Joshua Wong, Cheng Hwee Soh, Benjamen Wang, Thomas Marwick
{"title":"成年癌症幸存者心力衰竭的长期风险:系统回顾和荟萃分析。","authors":"Joshua Wong, Cheng Hwee Soh, Benjamen Wang, Thomas Marwick","doi":"10.1136/heartjnl-2024-324301","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cancer survivors are at increased risk of heart failure (HF). While cardiotoxicity is commonly sought at the time of cancer chemotherapy, HF develops as a result of multiple 'hits' over time, and there is limited evidence regarding the frequency and causes of HF during survivorship.</p><p><strong>Objectives: </strong>This systematic review sought to investigate the relationship between cardiotoxic cancer therapies and HF during survivorship.</p><p><strong>Methods: </strong>We searched the EMBASE, MEDLINE and CINAHL databases for studies reporting HF in adult survivors (≥50 years old), who were ≥5 years postpotential cardiotoxic cancer therapy. A random effects model was used to examine the associations of HF.</p><p><strong>Results: </strong>Thirteen papers were included, comprising 190 259 participants (mean age 53.5 years, 93% women). The risk of HF was increased (overall RR 1.47 (95% CI (1.17 to 1.86)). Cardiotoxic treatment, compared with cancer alone, provided a similar risk (RR of 1.46 (95% CI 0.98 to 2.16)). The overall HF incidence rate was 2.1% compared with 1.7% in the control arm-an absolute risk difference of 0.4%. In the breast cancer population ratio (11 studies), the overall HF RR was 2.57 (95% CI 1.35 to 4.90)). Although heterogeneity was significant (I<sup>2</sup>=77.2), this was explained by differences in patient characteristics; once multivariable analysis accounted for follow-up duration (OR 0.99, 95% CI (0.97 to 0.99), p=0.047), age (OR 1.14, 95% CI (1.04 to 1.25), p=0.003) and hypertension (OR 0.95, 95% CI (0.92 to 0.98), p<0.001), residual heterogeneity was low (I<sup>2</sup>=28.7).</p><p><strong>Conclusions: </strong>HF is increased in adult cancer survivors, associated with cardiotoxic cancer therapy and standard risk factors. However, the small absolute risk difference between survivors and controls suggests that universal screening of survivors is unjustifiable. A risk model based on age, cardiotoxic cancer therapy and standard risk factors may facilitate a selective screening process in this at-risk population.</p>","PeriodicalId":12835,"journal":{"name":"Heart","volume":" ","pages":"1188-1195"},"PeriodicalIF":4.4000,"publicationDate":"2024-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11420760/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term risk of heart failure in adult cancer survivors: a systematic review and meta-analysis.\",\"authors\":\"Joshua Wong, Cheng Hwee Soh, Benjamen Wang, Thomas Marwick\",\"doi\":\"10.1136/heartjnl-2024-324301\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cancer survivors are at increased risk of heart failure (HF). While cardiotoxicity is commonly sought at the time of cancer chemotherapy, HF develops as a result of multiple 'hits' over time, and there is limited evidence regarding the frequency and causes of HF during survivorship.</p><p><strong>Objectives: </strong>This systematic review sought to investigate the relationship between cardiotoxic cancer therapies and HF during survivorship.</p><p><strong>Methods: </strong>We searched the EMBASE, MEDLINE and CINAHL databases for studies reporting HF in adult survivors (≥50 years old), who were ≥5 years postpotential cardiotoxic cancer therapy. A random effects model was used to examine the associations of HF.</p><p><strong>Results: </strong>Thirteen papers were included, comprising 190 259 participants (mean age 53.5 years, 93% women). The risk of HF was increased (overall RR 1.47 (95% CI (1.17 to 1.86)). Cardiotoxic treatment, compared with cancer alone, provided a similar risk (RR of 1.46 (95% CI 0.98 to 2.16)). The overall HF incidence rate was 2.1% compared with 1.7% in the control arm-an absolute risk difference of 0.4%. In the breast cancer population ratio (11 studies), the overall HF RR was 2.57 (95% CI 1.35 to 4.90)). Although heterogeneity was significant (I<sup>2</sup>=77.2), this was explained by differences in patient characteristics; once multivariable analysis accounted for follow-up duration (OR 0.99, 95% CI (0.97 to 0.99), p=0.047), age (OR 1.14, 95% CI (1.04 to 1.25), p=0.003) and hypertension (OR 0.95, 95% CI (0.92 to 0.98), p<0.001), residual heterogeneity was low (I<sup>2</sup>=28.7).</p><p><strong>Conclusions: </strong>HF is increased in adult cancer survivors, associated with cardiotoxic cancer therapy and standard risk factors. However, the small absolute risk difference between survivors and controls suggests that universal screening of survivors is unjustifiable. A risk model based on age, cardiotoxic cancer therapy and standard risk factors may facilitate a selective screening process in this at-risk population.</p>\",\"PeriodicalId\":12835,\"journal\":{\"name\":\"Heart\",\"volume\":\" \",\"pages\":\"1188-1195\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2024-09-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11420760/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Heart\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/heartjnl-2024-324301\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/heartjnl-2024-324301","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:癌症幸存者患心力衰竭(HF)的风险增加。虽然心脏毒性通常是在癌症化疗时发现的,但随着时间的推移,心力衰竭是多重 "打击 "的结果,而关于幸存者期间心力衰竭的频率和原因的证据却很有限:本系统性综述旨在研究心脏毒性癌症疗法与生存期心房颤动之间的关系:我们在 EMBASE、MEDLINE 和 CINAHL 数据库中检索了报告成年幸存者(年龄≥50 岁)心房颤动的研究,这些患者在接受潜在的心脏毒性癌症治疗后≥5 年。研究采用随机效应模型来检验心房颤动的相关性:共纳入13篇论文,190 259名参与者(平均年龄53.5岁,93%为女性)。罹患心房颤动的风险增加(总RR为1.47(95% CI为1.17至1.86))。与单纯癌症相比,心脏毒性治疗的风险相似(RR 为 1.46(95% CI 为 0.98 至 2.16))。总体高血压发病率为 2.1%,而对照组为 1.7%,绝对风险差异为 0.4%。在乳腺癌人群比率(11 项研究)中,总体高频 RR 为 2.57(95% CI 1.35 至 4.90))。虽然异质性很明显(I2=77.2),但这是由患者特征的差异造成的;一旦多变量分析考虑了随访时间(OR 0.99,95% CI (0.97至0.99),p=0.047)、年龄(OR 1.14,95% CI (1.04至1.25),p=0.003)和高血压(OR 0.95,95% CI (0.92至0.98),p2=28.7),就可以解释这一点:结论:成年癌症幸存者患心房颤动的比例增加,这与心脏毒性癌症治疗和标准风险因素有关。然而,幸存者与对照组之间的绝对风险差异很小,这表明对幸存者进行普遍筛查是不合理的。基于年龄、心脏毒性癌症治疗和标准风险因素的风险模型可能有助于对这一高危人群进行选择性筛查。
Long-term risk of heart failure in adult cancer survivors: a systematic review and meta-analysis.
Background: Cancer survivors are at increased risk of heart failure (HF). While cardiotoxicity is commonly sought at the time of cancer chemotherapy, HF develops as a result of multiple 'hits' over time, and there is limited evidence regarding the frequency and causes of HF during survivorship.
Objectives: This systematic review sought to investigate the relationship between cardiotoxic cancer therapies and HF during survivorship.
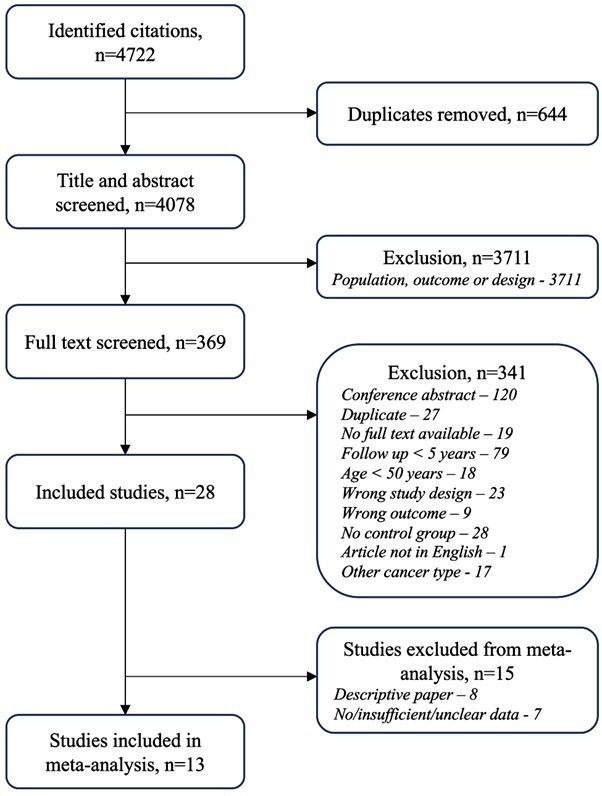
Methods: We searched the EMBASE, MEDLINE and CINAHL databases for studies reporting HF in adult survivors (≥50 years old), who were ≥5 years postpotential cardiotoxic cancer therapy. A random effects model was used to examine the associations of HF.
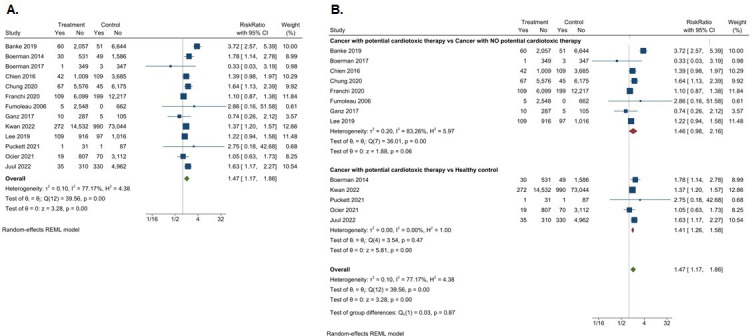
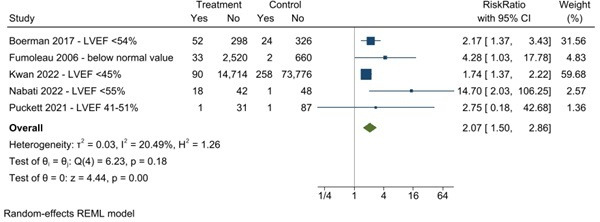
Results: Thirteen papers were included, comprising 190 259 participants (mean age 53.5 years, 93% women). The risk of HF was increased (overall RR 1.47 (95% CI (1.17 to 1.86)). Cardiotoxic treatment, compared with cancer alone, provided a similar risk (RR of 1.46 (95% CI 0.98 to 2.16)). The overall HF incidence rate was 2.1% compared with 1.7% in the control arm-an absolute risk difference of 0.4%. In the breast cancer population ratio (11 studies), the overall HF RR was 2.57 (95% CI 1.35 to 4.90)). Although heterogeneity was significant (I2=77.2), this was explained by differences in patient characteristics; once multivariable analysis accounted for follow-up duration (OR 0.99, 95% CI (0.97 to 0.99), p=0.047), age (OR 1.14, 95% CI (1.04 to 1.25), p=0.003) and hypertension (OR 0.95, 95% CI (0.92 to 0.98), p<0.001), residual heterogeneity was low (I2=28.7).
Conclusions: HF is increased in adult cancer survivors, associated with cardiotoxic cancer therapy and standard risk factors. However, the small absolute risk difference between survivors and controls suggests that universal screening of survivors is unjustifiable. A risk model based on age, cardiotoxic cancer therapy and standard risk factors may facilitate a selective screening process in this at-risk population.
期刊介绍:
Heart is an international peer reviewed journal that keeps cardiologists up to date with important research advances in cardiovascular disease. New scientific developments are highlighted in editorials and put in context with concise review articles. There is one free Editor’s Choice article in each issue, with open access options available to authors for all articles. Education in Heart articles provide a comprehensive, continuously updated, cardiology curriculum.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


