IBD patients on no therapy/ drug holiday had the highest rate of macroscopic inflammation (41%), compared to other treatment group (5-ASA: 23%; biologics: 17%; IM: 12%; combination group: 6%). An outcome of macroscopic inflammation was not associated with the source of referral (p>0.05). Raised FCP (≥200 μg/g) was associated with macroscopic inflammation for all indications although not statistically significant (p= 0.2), likely limited by the small sample size.
Conclusion: The rate of macroscopic inflammation in IBD patients is relatively high when presenting for surveillance colonoscopy, with a similar rate to those presenting with suspected active disease/ symptoms. As this limits the effectiveness of surveillance colonoscopy, further work is needed to develop strategies to optimise risk stratification of IBD patients with active disease prior to booking surveillance colonoscopy.
570
Acute severe ulcerative colitis management under general medicine: A novel inpatient approach?
Negar Hajiannejad, Suresh Ponnusamy and Zixiang Lim
St John of God Midland Hospital, Perth, Australia
Background and Aim: Traditionally patients with ASUC are managed under the direct care of gastroenterology. However, in SJOG Midland hospital, they are managed by general physicians with close gastroenterologist input. In this study, we have individually assessed the intrahospital and post-admission outcomes of ASUC patients at SJOG Midland Hospital.
Methods: This was a retrospective study assessing ASUC admissions at SJOG Midland Hospital from November 2015 to August 2023. Patients aged 18 and above who either met the TrueLove and Witts or endoscopic UCEIS >6) criteria for ASUC were analysed. Demographics, time to corticosteroids (CSC), venous thromboembolism (VTE) prophylaxis, intrahospital management, intrahospital, post-admission complications, colectomies and readmission rates up to one-year post-index admission were assessed.
Results: 46 patients (62 admissions) were analysed. High-dose CSC were commenced within the first 4 and 24 hours of admission in 20.9% and 64% of the cases respectively, while VTE prophylaxis was commenced within the first 4 and 24 hours in only 14.5% and 53.2% respectively. No VTE was reported during the one-year follow-up period. On 14 admissions, patients were biologic-experienced (28.5% Vediluzimab,14.2% Adalimumab and 57.1% Infliximab). Rescue therapy (Infliximab) was required in 13 admissions (20.9%); 1/13 (1.6%) resulted in same-admission colectomy, and an additional 2/13 (3.2%) received colectomy within one year. Same-admission colectomy was required in 10 admissions (16%), of which 5 (50%) were biologic-experienced pre-admission. 9/10 required direct surgery or had contraindications for biologic rescue therapy. Only one admission in this 7-year period resulted in an intrahospital complication (perforated diverticulitis). Colectomy was required in an additional 11.5% of admissions within one-year post-index admission. No complications were reported during this period.
References
1. Sasidharan, S., et al., Fecal calprotectin is a predictor of need for rescue therapy in hospitalized severe colitis. Inflammatory Bowel Diseases, 2022. 28(12): p. 1833-1837.
2. Vuyyuru, S., et al., P550 Short and long-term outcomes after acute severe ulcerative colitis in adults: A 12 year Canadian experience in the post biologic era. Journal of Crohn's and Colitis, 2024. 18(Supplement_1): p. i1082-i1083.
3. Moore, A.C. and B. Bressler, Acute severe ulcerative colitis: the oxford criteria no longer predict in-hospital colectomy rates. Digestive Diseases and Sciences, 2020. 65: p. 576-580.
4. Cushing, K.C., et al., Sarcopenia is a novel predictor of the need for rescue therapy in hospitalized ulcerative colitis patients. Journal of Crohn's and Colitis, 2018. 12(9): p. 1036-1041.
5. Adams, A., et al., Early management of acute severe UC in the biologics era: development and international validation of a prognostic clinical index to predict steroid response. Gut, 2023. 72(3): p. 433-442.
6. Li, A., M. Coote, and L. Thin, Prevalence and risk factors for early medical and surgical complications following an admission for acute severe ulcerative colitis. Therapeutic Advances in Gastroenterology, 2023. 16: p. 17562848231215148.
7. De Cristofaro, E., et al., Long-term risk of colectomy in patients with severe ulcerative colitis responding to intravenous corticosteroids or infliximab. Journal of Clinical Medicine, 2022. 11(6): p. 1679.
8. Le Baut, G., et al., A scoring system to determine patients’ risk of colectomy within 1 year after hospital admission for acute severe ulcerative colitis. Clinical Gastroenterology and Hepatology, 2021. 19(8): p. 1602-1610. e1.
9. Bernardo, S., et al., Predicting the course of disease in hospitalized patients with acute severe ulcerative colitis. Inflammatory Bowel Diseases, 2019. 25(3): p. 541-546.
571
The effect of consumer disease related knowledge on medication beliefs and adherence in IBD
Laura Rocha, Alex Barnes and Reme Mountifield
SAHLN and Flinders University, Bedford Park, Australia
Background and Aim: Inflammatory Bowel Disease (IBD) is a chronic condition requiring long-term medication adherence for effective management. Consumer non-adherence remains a significant challenge, influenced by several factors that have been identified as predictors of medication non-adherence in IBD. The relationship with consumer disease-related knowledge remains unclear. This study aims to investigate the association between the knowledge of IBD among consumers, their beliefs about their medication, and medication adherence.
Methods: A survey of IBD clinic consumers at a quaternary IBD centre included demographic data, IBD type, treatment history, IBD knowledge assessed by the IBD-KNOW score, medication adherence assessed by the Medication Adherence Report Scale (MARS-5), and Beliefs about Medicines Questionnaire (BMQ). Statistical analyses examined relationships between IBD knowledge, adherence, and other factors. High IBD knowledge was defined as an IBD-KNOW score in the upper quartile.
Results: A total of 210 participants completed the survey, predominantly female (63.3%), with a median age of 43 years (IQR: 31-59), and a median of 10 years (IQR: 4-15.5) since IBD diagnosis. The majority had Crohn's Disease (CD) (50.5%). Treatment history showed 29.9% had undergone IBD surgery, and the medication regimen included biologics (56.67%), immunosuppressants (17.14%), 5-ASA (10.95%), and steroids (6.19%). Consumers had a moderate level of IBD knowledge with a mean IBD-KNOW score of 11.9 (SD=4.8). The IBD-KNOW score weakly correlated with their MARS-5 adherence score (r=0.2261, p=0.0034). Non-adherence was not associated with a difference in IBD-KNOW scores (p=0.125). IBD knowledge scores weakly correlated with belief in the necessity of medication and less concern over medication (r=0.1607, p=0.0487), and negatively correlated with perceived overuse (r=-0.1567, p=0.0522), and harm from medications (r=-0.2807, p=0.0004). Those with high IBD-KNOW scores had a greater perception of the necessity of medication (p=0.0472). A multivariate linear regression model was constructed for IBD-KNOW scores, with the final model including biologic therapy (Coef=2.007, 95% CI [0.654, 3.362], p=0.004), previous surgery for IBD (Coef=1.618, 95% CI [0.214, 3.022], p=0.024), and beliefs about medication harm (Coef=-0.438, 95% CI [-0.677, -0.199], p<0.001).
Conclusion: A consumer’s understanding of their IBD knowledge correlates with medication adherence. Consumers with higher levels of knowledge of their condition had stronger beliefs in the necessity of medication and less perceived harm and overuse. Predictors of higher IBD in a multivariate model included biological therapy, a history of IBD surgery and beliefs about medication harm. Understanding these dynamics can inform tailored interventions to enhance medication adherence and optimise disease management in clinical practice.
Table: Correlation Between IBD Knowledge Score and Medication Beliefs/Adherence
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
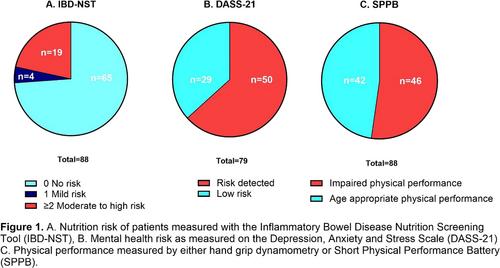
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


