Xing Xing , Xiaoqiang Liu , Yi Zhang , Lei Zhang , Gu Shen , Yulong Ge , Fang Wang
{"title":"心脏磁共振成像对结构性和非结构性心脏病致命性心律失常的预测价值","authors":"Xing Xing , Xiaoqiang Liu , Yi Zhang , Lei Zhang , Gu Shen , Yulong Ge , Fang Wang","doi":"10.1016/j.ijcha.2024.101462","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>The risk stratification for fatal arrhythmias remains inadequate. Cardiac magnetic resonance (CMR) imaging provides a detailed evaluation of arrhythmogenic substrates. This study investigated the predictive capacity of multiparametric CMR for fatal ventricular arrhythmias (VAs) in a heterogeneous disease cohort.</p></div><div><h3>Methods</h3><p>The study included 396 consecutive patients with structural heart disease (SHD, n = 248) and non-apparent SHD (n = 148) who underwent CMR scans between 2018 and 2022. The primary endpoint was fatal composite arrhythmias.</p></div><div><h3>Results</h3><p>Thirty-three patients (8.3 %) experienced fatal arrhythmias (25 with SHD, 8 with non-apparent SHD) over a median follow-up of 24 months. The independent risk factors for patients with SHD included syncope (hazard ratio [HR] = 5.347; <em>P</em> < 0.001), VA history (HR = 3.705; P = 0.004), right ventricular ejection fraction (RVEF) ≤ 45 % (HR = 2.587; <em>P</em> = 0.039), and the presence of late gadolinium enhancement (LGE) (HR = 4.767; <em>P</em> = 0.040). In the non-apparent SHD group, fatal arrhythmias were independently correlated with VA history (HR = 10.23; <em>P</em> = 0.005), RVEF ≤ 45 % (HR = 8.307; <em>P</em> = 0.015), and CMR myocardial abnormalities (HR = 5.203; <em>P</em> = 0.033). Patients at high risk of fatal arrhythmia in the SHD and non-apparent SHD groups exhibited 3-year event-free survival rates of 69.4 % and 83.5 %, respectively.</p></div><div><h3>Conclusion</h3><p>CMR provides effective prognostic information for patients with and without apparent SHD. The presence of LGE, CMR myocardial abnormalities, and right ventricular dysfunction are strong risk markers for fatal arrhythmias.</p></div>","PeriodicalId":38026,"journal":{"name":"IJC Heart and Vasculature","volume":"54 ","pages":"Article 101462"},"PeriodicalIF":2.5000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2352906724001283/pdfft?md5=6e15e2faef1d0e6d27fa64818539913f&pid=1-s2.0-S2352906724001283-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Predictive value of cardiac magnetic resonance imaging for fatal arrhythmias in structural and nonstructural heart diseases\",\"authors\":\"Xing Xing , Xiaoqiang Liu , Yi Zhang , Lei Zhang , Gu Shen , Yulong Ge , Fang Wang\",\"doi\":\"10.1016/j.ijcha.2024.101462\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>The risk stratification for fatal arrhythmias remains inadequate. Cardiac magnetic resonance (CMR) imaging provides a detailed evaluation of arrhythmogenic substrates. This study investigated the predictive capacity of multiparametric CMR for fatal ventricular arrhythmias (VAs) in a heterogeneous disease cohort.</p></div><div><h3>Methods</h3><p>The study included 396 consecutive patients with structural heart disease (SHD, n = 248) and non-apparent SHD (n = 148) who underwent CMR scans between 2018 and 2022. The primary endpoint was fatal composite arrhythmias.</p></div><div><h3>Results</h3><p>Thirty-three patients (8.3 %) experienced fatal arrhythmias (25 with SHD, 8 with non-apparent SHD) over a median follow-up of 24 months. The independent risk factors for patients with SHD included syncope (hazard ratio [HR] = 5.347; <em>P</em> < 0.001), VA history (HR = 3.705; P = 0.004), right ventricular ejection fraction (RVEF) ≤ 45 % (HR = 2.587; <em>P</em> = 0.039), and the presence of late gadolinium enhancement (LGE) (HR = 4.767; <em>P</em> = 0.040). In the non-apparent SHD group, fatal arrhythmias were independently correlated with VA history (HR = 10.23; <em>P</em> = 0.005), RVEF ≤ 45 % (HR = 8.307; <em>P</em> = 0.015), and CMR myocardial abnormalities (HR = 5.203; <em>P</em> = 0.033). Patients at high risk of fatal arrhythmia in the SHD and non-apparent SHD groups exhibited 3-year event-free survival rates of 69.4 % and 83.5 %, respectively.</p></div><div><h3>Conclusion</h3><p>CMR provides effective prognostic information for patients with and without apparent SHD. The presence of LGE, CMR myocardial abnormalities, and right ventricular dysfunction are strong risk markers for fatal arrhythmias.</p></div>\",\"PeriodicalId\":38026,\"journal\":{\"name\":\"IJC Heart and Vasculature\",\"volume\":\"54 \",\"pages\":\"Article 101462\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2352906724001283/pdfft?md5=6e15e2faef1d0e6d27fa64818539913f&pid=1-s2.0-S2352906724001283-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"IJC Heart and Vasculature\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2352906724001283\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJC Heart and Vasculature","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2352906724001283","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Predictive value of cardiac magnetic resonance imaging for fatal arrhythmias in structural and nonstructural heart diseases
Background
The risk stratification for fatal arrhythmias remains inadequate. Cardiac magnetic resonance (CMR) imaging provides a detailed evaluation of arrhythmogenic substrates. This study investigated the predictive capacity of multiparametric CMR for fatal ventricular arrhythmias (VAs) in a heterogeneous disease cohort.
Methods
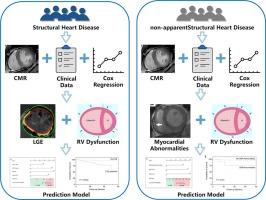
The study included 396 consecutive patients with structural heart disease (SHD, n = 248) and non-apparent SHD (n = 148) who underwent CMR scans between 2018 and 2022. The primary endpoint was fatal composite arrhythmias.
Results
Thirty-three patients (8.3 %) experienced fatal arrhythmias (25 with SHD, 8 with non-apparent SHD) over a median follow-up of 24 months. The independent risk factors for patients with SHD included syncope (hazard ratio [HR] = 5.347; P < 0.001), VA history (HR = 3.705; P = 0.004), right ventricular ejection fraction (RVEF) ≤ 45 % (HR = 2.587; P = 0.039), and the presence of late gadolinium enhancement (LGE) (HR = 4.767; P = 0.040). In the non-apparent SHD group, fatal arrhythmias were independently correlated with VA history (HR = 10.23; P = 0.005), RVEF ≤ 45 % (HR = 8.307; P = 0.015), and CMR myocardial abnormalities (HR = 5.203; P = 0.033). Patients at high risk of fatal arrhythmia in the SHD and non-apparent SHD groups exhibited 3-year event-free survival rates of 69.4 % and 83.5 %, respectively.
Conclusion
CMR provides effective prognostic information for patients with and without apparent SHD. The presence of LGE, CMR myocardial abnormalities, and right ventricular dysfunction are strong risk markers for fatal arrhythmias.
期刊介绍:
IJC Heart & Vasculature is an online-only, open-access journal dedicated to publishing original articles and reviews (also Editorials and Letters to the Editor) which report on structural and functional cardiovascular pathology, with an emphasis on imaging and disease pathophysiology. Articles must be authentic, educational, clinically relevant, and original in their content and scientific approach. IJC Heart & Vasculature requires the highest standards of scientific integrity in order to promote reliable, reproducible and verifiable research findings. All authors are advised to consult the Principles of Ethical Publishing in the International Journal of Cardiology before submitting a manuscript. Submission of a manuscript to this journal gives the publisher the right to publish that paper if it is accepted. Manuscripts may be edited to improve clarity and expression.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


