{"title":"墨点型白斑的数字成像:共聚焦显微镜和线场共聚焦光学相干断层扫描评估","authors":"Marisa Salvi, Simone Cappilli, Costantino Ricci, Gerardo Palmisano, Alessandro Di Stefani, Ketty Peris","doi":"10.1002/jvc2.471","DOIUrl":null,"url":null,"abstract":"<p>The reticulated black solar lentigo was initially described by Bolognia et al. in 1992 as a type of solar lentigo.<span><sup>1</sup></span> Ink spot lentigo (ISL), as commonly known, clinically presents as a solitary dark pigmented macule with ill-defined margins occurring on the back of fair skin individuals. Due to the peculiar appearance and the common association with multiple solar lentigos, ISL may be difficult to differentiate from melanoma.<span><sup>1, 2</sup></span> Dermoscopy may show criteria similar to those observed in melanocytic lesions as an irregular thick pigment network, angulated lines and rhomboidal structures, and in these cases biopsy should be considered to rule out malignancy.<span><sup>2, 3</sup></span> The use of noninvasive imaging techniques, like reflectance confocal microscopy (RCM), increases the diagnostic accuracy of equivocal skin lesions, allowing to obtain greater performances than dermoscopy alone.<span><sup>4, 5</sup></span> A new digital tool, Line-field confocal optical coherence tomography (LC-OCT), is capable to acquire images/videos of skin lesions in multimodal view (vertical and horizontal), creating also immediate 3D cubes.<span><sup>6</sup></span> Pivotal studies reported promising preliminary data for the in vivo diagnosis of skin cancers.<span><sup>6-8</sup></span></p><p>We report RCM and LC-OCT morphological features of consecutive ISLs, correlating in vivo imaging to histopathology. Twenty-five histopathologically confirmed ISLs of 24 patients (14 M, 10 F, mean age: 48 years old, range: 19–82 years old) were investigated by RCM and LC-OCT from January 2023 to January 2024. ISLs were located on the trunk (10/25, 40%), on the face (7/25, 28%), on the lower extremities (4/25, 16%) and upper extremities (4/25, 16%). Dermoscopy showed atypical (thick, unevenly distributed) pigment network with sharp margins (23/25, 92%), and angulated lines (5/25, 20%) (Figures 1 and 2). RCM mosaics and horizontal sections of LC-OCT displayed densely packed, round to polymorphous edged papillae (24/25, 96%) at dermal-epidermal junction (DEJ), variably associated to bright cords with bulbous projections (19/25, 76%); focal distribution of plump, bright cells in the papillary dermis (20/25, 80%) and keratin-filled invaginations (3/25, 12%) in the upper layers of epidermis (Figure 1). Vertical LC-OCT mode revealed a bright continuous junction (25/25) with evident tubular elongations downward in the dermis (23/25); 3D reconstructions highlighted the presence of architectural changes at the DEJ with a regular epidermis (Figure 2). Criteria indicating melanocytic nature of ISL were not seen either with RCM or with LC-OCT.</p><p>In our ISLs series, RCM and LC-OCT allowed the clear recognition of typical features associated to a solar lentigo, confirming the benign nature of the lesion.<span><sup>6, 9</sup></span> The RCM findings are in line with a single case-report recently described by Venturi et al., observing RCM features of ringed pattern with edged papillae, white reticulated collagen, and small inflammatory cells. The recognition of such findings allowed the authors to confirm the diagnosis of ISL with no need of further excisions.<span><sup>9</sup></span> Compared to RCM, which only provides horizontally oriented images reaching a depth of 150–200 µm, LC-OCT can detect features of skin lesions up to a depth of 500 µm even in vertical and 3D mode, closely resembling a classical histopathological perspective. In this series, the main histopathological criteria of ISL, lentiginous hyperplasia of the epidermis and hyperpigmentation of the basal layer (quite pronounced at the tips of elongated rete ridges) have been clearly recognized with LC-OCT, able to reproduce a “virtual biopsy” that detect in vivo the key clues of this entity.</p><p>As digital imaging represents a bridge between dermoscopy and histopathology, it has a meaningful diagnostic value for skin lesions of doubtful interpretation, as commonly occur when dealing with ISL.<span><sup>4, 5</sup></span> The recognition of typical imaging suggestive of a solar lentigo (being ISL a solar lentigo) may increase diagnostic confidence of clinicians, which could in turn optimize their clinical management, as well as reducing unnecessary invasive procedures.</p><p><b>Marisa Salvi, Alessandro Di Stefani, and Simone Cappilli</b>: Conceptualization; <b>Gerardo Palmisano and Costantino Ricci</b>: Methodology; <b>Marisa Salvi and Simone Cappilli</b>: Original draft preparation; <b>Alessandro Di Stefani and Ketty Peris</b>: Review and editing; <b>Ketty Peris</b>: Supervision. All authors have read and agreed to the published version of the manuscript.</p><p>Peris has received consulting fees and honoraria from Abbvie, Almirall, Biogen, Celgene, Janssen Galderma, Novartis, Lilly, Novartis, Pierre Fabre, Sandoz, Sanofi and Sun Pharma outside of the submitted work. The remaining authors declare no conflict of interest.</p><p>This study was conducted in accordance with the Declaration of Helsinki. All patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.</p>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1308-1311"},"PeriodicalIF":0.0000,"publicationDate":"2024-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.471","citationCount":"0","resultStr":"{\"title\":\"Digital imaging of ink spot lentigo: Confocal microscopy and line-field confocal optical coherence tomography assessment\",\"authors\":\"Marisa Salvi, Simone Cappilli, Costantino Ricci, Gerardo Palmisano, Alessandro Di Stefani, Ketty Peris\",\"doi\":\"10.1002/jvc2.471\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The reticulated black solar lentigo was initially described by Bolognia et al. in 1992 as a type of solar lentigo.<span><sup>1</sup></span> Ink spot lentigo (ISL), as commonly known, clinically presents as a solitary dark pigmented macule with ill-defined margins occurring on the back of fair skin individuals. Due to the peculiar appearance and the common association with multiple solar lentigos, ISL may be difficult to differentiate from melanoma.<span><sup>1, 2</sup></span> Dermoscopy may show criteria similar to those observed in melanocytic lesions as an irregular thick pigment network, angulated lines and rhomboidal structures, and in these cases biopsy should be considered to rule out malignancy.<span><sup>2, 3</sup></span> The use of noninvasive imaging techniques, like reflectance confocal microscopy (RCM), increases the diagnostic accuracy of equivocal skin lesions, allowing to obtain greater performances than dermoscopy alone.<span><sup>4, 5</sup></span> A new digital tool, Line-field confocal optical coherence tomography (LC-OCT), is capable to acquire images/videos of skin lesions in multimodal view (vertical and horizontal), creating also immediate 3D cubes.<span><sup>6</sup></span> Pivotal studies reported promising preliminary data for the in vivo diagnosis of skin cancers.<span><sup>6-8</sup></span></p><p>We report RCM and LC-OCT morphological features of consecutive ISLs, correlating in vivo imaging to histopathology. Twenty-five histopathologically confirmed ISLs of 24 patients (14 M, 10 F, mean age: 48 years old, range: 19–82 years old) were investigated by RCM and LC-OCT from January 2023 to January 2024. ISLs were located on the trunk (10/25, 40%), on the face (7/25, 28%), on the lower extremities (4/25, 16%) and upper extremities (4/25, 16%). Dermoscopy showed atypical (thick, unevenly distributed) pigment network with sharp margins (23/25, 92%), and angulated lines (5/25, 20%) (Figures 1 and 2). RCM mosaics and horizontal sections of LC-OCT displayed densely packed, round to polymorphous edged papillae (24/25, 96%) at dermal-epidermal junction (DEJ), variably associated to bright cords with bulbous projections (19/25, 76%); focal distribution of plump, bright cells in the papillary dermis (20/25, 80%) and keratin-filled invaginations (3/25, 12%) in the upper layers of epidermis (Figure 1). Vertical LC-OCT mode revealed a bright continuous junction (25/25) with evident tubular elongations downward in the dermis (23/25); 3D reconstructions highlighted the presence of architectural changes at the DEJ with a regular epidermis (Figure 2). Criteria indicating melanocytic nature of ISL were not seen either with RCM or with LC-OCT.</p><p>In our ISLs series, RCM and LC-OCT allowed the clear recognition of typical features associated to a solar lentigo, confirming the benign nature of the lesion.<span><sup>6, 9</sup></span> The RCM findings are in line with a single case-report recently described by Venturi et al., observing RCM features of ringed pattern with edged papillae, white reticulated collagen, and small inflammatory cells. The recognition of such findings allowed the authors to confirm the diagnosis of ISL with no need of further excisions.<span><sup>9</sup></span> Compared to RCM, which only provides horizontally oriented images reaching a depth of 150–200 µm, LC-OCT can detect features of skin lesions up to a depth of 500 µm even in vertical and 3D mode, closely resembling a classical histopathological perspective. In this series, the main histopathological criteria of ISL, lentiginous hyperplasia of the epidermis and hyperpigmentation of the basal layer (quite pronounced at the tips of elongated rete ridges) have been clearly recognized with LC-OCT, able to reproduce a “virtual biopsy” that detect in vivo the key clues of this entity.</p><p>As digital imaging represents a bridge between dermoscopy and histopathology, it has a meaningful diagnostic value for skin lesions of doubtful interpretation, as commonly occur when dealing with ISL.<span><sup>4, 5</sup></span> The recognition of typical imaging suggestive of a solar lentigo (being ISL a solar lentigo) may increase diagnostic confidence of clinicians, which could in turn optimize their clinical management, as well as reducing unnecessary invasive procedures.</p><p><b>Marisa Salvi, Alessandro Di Stefani, and Simone Cappilli</b>: Conceptualization; <b>Gerardo Palmisano and Costantino Ricci</b>: Methodology; <b>Marisa Salvi and Simone Cappilli</b>: Original draft preparation; <b>Alessandro Di Stefani and Ketty Peris</b>: Review and editing; <b>Ketty Peris</b>: Supervision. All authors have read and agreed to the published version of the manuscript.</p><p>Peris has received consulting fees and honoraria from Abbvie, Almirall, Biogen, Celgene, Janssen Galderma, Novartis, Lilly, Novartis, Pierre Fabre, Sandoz, Sanofi and Sun Pharma outside of the submitted work. The remaining authors declare no conflict of interest.</p><p>This study was conducted in accordance with the Declaration of Helsinki. All patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.</p>\",\"PeriodicalId\":94325,\"journal\":{\"name\":\"JEADV clinical practice\",\"volume\":\"3 4\",\"pages\":\"1308-1311\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-05-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.471\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JEADV clinical practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.471\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.471","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Digital imaging of ink spot lentigo: Confocal microscopy and line-field confocal optical coherence tomography assessment
The reticulated black solar lentigo was initially described by Bolognia et al. in 1992 as a type of solar lentigo.1 Ink spot lentigo (ISL), as commonly known, clinically presents as a solitary dark pigmented macule with ill-defined margins occurring on the back of fair skin individuals. Due to the peculiar appearance and the common association with multiple solar lentigos, ISL may be difficult to differentiate from melanoma.1, 2 Dermoscopy may show criteria similar to those observed in melanocytic lesions as an irregular thick pigment network, angulated lines and rhomboidal structures, and in these cases biopsy should be considered to rule out malignancy.2, 3 The use of noninvasive imaging techniques, like reflectance confocal microscopy (RCM), increases the diagnostic accuracy of equivocal skin lesions, allowing to obtain greater performances than dermoscopy alone.4, 5 A new digital tool, Line-field confocal optical coherence tomography (LC-OCT), is capable to acquire images/videos of skin lesions in multimodal view (vertical and horizontal), creating also immediate 3D cubes.6 Pivotal studies reported promising preliminary data for the in vivo diagnosis of skin cancers.6-8
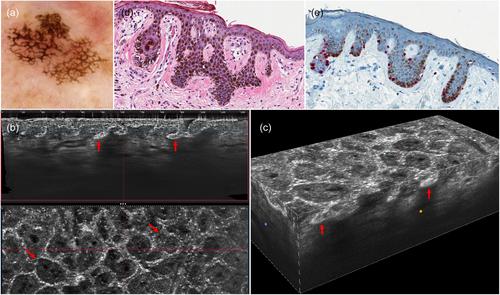
We report RCM and LC-OCT morphological features of consecutive ISLs, correlating in vivo imaging to histopathology. Twenty-five histopathologically confirmed ISLs of 24 patients (14 M, 10 F, mean age: 48 years old, range: 19–82 years old) were investigated by RCM and LC-OCT from January 2023 to January 2024. ISLs were located on the trunk (10/25, 40%), on the face (7/25, 28%), on the lower extremities (4/25, 16%) and upper extremities (4/25, 16%). Dermoscopy showed atypical (thick, unevenly distributed) pigment network with sharp margins (23/25, 92%), and angulated lines (5/25, 20%) (Figures 1 and 2). RCM mosaics and horizontal sections of LC-OCT displayed densely packed, round to polymorphous edged papillae (24/25, 96%) at dermal-epidermal junction (DEJ), variably associated to bright cords with bulbous projections (19/25, 76%); focal distribution of plump, bright cells in the papillary dermis (20/25, 80%) and keratin-filled invaginations (3/25, 12%) in the upper layers of epidermis (Figure 1). Vertical LC-OCT mode revealed a bright continuous junction (25/25) with evident tubular elongations downward in the dermis (23/25); 3D reconstructions highlighted the presence of architectural changes at the DEJ with a regular epidermis (Figure 2). Criteria indicating melanocytic nature of ISL were not seen either with RCM or with LC-OCT.
In our ISLs series, RCM and LC-OCT allowed the clear recognition of typical features associated to a solar lentigo, confirming the benign nature of the lesion.6, 9 The RCM findings are in line with a single case-report recently described by Venturi et al., observing RCM features of ringed pattern with edged papillae, white reticulated collagen, and small inflammatory cells. The recognition of such findings allowed the authors to confirm the diagnosis of ISL with no need of further excisions.9 Compared to RCM, which only provides horizontally oriented images reaching a depth of 150–200 µm, LC-OCT can detect features of skin lesions up to a depth of 500 µm even in vertical and 3D mode, closely resembling a classical histopathological perspective. In this series, the main histopathological criteria of ISL, lentiginous hyperplasia of the epidermis and hyperpigmentation of the basal layer (quite pronounced at the tips of elongated rete ridges) have been clearly recognized with LC-OCT, able to reproduce a “virtual biopsy” that detect in vivo the key clues of this entity.
As digital imaging represents a bridge between dermoscopy and histopathology, it has a meaningful diagnostic value for skin lesions of doubtful interpretation, as commonly occur when dealing with ISL.4, 5 The recognition of typical imaging suggestive of a solar lentigo (being ISL a solar lentigo) may increase diagnostic confidence of clinicians, which could in turn optimize their clinical management, as well as reducing unnecessary invasive procedures.
Marisa Salvi, Alessandro Di Stefani, and Simone Cappilli: Conceptualization; Gerardo Palmisano and Costantino Ricci: Methodology; Marisa Salvi and Simone Cappilli: Original draft preparation; Alessandro Di Stefani and Ketty Peris: Review and editing; Ketty Peris: Supervision. All authors have read and agreed to the published version of the manuscript.
Peris has received consulting fees and honoraria from Abbvie, Almirall, Biogen, Celgene, Janssen Galderma, Novartis, Lilly, Novartis, Pierre Fabre, Sandoz, Sanofi and Sun Pharma outside of the submitted work. The remaining authors declare no conflict of interest.
This study was conducted in accordance with the Declaration of Helsinki. All patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


