Quinten Verhalleman, Marc Miserez, Annouschka Laenen, Lawrence Bonne, Eveline Claus, Jo Peluso, Alexander Wilmer, Geert Maleux
{"title":"经导管动脉栓塞治疗小肠出血:技术和临床结果以及早期复发性出血的风险因素。","authors":"Quinten Verhalleman, Marc Miserez, Annouschka Laenen, Lawrence Bonne, Eveline Claus, Jo Peluso, Alexander Wilmer, Geert Maleux","doi":"10.20524/aog.2024.0903","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study evaluated the technical and clinical outcomes of transcatheter arterial embolization (TAE) in patients with acute small-bowel bleeding (SBB) and aimed to identify potential risk factors for early recurrent bleeding after TAE.</p><p><strong>Methods: </strong>Thirty-one patients with SBB managed with TAE between January 2006 and December 2021 were included. Technical and clinical success was defined as angiographic occlusion of the bleeding artery and disappearance of clinical or laboratory signs of persistent bleeding without major complications. Complications were classified according to the Society of Interventional Radiology's guidelines. Kaplan-Meier estimates assessed overall survival, and logistic regression models determined risk factors for clinical success and early rebleeding.</p><p><strong>Results: </strong>Technical and clinical success were achieved in 30/31 (97%) and 19 (61%), respectively. Early recurrent bleeding was present in 9 (29%) patients, and was treated by repeat embolization in 4 patients, conversion to surgery in 4, and comfort therapy in 1 patient. TAE-related small bowel ischemia requiring surgery was found in 2 (6.5%) patients. Thirty-day and in-hospital mortality were 19% (6/31) and 23% (7/31), respectively; overall 5-year estimated survival was 60%. Thrombocytopenia and elevated prothrombin time (PT)/activated partial thromboplastin time (aPTT) levels prior to TAE were identified as risk factors for clinical failure (P=0.0026 and P=0.027, respectively), and for residual or early recurrent bleeding (P<0.001 and P=0.01, respectively).</p><p><strong>Conclusions: </strong>TAE is safe and effective for managing severe SBB; however, early recurrent bleeding was found in nearly one third of patients. Thrombocytopenia and elevated PT/aPTT levels were risk factors for early recurrent bleeding.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 5","pages":"559-566"},"PeriodicalIF":2.2000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11372541/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transcatheter arterial embolization for small-bowel bleeding: technical and clinical outcomes and risk factors for early recurrent bleeding.\",\"authors\":\"Quinten Verhalleman, Marc Miserez, Annouschka Laenen, Lawrence Bonne, Eveline Claus, Jo Peluso, Alexander Wilmer, Geert Maleux\",\"doi\":\"10.20524/aog.2024.0903\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study evaluated the technical and clinical outcomes of transcatheter arterial embolization (TAE) in patients with acute small-bowel bleeding (SBB) and aimed to identify potential risk factors for early recurrent bleeding after TAE.</p><p><strong>Methods: </strong>Thirty-one patients with SBB managed with TAE between January 2006 and December 2021 were included. Technical and clinical success was defined as angiographic occlusion of the bleeding artery and disappearance of clinical or laboratory signs of persistent bleeding without major complications. Complications were classified according to the Society of Interventional Radiology's guidelines. Kaplan-Meier estimates assessed overall survival, and logistic regression models determined risk factors for clinical success and early rebleeding.</p><p><strong>Results: </strong>Technical and clinical success were achieved in 30/31 (97%) and 19 (61%), respectively. Early recurrent bleeding was present in 9 (29%) patients, and was treated by repeat embolization in 4 patients, conversion to surgery in 4, and comfort therapy in 1 patient. TAE-related small bowel ischemia requiring surgery was found in 2 (6.5%) patients. Thirty-day and in-hospital mortality were 19% (6/31) and 23% (7/31), respectively; overall 5-year estimated survival was 60%. Thrombocytopenia and elevated prothrombin time (PT)/activated partial thromboplastin time (aPTT) levels prior to TAE were identified as risk factors for clinical failure (P=0.0026 and P=0.027, respectively), and for residual or early recurrent bleeding (P<0.001 and P=0.01, respectively).</p><p><strong>Conclusions: </strong>TAE is safe and effective for managing severe SBB; however, early recurrent bleeding was found in nearly one third of patients. Thrombocytopenia and elevated PT/aPTT levels were risk factors for early recurrent bleeding.</p>\",\"PeriodicalId\":7978,\"journal\":{\"name\":\"Annals of Gastroenterology\",\"volume\":\"37 5\",\"pages\":\"559-566\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11372541/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20524/aog.2024.0903\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0903","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Transcatheter arterial embolization for small-bowel bleeding: technical and clinical outcomes and risk factors for early recurrent bleeding.
Background: This study evaluated the technical and clinical outcomes of transcatheter arterial embolization (TAE) in patients with acute small-bowel bleeding (SBB) and aimed to identify potential risk factors for early recurrent bleeding after TAE.
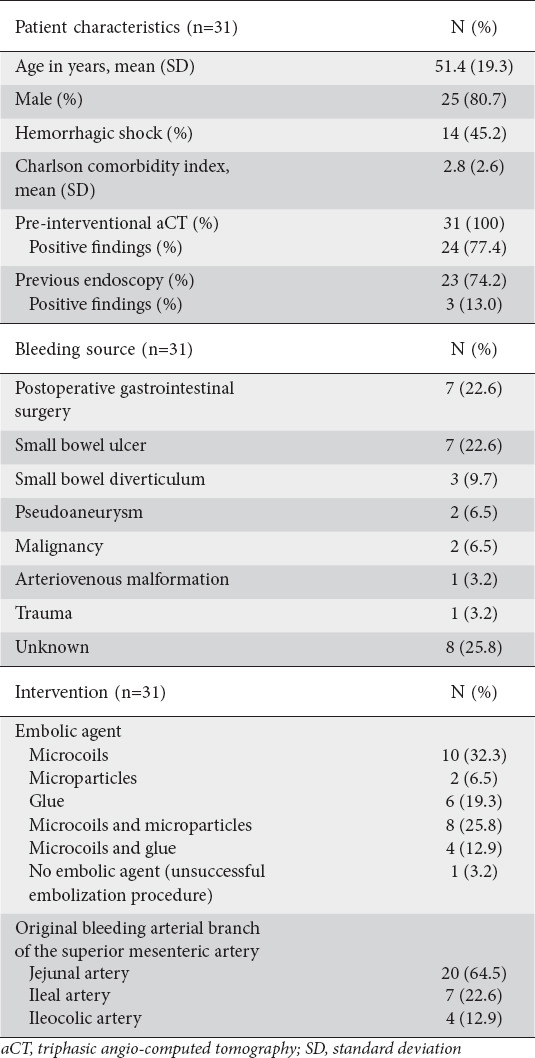
Methods: Thirty-one patients with SBB managed with TAE between January 2006 and December 2021 were included. Technical and clinical success was defined as angiographic occlusion of the bleeding artery and disappearance of clinical or laboratory signs of persistent bleeding without major complications. Complications were classified according to the Society of Interventional Radiology's guidelines. Kaplan-Meier estimates assessed overall survival, and logistic regression models determined risk factors for clinical success and early rebleeding.
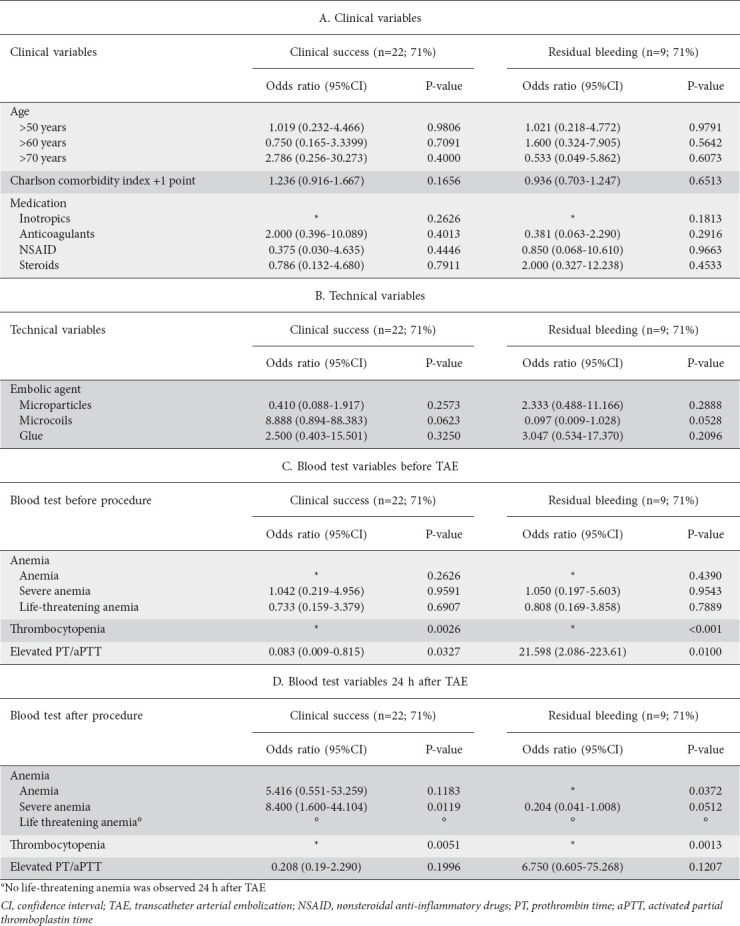
Results: Technical and clinical success were achieved in 30/31 (97%) and 19 (61%), respectively. Early recurrent bleeding was present in 9 (29%) patients, and was treated by repeat embolization in 4 patients, conversion to surgery in 4, and comfort therapy in 1 patient. TAE-related small bowel ischemia requiring surgery was found in 2 (6.5%) patients. Thirty-day and in-hospital mortality were 19% (6/31) and 23% (7/31), respectively; overall 5-year estimated survival was 60%. Thrombocytopenia and elevated prothrombin time (PT)/activated partial thromboplastin time (aPTT) levels prior to TAE were identified as risk factors for clinical failure (P=0.0026 and P=0.027, respectively), and for residual or early recurrent bleeding (P<0.001 and P=0.01, respectively).
Conclusions: TAE is safe and effective for managing severe SBB; however, early recurrent bleeding was found in nearly one third of patients. Thrombocytopenia and elevated PT/aPTT levels were risk factors for early recurrent bleeding.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


