Gad Cotter, Beth A. Davison, Yonathan Freund, Adriaan A. Voors, Christopher Edwards, Maria Novosadova, Koji Takagi, Hamlet Hayrapetyan, Andranik Mshetsyan, Drambyan Mayranush, Alain Cohen-Solal, Jozine M. ter Maaten, Jan Biegus, Piotr Ponikowski, Gerasimos Filippatos, Ovidiu Chioncel, Malha Sadoune, Matteo Pagnesi, Tabassome Simon, Marco Metra, Douglas L. Mann, Alexandre Mebazaa
{"title":"急性心力衰竭的类固醇脉冲疗法:CORTAHF 随机、开放标签试点试验","authors":"Gad Cotter, Beth A. Davison, Yonathan Freund, Adriaan A. Voors, Christopher Edwards, Maria Novosadova, Koji Takagi, Hamlet Hayrapetyan, Andranik Mshetsyan, Drambyan Mayranush, Alain Cohen-Solal, Jozine M. ter Maaten, Jan Biegus, Piotr Ponikowski, Gerasimos Filippatos, Ovidiu Chioncel, Malha Sadoune, Matteo Pagnesi, Tabassome Simon, Marco Metra, Douglas L. Mann, Alexandre Mebazaa","doi":"10.1002/ejhf.3452","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>Burst steroid therapy, effective in acute respiratory diseases, may benefit patients with acute heart failure (AHF) in whom inflammatory activation is associated with adverse outcomes.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>CORTAHF assessed whether burst steroid therapy reduces inflammation and results in better quality of life and clinical outcomes in AHF. Patients with AHF, N-terminal pro-B-type natriuretic peptide >1500 pg/ml, and high-sensitivity C-reactive protein (hsCRP) >20 mg/L were randomized 1:1 to oral, once daily 40 mg prednisone for 7 days or usual care, without blinding. Patients were followed for 90 days. A total of 101 patients were randomized. At day 7 the primary endpoint, hsCRP decreased in both arms – adjusted geometric mean ratios (GMRs) were 0.30 and 0.40 in the prednisone and usual care arms (ratio of GMRs 0.75, 95% confidence interval [CI] 0.56–1.00, <i>p</i> = 0.0498). The 90-day risk of worsening heart failure (HF), HF readmission or death as reported by the unblinded investigators was significantly lower in the prednisone group (10.4%) than in usual care (30.8%) (hazard ratio 0.31, 95% CI 0.11–0.86, <i>p</i> = 0.016). The EQ-5D visual analogue scale score as reported by the unblinded patients increased more in the prednisone group on day 7 (least squares mean difference 2.57, 95% CI 0.12–5.01 points, <i>p</i> = 0.040). All effects were statistically significant in the pre-specified subgroup with centrally-measured interleukin-6 >13 pg/ml. Adverse events, particularly hyperglycaemia, occurred more in the prednisone group with no difference in infection rate.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In this small open-label study of patients with AHF, burst steroid therapy was associated with reduced inflammation as measured by hsCRP levels at day 7 (primary endpoint). Secondary endpoints showed improved quality of life at day 7 and reduced 90-day risk of death or worsening HF. Large prospective studies are needed to evaluate these findings.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"26 10","pages":"2282-2292"},"PeriodicalIF":16.9000,"publicationDate":"2024-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3452","citationCount":"0","resultStr":"{\"title\":\"Burst steroid therapy for acute heart failure: The CORTAHF randomized, open-label, pilot trial\",\"authors\":\"Gad Cotter, Beth A. Davison, Yonathan Freund, Adriaan A. Voors, Christopher Edwards, Maria Novosadova, Koji Takagi, Hamlet Hayrapetyan, Andranik Mshetsyan, Drambyan Mayranush, Alain Cohen-Solal, Jozine M. ter Maaten, Jan Biegus, Piotr Ponikowski, Gerasimos Filippatos, Ovidiu Chioncel, Malha Sadoune, Matteo Pagnesi, Tabassome Simon, Marco Metra, Douglas L. Mann, Alexandre Mebazaa\",\"doi\":\"10.1002/ejhf.3452\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Burst steroid therapy, effective in acute respiratory diseases, may benefit patients with acute heart failure (AHF) in whom inflammatory activation is associated with adverse outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>CORTAHF assessed whether burst steroid therapy reduces inflammation and results in better quality of life and clinical outcomes in AHF. Patients with AHF, N-terminal pro-B-type natriuretic peptide >1500 pg/ml, and high-sensitivity C-reactive protein (hsCRP) >20 mg/L were randomized 1:1 to oral, once daily 40 mg prednisone for 7 days or usual care, without blinding. Patients were followed for 90 days. A total of 101 patients were randomized. At day 7 the primary endpoint, hsCRP decreased in both arms – adjusted geometric mean ratios (GMRs) were 0.30 and 0.40 in the prednisone and usual care arms (ratio of GMRs 0.75, 95% confidence interval [CI] 0.56–1.00, <i>p</i> = 0.0498). The 90-day risk of worsening heart failure (HF), HF readmission or death as reported by the unblinded investigators was significantly lower in the prednisone group (10.4%) than in usual care (30.8%) (hazard ratio 0.31, 95% CI 0.11–0.86, <i>p</i> = 0.016). The EQ-5D visual analogue scale score as reported by the unblinded patients increased more in the prednisone group on day 7 (least squares mean difference 2.57, 95% CI 0.12–5.01 points, <i>p</i> = 0.040). All effects were statistically significant in the pre-specified subgroup with centrally-measured interleukin-6 >13 pg/ml. Adverse events, particularly hyperglycaemia, occurred more in the prednisone group with no difference in infection rate.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In this small open-label study of patients with AHF, burst steroid therapy was associated with reduced inflammation as measured by hsCRP levels at day 7 (primary endpoint). Secondary endpoints showed improved quality of life at day 7 and reduced 90-day risk of death or worsening HF. Large prospective studies are needed to evaluate these findings.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"26 10\",\"pages\":\"2282-2292\"},\"PeriodicalIF\":16.9000,\"publicationDate\":\"2024-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3452\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3452\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3452","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Burst steroid therapy for acute heart failure: The CORTAHF randomized, open-label, pilot trial
Aims
Burst steroid therapy, effective in acute respiratory diseases, may benefit patients with acute heart failure (AHF) in whom inflammatory activation is associated with adverse outcomes.
Methods and results
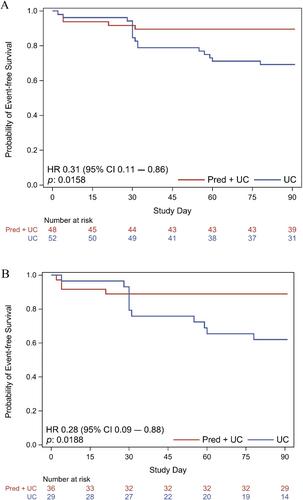
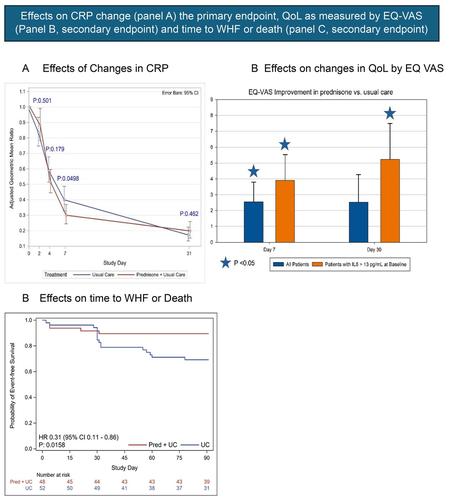
CORTAHF assessed whether burst steroid therapy reduces inflammation and results in better quality of life and clinical outcomes in AHF. Patients with AHF, N-terminal pro-B-type natriuretic peptide >1500 pg/ml, and high-sensitivity C-reactive protein (hsCRP) >20 mg/L were randomized 1:1 to oral, once daily 40 mg prednisone for 7 days or usual care, without blinding. Patients were followed for 90 days. A total of 101 patients were randomized. At day 7 the primary endpoint, hsCRP decreased in both arms – adjusted geometric mean ratios (GMRs) were 0.30 and 0.40 in the prednisone and usual care arms (ratio of GMRs 0.75, 95% confidence interval [CI] 0.56–1.00, p = 0.0498). The 90-day risk of worsening heart failure (HF), HF readmission or death as reported by the unblinded investigators was significantly lower in the prednisone group (10.4%) than in usual care (30.8%) (hazard ratio 0.31, 95% CI 0.11–0.86, p = 0.016). The EQ-5D visual analogue scale score as reported by the unblinded patients increased more in the prednisone group on day 7 (least squares mean difference 2.57, 95% CI 0.12–5.01 points, p = 0.040). All effects were statistically significant in the pre-specified subgroup with centrally-measured interleukin-6 >13 pg/ml. Adverse events, particularly hyperglycaemia, occurred more in the prednisone group with no difference in infection rate.
Conclusion
In this small open-label study of patients with AHF, burst steroid therapy was associated with reduced inflammation as measured by hsCRP levels at day 7 (primary endpoint). Secondary endpoints showed improved quality of life at day 7 and reduced 90-day risk of death or worsening HF. Large prospective studies are needed to evaluate these findings.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


