Muhammad Omar Larik, Ayesha Ahmed, Abdul Rehman Shahid, Hamza Irfan, Areeka Irfan, Muhammad Jibran
{"title":"既往冠状动脉旁路移植术对经皮冠状动脉介入治疗后临床结果的影响:对 250 684 例患者的 Meta 分析。","authors":"Muhammad Omar Larik, Ayesha Ahmed, Abdul Rehman Shahid, Hamza Irfan, Areeka Irfan, Muhammad Jibran","doi":"10.1177/11795468241274588","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Percutaneous coronary intervention (PCI), also known as coronary angioplasty, is the preferred strategy for treating obstructive coronary artery disease. Existing literature suggests the worsening of clinical outcomes in patients with previous coronary artery bypass grafting (CABG) history. In light of this, a comprehensive systematic review and meta-analysis was performed.</p><p><strong>Methods: </strong>Databases including PubMed, Cochrane Library, and ScienceDirect were utilized for the inclusive systematic search dating from inception to September 01, 2023. The risk of bias assessment was performed using the Newcastle-Ottawa scale for cohort studies, and the Cochrane Risk of Bias Tool for randomized controlled trials.</p><p><strong>Results: </strong>Ultimately, there were 16 eligible studies pooled together, involving a total of 250 684 patients, including 231 552 CABG-naïve patients, and 19 132 patients with a prior history of CABG. Overall, patients with CABG history were associated with significantly greater short-term mortality (<i>P</i> = .004), long-term mortality (<i>P</i> = .005), myocardial infarction (<i>P</i> < .00001), major adverse cardiovascular events (<i>P</i> = .0001), and procedural perforation (<i>P</i> < .00001). Contrastingly, CABG-naïve patients were associated with significantly greater risk of cardiac tamponade (<i>P</i> = .02) and repeat CABG (<i>P</i> = .03). No significant differences in stroke, bleeding, revascularization, or repeat PCI were observed.</p><p><strong>Conclusion: </strong>Comparatively worsened clinical outcomes were observed, as patients with prior CABG history typically exhibit complex coronary anatomy, and have higher rates of comorbidities in comparison to their CABG-naïve counterparts. The refinement of current procedural and surgical techniques, in conjunction with continued research endeavors, are needed in order to effectively address this trend.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"18 ","pages":"11795468241274588"},"PeriodicalIF":3.3000,"publicationDate":"2024-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11366107/pdf/","citationCount":"0","resultStr":"{\"title\":\"Influence of Previous Coronary Artery Bypass Grafting on Clinical Outcomes After Percutaneous Coronary Intervention: A Meta-Analysis of 250 684 Patients.\",\"authors\":\"Muhammad Omar Larik, Ayesha Ahmed, Abdul Rehman Shahid, Hamza Irfan, Areeka Irfan, Muhammad Jibran\",\"doi\":\"10.1177/11795468241274588\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Percutaneous coronary intervention (PCI), also known as coronary angioplasty, is the preferred strategy for treating obstructive coronary artery disease. Existing literature suggests the worsening of clinical outcomes in patients with previous coronary artery bypass grafting (CABG) history. In light of this, a comprehensive systematic review and meta-analysis was performed.</p><p><strong>Methods: </strong>Databases including PubMed, Cochrane Library, and ScienceDirect were utilized for the inclusive systematic search dating from inception to September 01, 2023. The risk of bias assessment was performed using the Newcastle-Ottawa scale for cohort studies, and the Cochrane Risk of Bias Tool for randomized controlled trials.</p><p><strong>Results: </strong>Ultimately, there were 16 eligible studies pooled together, involving a total of 250 684 patients, including 231 552 CABG-naïve patients, and 19 132 patients with a prior history of CABG. Overall, patients with CABG history were associated with significantly greater short-term mortality (<i>P</i> = .004), long-term mortality (<i>P</i> = .005), myocardial infarction (<i>P</i> < .00001), major adverse cardiovascular events (<i>P</i> = .0001), and procedural perforation (<i>P</i> < .00001). Contrastingly, CABG-naïve patients were associated with significantly greater risk of cardiac tamponade (<i>P</i> = .02) and repeat CABG (<i>P</i> = .03). No significant differences in stroke, bleeding, revascularization, or repeat PCI were observed.</p><p><strong>Conclusion: </strong>Comparatively worsened clinical outcomes were observed, as patients with prior CABG history typically exhibit complex coronary anatomy, and have higher rates of comorbidities in comparison to their CABG-naïve counterparts. The refinement of current procedural and surgical techniques, in conjunction with continued research endeavors, are needed in order to effectively address this trend.</p>\",\"PeriodicalId\":10419,\"journal\":{\"name\":\"Clinical Medicine Insights. Cardiology\",\"volume\":\"18 \",\"pages\":\"11795468241274588\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11366107/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795468241274588\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795468241274588","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Influence of Previous Coronary Artery Bypass Grafting on Clinical Outcomes After Percutaneous Coronary Intervention: A Meta-Analysis of 250 684 Patients.
Background: Percutaneous coronary intervention (PCI), also known as coronary angioplasty, is the preferred strategy for treating obstructive coronary artery disease. Existing literature suggests the worsening of clinical outcomes in patients with previous coronary artery bypass grafting (CABG) history. In light of this, a comprehensive systematic review and meta-analysis was performed.
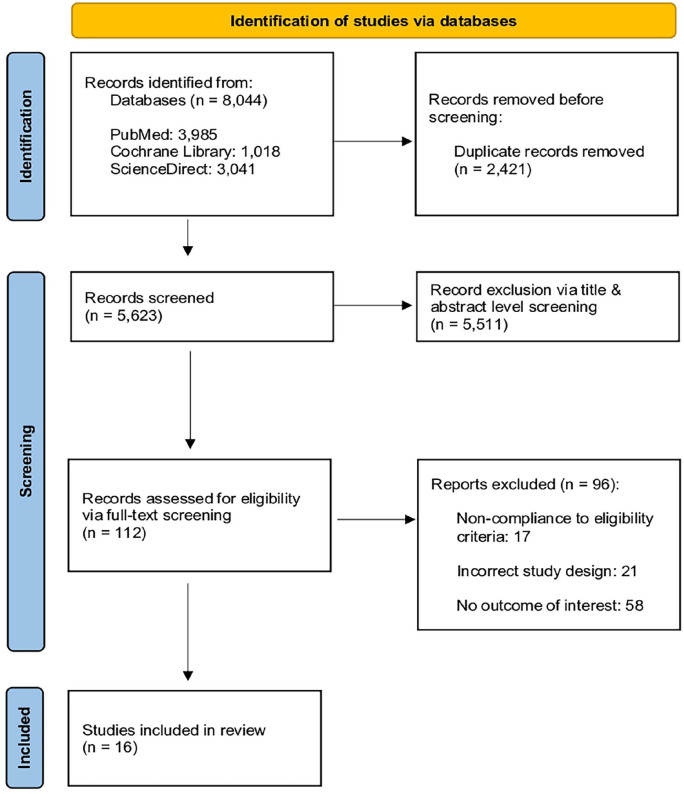
Methods: Databases including PubMed, Cochrane Library, and ScienceDirect were utilized for the inclusive systematic search dating from inception to September 01, 2023. The risk of bias assessment was performed using the Newcastle-Ottawa scale for cohort studies, and the Cochrane Risk of Bias Tool for randomized controlled trials.
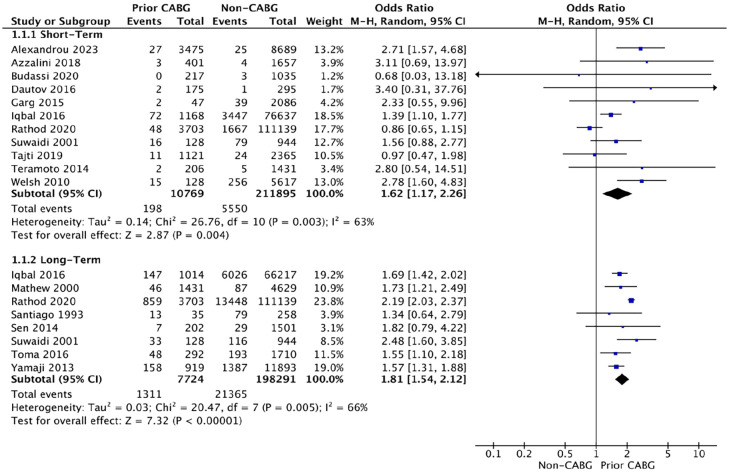
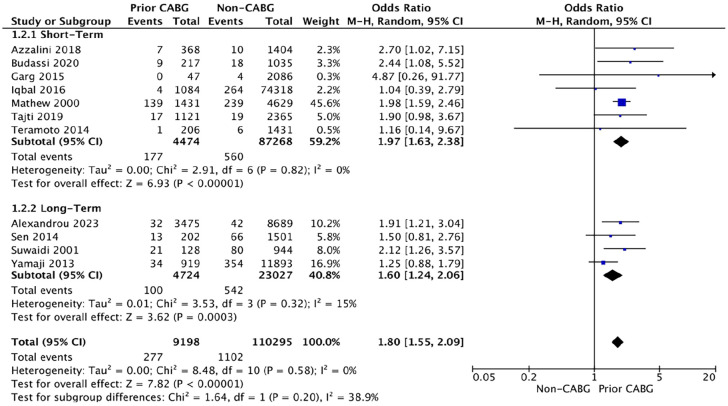
Results: Ultimately, there were 16 eligible studies pooled together, involving a total of 250 684 patients, including 231 552 CABG-naïve patients, and 19 132 patients with a prior history of CABG. Overall, patients with CABG history were associated with significantly greater short-term mortality (P = .004), long-term mortality (P = .005), myocardial infarction (P < .00001), major adverse cardiovascular events (P = .0001), and procedural perforation (P < .00001). Contrastingly, CABG-naïve patients were associated with significantly greater risk of cardiac tamponade (P = .02) and repeat CABG (P = .03). No significant differences in stroke, bleeding, revascularization, or repeat PCI were observed.
Conclusion: Comparatively worsened clinical outcomes were observed, as patients with prior CABG history typically exhibit complex coronary anatomy, and have higher rates of comorbidities in comparison to their CABG-naïve counterparts. The refinement of current procedural and surgical techniques, in conjunction with continued research endeavors, are needed in order to effectively address this trend.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


