Nai-Xin Zheng, Hu Ai, Ying Zhao, Hui Li, Guo-Jian Yang, Guo-Dong Tang, Xi Peng, Fu-Cheng Sun, Hui-Ping Zhang
{"title":"先前失败的尝试对后续慢性全闭塞经皮冠状动脉介入治疗结果的影响。","authors":"Nai-Xin Zheng, Hu Ai, Ying Zhao, Hui Li, Guo-Jian Yang, Guo-Dong Tang, Xi Peng, Fu-Cheng Sun, Hui-Ping Zhang","doi":"10.1002/agm2.12350","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objectives</h3>\n \n <p>Patients undergoing a prior failed attempt of chronic total occlusion-percutaneous coronary intervention (CTO-PCI) represent a challenging subgroup across all patients undergoing CTO-PCI. There are limited data on the effects of a prior failed attempt on the outcomes of subsequent CTO-PCI. We aimed to compare the procedural results and 24-month outcomes of prior-failed-attempt CTO-PCI with those of initial-attempt CTO-PCI.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients who underwent attempted CTO-PCI between January 2017 and December 2019 were prospectively enrolled. We analyzed the procedural results and 24-month major adverse cardiac events (MACE) between patients who underwent prior-failed-attempt and initial-attempt CTO-PCI. MACE was defined as a composite of cardiac death, target vessel-related myocardial infarction, and ischemia-driven target vessel revascularization (TVR) during follow-up.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In total, 484 patients who underwent CTO-PCI (prior-failed-attempt, <i>n</i> = 49; initial-attempt, <i>n</i> = 435) were enrolled during the study period. After propensity score matching (1:3), 147 patients were included in the initial-attempt group. The proportion of the Japanese-CTO (J-CTO) score ≥2 was higher in the patients who underwent prior failed attempt than in those who underwent initial attempt (77.5% vs. 38.8%, <i>p</i> < 0.001). The retrograde approach was more often adopted in the prior-failed-attempt group than in the initial-attempt group (32.7% vs. 3.4%, [<i>P</i>< 0.001). Successful CTO revascularization rates were significantly lower in the prior-failed attempt-group than in the initial attempt group (53.1% vs. 83.3%, <i>P</i> < 0.001). The multivariate analysis revealed that J-CTO score ≥2 [odds ratio (OR), 0.359; 95% confidence interval (CI), 0.159–0.812; <i>P</i> = 0.014], intravascular ultrasound procedure (OR, 4.640; 95% CI, 1.380–15.603; <i>P</i> = 0.013), and prior failed attempt (OR, 0.285; 95% CI, 0.125–0.648; <i>P</i> = 0.003) were the independent predictors for successful CTO revascularization. There were no significant differences in major procedural complications (2.0% vs. 0.7%, <i>p</i> = 0.438) and MACE rates (4.1% vs. 8.8%, <i>p</i> = 0.438) between the groups, mainly due to the TVR rate (4.1% vs. 8.2%, <i>P</i> = 0.522).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Compared with initial-attempt CTO-PCI, prior-failed-attempt CTO-PCI deserves more attention, since it is associated with a lower successful CTO revascularization rate. Prior failed attempt, J-CTO score ≥2, and IVUS procedure are the determining factors for predicting successful CTO revascularization. There are no significantly different unfavorable outcomes between patients who undergo prior-failed-attempt and initial-attempt CTO-PCI.</p>\n </section>\n </div>","PeriodicalId":32862,"journal":{"name":"Aging Medicine","volume":"7 4","pages":"463-471"},"PeriodicalIF":2.5000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11369334/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of a prior failed attempt on the outcomes of subsequent chronic total occlusion-percutaneous coronary intervention\",\"authors\":\"Nai-Xin Zheng, Hu Ai, Ying Zhao, Hui Li, Guo-Jian Yang, Guo-Dong Tang, Xi Peng, Fu-Cheng Sun, Hui-Ping Zhang\",\"doi\":\"10.1002/agm2.12350\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>Patients undergoing a prior failed attempt of chronic total occlusion-percutaneous coronary intervention (CTO-PCI) represent a challenging subgroup across all patients undergoing CTO-PCI. There are limited data on the effects of a prior failed attempt on the outcomes of subsequent CTO-PCI. We aimed to compare the procedural results and 24-month outcomes of prior-failed-attempt CTO-PCI with those of initial-attempt CTO-PCI.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Patients who underwent attempted CTO-PCI between January 2017 and December 2019 were prospectively enrolled. We analyzed the procedural results and 24-month major adverse cardiac events (MACE) between patients who underwent prior-failed-attempt and initial-attempt CTO-PCI. MACE was defined as a composite of cardiac death, target vessel-related myocardial infarction, and ischemia-driven target vessel revascularization (TVR) during follow-up.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>In total, 484 patients who underwent CTO-PCI (prior-failed-attempt, <i>n</i> = 49; initial-attempt, <i>n</i> = 435) were enrolled during the study period. After propensity score matching (1:3), 147 patients were included in the initial-attempt group. The proportion of the Japanese-CTO (J-CTO) score ≥2 was higher in the patients who underwent prior failed attempt than in those who underwent initial attempt (77.5% vs. 38.8%, <i>p</i> < 0.001). The retrograde approach was more often adopted in the prior-failed-attempt group than in the initial-attempt group (32.7% vs. 3.4%, [<i>P</i>< 0.001). Successful CTO revascularization rates were significantly lower in the prior-failed attempt-group than in the initial attempt group (53.1% vs. 83.3%, <i>P</i> < 0.001). The multivariate analysis revealed that J-CTO score ≥2 [odds ratio (OR), 0.359; 95% confidence interval (CI), 0.159–0.812; <i>P</i> = 0.014], intravascular ultrasound procedure (OR, 4.640; 95% CI, 1.380–15.603; <i>P</i> = 0.013), and prior failed attempt (OR, 0.285; 95% CI, 0.125–0.648; <i>P</i> = 0.003) were the independent predictors for successful CTO revascularization. There were no significant differences in major procedural complications (2.0% vs. 0.7%, <i>p</i> = 0.438) and MACE rates (4.1% vs. 8.8%, <i>p</i> = 0.438) between the groups, mainly due to the TVR rate (4.1% vs. 8.2%, <i>P</i> = 0.522).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Compared with initial-attempt CTO-PCI, prior-failed-attempt CTO-PCI deserves more attention, since it is associated with a lower successful CTO revascularization rate. Prior failed attempt, J-CTO score ≥2, and IVUS procedure are the determining factors for predicting successful CTO revascularization. There are no significantly different unfavorable outcomes between patients who undergo prior-failed-attempt and initial-attempt CTO-PCI.</p>\\n </section>\\n </div>\",\"PeriodicalId\":32862,\"journal\":{\"name\":\"Aging Medicine\",\"volume\":\"7 4\",\"pages\":\"463-471\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11369334/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Aging Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/agm2.12350\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Aging Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/agm2.12350","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:接受慢性全闭塞经皮冠状动脉介入治疗(CTO-PCI)的患者是所有接受 CTO-PCI 患者中具有挑战性的亚组。关于先前尝试失败对后续 CTO-PCI 结果的影响,目前的数据还很有限。我们旨在比较既往尝试CTO-PCI失败者与初次尝试CTO-PCI者的手术结果和24个月后的预后:我们前瞻性地纳入了2017年1月至2019年12月期间接受CTO-PCI尝试的患者。我们分析了之前尝试CTO-PCI失败的患者和首次尝试CTO-PCI的患者的手术结果和24个月的主要心脏不良事件(MACE)。MACE定义为随访期间心脏死亡、靶血管相关心肌梗死和缺血驱动的靶血管血运重建(TVR)的综合结果:在研究期间,共有484名患者接受了CTO-PCI(之前失败-尝试,49人;初始-尝试,435人)。经过倾向评分匹配(1:3)后,147 名患者被纳入初次尝试组。之前尝试失败的患者中日本-CTO(J-CTO)评分≥2分的比例高于首次尝试的患者(77.5% vs. 38.8%,PP P = 0.014),血管内超声程序(OR,4.640;95% CI,1.380-15.603;P = 0.013)和之前尝试失败的患者(OR,0.285;95% CI,0.125-0.648;P = 0.003)是成功进行CTO血管再通的独立预测因素。两组间主要手术并发症(2.0% vs. 0.7%,P = 0.438)和MACE发生率(4.1% vs. 8.8%,P = 0.438)无明显差异,主要是TVR发生率(4.1% vs. 8.2%,P = 0.522):结论:与初次尝试的 CTO-PCI 相比,先前失败尝试的 CTO-PCI 更值得关注,因为它与较低的 CTO 再血管化成功率相关。既往尝试失败、J-CTO 评分≥2 和 IVUS 手术是预测 CTO 血管再通成功率的决定性因素。既往尝试失败的患者与初次尝试 CTO-PCI 的患者的不良预后无明显差异。
Effects of a prior failed attempt on the outcomes of subsequent chronic total occlusion-percutaneous coronary intervention
Objectives
Patients undergoing a prior failed attempt of chronic total occlusion-percutaneous coronary intervention (CTO-PCI) represent a challenging subgroup across all patients undergoing CTO-PCI. There are limited data on the effects of a prior failed attempt on the outcomes of subsequent CTO-PCI. We aimed to compare the procedural results and 24-month outcomes of prior-failed-attempt CTO-PCI with those of initial-attempt CTO-PCI.
Methods
Patients who underwent attempted CTO-PCI between January 2017 and December 2019 were prospectively enrolled. We analyzed the procedural results and 24-month major adverse cardiac events (MACE) between patients who underwent prior-failed-attempt and initial-attempt CTO-PCI. MACE was defined as a composite of cardiac death, target vessel-related myocardial infarction, and ischemia-driven target vessel revascularization (TVR) during follow-up.
Results
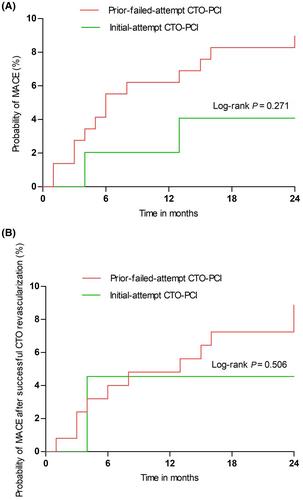
In total, 484 patients who underwent CTO-PCI (prior-failed-attempt, n = 49; initial-attempt, n = 435) were enrolled during the study period. After propensity score matching (1:3), 147 patients were included in the initial-attempt group. The proportion of the Japanese-CTO (J-CTO) score ≥2 was higher in the patients who underwent prior failed attempt than in those who underwent initial attempt (77.5% vs. 38.8%, p < 0.001). The retrograde approach was more often adopted in the prior-failed-attempt group than in the initial-attempt group (32.7% vs. 3.4%, [P< 0.001). Successful CTO revascularization rates were significantly lower in the prior-failed attempt-group than in the initial attempt group (53.1% vs. 83.3%, P < 0.001). The multivariate analysis revealed that J-CTO score ≥2 [odds ratio (OR), 0.359; 95% confidence interval (CI), 0.159–0.812; P = 0.014], intravascular ultrasound procedure (OR, 4.640; 95% CI, 1.380–15.603; P = 0.013), and prior failed attempt (OR, 0.285; 95% CI, 0.125–0.648; P = 0.003) were the independent predictors for successful CTO revascularization. There were no significant differences in major procedural complications (2.0% vs. 0.7%, p = 0.438) and MACE rates (4.1% vs. 8.8%, p = 0.438) between the groups, mainly due to the TVR rate (4.1% vs. 8.2%, P = 0.522).
Conclusions
Compared with initial-attempt CTO-PCI, prior-failed-attempt CTO-PCI deserves more attention, since it is associated with a lower successful CTO revascularization rate. Prior failed attempt, J-CTO score ≥2, and IVUS procedure are the determining factors for predicting successful CTO revascularization. There are no significantly different unfavorable outcomes between patients who undergo prior-failed-attempt and initial-attempt CTO-PCI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


