Jin Lin Tan, Thomas Lokan, Mohamed Asif Chinnaratha, Martin Veysey
{"title":"慢性肝病和凝血功能障碍患者腹腔穿刺术后出血的风险:系统回顾和荟萃分析。","authors":"Jin Lin Tan, Thomas Lokan, Mohamed Asif Chinnaratha, Martin Veysey","doi":"10.1002/jgh3.70013","DOIUrl":null,"url":null,"abstract":"<p>Abdominal paracentesis is a common procedure performed for both diagnostic and therapeutic purposes in patients with chronic liver disease and ascites. This review aims to provide an overview of the current evidence on the risk of bleeding associated with abdominal paracentesis. Electronic search was performed using PubMed, MEDLINE, and Ovid EMBASE from inception to 29 October 2023. Studies were included if they examined the risk of bleeding post-abdominal paracentesis or the efficacy of interventions to reduce bleeding in patients with chronic liver disease. Random-effects model was used to calculate the pooled proportions of bleeding events following abdominal paracentesis. Heterogeneity was determined by <i>I</i><sup>2</sup>, τ<sup>2</sup> statistics, and <i>P</i>-value. Eight studies were included for review. Six studies reported incident events of post-abdominal paracentesis bleeding. Pooled proportion of bleeding events following abdominal paracentesis was 0.32% (95% CI: 0.15–0.69%). The mean values for pre-procedural INR and platelet count of patients in these studies ranged between 1.4 and 2.0, and 50 and 153 × 10<sup>9</sup>/L, respectively. The highest recorded INR was 8.7, and the lowest platelet count was 19 × 10<sup>9</sup>/L. Major bleeding after abdominal paracentesis occurred in 0–0.97% of the study cohorts. Two studies demonstrated that the use of thromboelastography (TEG) before paracentesis in patients with chronic liver disease identified those at risk of procedure-related bleeding and reduced transfusion requirements. The overall risk of major bleeding after abdominal paracentesis is low in patients with chronic liver disease and coagulopathy. TEG may be used to predict bleeding risk and guide transfusion requirements.</p>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"8 8","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11331248/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk of bleeding after abdominal paracentesis in patients with chronic liver disease and coagulopathy: A systematic review and meta-analysis\",\"authors\":\"Jin Lin Tan, Thomas Lokan, Mohamed Asif Chinnaratha, Martin Veysey\",\"doi\":\"10.1002/jgh3.70013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Abdominal paracentesis is a common procedure performed for both diagnostic and therapeutic purposes in patients with chronic liver disease and ascites. This review aims to provide an overview of the current evidence on the risk of bleeding associated with abdominal paracentesis. Electronic search was performed using PubMed, MEDLINE, and Ovid EMBASE from inception to 29 October 2023. Studies were included if they examined the risk of bleeding post-abdominal paracentesis or the efficacy of interventions to reduce bleeding in patients with chronic liver disease. Random-effects model was used to calculate the pooled proportions of bleeding events following abdominal paracentesis. Heterogeneity was determined by <i>I</i><sup>2</sup>, τ<sup>2</sup> statistics, and <i>P</i>-value. Eight studies were included for review. Six studies reported incident events of post-abdominal paracentesis bleeding. Pooled proportion of bleeding events following abdominal paracentesis was 0.32% (95% CI: 0.15–0.69%). The mean values for pre-procedural INR and platelet count of patients in these studies ranged between 1.4 and 2.0, and 50 and 153 × 10<sup>9</sup>/L, respectively. The highest recorded INR was 8.7, and the lowest platelet count was 19 × 10<sup>9</sup>/L. Major bleeding after abdominal paracentesis occurred in 0–0.97% of the study cohorts. Two studies demonstrated that the use of thromboelastography (TEG) before paracentesis in patients with chronic liver disease identified those at risk of procedure-related bleeding and reduced transfusion requirements. The overall risk of major bleeding after abdominal paracentesis is low in patients with chronic liver disease and coagulopathy. TEG may be used to predict bleeding risk and guide transfusion requirements.</p>\",\"PeriodicalId\":45861,\"journal\":{\"name\":\"JGH Open\",\"volume\":\"8 8\",\"pages\":\"\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11331248/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JGH Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.70013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.70013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Risk of bleeding after abdominal paracentesis in patients with chronic liver disease and coagulopathy: A systematic review and meta-analysis
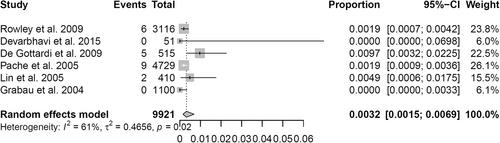
Abdominal paracentesis is a common procedure performed for both diagnostic and therapeutic purposes in patients with chronic liver disease and ascites. This review aims to provide an overview of the current evidence on the risk of bleeding associated with abdominal paracentesis. Electronic search was performed using PubMed, MEDLINE, and Ovid EMBASE from inception to 29 October 2023. Studies were included if they examined the risk of bleeding post-abdominal paracentesis or the efficacy of interventions to reduce bleeding in patients with chronic liver disease. Random-effects model was used to calculate the pooled proportions of bleeding events following abdominal paracentesis. Heterogeneity was determined by I2, τ2 statistics, and P-value. Eight studies were included for review. Six studies reported incident events of post-abdominal paracentesis bleeding. Pooled proportion of bleeding events following abdominal paracentesis was 0.32% (95% CI: 0.15–0.69%). The mean values for pre-procedural INR and platelet count of patients in these studies ranged between 1.4 and 2.0, and 50 and 153 × 109/L, respectively. The highest recorded INR was 8.7, and the lowest platelet count was 19 × 109/L. Major bleeding after abdominal paracentesis occurred in 0–0.97% of the study cohorts. Two studies demonstrated that the use of thromboelastography (TEG) before paracentesis in patients with chronic liver disease identified those at risk of procedure-related bleeding and reduced transfusion requirements. The overall risk of major bleeding after abdominal paracentesis is low in patients with chronic liver disease and coagulopathy. TEG may be used to predict bleeding risk and guide transfusion requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


