{"title":"急性冠状动脉综合征和多血管疾病患者立即完全血管重建与分阶段完全血管重建对短期和长期临床结果的影响:系统综述与元分析》。","authors":"Qiufeng Jia, Ankai Zuo, Chengrui Zhang, Danning Yang, Yu Zhang, Jing Li, Fengshuang An","doi":"10.1002/clc.70011","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>In patients with acute coronary syndrome (ACS) and multivessel disease (MVD), complete revascularization (CR) improves prognosis. This meta-analysis, summarizing recent RCTs, contrasts short-term and long-term clinical outcomes between immediate complete revascularization (ICR) and staged complete revascularization (SCR).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We systematically searched the online database and eight RCTs were involved. The primary outcomes included long-term unplanned ischemia-driven revascularization, re-infarction, combined cardiovascular (CV) death or myocardial infarction (MI), all-cause death, CV death, stroke, and hospitalization for heart failure (HHF). The secondary outcomes were 1-month unplanned ischemia-driven revascularization, re-infarction, all-cause death, and CV death. Safety endpoints included stent thrombosis and major bleeding.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Eight RCTs comprising 5198 patients were involved. ICR reduced long-term unplanned ischemia-driven revascularization (RR 0.64, 95% CI 0.51–0.81, <i>p</i> < 0.001), combined CV death or MI (HR 0.51, 95% CI 0.34–0.78, <i>p</i> = 0.002), and re-infarction (RR 0.66,95% CI 0.48 to 0.91, <i>p</i> = 0.012) compared with SCR. ICR also decreased 1-month unplanned ischemia-driven revascularization (RR 0.41, 95% CI: 0.21–0.77, <i>p</i> = 0.006) and re-infarction (RR 0.33, 95% CI:0.15–0.74, <i>p</i> = 0.007) but increased 1-month all-cause death (RR 2.22, 95% CI 1.06–4.65, <i>p</i> = 0.034).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In ACS patients with MVD, we first found that ICR significantly lowered the risk of both short-term and long-term unplanned ischemia-driven revascularization and re-infarction, as well as the long-term composite outcome of CV death or MI compared with SCR. However, there may be an increase in 1-month all-cause death in the ICR group.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 9","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70011","citationCount":"0","resultStr":"{\"title\":\"Impact of Immediate Versus Staged Complete Revascularization on Short-Term and Long-Term Clinical Outcomes in Patients With Acute Coronary Syndrome and Multivessel Disease: A Systematic Review and Meta-Analysis\",\"authors\":\"Qiufeng Jia, Ankai Zuo, Chengrui Zhang, Danning Yang, Yu Zhang, Jing Li, Fengshuang An\",\"doi\":\"10.1002/clc.70011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>In patients with acute coronary syndrome (ACS) and multivessel disease (MVD), complete revascularization (CR) improves prognosis. This meta-analysis, summarizing recent RCTs, contrasts short-term and long-term clinical outcomes between immediate complete revascularization (ICR) and staged complete revascularization (SCR).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We systematically searched the online database and eight RCTs were involved. The primary outcomes included long-term unplanned ischemia-driven revascularization, re-infarction, combined cardiovascular (CV) death or myocardial infarction (MI), all-cause death, CV death, stroke, and hospitalization for heart failure (HHF). The secondary outcomes were 1-month unplanned ischemia-driven revascularization, re-infarction, all-cause death, and CV death. Safety endpoints included stent thrombosis and major bleeding.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Eight RCTs comprising 5198 patients were involved. ICR reduced long-term unplanned ischemia-driven revascularization (RR 0.64, 95% CI 0.51–0.81, <i>p</i> < 0.001), combined CV death or MI (HR 0.51, 95% CI 0.34–0.78, <i>p</i> = 0.002), and re-infarction (RR 0.66,95% CI 0.48 to 0.91, <i>p</i> = 0.012) compared with SCR. ICR also decreased 1-month unplanned ischemia-driven revascularization (RR 0.41, 95% CI: 0.21–0.77, <i>p</i> = 0.006) and re-infarction (RR 0.33, 95% CI:0.15–0.74, <i>p</i> = 0.007) but increased 1-month all-cause death (RR 2.22, 95% CI 1.06–4.65, <i>p</i> = 0.034).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In ACS patients with MVD, we first found that ICR significantly lowered the risk of both short-term and long-term unplanned ischemia-driven revascularization and re-infarction, as well as the long-term composite outcome of CV death or MI compared with SCR. However, there may be an increase in 1-month all-cause death in the ICR group.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"47 9\",\"pages\":\"\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70011\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.70011\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.70011","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:对于急性冠状动脉综合征(ACS)和多血管疾病(MVD)患者,完全血运重建(CR)可改善预后。这项荟萃分析总结了近期的研究数据,对比了立即完全血管再通(ICR)和分阶段完全血管再通(SCR)的短期和长期临床结果:方法:我们系统地搜索了在线数据库,共涉及 8 项研究。主要结果包括长期非计划缺血驱动血管再通、再梗死、合并心血管(CV)死亡或心肌梗死(MI)、全因死亡、CV死亡、中风和心衰住院(HHF)。次要结局为1个月内非计划性缺血驱动血管再通、再梗死、全因死亡和CV死亡。安全性终点包括支架血栓形成和大出血:结果:8项研究共涉及5198名患者。ICR减少了长期非计划缺血驱动的血管再通术(RR 0.64,95% CI 0.51-0.81,p 结论:ICR减少了长期非计划缺血驱动的血管再通术(RR 0.64,95% CI 0.51-0.81,p在患有 MVD 的 ACS 患者中,我们首先发现,与 SCR 相比,ICR 能显著降低短期和长期计划外缺血驱动血管再通和再梗死的风险,以及心血管死亡或心肌梗死的长期综合结局。不过,ICR 组 1 个月内全因死亡人数可能会增加。
Impact of Immediate Versus Staged Complete Revascularization on Short-Term and Long-Term Clinical Outcomes in Patients With Acute Coronary Syndrome and Multivessel Disease: A Systematic Review and Meta-Analysis
Background
In patients with acute coronary syndrome (ACS) and multivessel disease (MVD), complete revascularization (CR) improves prognosis. This meta-analysis, summarizing recent RCTs, contrasts short-term and long-term clinical outcomes between immediate complete revascularization (ICR) and staged complete revascularization (SCR).
Methods
We systematically searched the online database and eight RCTs were involved. The primary outcomes included long-term unplanned ischemia-driven revascularization, re-infarction, combined cardiovascular (CV) death or myocardial infarction (MI), all-cause death, CV death, stroke, and hospitalization for heart failure (HHF). The secondary outcomes were 1-month unplanned ischemia-driven revascularization, re-infarction, all-cause death, and CV death. Safety endpoints included stent thrombosis and major bleeding.
Results
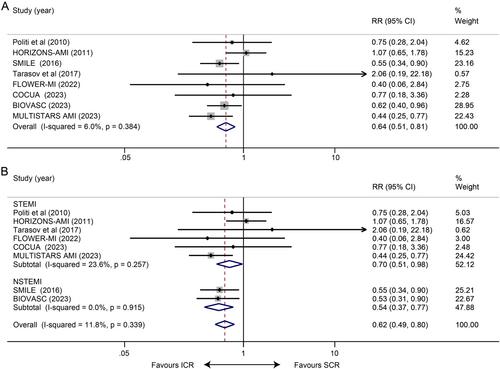
Eight RCTs comprising 5198 patients were involved. ICR reduced long-term unplanned ischemia-driven revascularization (RR 0.64, 95% CI 0.51–0.81, p < 0.001), combined CV death or MI (HR 0.51, 95% CI 0.34–0.78, p = 0.002), and re-infarction (RR 0.66,95% CI 0.48 to 0.91, p = 0.012) compared with SCR. ICR also decreased 1-month unplanned ischemia-driven revascularization (RR 0.41, 95% CI: 0.21–0.77, p = 0.006) and re-infarction (RR 0.33, 95% CI:0.15–0.74, p = 0.007) but increased 1-month all-cause death (RR 2.22, 95% CI 1.06–4.65, p = 0.034).
Conclusion
In ACS patients with MVD, we first found that ICR significantly lowered the risk of both short-term and long-term unplanned ischemia-driven revascularization and re-infarction, as well as the long-term composite outcome of CV death or MI compared with SCR. However, there may be an increase in 1-month all-cause death in the ICR group.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


