Lucas Guimarães Campos Roriz de Amorim, Marcelo Esteves Chaves Campos, Lígia Sant'Ana Dumont, José Augusto Rojas Peñafiel, Eliabe Silva de Abreu, Giovanni Scala Marchini, Manoj Monga, Eduardo Mazzucchi
{"title":"使用或不使用输尿管入路鞘的逆行肾内手术:随机对照试验的系统性回顾和荟萃分析。","authors":"Lucas Guimarães Campos Roriz de Amorim, Marcelo Esteves Chaves Campos, Lígia Sant'Ana Dumont, José Augusto Rojas Peñafiel, Eliabe Silva de Abreu, Giovanni Scala Marchini, Manoj Monga, Eduardo Mazzucchi","doi":"10.1590/S1677-5538.IBJU.2024.0452","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The ureteral access sheath (UAS) is a medical device that enables repeated entrance into the ureter and collecting system during retrograde intrarenal surgery (RIRS). Its impact on stone-free rates, ureteral injuries, operative time, and postoperative complications remains controversial. Therefore, we performed a systematic review and meta-analysis comparing RIRS with versus without UAS for urolithiasis management.</p><p><strong>Purpose: </strong>To compare outcomes from retrograde intrarenal surgery (RIRS) for stone extraction with or without ureteral access sheath (UAS); evaluating stone-free rate (SFR), ureteral injuries, operative time, and postoperative complications.</p><p><strong>Materials and methods: </strong>We systematically searched PubMed, Embase, and Cochrane Library in June 2024 for randomized controlled trials (RCTs) evaluating the efficacy and safety outcomes of UAS use in RIRS for urolithiasis treatment. Articles published between 2014 and 2024 were included. Pooled risk ratios (RRs) and mean differences (MDs) were calculated for binary and continuous outcomes, respectively.</p><p><strong>Results: </strong>Five RCTs comprising 466 procedures were included. Of these, 246 (52.7%) utilized UAS. The follow-up ranged from 1 week to 1 month. UAS reduced the incidence of postoperative fever (RR 0.49; 95% confidence interval [CI] 0.29-0.84; p=0.009), and postoperative infection (RR 0.50; 95% CI 0.30-0.83; p=0.008). There were no significant differences between groups in terms of SFR (RR 1.05; 95% CI 0.99-1.11; p=0.10), ureteral injuries (RR 1.29; 95% CI 0.95-1.75; p=0.11), operative time (MD 3.56 minutes; 95% CI -4.15 to 11.27 minutes; p=0.36), or length of stay (MD 0.32 days; 95% CI -0.42 to 1.07 days; p=0.40).</p><p><strong>Conclusion: </strong>UAS leads to a lower rate of post-operative fever and infection. However, UAS did not significantly reduce or increase the SFR or the rate of ureteral injuries during RIRS for patients with urolithiasis. The use of UAS should be considered to decrease the risk of infectious complications, particularly in those who may be at higher risk for such complications.</p>","PeriodicalId":49283,"journal":{"name":"International Braz J Urol","volume":"50 ","pages":"670-682"},"PeriodicalIF":4.5000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11554284/pdf/","citationCount":"0","resultStr":"{\"title\":\"Retrograde intrarenal surgery with or without ureteral access sheath: a systematic review and meta-analysis of randomized controlled trials.\",\"authors\":\"Lucas Guimarães Campos Roriz de Amorim, Marcelo Esteves Chaves Campos, Lígia Sant'Ana Dumont, José Augusto Rojas Peñafiel, Eliabe Silva de Abreu, Giovanni Scala Marchini, Manoj Monga, Eduardo Mazzucchi\",\"doi\":\"10.1590/S1677-5538.IBJU.2024.0452\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The ureteral access sheath (UAS) is a medical device that enables repeated entrance into the ureter and collecting system during retrograde intrarenal surgery (RIRS). Its impact on stone-free rates, ureteral injuries, operative time, and postoperative complications remains controversial. Therefore, we performed a systematic review and meta-analysis comparing RIRS with versus without UAS for urolithiasis management.</p><p><strong>Purpose: </strong>To compare outcomes from retrograde intrarenal surgery (RIRS) for stone extraction with or without ureteral access sheath (UAS); evaluating stone-free rate (SFR), ureteral injuries, operative time, and postoperative complications.</p><p><strong>Materials and methods: </strong>We systematically searched PubMed, Embase, and Cochrane Library in June 2024 for randomized controlled trials (RCTs) evaluating the efficacy and safety outcomes of UAS use in RIRS for urolithiasis treatment. Articles published between 2014 and 2024 were included. Pooled risk ratios (RRs) and mean differences (MDs) were calculated for binary and continuous outcomes, respectively.</p><p><strong>Results: </strong>Five RCTs comprising 466 procedures were included. Of these, 246 (52.7%) utilized UAS. The follow-up ranged from 1 week to 1 month. UAS reduced the incidence of postoperative fever (RR 0.49; 95% confidence interval [CI] 0.29-0.84; p=0.009), and postoperative infection (RR 0.50; 95% CI 0.30-0.83; p=0.008). There were no significant differences between groups in terms of SFR (RR 1.05; 95% CI 0.99-1.11; p=0.10), ureteral injuries (RR 1.29; 95% CI 0.95-1.75; p=0.11), operative time (MD 3.56 minutes; 95% CI -4.15 to 11.27 minutes; p=0.36), or length of stay (MD 0.32 days; 95% CI -0.42 to 1.07 days; p=0.40).</p><p><strong>Conclusion: </strong>UAS leads to a lower rate of post-operative fever and infection. However, UAS did not significantly reduce or increase the SFR or the rate of ureteral injuries during RIRS for patients with urolithiasis. The use of UAS should be considered to decrease the risk of infectious complications, particularly in those who may be at higher risk for such complications.</p>\",\"PeriodicalId\":49283,\"journal\":{\"name\":\"International Braz J Urol\",\"volume\":\"50 \",\"pages\":\"670-682\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11554284/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Braz J Urol\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1590/S1677-5538.IBJU.2024.0452\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Braz J Urol","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1590/S1677-5538.IBJU.2024.0452","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Retrograde intrarenal surgery with or without ureteral access sheath: a systematic review and meta-analysis of randomized controlled trials.
Introduction: The ureteral access sheath (UAS) is a medical device that enables repeated entrance into the ureter and collecting system during retrograde intrarenal surgery (RIRS). Its impact on stone-free rates, ureteral injuries, operative time, and postoperative complications remains controversial. Therefore, we performed a systematic review and meta-analysis comparing RIRS with versus without UAS for urolithiasis management.
Purpose: To compare outcomes from retrograde intrarenal surgery (RIRS) for stone extraction with or without ureteral access sheath (UAS); evaluating stone-free rate (SFR), ureteral injuries, operative time, and postoperative complications.
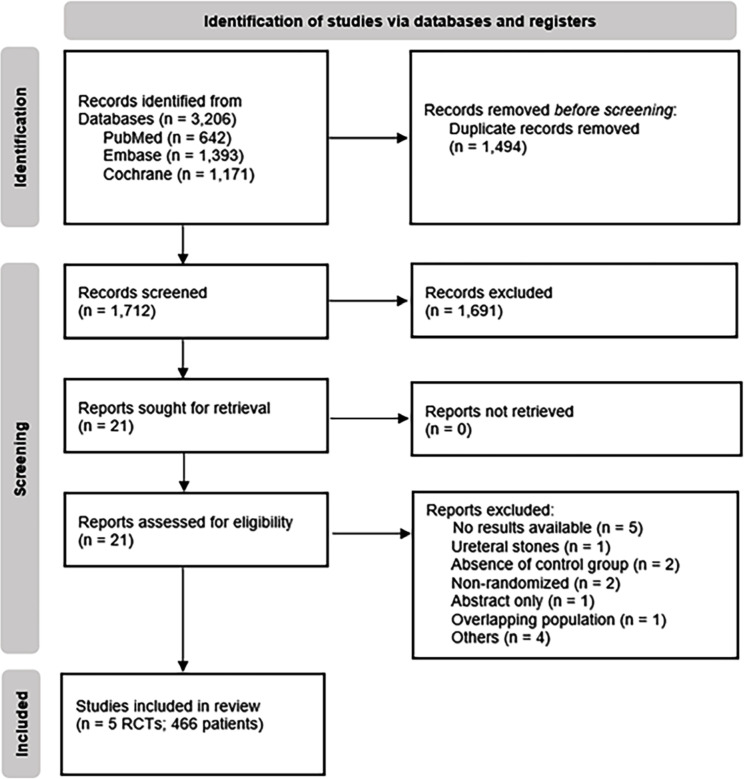
Materials and methods: We systematically searched PubMed, Embase, and Cochrane Library in June 2024 for randomized controlled trials (RCTs) evaluating the efficacy and safety outcomes of UAS use in RIRS for urolithiasis treatment. Articles published between 2014 and 2024 were included. Pooled risk ratios (RRs) and mean differences (MDs) were calculated for binary and continuous outcomes, respectively.
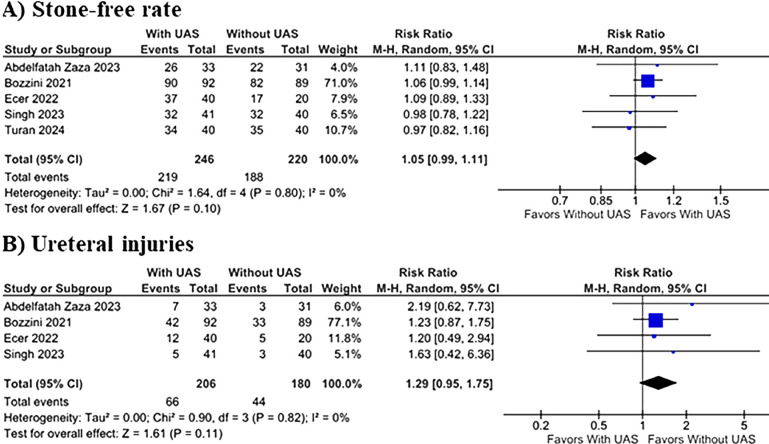
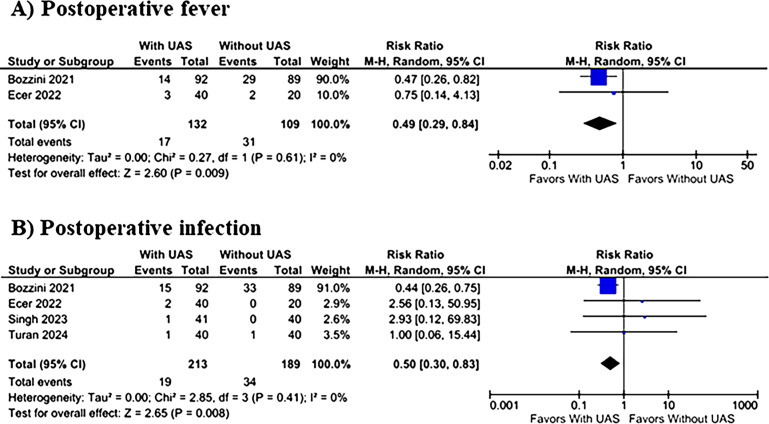
Results: Five RCTs comprising 466 procedures were included. Of these, 246 (52.7%) utilized UAS. The follow-up ranged from 1 week to 1 month. UAS reduced the incidence of postoperative fever (RR 0.49; 95% confidence interval [CI] 0.29-0.84; p=0.009), and postoperative infection (RR 0.50; 95% CI 0.30-0.83; p=0.008). There were no significant differences between groups in terms of SFR (RR 1.05; 95% CI 0.99-1.11; p=0.10), ureteral injuries (RR 1.29; 95% CI 0.95-1.75; p=0.11), operative time (MD 3.56 minutes; 95% CI -4.15 to 11.27 minutes; p=0.36), or length of stay (MD 0.32 days; 95% CI -0.42 to 1.07 days; p=0.40).
Conclusion: UAS leads to a lower rate of post-operative fever and infection. However, UAS did not significantly reduce or increase the SFR or the rate of ureteral injuries during RIRS for patients with urolithiasis. The use of UAS should be considered to decrease the risk of infectious complications, particularly in those who may be at higher risk for such complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


