Gillian M Nixon, David G McNamara, David S Armstrong
{"title":"抗IL-5疗法是治疗慢性重症哮喘的有效辅助手段。","authors":"Gillian M Nixon, David G McNamara, David S Armstrong","doi":"10.1111/jpc.16639","DOIUrl":null,"url":null,"abstract":"<p>https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010834.pub4/full?highlightAbstract=asthma%7Casthm</p><p>Farne HA, Wilson A, Milan S, Banchoff E, Yang F, Powell CVE. Anti-IL-5 therapies for asthma. Cochrane Database Syst. Rev. 2022; Issue 7: Art. No.: CD010834. DOI: 10.1002/14651858.CD010834.pub4. Accessed 23 December 2022.</p><p>The efficacy and safety of monoclonal anti-interleukin (IL)-5 antibodies (mepolizumab, reslizumab and benralizumab) for the treatment of chronic asthma, including both adults and children.<span><sup>1</sup></span> These treatments target IL-5 (mepolizumab and reslizumab) or the IL-5 receptor found on eosinophils and basophils (benralizumab), affecting the proliferation, maturation, activation, recruitment and survival of eosinophils.</p><p>Seventeen randomised controlled trials of anti-IL-5 therapy compared to placebo were included, six for mepolizumab (total of 2294 participants), five for reslizumab (2232 participants) and six for benralizumab (3888 participants). Seven included adult participants only, one (presented only in abstract form) included only children aged 6 to 17 years<span><sup>2</sup></span> and the remaining nine included adolescents aged over 12 years and adults. The majority of studies were considered to be at low risk of bias (15 studies), unclear in one study (the paediatric study presented only in abstract form)<span><sup>2</sup></span> and high in only one study of benralizumab that was terminated due to sponsor decision after randomising 13 participants. Using the GRADE system, evidence for all comparisons was considered to be high overall except for mepolizumab IV and reslizumab SC, which are not currently licensed delivery routes. The following summary is therefore limited to subcutaneous mepolizumab and benralizumab, the agents and routes currently funded for use in Australia and New Zealand.</p><p>Although children over 12 years were included in many of the studies in this review, results in adolescents were not reported separately and so a sub-group analysis could not be performed. This resulted in the review finding that there is insufficient data to reach a conclusion about efficacy and safety in this population. However, the single study exclusively in children and adolescents that was included in the review, with results only in abstract form, was consistent with the findings in adults.<span><sup>2</sup></span> That study has since been published and confirmed the efficacy of SC mepolizumab for 52 weeks in reducing asthma exacerbations requiring systemic corticosteroids (rate ratio 0.73; 95% CI 0.56–0.96; <i>P</i> = 0.027).<span><sup>5</sup></span> Treatment-emergent adverse events occurred in 42 (29%) of 146 participants in the mepolizumab group versus 16 (11%) of 144 participants in the placebo group.<span><sup>5</sup></span> Long-term safety of mepolizumab in 6–11 year old children with severe eosinophilic asthma has also been supported by an open label study (<i>n</i> = 30) which showed no treatment-related serious adverse events and improved asthma exacerbations and control compared to baseline.<span><sup>6</sup></span></p><p>There are increasing concerns about the safety of lifetime exposure to systemic corticosteroids with an increased risk of chronic adverse effects after only four lifetime short (5 day) courses<span><sup>7</sup></span> and recent calls for improved steroid stewardship.<span><sup>8</sup></span> Excess corticosteroid use places patients at risk of increased infection, gastrointestinal events, type 2 diabetes, fractures and cardiovascular and psychiatric complications.<span><sup>7</sup></span> Biologic agents will play a crucial role in reducing steroid exposure, particularly long-term use.</p><p>The use of biologic agents for the management of asthma sits in Step 5 of the latest Global Initiative for Asthma treatment algorithm.<span><sup>9</sup></span> Adolescents with eosinophilic asthma and at least two exacerbations requiring systemic corticosteroids per year despite at least medium dose inhaled corticosteroids, or poor control demonstrated by an Asthma Control Questionnaire<span><sup>10</sup></span> of ≥1.5, are likely to benefit from treatment with one of these agents. In practice, many of these young people are taking high dose inhaled corticosteroids and often using other agents.</p><p>Currently mepolizumab and benralizumab for subcutaneous use are funded by the Pharmaceutical Benefits Scheme (PBS) in Australia for adolescents who are aged over 12 years with uncontrolled severe asthma despite optimised asthma therapy and who have eosinophilia. Eosinophilia is defined as a blood eosinophil count in the last 12 months greater than or equal to 300 cells per microlitre, or greater than or equal to 150 cells per microlitre whilst receiving treatment with oral corticosteroids. Funding is available for mepolizumab and benralizumab on the Pharmac community schedule in New Zealand with similar requirements apart from a higher eosinophil count of 500 cells per microlitre. Pharmac NZ funding requires application from a respiratory specialist or immunologist whilst PBS Australia requires the patients be treated by a respiratory physician, clinical immunologist, allergist or general physician experienced in the management of patients with severe asthma. Reslizumab is not currently funded in Australia or New Zealand. Other ‘biologic’ agents for asthma, dupilumab (anti-IL-4 and IL-13 monoclonal antibody) and omalizumab (anti-IgE monoclonal antibody), are funded under the PBS for severe asthma in Australia, and omalizumab is funded in New Zealand.</p><p>Many patients may qualify for more than one monoclonal antibody therapy and there are no head-to-head studies to guide the first choice of biologic agent. However, patients who are only partially responsive to one treatment may respond to a change in agent even within a receptor class.<span><sup>11, 12</sup></span> The decision on the choice of agent should be shared between physician and patient, considering patient age (only omalizumab is funded at the current time for use in the 6–12 years age group), availability, co-morbid severe atopic dermatitis (dupilumab), IgE and eosinophil counts, need for maintenance oral corticosteroids (best steroid sparing evidence for mepolizumab, benralizumab and dupilumab<span><sup>13</sup></span>) and the preferred dosing regimen (2 weekly for dupilumab, 2–4 weekly variable dose for omalizumab, 4 weekly for mepolizumab and 8 weekly after the first 3 doses for benralizumab). Administrative requirements for use of these agents are relatively arduous, with strict eligibility criteria. Continuation of treatment beyond 6 months requires documentation of improvement in symptomatology in both New Zealand and Australia, and a reduction of at least 50% in systemic corticosteroid use in New Zealand. Only one biological agent is allowed at a time, and a break of 4 weeks is required between agents.</p><p>Whilst the large majority of children with asthma will be successfully managed with inhaled treatments, biologic agents are an important tool for the control of asthma exacerbations in those with the most severe disease, improving quality of life and reducing steroid exposure. Use of these agents is likely to become more common with new agents, changing criteria and emerging evidence in younger patients. Whilst of great benefit to patients, these treatments will have implications for services in terms of administrative requirements and accessing day-stay facilities for treatment.</p>","PeriodicalId":16648,"journal":{"name":"Journal of paediatrics and child health","volume":"60 10","pages":"613-615"},"PeriodicalIF":1.6000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16639","citationCount":"0","resultStr":"{\"title\":\"Anti-IL-5 treatments are a useful adjunct for treatment of chronic severe asthma\",\"authors\":\"Gillian M Nixon, David G McNamara, David S Armstrong\",\"doi\":\"10.1111/jpc.16639\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010834.pub4/full?highlightAbstract=asthma%7Casthm</p><p>Farne HA, Wilson A, Milan S, Banchoff E, Yang F, Powell CVE. Anti-IL-5 therapies for asthma. Cochrane Database Syst. Rev. 2022; Issue 7: Art. No.: CD010834. DOI: 10.1002/14651858.CD010834.pub4. Accessed 23 December 2022.</p><p>The efficacy and safety of monoclonal anti-interleukin (IL)-5 antibodies (mepolizumab, reslizumab and benralizumab) for the treatment of chronic asthma, including both adults and children.<span><sup>1</sup></span> These treatments target IL-5 (mepolizumab and reslizumab) or the IL-5 receptor found on eosinophils and basophils (benralizumab), affecting the proliferation, maturation, activation, recruitment and survival of eosinophils.</p><p>Seventeen randomised controlled trials of anti-IL-5 therapy compared to placebo were included, six for mepolizumab (total of 2294 participants), five for reslizumab (2232 participants) and six for benralizumab (3888 participants). Seven included adult participants only, one (presented only in abstract form) included only children aged 6 to 17 years<span><sup>2</sup></span> and the remaining nine included adolescents aged over 12 years and adults. The majority of studies were considered to be at low risk of bias (15 studies), unclear in one study (the paediatric study presented only in abstract form)<span><sup>2</sup></span> and high in only one study of benralizumab that was terminated due to sponsor decision after randomising 13 participants. Using the GRADE system, evidence for all comparisons was considered to be high overall except for mepolizumab IV and reslizumab SC, which are not currently licensed delivery routes. The following summary is therefore limited to subcutaneous mepolizumab and benralizumab, the agents and routes currently funded for use in Australia and New Zealand.</p><p>Although children over 12 years were included in many of the studies in this review, results in adolescents were not reported separately and so a sub-group analysis could not be performed. This resulted in the review finding that there is insufficient data to reach a conclusion about efficacy and safety in this population. However, the single study exclusively in children and adolescents that was included in the review, with results only in abstract form, was consistent with the findings in adults.<span><sup>2</sup></span> That study has since been published and confirmed the efficacy of SC mepolizumab for 52 weeks in reducing asthma exacerbations requiring systemic corticosteroids (rate ratio 0.73; 95% CI 0.56–0.96; <i>P</i> = 0.027).<span><sup>5</sup></span> Treatment-emergent adverse events occurred in 42 (29%) of 146 participants in the mepolizumab group versus 16 (11%) of 144 participants in the placebo group.<span><sup>5</sup></span> Long-term safety of mepolizumab in 6–11 year old children with severe eosinophilic asthma has also been supported by an open label study (<i>n</i> = 30) which showed no treatment-related serious adverse events and improved asthma exacerbations and control compared to baseline.<span><sup>6</sup></span></p><p>There are increasing concerns about the safety of lifetime exposure to systemic corticosteroids with an increased risk of chronic adverse effects after only four lifetime short (5 day) courses<span><sup>7</sup></span> and recent calls for improved steroid stewardship.<span><sup>8</sup></span> Excess corticosteroid use places patients at risk of increased infection, gastrointestinal events, type 2 diabetes, fractures and cardiovascular and psychiatric complications.<span><sup>7</sup></span> Biologic agents will play a crucial role in reducing steroid exposure, particularly long-term use.</p><p>The use of biologic agents for the management of asthma sits in Step 5 of the latest Global Initiative for Asthma treatment algorithm.<span><sup>9</sup></span> Adolescents with eosinophilic asthma and at least two exacerbations requiring systemic corticosteroids per year despite at least medium dose inhaled corticosteroids, or poor control demonstrated by an Asthma Control Questionnaire<span><sup>10</sup></span> of ≥1.5, are likely to benefit from treatment with one of these agents. In practice, many of these young people are taking high dose inhaled corticosteroids and often using other agents.</p><p>Currently mepolizumab and benralizumab for subcutaneous use are funded by the Pharmaceutical Benefits Scheme (PBS) in Australia for adolescents who are aged over 12 years with uncontrolled severe asthma despite optimised asthma therapy and who have eosinophilia. Eosinophilia is defined as a blood eosinophil count in the last 12 months greater than or equal to 300 cells per microlitre, or greater than or equal to 150 cells per microlitre whilst receiving treatment with oral corticosteroids. Funding is available for mepolizumab and benralizumab on the Pharmac community schedule in New Zealand with similar requirements apart from a higher eosinophil count of 500 cells per microlitre. Pharmac NZ funding requires application from a respiratory specialist or immunologist whilst PBS Australia requires the patients be treated by a respiratory physician, clinical immunologist, allergist or general physician experienced in the management of patients with severe asthma. Reslizumab is not currently funded in Australia or New Zealand. Other ‘biologic’ agents for asthma, dupilumab (anti-IL-4 and IL-13 monoclonal antibody) and omalizumab (anti-IgE monoclonal antibody), are funded under the PBS for severe asthma in Australia, and omalizumab is funded in New Zealand.</p><p>Many patients may qualify for more than one monoclonal antibody therapy and there are no head-to-head studies to guide the first choice of biologic agent. However, patients who are only partially responsive to one treatment may respond to a change in agent even within a receptor class.<span><sup>11, 12</sup></span> The decision on the choice of agent should be shared between physician and patient, considering patient age (only omalizumab is funded at the current time for use in the 6–12 years age group), availability, co-morbid severe atopic dermatitis (dupilumab), IgE and eosinophil counts, need for maintenance oral corticosteroids (best steroid sparing evidence for mepolizumab, benralizumab and dupilumab<span><sup>13</sup></span>) and the preferred dosing regimen (2 weekly for dupilumab, 2–4 weekly variable dose for omalizumab, 4 weekly for mepolizumab and 8 weekly after the first 3 doses for benralizumab). Administrative requirements for use of these agents are relatively arduous, with strict eligibility criteria. Continuation of treatment beyond 6 months requires documentation of improvement in symptomatology in both New Zealand and Australia, and a reduction of at least 50% in systemic corticosteroid use in New Zealand. Only one biological agent is allowed at a time, and a break of 4 weeks is required between agents.</p><p>Whilst the large majority of children with asthma will be successfully managed with inhaled treatments, biologic agents are an important tool for the control of asthma exacerbations in those with the most severe disease, improving quality of life and reducing steroid exposure. Use of these agents is likely to become more common with new agents, changing criteria and emerging evidence in younger patients. Whilst of great benefit to patients, these treatments will have implications for services in terms of administrative requirements and accessing day-stay facilities for treatment.</p>\",\"PeriodicalId\":16648,\"journal\":{\"name\":\"Journal of paediatrics and child health\",\"volume\":\"60 10\",\"pages\":\"613-615\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16639\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of paediatrics and child health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16639\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of paediatrics and child health","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16639","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Farne HA, Wilson A, Milan S, Banchoff E, Yang F, Powell CVE. Anti-IL-5 therapies for asthma. Cochrane Database Syst. Rev. 2022; Issue 7: Art. No.: CD010834. DOI: 10.1002/14651858.CD010834.pub4. Accessed 23 December 2022.
The efficacy and safety of monoclonal anti-interleukin (IL)-5 antibodies (mepolizumab, reslizumab and benralizumab) for the treatment of chronic asthma, including both adults and children.1 These treatments target IL-5 (mepolizumab and reslizumab) or the IL-5 receptor found on eosinophils and basophils (benralizumab), affecting the proliferation, maturation, activation, recruitment and survival of eosinophils.
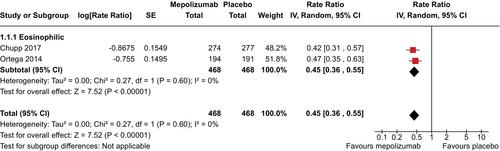
Seventeen randomised controlled trials of anti-IL-5 therapy compared to placebo were included, six for mepolizumab (total of 2294 participants), five for reslizumab (2232 participants) and six for benralizumab (3888 participants). Seven included adult participants only, one (presented only in abstract form) included only children aged 6 to 17 years2 and the remaining nine included adolescents aged over 12 years and adults. The majority of studies were considered to be at low risk of bias (15 studies), unclear in one study (the paediatric study presented only in abstract form)2 and high in only one study of benralizumab that was terminated due to sponsor decision after randomising 13 participants. Using the GRADE system, evidence for all comparisons was considered to be high overall except for mepolizumab IV and reslizumab SC, which are not currently licensed delivery routes. The following summary is therefore limited to subcutaneous mepolizumab and benralizumab, the agents and routes currently funded for use in Australia and New Zealand.
Although children over 12 years were included in many of the studies in this review, results in adolescents were not reported separately and so a sub-group analysis could not be performed. This resulted in the review finding that there is insufficient data to reach a conclusion about efficacy and safety in this population. However, the single study exclusively in children and adolescents that was included in the review, with results only in abstract form, was consistent with the findings in adults.2 That study has since been published and confirmed the efficacy of SC mepolizumab for 52 weeks in reducing asthma exacerbations requiring systemic corticosteroids (rate ratio 0.73; 95% CI 0.56–0.96; P = 0.027).5 Treatment-emergent adverse events occurred in 42 (29%) of 146 participants in the mepolizumab group versus 16 (11%) of 144 participants in the placebo group.5 Long-term safety of mepolizumab in 6–11 year old children with severe eosinophilic asthma has also been supported by an open label study (n = 30) which showed no treatment-related serious adverse events and improved asthma exacerbations and control compared to baseline.6
There are increasing concerns about the safety of lifetime exposure to systemic corticosteroids with an increased risk of chronic adverse effects after only four lifetime short (5 day) courses7 and recent calls for improved steroid stewardship.8 Excess corticosteroid use places patients at risk of increased infection, gastrointestinal events, type 2 diabetes, fractures and cardiovascular and psychiatric complications.7 Biologic agents will play a crucial role in reducing steroid exposure, particularly long-term use.
The use of biologic agents for the management of asthma sits in Step 5 of the latest Global Initiative for Asthma treatment algorithm.9 Adolescents with eosinophilic asthma and at least two exacerbations requiring systemic corticosteroids per year despite at least medium dose inhaled corticosteroids, or poor control demonstrated by an Asthma Control Questionnaire10 of ≥1.5, are likely to benefit from treatment with one of these agents. In practice, many of these young people are taking high dose inhaled corticosteroids and often using other agents.
Currently mepolizumab and benralizumab for subcutaneous use are funded by the Pharmaceutical Benefits Scheme (PBS) in Australia for adolescents who are aged over 12 years with uncontrolled severe asthma despite optimised asthma therapy and who have eosinophilia. Eosinophilia is defined as a blood eosinophil count in the last 12 months greater than or equal to 300 cells per microlitre, or greater than or equal to 150 cells per microlitre whilst receiving treatment with oral corticosteroids. Funding is available for mepolizumab and benralizumab on the Pharmac community schedule in New Zealand with similar requirements apart from a higher eosinophil count of 500 cells per microlitre. Pharmac NZ funding requires application from a respiratory specialist or immunologist whilst PBS Australia requires the patients be treated by a respiratory physician, clinical immunologist, allergist or general physician experienced in the management of patients with severe asthma. Reslizumab is not currently funded in Australia or New Zealand. Other ‘biologic’ agents for asthma, dupilumab (anti-IL-4 and IL-13 monoclonal antibody) and omalizumab (anti-IgE monoclonal antibody), are funded under the PBS for severe asthma in Australia, and omalizumab is funded in New Zealand.
Many patients may qualify for more than one monoclonal antibody therapy and there are no head-to-head studies to guide the first choice of biologic agent. However, patients who are only partially responsive to one treatment may respond to a change in agent even within a receptor class.11, 12 The decision on the choice of agent should be shared between physician and patient, considering patient age (only omalizumab is funded at the current time for use in the 6–12 years age group), availability, co-morbid severe atopic dermatitis (dupilumab), IgE and eosinophil counts, need for maintenance oral corticosteroids (best steroid sparing evidence for mepolizumab, benralizumab and dupilumab13) and the preferred dosing regimen (2 weekly for dupilumab, 2–4 weekly variable dose for omalizumab, 4 weekly for mepolizumab and 8 weekly after the first 3 doses for benralizumab). Administrative requirements for use of these agents are relatively arduous, with strict eligibility criteria. Continuation of treatment beyond 6 months requires documentation of improvement in symptomatology in both New Zealand and Australia, and a reduction of at least 50% in systemic corticosteroid use in New Zealand. Only one biological agent is allowed at a time, and a break of 4 weeks is required between agents.
Whilst the large majority of children with asthma will be successfully managed with inhaled treatments, biologic agents are an important tool for the control of asthma exacerbations in those with the most severe disease, improving quality of life and reducing steroid exposure. Use of these agents is likely to become more common with new agents, changing criteria and emerging evidence in younger patients. Whilst of great benefit to patients, these treatments will have implications for services in terms of administrative requirements and accessing day-stay facilities for treatment.
期刊介绍:
The Journal of Paediatrics and Child Health publishes original research articles of scientific excellence in paediatrics and child health. Research Articles, Case Reports and Letters to the Editor are published, together with invited Reviews, Annotations, Editorial Comments and manuscripts of educational interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


