肾功能和肾动脉解剖方面作为肾脏去神经支配的适应症。
IF 4.3
2区 医学
Q1 PERIPHERAL VASCULAR DISEASE
引用次数: 0
摘要
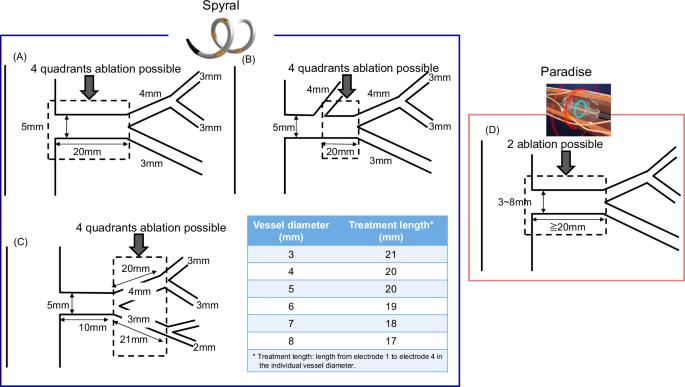
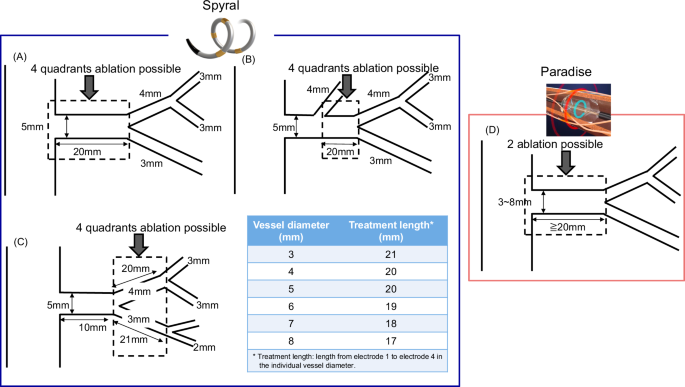
肾脏去神经支配(RDN)是一种微创、基于血管内导管的手术,使用射频、超声或酒精介导消融来治疗耐药性高血压。随着肾交感神经作为高血压的病因和治疗目标受到越来越多的关注,了解肾动脉的解剖结构可能对确定血管内治疗策略以及未来选择设备和 RDN 治疗的合适人选具有重要意义。然而,肾动脉(RA)的解剖结构复杂,缺乏对肾动脉结构的标准化形态学评估。计算机断层扫描血管造影或磁共振血管造影成像有助于在进行 RDN 之前评估 RA 的解剖结构。RA 超声心动图是一种成熟的无创筛查方法,可筛查明显的狭窄。主要的随机对照试验仅限于肾功能保持良好的患者参加,肾功能保持良好通常是指估计肾小球滤过率(eGFR)≥ 45 mL/min/1.73 m2。因此,RDN 的肾功能水平尚未确定。本微型综述总结了构成肾脏去神经支配适应症的肾动脉解剖和肾功能特征。(临床试验的作用:K. Kario 是 Spyral OFF MED、Spyral ON MED、DUO 和 REQUIRE 的执行委员会主要研究者;TCD-16164 研究的协调研究者;HTN-J、Spyral OFF MED、Spyral ON MED、DUO、REQUIRE 和 TCD-16164 研究的现场主要研究者)。评估射频肾脏去神经支配的肾动脉。A 在主肾动脉或与主肾动脉相当的肾动脉的四个部位同时进行象限消融。B 如果主肾动脉中部有直径大于 3 毫米的肾动脉分支,则该分支为主肾动脉的远端。在这种情况下,可对等同的肾动脉同时进行四次象限消融。C 可以在肾动脉分支上同时进行四次象限消融。D 超声波消融应至少间隔 5 毫米(一个探头*)。在动脉分叉近端 2 至 3 毫米处进行。在腹主动脉入口远端 2 至 3 毫米处进行。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Aspects of renal function and renal artery anatomy as indications for renal denervation
Renal denervation (RDN) is a minimally invasive, endovascular catheter-based procedure using radiofrequency, ultrasound, or alcohol-mediated ablation to treat resistant hypertension. As more attention is focused on the renal sympathetic nerve as a cause and treatment target of hypertension, understanding the anatomy of the renal artery may have important implications for determining endovascular treatment strategies as well as for future selection of devices and appropriate candidates for RDN treatment. However, the anatomical structure of the renal artery (RA) is complex, and standardized morphological evaluations of the RA structure are lacking. Computed tomography angiography or magnetic resonance angiography imaging is useful for assessing RA anatomy before conducting RDN. RA echocardiography is an established noninvasive screening method for significant stenosis. Major randomized controlled trials have limited enrollment to patients with preserved renal function, usually defined as an estimated glomerular filtration rate (eGFR) ≥ 45 mL/min/1.73 m2. Therefore, the level of renal function at which RDN is indicated has not yet been determined. This mini-review summarizes the characteristics of renal artery anatomy and renal function that constitute indications for renal denervation. (Role of Clinical Trials: K. Kario is an Executive Committee Principal Investigator for the Spyral OFF MED, the Spyral ON MED, the DUO and the REQUIRE; a Coordinating investigator for the TCD-16164 study; a Site Principal Investigator for the HTN-J, the Spyral OFF MED, the Spyral ON MED, the DUO, the REQUIRE and the TCD-16164 study). Evaluation of renal arteries for radiofrequency renal denervation. (A) Simultaneous quadrantal ablations at four sites in the main renal artery or the equivalent renal artery to the main renal artery. (B) If there is a renal artery branch with a diameter >3 mm in the middle of the main renal artery, this branch is the distal end of the main renal artery. In this case, four simultaneous and quadrantal ablations can be performed on the equivalent renal arteries. (C) Four simultaneous and quadrantal ablations can be performed in the branch renal artery. (D) Sonication should be spaced at least 5 mm (one transducer*) apart. Perform 2 to 3 mm proximal to the arterial bifurcation. Perform 2 to 3 mm distal to the abdominal aortic inlet.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Hypertension Research
医学-外周血管病
CiteScore
7.40
自引率
16.70%
发文量
249
审稿时长
3-8 weeks
期刊介绍:
Hypertension Research is the official publication of the Japanese Society of Hypertension. The journal publishes papers reporting original clinical and experimental research that contribute to the advancement of knowledge in the field of hypertension and related cardiovascular diseases. The journal publishes Review Articles, Articles, Correspondence and Comments.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


