{"title":"胃肠道播散性巴西双孢子菌病:病例报告与诊断线索回顾。","authors":"Neda Soleimani, Mohammad Hossein Anbardar, Hamed Nikoupour, Faranak Derakhshan, Mojtaba Shafiekhani, Sahand Mohammadzadeh, Seyed Mohamad Sakhaei, Mahsa Farhadi","doi":"10.1155/2024/5741625","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Basidiobolomycosis is a rare fungal infection caused by an environmental saprophyte, <i>Basidiobolus ranarum</i>. It usually presents as a chronic subcutaneous infection; however, few cases of gastrointestinal involvement have been reported. The exact transmission route of gastrointestinal cases is not clear, and diagnosis always requires a high index of suspicion because it tends to mimic other inflammatory and neoplastic conditions. <i>Case Report</i>. A 31-year-old immunocompetent woman presented with abdominal pain and an advanced colon mass. She was completely well until about 1.5 years ago, when she underwent bariatric surgery. One year after surgery, chronic abdominal pain developed. A colonoscopy showed an ulcerative lesion in the descending colon, and the biopsy was in favor of ulcerative colitis. Despite immunosuppressive treatment, there was no improvement, and with worsening symptoms, more investigations revealed advanced colon mass with entrapment of the stomach and pancreas. Colonic mucosa biopsy and trucut biopsy of the mass showed just necrosis and acute inflammation; thus, she underwent exploratory laparotomy with colectomy, partial gastrectomy, distal pancreatectomy, and left nephrectomy. On pathologic examination, there was granulomatous inflammation plus the Splendore-Hoeppli phenomenon around fungal hyphae, which was diagnostic for gastrointestinal basidiobolomycosis. Previous pathology slides were reviewed and revealed a tiny focus of basidiobolomycosis. After 6 months of treatment with itraconazole, she is relatively well without any clinical or radiologic abnormalities.</p><p><strong>Conclusion: </strong>Our case highlights the significance of suspicion for basidiobolomycosis in ulcerative and necrotic lesions with increased eosinophils, especially in the presence of abdominal mass and systemic eosinophilia.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":"2024 ","pages":"5741625"},"PeriodicalIF":0.7000,"publicationDate":"2024-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11374415/pdf/","citationCount":"0","resultStr":"{\"title\":\"Disseminated Gastrointestinal Basidiobolomycosis: A Case Report with Review of Diagnostic Clues.\",\"authors\":\"Neda Soleimani, Mohammad Hossein Anbardar, Hamed Nikoupour, Faranak Derakhshan, Mojtaba Shafiekhani, Sahand Mohammadzadeh, Seyed Mohamad Sakhaei, Mahsa Farhadi\",\"doi\":\"10.1155/2024/5741625\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Basidiobolomycosis is a rare fungal infection caused by an environmental saprophyte, <i>Basidiobolus ranarum</i>. It usually presents as a chronic subcutaneous infection; however, few cases of gastrointestinal involvement have been reported. The exact transmission route of gastrointestinal cases is not clear, and diagnosis always requires a high index of suspicion because it tends to mimic other inflammatory and neoplastic conditions. <i>Case Report</i>. A 31-year-old immunocompetent woman presented with abdominal pain and an advanced colon mass. She was completely well until about 1.5 years ago, when she underwent bariatric surgery. One year after surgery, chronic abdominal pain developed. A colonoscopy showed an ulcerative lesion in the descending colon, and the biopsy was in favor of ulcerative colitis. Despite immunosuppressive treatment, there was no improvement, and with worsening symptoms, more investigations revealed advanced colon mass with entrapment of the stomach and pancreas. Colonic mucosa biopsy and trucut biopsy of the mass showed just necrosis and acute inflammation; thus, she underwent exploratory laparotomy with colectomy, partial gastrectomy, distal pancreatectomy, and left nephrectomy. On pathologic examination, there was granulomatous inflammation plus the Splendore-Hoeppli phenomenon around fungal hyphae, which was diagnostic for gastrointestinal basidiobolomycosis. Previous pathology slides were reviewed and revealed a tiny focus of basidiobolomycosis. After 6 months of treatment with itraconazole, she is relatively well without any clinical or radiologic abnormalities.</p><p><strong>Conclusion: </strong>Our case highlights the significance of suspicion for basidiobolomycosis in ulcerative and necrotic lesions with increased eosinophils, especially in the presence of abdominal mass and systemic eosinophilia.</p>\",\"PeriodicalId\":9627,\"journal\":{\"name\":\"Case Reports in Medicine\",\"volume\":\"2024 \",\"pages\":\"5741625\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-08-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11374415/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/5741625\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/5741625","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Disseminated Gastrointestinal Basidiobolomycosis: A Case Report with Review of Diagnostic Clues.
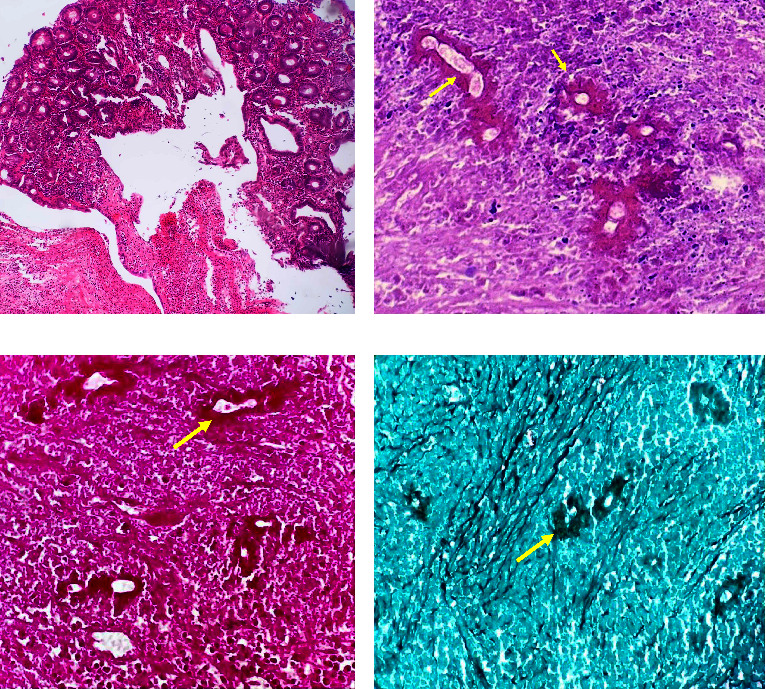
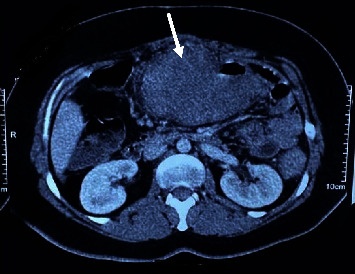
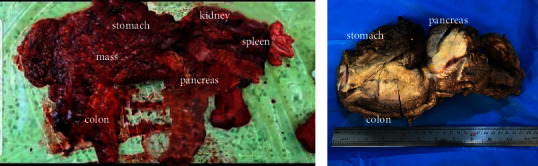
Introduction: Basidiobolomycosis is a rare fungal infection caused by an environmental saprophyte, Basidiobolus ranarum. It usually presents as a chronic subcutaneous infection; however, few cases of gastrointestinal involvement have been reported. The exact transmission route of gastrointestinal cases is not clear, and diagnosis always requires a high index of suspicion because it tends to mimic other inflammatory and neoplastic conditions. Case Report. A 31-year-old immunocompetent woman presented with abdominal pain and an advanced colon mass. She was completely well until about 1.5 years ago, when she underwent bariatric surgery. One year after surgery, chronic abdominal pain developed. A colonoscopy showed an ulcerative lesion in the descending colon, and the biopsy was in favor of ulcerative colitis. Despite immunosuppressive treatment, there was no improvement, and with worsening symptoms, more investigations revealed advanced colon mass with entrapment of the stomach and pancreas. Colonic mucosa biopsy and trucut biopsy of the mass showed just necrosis and acute inflammation; thus, she underwent exploratory laparotomy with colectomy, partial gastrectomy, distal pancreatectomy, and left nephrectomy. On pathologic examination, there was granulomatous inflammation plus the Splendore-Hoeppli phenomenon around fungal hyphae, which was diagnostic for gastrointestinal basidiobolomycosis. Previous pathology slides were reviewed and revealed a tiny focus of basidiobolomycosis. After 6 months of treatment with itraconazole, she is relatively well without any clinical or radiologic abnormalities.
Conclusion: Our case highlights the significance of suspicion for basidiobolomycosis in ulcerative and necrotic lesions with increased eosinophils, especially in the presence of abdominal mass and systemic eosinophilia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


