Eric Simpson, Peter Lio, Evangeline Pierce, Angel Cronin, Robert R. McLean, Thomas Eckmann, Amber Reck Atwater, Zach Dawson, Jonathan I. Silverberg
{"title":"特应性皮炎皮损位置和程度对患者负担的影响:真实世界研究","authors":"Eric Simpson, Peter Lio, Evangeline Pierce, Angel Cronin, Robert R. McLean, Thomas Eckmann, Amber Reck Atwater, Zach Dawson, Jonathan I. Silverberg","doi":"10.1002/jvc2.413","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Atopic dermatitis (AD) is associated with patient burden, but few studies describe the anatomic distribution of the disease or the impact of number of lesion locations.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>To describe lesion locations and assess the relationship between the number of lesion locations (disease extent) and disease burden in patients with AD.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This cross-sectional study included adults with dermatologist- or dermatology practitioner-diagnosed AD enroled in the CorEvitas AD Registry (2020–2021) who initiated systemic therapy within 12 months prior to or at enrolment or had moderate-to-severe AD (vIGA-AD® ≥3 and EASI ≥12) at enrolment. Thirteen areas of lesion involvement were assessed using a body map, and numbers of lesion locations were categorised as: 0, 1, 2–3, 4–6 and ≥7. Demographics, disease characteristics, PROs by number of lesion locations were descriptively compared using effect sizes (ES). The ES thresholds for small, medium, and large differences, respectively, were 0.10, 0.30, and 0.50 for phi (categorical outcomes) and 0.10, 0.25 and 0.40 for Cohen's f (continuous outcomes).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Among 1211 patients, lesion involvement was most frequent on the arms (69.5%) and lower limbs (61.7%). A total of 10.6%, 9.3%, 20.1%, 26.3% and 33.8% of patients had 0, 1, 2–3, 4–6 and ≥7 lesion locations, respectively. Current use of systemic (≥81.2%) and topical ( ≥74.7%) therapies was common, irrespective of lesion location. Disease severity increased with number of lesion locations: mean total BSA (ES = 1.17), EASI (ES = 1.11), and SCORAD (ES = 1.21). vIGA-AD ≥3 was observed in 28.3%, 45.3%, 78.0%, and 93.9% of patients with 1, 2–3, 4–6 and ≥7 locations, respectively (ES = 0.63). Greater number of lesion locations was associated with worse PROs: mean POEM (ES = 0.57), sleep loss (ES = 0.41), peak pruritus (ES = 0.50), DLQI (ES = 0.40), and ADCT (ES = 0.53). Uncontrolled AD (ADCT ≥7) was observed in 48.2%, 52.9%, 70.4%, 81.6% of patients with 1, 2–3, 4–6 and ≥7 locations, respectively (ES = 0.42).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>AD lesions were reported for each body area assessed. Greater number of lesion locations was associated with increased disease severity, poor disease control, and decreased quality of life. Patients experienced substantial disease burden regardless of number of lesion locations involved.</p>\n </section>\n </div>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1061-1075"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.413","citationCount":"0","resultStr":"{\"title\":\"Impact of atopic dermatitis lesion locations and extent on patient burden: A real-world study\",\"authors\":\"Eric Simpson, Peter Lio, Evangeline Pierce, Angel Cronin, Robert R. McLean, Thomas Eckmann, Amber Reck Atwater, Zach Dawson, Jonathan I. Silverberg\",\"doi\":\"10.1002/jvc2.413\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Atopic dermatitis (AD) is associated with patient burden, but few studies describe the anatomic distribution of the disease or the impact of number of lesion locations.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>To describe lesion locations and assess the relationship between the number of lesion locations (disease extent) and disease burden in patients with AD.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This cross-sectional study included adults with dermatologist- or dermatology practitioner-diagnosed AD enroled in the CorEvitas AD Registry (2020–2021) who initiated systemic therapy within 12 months prior to or at enrolment or had moderate-to-severe AD (vIGA-AD® ≥3 and EASI ≥12) at enrolment. Thirteen areas of lesion involvement were assessed using a body map, and numbers of lesion locations were categorised as: 0, 1, 2–3, 4–6 and ≥7. Demographics, disease characteristics, PROs by number of lesion locations were descriptively compared using effect sizes (ES). The ES thresholds for small, medium, and large differences, respectively, were 0.10, 0.30, and 0.50 for phi (categorical outcomes) and 0.10, 0.25 and 0.40 for Cohen's f (continuous outcomes).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Among 1211 patients, lesion involvement was most frequent on the arms (69.5%) and lower limbs (61.7%). A total of 10.6%, 9.3%, 20.1%, 26.3% and 33.8% of patients had 0, 1, 2–3, 4–6 and ≥7 lesion locations, respectively. Current use of systemic (≥81.2%) and topical ( ≥74.7%) therapies was common, irrespective of lesion location. Disease severity increased with number of lesion locations: mean total BSA (ES = 1.17), EASI (ES = 1.11), and SCORAD (ES = 1.21). vIGA-AD ≥3 was observed in 28.3%, 45.3%, 78.0%, and 93.9% of patients with 1, 2–3, 4–6 and ≥7 locations, respectively (ES = 0.63). Greater number of lesion locations was associated with worse PROs: mean POEM (ES = 0.57), sleep loss (ES = 0.41), peak pruritus (ES = 0.50), DLQI (ES = 0.40), and ADCT (ES = 0.53). Uncontrolled AD (ADCT ≥7) was observed in 48.2%, 52.9%, 70.4%, 81.6% of patients with 1, 2–3, 4–6 and ≥7 locations, respectively (ES = 0.42).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>AD lesions were reported for each body area assessed. Greater number of lesion locations was associated with increased disease severity, poor disease control, and decreased quality of life. Patients experienced substantial disease burden regardless of number of lesion locations involved.</p>\\n </section>\\n </div>\",\"PeriodicalId\":94325,\"journal\":{\"name\":\"JEADV clinical practice\",\"volume\":\"3 4\",\"pages\":\"1061-1075\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-04-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.413\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JEADV clinical practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.413\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.413","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Impact of atopic dermatitis lesion locations and extent on patient burden: A real-world study
Background
Atopic dermatitis (AD) is associated with patient burden, but few studies describe the anatomic distribution of the disease or the impact of number of lesion locations.
Objectives
To describe lesion locations and assess the relationship between the number of lesion locations (disease extent) and disease burden in patients with AD.
Methods
This cross-sectional study included adults with dermatologist- or dermatology practitioner-diagnosed AD enroled in the CorEvitas AD Registry (2020–2021) who initiated systemic therapy within 12 months prior to or at enrolment or had moderate-to-severe AD (vIGA-AD® ≥3 and EASI ≥12) at enrolment. Thirteen areas of lesion involvement were assessed using a body map, and numbers of lesion locations were categorised as: 0, 1, 2–3, 4–6 and ≥7. Demographics, disease characteristics, PROs by number of lesion locations were descriptively compared using effect sizes (ES). The ES thresholds for small, medium, and large differences, respectively, were 0.10, 0.30, and 0.50 for phi (categorical outcomes) and 0.10, 0.25 and 0.40 for Cohen's f (continuous outcomes).
Results
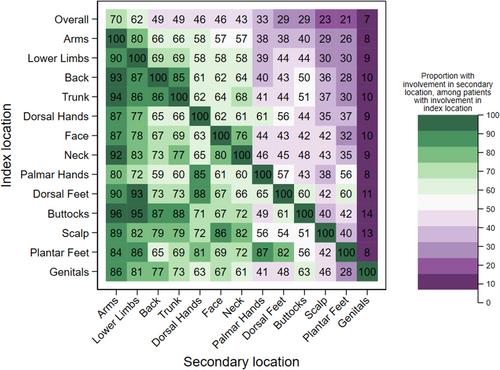
Among 1211 patients, lesion involvement was most frequent on the arms (69.5%) and lower limbs (61.7%). A total of 10.6%, 9.3%, 20.1%, 26.3% and 33.8% of patients had 0, 1, 2–3, 4–6 and ≥7 lesion locations, respectively. Current use of systemic (≥81.2%) and topical ( ≥74.7%) therapies was common, irrespective of lesion location. Disease severity increased with number of lesion locations: mean total BSA (ES = 1.17), EASI (ES = 1.11), and SCORAD (ES = 1.21). vIGA-AD ≥3 was observed in 28.3%, 45.3%, 78.0%, and 93.9% of patients with 1, 2–3, 4–6 and ≥7 locations, respectively (ES = 0.63). Greater number of lesion locations was associated with worse PROs: mean POEM (ES = 0.57), sleep loss (ES = 0.41), peak pruritus (ES = 0.50), DLQI (ES = 0.40), and ADCT (ES = 0.53). Uncontrolled AD (ADCT ≥7) was observed in 48.2%, 52.9%, 70.4%, 81.6% of patients with 1, 2–3, 4–6 and ≥7 locations, respectively (ES = 0.42).
Conclusions
AD lesions were reported for each body area assessed. Greater number of lesion locations was associated with increased disease severity, poor disease control, and decreased quality of life. Patients experienced substantial disease burden regardless of number of lesion locations involved.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


