Hubertus Himmerich, Johanna Louise Keeler, Kate Tchanturia, Janet Treasure
{"title":"神经性厌食症患者的治疗升级:环境、疗法和营养干预。","authors":"Hubertus Himmerich, Johanna Louise Keeler, Kate Tchanturia, Janet Treasure","doi":"10.1097/YCO.0000000000000964","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>Adult patients with severe anorexia nervosa often receive the same unsuccessful treatment without changes regarding the setting, the therapies, or nutritional interventions.</p><p><strong>Recent findings: </strong>Settings where people with anorexia nervosa are treated include their general practitioner, an independent psychiatric practice, a community mental health team (CMHT), a specialized eating disorder outpatient service, eating disorder early intervention services, a highly intensive eating disorder outpatient or home treatment programme, eating disorder daycare, an inpatient eating disorder service, a general hospital or a general psychiatric hospital, or residential treatment. At a specialized eating disorder service, patients should be offered evidence-based psychotherapy for anorexia nervosa, dietary advice and physical health monitoring as a first step. Additionally, they may be allocated to a specific treatment pathway, family interventions and creative therapies. As a second step, clinicians may consider integrating interventions targeting psychiatric or physical comorbidities, medication for anorexia nervosa or noninvasive neurostimulation. After several years of futile treatment, deep brain stimulation (DBS) should be considered to prevent a chronic course of anorexia nervosa. Nutritional interventions can be escalated from nutritional counselling to nasogastric tube feeding. Patients who rely on nasogastric tube feeding might benefit from percutaneous endoscopic gastrostomy (PEG). Patients who vomit despite a nasogastric tube, might need nasojejunal tube feeding.</p><p><strong>Summary: </strong>Treatment for people with anorexia nervosa should be regularly reviewed and, if necessary, escalated to avoid a chronic and longstanding disease course.</p>","PeriodicalId":11022,"journal":{"name":"Current Opinion in Psychiatry","volume":" ","pages":"404-416"},"PeriodicalIF":4.9000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11426991/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment escalation for people with anorexia nervosa: setting, therapies and nutritional interventions.\",\"authors\":\"Hubertus Himmerich, Johanna Louise Keeler, Kate Tchanturia, Janet Treasure\",\"doi\":\"10.1097/YCO.0000000000000964\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose of review: </strong>Adult patients with severe anorexia nervosa often receive the same unsuccessful treatment without changes regarding the setting, the therapies, or nutritional interventions.</p><p><strong>Recent findings: </strong>Settings where people with anorexia nervosa are treated include their general practitioner, an independent psychiatric practice, a community mental health team (CMHT), a specialized eating disorder outpatient service, eating disorder early intervention services, a highly intensive eating disorder outpatient or home treatment programme, eating disorder daycare, an inpatient eating disorder service, a general hospital or a general psychiatric hospital, or residential treatment. At a specialized eating disorder service, patients should be offered evidence-based psychotherapy for anorexia nervosa, dietary advice and physical health monitoring as a first step. Additionally, they may be allocated to a specific treatment pathway, family interventions and creative therapies. As a second step, clinicians may consider integrating interventions targeting psychiatric or physical comorbidities, medication for anorexia nervosa or noninvasive neurostimulation. After several years of futile treatment, deep brain stimulation (DBS) should be considered to prevent a chronic course of anorexia nervosa. Nutritional interventions can be escalated from nutritional counselling to nasogastric tube feeding. Patients who rely on nasogastric tube feeding might benefit from percutaneous endoscopic gastrostomy (PEG). Patients who vomit despite a nasogastric tube, might need nasojejunal tube feeding.</p><p><strong>Summary: </strong>Treatment for people with anorexia nervosa should be regularly reviewed and, if necessary, escalated to avoid a chronic and longstanding disease course.</p>\",\"PeriodicalId\":11022,\"journal\":{\"name\":\"Current Opinion in Psychiatry\",\"volume\":\" \",\"pages\":\"404-416\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11426991/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Opinion in Psychiatry\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/YCO.0000000000000964\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Opinion in Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/YCO.0000000000000964","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
Treatment escalation for people with anorexia nervosa: setting, therapies and nutritional interventions.
Purpose of review: Adult patients with severe anorexia nervosa often receive the same unsuccessful treatment without changes regarding the setting, the therapies, or nutritional interventions.
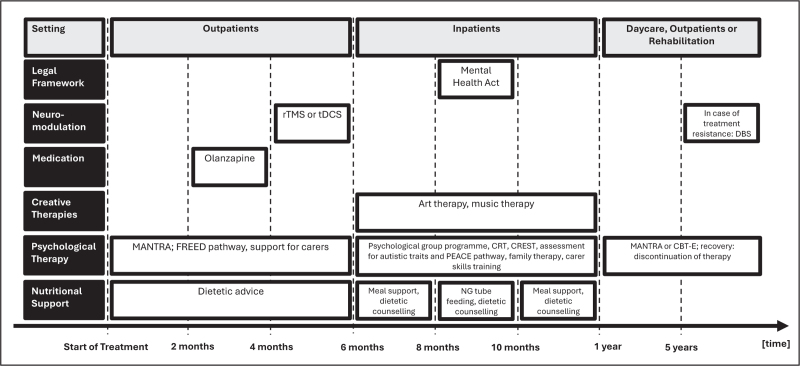
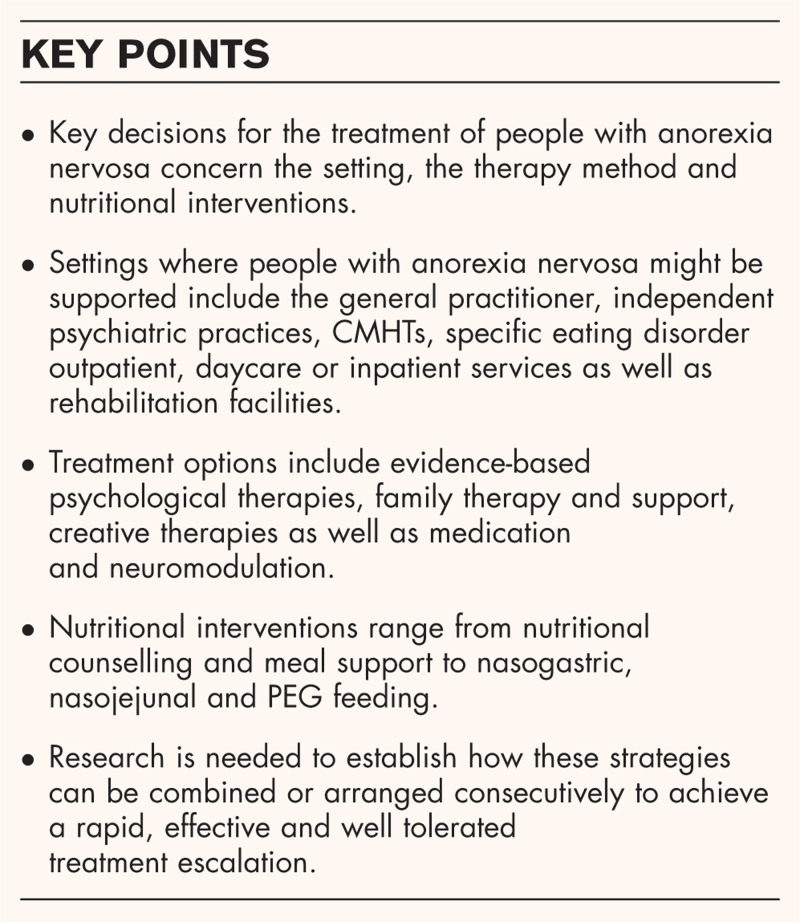
Recent findings: Settings where people with anorexia nervosa are treated include their general practitioner, an independent psychiatric practice, a community mental health team (CMHT), a specialized eating disorder outpatient service, eating disorder early intervention services, a highly intensive eating disorder outpatient or home treatment programme, eating disorder daycare, an inpatient eating disorder service, a general hospital or a general psychiatric hospital, or residential treatment. At a specialized eating disorder service, patients should be offered evidence-based psychotherapy for anorexia nervosa, dietary advice and physical health monitoring as a first step. Additionally, they may be allocated to a specific treatment pathway, family interventions and creative therapies. As a second step, clinicians may consider integrating interventions targeting psychiatric or physical comorbidities, medication for anorexia nervosa or noninvasive neurostimulation. After several years of futile treatment, deep brain stimulation (DBS) should be considered to prevent a chronic course of anorexia nervosa. Nutritional interventions can be escalated from nutritional counselling to nasogastric tube feeding. Patients who rely on nasogastric tube feeding might benefit from percutaneous endoscopic gastrostomy (PEG). Patients who vomit despite a nasogastric tube, might need nasojejunal tube feeding.
Summary: Treatment for people with anorexia nervosa should be regularly reviewed and, if necessary, escalated to avoid a chronic and longstanding disease course.
期刊介绍:
Current Opinion in Psychiatry is an easy-to-digest bimonthly journal covering the most interesting and important advances in the field of psychiatry. Eight sections on mental health disorders including schizophrenia, neurodevelopmental disorders and eating disorders, are presented alongside five area-specific sections, offering an expert evaluation on the most exciting developments in the field.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


