{"title":"阿特珠单抗诱发的圆形气胸免疫相关肺炎","authors":"Satoru Yanagisawa, Takaya Yui, Hiroki Takechi, Satoshi Wasamoto","doi":"10.1111/crj.70008","DOIUrl":null,"url":null,"abstract":"<p>Dear editor:</p><p>An 82-year-old man with a heavy smoking history (35 pack-years) was diagnosed with right upper lung small cell lung cancer (extensive-disease, cT1cN3M1c: cStage IVB, LYM, OSS, HEP) in June 2023. He was a retired electrician who had been exposed to construction dust and asbestos fibers for decades. Chest computed tomography (CT) revealed partially calcified pleural plaques and posterior left lower lobe rounded atelectasis (RA) with “comet tail sign” [<span>1</span>] (Figure 1A,B). Retrospectively, the RA appeared to remain the same shape and size since 2017. Positron emission tomography revealed <sup>18</sup>F-fluorodeoxyglucose uptake in the right upper lobe primary tumor, but not in the pleural plaque or RA (Figure 1C–E). Subsequently, the patient was treated with carboplatin/etoposide plus atezolizumab as first-line chemotherapy in July 2023. Soon after atezolizumab infusion, he developed a transient fever; thereafter, he gradually complained of worsening dyspnea on exertion, with mild desaturation. On day 9 after chemotherapy induction, chest CT showed a new-onset consolidative shadow on the left lower lung that appeared around the preexisting RA (Figure 2A,B). The laboratory test results, including infectious serology and culture results, were unremarkable. Additional inflammatory serologies (antinuclear and antineutrophil cytoplasmic antibodies) were negative. Due to hypoxemia, further diagnostic studies, such as bronchoscopy, could not be conducted. We suspected that the lesion was consistent with atezolizumab-induced interstitial lung disease (immune-related adverse event [irAE]) and started intravenous prednisolone (40 mg daily). After the initiation of steroid treatment, his hypoxemia and lung shadow were almost completely cleared (Figure 2C,D), which supported the diagnosis of irAE pneumonia in RA. We decided to refrain from atezolizumab treatment and continued carboplatin/etoposide therapy alone without recurrence of irAEs.</p><p>RA [<span>2</span>], also known as “folded lung” or “Blesovsky's syndrome,” is a subtype of lung atelectasis caused by invagination of the redundant visceral pleura [<span>3</span>]. Although most RA are believed to be associated with asbestos lung exposure [<span>4</span>], it is sometimes difficult to differentiate RA from other asbestos exposure-associated malignant diseases such as lung cancer and malignant pleural mesothelioma [<span>5</span>]. RA usually maintains the same volume and even shrinks on serial scans [<span>4-6</span>], which supports the benign feature of the lesion and justifies careful follow-up without intervention. However, there are some reports of RA that gradually enlarge and eventually necessitate surgical biopsy or excision [<span>7</span>]. Although the precise mechanism of RA enlargement is yet to be elucidated, persistent chronic pleural inflammation may be associated. In our case, subpleural consolidation around the RA expanded after the initiation of atezolizumab treatment, and it is possible that the pleural damage around the RA contributed to the occurrence of irAE pneumonia. Sakata et al. reported nivolumab-induced severe interstitial pneumonia that occurred after talc pleurodesis [<span>8</span>]. They speculated that nivolumab may have exaggerated talc-induced damage to pleural mesothelial cells, and that chemical inflammation eventually resulted in severe interstitial pneumonia. Although asbestos-associated RA is usually considered an old inflammatory change, it may be a latent stage with the potential to flare with the use of immune checkpoint inhibitors (ICIs).</p><p>In conclusion, this was a case of atezolizumab-induced irAE pneumonia, which occurred in a patient with RA. As asbestos exposure is associated with RA, it is important to appropriately diagnose drug-induced pneumonia, which may exaggerate pre-existing RA. In addition, RA-associated pleural inflammation may become apparent upon ICIs treatment.</p><p>Satoru Yanagisawa and Satoshi Wasamoto conceived the study and drafted the manuscript. Hiroki Takechi and Takaya Yui were involved in the discussion and manuscript preparation.</p><p>All authors reviewed this manuscript and agreed to submit this manuscript.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":55247,"journal":{"name":"Clinical Respiratory Journal","volume":"18 9","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11370623/pdf/","citationCount":"0","resultStr":"{\"title\":\"Atezolizumab-Induced Immune-Related Pneumonia on Rounded Atelectasis\",\"authors\":\"Satoru Yanagisawa, Takaya Yui, Hiroki Takechi, Satoshi Wasamoto\",\"doi\":\"10.1111/crj.70008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Dear editor:</p><p>An 82-year-old man with a heavy smoking history (35 pack-years) was diagnosed with right upper lung small cell lung cancer (extensive-disease, cT1cN3M1c: cStage IVB, LYM, OSS, HEP) in June 2023. He was a retired electrician who had been exposed to construction dust and asbestos fibers for decades. Chest computed tomography (CT) revealed partially calcified pleural plaques and posterior left lower lobe rounded atelectasis (RA) with “comet tail sign” [<span>1</span>] (Figure 1A,B). Retrospectively, the RA appeared to remain the same shape and size since 2017. Positron emission tomography revealed <sup>18</sup>F-fluorodeoxyglucose uptake in the right upper lobe primary tumor, but not in the pleural plaque or RA (Figure 1C–E). Subsequently, the patient was treated with carboplatin/etoposide plus atezolizumab as first-line chemotherapy in July 2023. Soon after atezolizumab infusion, he developed a transient fever; thereafter, he gradually complained of worsening dyspnea on exertion, with mild desaturation. On day 9 after chemotherapy induction, chest CT showed a new-onset consolidative shadow on the left lower lung that appeared around the preexisting RA (Figure 2A,B). The laboratory test results, including infectious serology and culture results, were unremarkable. Additional inflammatory serologies (antinuclear and antineutrophil cytoplasmic antibodies) were negative. Due to hypoxemia, further diagnostic studies, such as bronchoscopy, could not be conducted. We suspected that the lesion was consistent with atezolizumab-induced interstitial lung disease (immune-related adverse event [irAE]) and started intravenous prednisolone (40 mg daily). After the initiation of steroid treatment, his hypoxemia and lung shadow were almost completely cleared (Figure 2C,D), which supported the diagnosis of irAE pneumonia in RA. We decided to refrain from atezolizumab treatment and continued carboplatin/etoposide therapy alone without recurrence of irAEs.</p><p>RA [<span>2</span>], also known as “folded lung” or “Blesovsky's syndrome,” is a subtype of lung atelectasis caused by invagination of the redundant visceral pleura [<span>3</span>]. Although most RA are believed to be associated with asbestos lung exposure [<span>4</span>], it is sometimes difficult to differentiate RA from other asbestos exposure-associated malignant diseases such as lung cancer and malignant pleural mesothelioma [<span>5</span>]. RA usually maintains the same volume and even shrinks on serial scans [<span>4-6</span>], which supports the benign feature of the lesion and justifies careful follow-up without intervention. However, there are some reports of RA that gradually enlarge and eventually necessitate surgical biopsy or excision [<span>7</span>]. Although the precise mechanism of RA enlargement is yet to be elucidated, persistent chronic pleural inflammation may be associated. In our case, subpleural consolidation around the RA expanded after the initiation of atezolizumab treatment, and it is possible that the pleural damage around the RA contributed to the occurrence of irAE pneumonia. Sakata et al. reported nivolumab-induced severe interstitial pneumonia that occurred after talc pleurodesis [<span>8</span>]. They speculated that nivolumab may have exaggerated talc-induced damage to pleural mesothelial cells, and that chemical inflammation eventually resulted in severe interstitial pneumonia. Although asbestos-associated RA is usually considered an old inflammatory change, it may be a latent stage with the potential to flare with the use of immune checkpoint inhibitors (ICIs).</p><p>In conclusion, this was a case of atezolizumab-induced irAE pneumonia, which occurred in a patient with RA. As asbestos exposure is associated with RA, it is important to appropriately diagnose drug-induced pneumonia, which may exaggerate pre-existing RA. In addition, RA-associated pleural inflammation may become apparent upon ICIs treatment.</p><p>Satoru Yanagisawa and Satoshi Wasamoto conceived the study and drafted the manuscript. Hiroki Takechi and Takaya Yui were involved in the discussion and manuscript preparation.</p><p>All authors reviewed this manuscript and agreed to submit this manuscript.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":55247,\"journal\":{\"name\":\"Clinical Respiratory Journal\",\"volume\":\"18 9\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11370623/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Respiratory Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/crj.70008\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Respiratory Journal","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/crj.70008","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
亲爱的编辑:一位有严重吸烟史(35 包年)的 82 岁男性于 2023 年 6 月被诊断为右上肺小细胞肺癌(广泛病变,cT1cN3M1c:c IVB 期,LYM,OSS,HEP)。他是一名退休电工,数十年来一直接触建筑粉尘和石棉纤维。胸部计算机断层扫描(CT)显示部分钙化胸膜斑块和左下叶后部圆形脑积水(RA),并伴有 "彗尾征"[1](图 1A、B)。回想起来,自2017年以来,RA的形状和大小似乎保持不变。正电子发射断层扫描显示右上叶原发肿瘤摄取18F-氟脱氧葡萄糖,但胸膜斑块或RA未摄取18F-氟脱氧葡萄糖(图1C-E)。随后,患者于2023年7月接受了卡铂/依托泊苷加阿特珠单抗的一线化疗。输注阿特珠单抗后不久,他出现了一过性发热;此后,他逐渐主诉劳累时呼吸困难加重,并伴有轻度饱和度降低。化疗诱导后第9天,胸部CT显示左下肺出现新发合并影,出现在原有RA周围(图2A,B)。实验室检查结果,包括感染血清学和培养结果,均无异常。其他炎症血清学检查(抗核抗体和抗中性粒细胞胞浆抗体)均为阴性。由于低氧血症,无法进行进一步的诊断检查,如支气管镜检查。我们怀疑该病变与阿特珠单抗诱发的间质性肺病(免疫相关不良事件[irAE])一致,并开始静脉注射泼尼松龙(每天40毫克)。开始类固醇治疗后,他的低氧血症和肺部阴影几乎完全消失(图2C,D),这支持了RAirAE肺炎的诊断。RA[2]又称 "折叠肺 "或 "Blesovsky综合征",是由多余的内脏胸膜内陷引起的肺大泡的一种亚型[3]。虽然大多数 RA 被认为与石棉肺暴露有关[4],但有时很难将 RA 与其他与石棉暴露有关的恶性疾病(如肺癌和恶性胸膜间皮瘤)区分开来[5]。在连续扫描中,RA 的体积通常保持不变,甚至会缩小[4-6],这支持了病变的良性特征,因此有理由在不进行干预的情况下进行仔细随访。不过,也有一些 RA 逐渐增大,最终需要手术活检或切除的报道[7]。虽然 RA 扩大的确切机制尚未阐明,但持续的慢性胸膜炎症可能与此有关。在我们的病例中,开始使用阿特珠单抗治疗后,RA 周围的胸膜下合并症扩大,可能是 RA 周围的胸膜损伤导致了虹膜急性外膜炎肺炎的发生。Sakata 等人报道了滑石粉胸膜穿刺术后发生的 nivolumab 诱导的严重间质性肺炎[8]。他们推测,nivolumab 可能夸大了滑石粉诱导的胸膜间皮细胞损伤,化学炎症最终导致了严重的间质性肺炎。尽管石棉相关的RA通常被认为是一种陈旧性炎症改变,但它可能是一种潜伏期,有可能在使用免疫检查点抑制剂(ICIs)后发作。总之,这是一例阿特珠单抗诱发的irAE肺炎,发生在一名RA患者身上。由于石棉暴露与 RA 相关,因此适当诊断药物诱导的肺炎非常重要,因为这可能会夸大已存在的 RA。此外,在接受 ICIs 治疗后,与 RA 相关的胸膜炎症可能会变得明显。所有作者均审阅了本稿件,并同意提交本稿件。
Atezolizumab-Induced Immune-Related Pneumonia on Rounded Atelectasis
Dear editor:
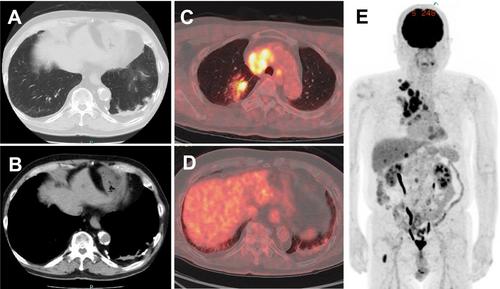
An 82-year-old man with a heavy smoking history (35 pack-years) was diagnosed with right upper lung small cell lung cancer (extensive-disease, cT1cN3M1c: cStage IVB, LYM, OSS, HEP) in June 2023. He was a retired electrician who had been exposed to construction dust and asbestos fibers for decades. Chest computed tomography (CT) revealed partially calcified pleural plaques and posterior left lower lobe rounded atelectasis (RA) with “comet tail sign” [1] (Figure 1A,B). Retrospectively, the RA appeared to remain the same shape and size since 2017. Positron emission tomography revealed 18F-fluorodeoxyglucose uptake in the right upper lobe primary tumor, but not in the pleural plaque or RA (Figure 1C–E). Subsequently, the patient was treated with carboplatin/etoposide plus atezolizumab as first-line chemotherapy in July 2023. Soon after atezolizumab infusion, he developed a transient fever; thereafter, he gradually complained of worsening dyspnea on exertion, with mild desaturation. On day 9 after chemotherapy induction, chest CT showed a new-onset consolidative shadow on the left lower lung that appeared around the preexisting RA (Figure 2A,B). The laboratory test results, including infectious serology and culture results, were unremarkable. Additional inflammatory serologies (antinuclear and antineutrophil cytoplasmic antibodies) were negative. Due to hypoxemia, further diagnostic studies, such as bronchoscopy, could not be conducted. We suspected that the lesion was consistent with atezolizumab-induced interstitial lung disease (immune-related adverse event [irAE]) and started intravenous prednisolone (40 mg daily). After the initiation of steroid treatment, his hypoxemia and lung shadow were almost completely cleared (Figure 2C,D), which supported the diagnosis of irAE pneumonia in RA. We decided to refrain from atezolizumab treatment and continued carboplatin/etoposide therapy alone without recurrence of irAEs.
RA [2], also known as “folded lung” or “Blesovsky's syndrome,” is a subtype of lung atelectasis caused by invagination of the redundant visceral pleura [3]. Although most RA are believed to be associated with asbestos lung exposure [4], it is sometimes difficult to differentiate RA from other asbestos exposure-associated malignant diseases such as lung cancer and malignant pleural mesothelioma [5]. RA usually maintains the same volume and even shrinks on serial scans [4-6], which supports the benign feature of the lesion and justifies careful follow-up without intervention. However, there are some reports of RA that gradually enlarge and eventually necessitate surgical biopsy or excision [7]. Although the precise mechanism of RA enlargement is yet to be elucidated, persistent chronic pleural inflammation may be associated. In our case, subpleural consolidation around the RA expanded after the initiation of atezolizumab treatment, and it is possible that the pleural damage around the RA contributed to the occurrence of irAE pneumonia. Sakata et al. reported nivolumab-induced severe interstitial pneumonia that occurred after talc pleurodesis [8]. They speculated that nivolumab may have exaggerated talc-induced damage to pleural mesothelial cells, and that chemical inflammation eventually resulted in severe interstitial pneumonia. Although asbestos-associated RA is usually considered an old inflammatory change, it may be a latent stage with the potential to flare with the use of immune checkpoint inhibitors (ICIs).
In conclusion, this was a case of atezolizumab-induced irAE pneumonia, which occurred in a patient with RA. As asbestos exposure is associated with RA, it is important to appropriately diagnose drug-induced pneumonia, which may exaggerate pre-existing RA. In addition, RA-associated pleural inflammation may become apparent upon ICIs treatment.
Satoru Yanagisawa and Satoshi Wasamoto conceived the study and drafted the manuscript. Hiroki Takechi and Takaya Yui were involved in the discussion and manuscript preparation.
All authors reviewed this manuscript and agreed to submit this manuscript.
期刊介绍:
Overview
Effective with the 2016 volume, this journal will be published in an online-only format.
Aims and Scope
The Clinical Respiratory Journal (CRJ) provides a forum for clinical research in all areas of respiratory medicine from clinical lung disease to basic research relevant to the clinic.
We publish original research, review articles, case studies, editorials and book reviews in all areas of clinical lung disease including:
Asthma
Allergy
COPD
Non-invasive ventilation
Sleep related breathing disorders
Interstitial lung diseases
Lung cancer
Clinical genetics
Rhinitis
Airway and lung infection
Epidemiology
Pediatrics
CRJ provides a fast-track service for selected Phase II and Phase III trial studies.
Keywords
Clinical Respiratory Journal, respiratory, pulmonary, medicine, clinical, lung disease,
Abstracting and Indexing Information
Academic Search (EBSCO Publishing)
Academic Search Alumni Edition (EBSCO Publishing)
Embase (Elsevier)
Health & Medical Collection (ProQuest)
Health Research Premium Collection (ProQuest)
HEED: Health Economic Evaluations Database (Wiley-Blackwell)
Hospital Premium Collection (ProQuest)
Journal Citation Reports/Science Edition (Clarivate Analytics)
MEDLINE/PubMed (NLM)
ProQuest Central (ProQuest)
Science Citation Index Expanded (Clarivate Analytics)
SCOPUS (Elsevier)

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


