Maryam Barkhordarian, Mark Grijalva, Albert Lee, Amer Jarri, Anna Belyayeva, Simcha Weissman
{"title":"他汀类药物诱发的自身免疫性肌病:肌肉无力的诊断难题。","authors":"Maryam Barkhordarian, Mark Grijalva, Albert Lee, Amer Jarri, Anna Belyayeva, Simcha Weissman","doi":"10.12659/AJCR.944261","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Statin-induced myopathy can present with symptoms ranging from mild myalgia to significant muscle weakness. Muscle-related adverse effects of statins have been very challenging in clinical practice and they necessitate high clinical suspicion. This case report highlights how statin-induced autoimmune myopathy often goes undiagnosed. CASE REPORT We present a 69-year-old man with a past medical history of coronary artery disease who presented with myalgia and progressive proximal muscle weakness for 2 months, with a creatinine kinase of 8323 U/L. Atorvastatin was held on admission and the patient received intravenous (IV) fluid as treatment for presumed rhabdomyolysis. Although CK was trending down, he did not show significant improvement in muscle weakness or myalgia. At this point, myositis was suspected, so a myositis panel including anti-HMG Co-A reductase antibody was ordered and he was started on IV steroids. Anti-HMG Co-A reductase antibody was positive, and the rest of myopathy workup was negative. Meanwhile, the patient's muscle weakness significantly improved with IV steroid. He was discharged on methylprednisolone with close outpatient rheumatology follow-up. CONCLUSIONS Muscle-related adverse effects of statins, including rhabdomyolysis and myopathy, can fail to respond to conservative management. It is crucial to identify and manage statin-induced autoimmune myopathy as a possible differential diagnosis in patients with muscle weakness and elevated CK while on statin therapy who do not respond to intravenous fluid alone.</p>","PeriodicalId":39064,"journal":{"name":"American Journal of Case Reports","volume":"25 ","pages":"e944261"},"PeriodicalIF":0.7000,"publicationDate":"2024-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11380920/pdf/","citationCount":"0","resultStr":"{\"title\":\"Statin-Induced Autoimmune Myopathy: A Diagnostic Challenge in Muscle Weakness.\",\"authors\":\"Maryam Barkhordarian, Mark Grijalva, Albert Lee, Amer Jarri, Anna Belyayeva, Simcha Weissman\",\"doi\":\"10.12659/AJCR.944261\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND Statin-induced myopathy can present with symptoms ranging from mild myalgia to significant muscle weakness. Muscle-related adverse effects of statins have been very challenging in clinical practice and they necessitate high clinical suspicion. This case report highlights how statin-induced autoimmune myopathy often goes undiagnosed. CASE REPORT We present a 69-year-old man with a past medical history of coronary artery disease who presented with myalgia and progressive proximal muscle weakness for 2 months, with a creatinine kinase of 8323 U/L. Atorvastatin was held on admission and the patient received intravenous (IV) fluid as treatment for presumed rhabdomyolysis. Although CK was trending down, he did not show significant improvement in muscle weakness or myalgia. At this point, myositis was suspected, so a myositis panel including anti-HMG Co-A reductase antibody was ordered and he was started on IV steroids. Anti-HMG Co-A reductase antibody was positive, and the rest of myopathy workup was negative. Meanwhile, the patient's muscle weakness significantly improved with IV steroid. He was discharged on methylprednisolone with close outpatient rheumatology follow-up. CONCLUSIONS Muscle-related adverse effects of statins, including rhabdomyolysis and myopathy, can fail to respond to conservative management. It is crucial to identify and manage statin-induced autoimmune myopathy as a possible differential diagnosis in patients with muscle weakness and elevated CK while on statin therapy who do not respond to intravenous fluid alone.</p>\",\"PeriodicalId\":39064,\"journal\":{\"name\":\"American Journal of Case Reports\",\"volume\":\"25 \",\"pages\":\"e944261\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11380920/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12659/AJCR.944261\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.944261","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Statin-Induced Autoimmune Myopathy: A Diagnostic Challenge in Muscle Weakness.
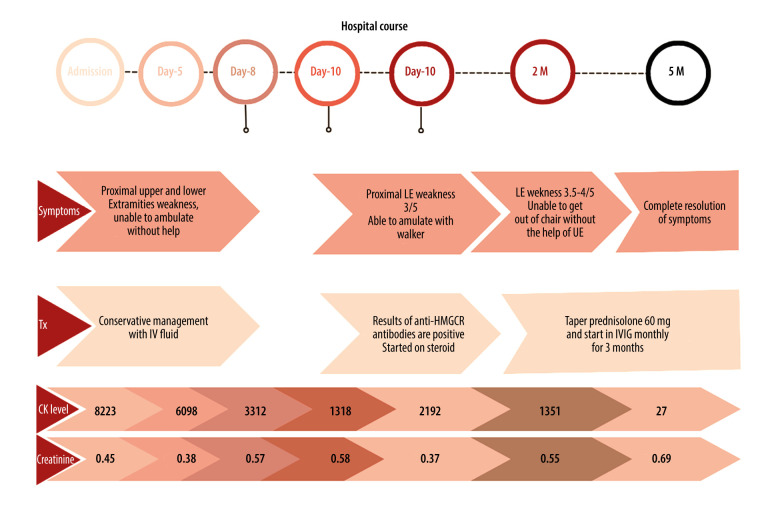
BACKGROUND Statin-induced myopathy can present with symptoms ranging from mild myalgia to significant muscle weakness. Muscle-related adverse effects of statins have been very challenging in clinical practice and they necessitate high clinical suspicion. This case report highlights how statin-induced autoimmune myopathy often goes undiagnosed. CASE REPORT We present a 69-year-old man with a past medical history of coronary artery disease who presented with myalgia and progressive proximal muscle weakness for 2 months, with a creatinine kinase of 8323 U/L. Atorvastatin was held on admission and the patient received intravenous (IV) fluid as treatment for presumed rhabdomyolysis. Although CK was trending down, he did not show significant improvement in muscle weakness or myalgia. At this point, myositis was suspected, so a myositis panel including anti-HMG Co-A reductase antibody was ordered and he was started on IV steroids. Anti-HMG Co-A reductase antibody was positive, and the rest of myopathy workup was negative. Meanwhile, the patient's muscle weakness significantly improved with IV steroid. He was discharged on methylprednisolone with close outpatient rheumatology follow-up. CONCLUSIONS Muscle-related adverse effects of statins, including rhabdomyolysis and myopathy, can fail to respond to conservative management. It is crucial to identify and manage statin-induced autoimmune myopathy as a possible differential diagnosis in patients with muscle weakness and elevated CK while on statin therapy who do not respond to intravenous fluid alone.
期刊介绍:
American Journal of Case Reports is an international, peer-reviewed scientific journal that publishes single and series case reports in all medical fields. American Journal of Case Reports is issued on a continuous basis as a primary electronic journal. Print copies of a single article or a set of articles can be ordered on demand.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


