Kirstine Shrubsole, Marissa Stone, Dominique A. Cadilhac, Monique F. Kilkenny, Emma Power, Elizabeth Lynch, John E. Pierce, David A. Copland, Erin Godecke, Bridget Burton, Emily Brogan, Sarah J. Wallace
{"title":"通过最终用户参与,制定脑卒中后失语症服务的质量指标和实施重点。","authors":"Kirstine Shrubsole, Marissa Stone, Dominique A. Cadilhac, Monique F. Kilkenny, Emma Power, Elizabeth Lynch, John E. Pierce, David A. Copland, Erin Godecke, Bridget Burton, Emily Brogan, Sarah J. Wallace","doi":"10.1111/hex.14173","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Currently, there are no agreed quality standards for post-stroke aphasia services. Therefore, it is unknown if care reflects best practices or meets the expectations of people living with aphasia. We aimed to (1) shortlist, (2) operationalise and (3) prioritise best practice recommendations for post-stroke aphasia care.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Three phases of research were conducted. In Phase 1, recommendations with strong evidence and/or known to be important to people with lived experience of aphasia were identified. People with lived experience and health professionals rated the importance of each recommendation through a two-round e-Delphi exercise. Recommendations were then ranked for importance and feasibility and analysed using a graph theory–based voting system. In Phase 2, shortlisted recommendations from Phase 1 were converted into quality indicators for appraisal and voting in consensus meetings. In Phase 3, priorities for implementation were established by people with lived experience and health professionals following discussion and anonymous voting.</p>\n </section>\n \n <section>\n \n <h3> Findings</h3>\n \n <p>In Phase 1, 23 best practice recommendations were identified and rated by people with lived experience (<i>n</i> = 26) and health professionals (<i>n</i> = 81). Ten recommendations were shortlisted. In Phase 2, people with lived experience (<i>n</i> = 4) and health professionals (<i>n</i> = 17) reached a consensus on 11 quality indicators, relating to assessment (<i>n</i> = 2), information provision (<i>n</i> = 3), communication partner training (<i>n</i> = 3), goal setting (<i>n</i> = 1), person and family-centred care (<i>n</i> = 1) and provision of treatment (<i>n</i> = 1). In Phase 3, people with lived experience (<i>n</i> = 5) and health professionals (<i>n</i> = 7) identified three implementation priorities: assessment of aphasia, provision of aphasia-friendly information and provision of therapy.</p>\n </section>\n \n <section>\n \n <h3> Interpretation</h3>\n \n <p>Our 11 quality indicators and 3 implementation priorities are the first step to enabling systematic, efficient and person-centred measurement and quality improvement in post-stroke aphasia services. Quality indicators will be embedded in routine data collection systems, and strategies will be developed to address implementation priorities.</p>\n </section>\n \n <section>\n \n <h3> Patient and Public Contribution</h3>\n \n <p>Protocol development was informed by our previous research, which explored the perspectives of 23 people living with aphasia about best practice aphasia services. Individuals with lived experience of aphasia participated as expert panel members in our three consensus meetings. We received support from consumer advisory networks associated with the Centre for Research Excellence in Aphasia Rehabilitation and Recovery and the Queensland Aphasia Research Centre.</p>\n </section>\n </div>","PeriodicalId":55070,"journal":{"name":"Health Expectations","volume":"27 5","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2024-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11369030/pdf/","citationCount":"0","resultStr":"{\"title\":\"Establishing Quality Indicators and Implementation Priorities for Post-Stroke Aphasia Services Through End-User Involvement\",\"authors\":\"Kirstine Shrubsole, Marissa Stone, Dominique A. Cadilhac, Monique F. Kilkenny, Emma Power, Elizabeth Lynch, John E. Pierce, David A. Copland, Erin Godecke, Bridget Burton, Emily Brogan, Sarah J. Wallace\",\"doi\":\"10.1111/hex.14173\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Currently, there are no agreed quality standards for post-stroke aphasia services. Therefore, it is unknown if care reflects best practices or meets the expectations of people living with aphasia. We aimed to (1) shortlist, (2) operationalise and (3) prioritise best practice recommendations for post-stroke aphasia care.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Three phases of research were conducted. In Phase 1, recommendations with strong evidence and/or known to be important to people with lived experience of aphasia were identified. People with lived experience and health professionals rated the importance of each recommendation through a two-round e-Delphi exercise. Recommendations were then ranked for importance and feasibility and analysed using a graph theory–based voting system. In Phase 2, shortlisted recommendations from Phase 1 were converted into quality indicators for appraisal and voting in consensus meetings. In Phase 3, priorities for implementation were established by people with lived experience and health professionals following discussion and anonymous voting.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Findings</h3>\\n \\n <p>In Phase 1, 23 best practice recommendations were identified and rated by people with lived experience (<i>n</i> = 26) and health professionals (<i>n</i> = 81). Ten recommendations were shortlisted. In Phase 2, people with lived experience (<i>n</i> = 4) and health professionals (<i>n</i> = 17) reached a consensus on 11 quality indicators, relating to assessment (<i>n</i> = 2), information provision (<i>n</i> = 3), communication partner training (<i>n</i> = 3), goal setting (<i>n</i> = 1), person and family-centred care (<i>n</i> = 1) and provision of treatment (<i>n</i> = 1). In Phase 3, people with lived experience (<i>n</i> = 5) and health professionals (<i>n</i> = 7) identified three implementation priorities: assessment of aphasia, provision of aphasia-friendly information and provision of therapy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Interpretation</h3>\\n \\n <p>Our 11 quality indicators and 3 implementation priorities are the first step to enabling systematic, efficient and person-centred measurement and quality improvement in post-stroke aphasia services. Quality indicators will be embedded in routine data collection systems, and strategies will be developed to address implementation priorities.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Patient and Public Contribution</h3>\\n \\n <p>Protocol development was informed by our previous research, which explored the perspectives of 23 people living with aphasia about best practice aphasia services. Individuals with lived experience of aphasia participated as expert panel members in our three consensus meetings. We received support from consumer advisory networks associated with the Centre for Research Excellence in Aphasia Rehabilitation and Recovery and the Queensland Aphasia Research Centre.</p>\\n </section>\\n </div>\",\"PeriodicalId\":55070,\"journal\":{\"name\":\"Health Expectations\",\"volume\":\"27 5\",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11369030/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Expectations\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/hex.14173\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Expectations","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/hex.14173","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Establishing Quality Indicators and Implementation Priorities for Post-Stroke Aphasia Services Through End-User Involvement
Background
Currently, there are no agreed quality standards for post-stroke aphasia services. Therefore, it is unknown if care reflects best practices or meets the expectations of people living with aphasia. We aimed to (1) shortlist, (2) operationalise and (3) prioritise best practice recommendations for post-stroke aphasia care.
Methods
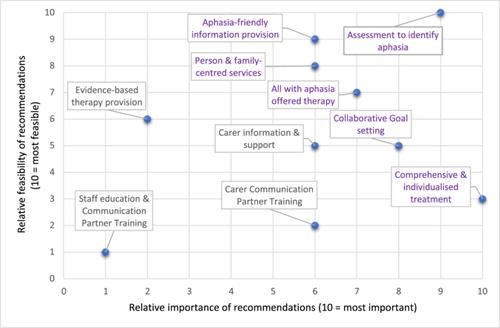
Three phases of research were conducted. In Phase 1, recommendations with strong evidence and/or known to be important to people with lived experience of aphasia were identified. People with lived experience and health professionals rated the importance of each recommendation through a two-round e-Delphi exercise. Recommendations were then ranked for importance and feasibility and analysed using a graph theory–based voting system. In Phase 2, shortlisted recommendations from Phase 1 were converted into quality indicators for appraisal and voting in consensus meetings. In Phase 3, priorities for implementation were established by people with lived experience and health professionals following discussion and anonymous voting.
Findings
In Phase 1, 23 best practice recommendations were identified and rated by people with lived experience (n = 26) and health professionals (n = 81). Ten recommendations were shortlisted. In Phase 2, people with lived experience (n = 4) and health professionals (n = 17) reached a consensus on 11 quality indicators, relating to assessment (n = 2), information provision (n = 3), communication partner training (n = 3), goal setting (n = 1), person and family-centred care (n = 1) and provision of treatment (n = 1). In Phase 3, people with lived experience (n = 5) and health professionals (n = 7) identified three implementation priorities: assessment of aphasia, provision of aphasia-friendly information and provision of therapy.
Interpretation
Our 11 quality indicators and 3 implementation priorities are the first step to enabling systematic, efficient and person-centred measurement and quality improvement in post-stroke aphasia services. Quality indicators will be embedded in routine data collection systems, and strategies will be developed to address implementation priorities.
Patient and Public Contribution
Protocol development was informed by our previous research, which explored the perspectives of 23 people living with aphasia about best practice aphasia services. Individuals with lived experience of aphasia participated as expert panel members in our three consensus meetings. We received support from consumer advisory networks associated with the Centre for Research Excellence in Aphasia Rehabilitation and Recovery and the Queensland Aphasia Research Centre.
期刊介绍:
Health Expectations promotes critical thinking and informed debate about all aspects of patient and public involvement and engagement (PPIE) in health and social care, health policy and health services research including:
• Person-centred care and quality improvement
• Patients'' participation in decisions about disease prevention and management
• Public perceptions of health services
• Citizen involvement in health care policy making and priority-setting
• Methods for monitoring and evaluating participation
• Empowerment and consumerism
• Patients'' role in safety and quality
• Patient and public role in health services research
• Co-production (researchers working with patients and the public) of research, health care and policy
Health Expectations is a quarterly, peer-reviewed journal publishing original research, review articles and critical commentaries. It includes papers which clarify concepts, develop theories, and critically analyse and evaluate specific policies and practices. The Journal provides an inter-disciplinary and international forum in which researchers (including PPIE researchers) from a range of backgrounds and expertise can present their work to other researchers, policy-makers, health care professionals, managers, patients and consumer advocates.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


