{"title":"新辅助治疗会增加食管癌吻合口漏的风险吗?一项网络荟萃分析。","authors":"Da Zhou, Donglai Chen, Peidong Song, Zihao Hu, Sukai Xu, Rongying Zhu, Yongbing Chen","doi":"10.1111/jebm.12634","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>Conflicting results have been reported about the impact of neoadjuvant therapy on anastomotic leakage (AL) after esophagectomy. We aimed to unravel the potential effect of neoadjuvant therapy on AL after esophagectomy through a network meta-analysis.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A Bayesian network meta-analysis was performed by retrieving relevant literature from PubMed, EMbase, The Cochrane Library and Web of Science Core Collection. Randomized clinical trials (RCTs) and retrospective studies (RS) comparing the following treatment modalities were included: neoadjuvant chemoradiation (nCRT), neoadjuvant chemotherapy (nCT), neoadjuvant radiotherapy (nR), neoadjuvant immunochemotherapy (nICT), and surgery alone (SA). Subgroup analyses by radiation dose, examined lymph nodes (ELN), route of reconstruction, site of anastomosis, and surgical approach were also conducted.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 62 studies with 12,746 patients were included for the present study, among which 17 were RCTs. There were no significantly statistical differences observed among the five treatment modalities in AL for both RCTs (nCRT-nICT: risk ratio 1.51, 95% confidence interval 0.52–4.4; nCT-nICT: 1.71, 0.56–5.08; nICT-nR: 0.79, 0.12–8.02; nICT-SA: 0.59, 0.2–1.84) and RS (nCRT-nICT: odds ratio 1.53, 95% confidence interval 0.84–2.84; nCT-nICT: 1.56, 0.87–2.88; nICT-SA: 0.6, 0.31–1.12; nICT-nR: 1.08, 0.09–36.02). Subgroup analysis revealed that no significant difference in AL was observed among the five treatment modalities except for the impact of nCRT versus nCT (0.21, 0.05–0.73) on AL with a radiation dose ≥41.4 Gy.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Neoadjuvant therapy do not significantly increase the incidence of AL after esophagectomy. Administration of irradiation with a moderate dose is not associated with elevated risk in AL. Clinicians can be less apprehensive about prescribing nCRT.</p>\n </section>\n </div>","PeriodicalId":16090,"journal":{"name":"Journal of Evidence‐Based Medicine","volume":"17 3","pages":"559-574"},"PeriodicalIF":3.6000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jebm.12634","citationCount":"0","resultStr":"{\"title\":\"Does neoadjuvant therapy contribute to increased risk in anastomotic leakage of esophageal cancer? A network meta-analysis\",\"authors\":\"Da Zhou, Donglai Chen, Peidong Song, Zihao Hu, Sukai Xu, Rongying Zhu, Yongbing Chen\",\"doi\":\"10.1111/jebm.12634\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>Conflicting results have been reported about the impact of neoadjuvant therapy on anastomotic leakage (AL) after esophagectomy. We aimed to unravel the potential effect of neoadjuvant therapy on AL after esophagectomy through a network meta-analysis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A Bayesian network meta-analysis was performed by retrieving relevant literature from PubMed, EMbase, The Cochrane Library and Web of Science Core Collection. Randomized clinical trials (RCTs) and retrospective studies (RS) comparing the following treatment modalities were included: neoadjuvant chemoradiation (nCRT), neoadjuvant chemotherapy (nCT), neoadjuvant radiotherapy (nR), neoadjuvant immunochemotherapy (nICT), and surgery alone (SA). Subgroup analyses by radiation dose, examined lymph nodes (ELN), route of reconstruction, site of anastomosis, and surgical approach were also conducted.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 62 studies with 12,746 patients were included for the present study, among which 17 were RCTs. There were no significantly statistical differences observed among the five treatment modalities in AL for both RCTs (nCRT-nICT: risk ratio 1.51, 95% confidence interval 0.52–4.4; nCT-nICT: 1.71, 0.56–5.08; nICT-nR: 0.79, 0.12–8.02; nICT-SA: 0.59, 0.2–1.84) and RS (nCRT-nICT: odds ratio 1.53, 95% confidence interval 0.84–2.84; nCT-nICT: 1.56, 0.87–2.88; nICT-SA: 0.6, 0.31–1.12; nICT-nR: 1.08, 0.09–36.02). Subgroup analysis revealed that no significant difference in AL was observed among the five treatment modalities except for the impact of nCRT versus nCT (0.21, 0.05–0.73) on AL with a radiation dose ≥41.4 Gy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Neoadjuvant therapy do not significantly increase the incidence of AL after esophagectomy. Administration of irradiation with a moderate dose is not associated with elevated risk in AL. Clinicians can be less apprehensive about prescribing nCRT.</p>\\n </section>\\n </div>\",\"PeriodicalId\":16090,\"journal\":{\"name\":\"Journal of Evidence‐Based Medicine\",\"volume\":\"17 3\",\"pages\":\"559-574\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jebm.12634\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Evidence‐Based Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jebm.12634\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Evidence‐Based Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jebm.12634","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
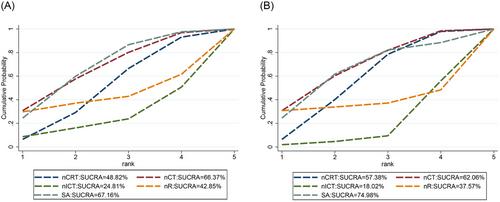
目的:关于新辅助治疗对食管切除术后吻合口漏(AL)的影响,目前的报道结果不一。我们旨在通过网络荟萃分析揭示新辅助治疗对食管切除术后吻合口漏的潜在影响:我们从 PubMed、EMbase、The Cochrane Library 和 Web of Science Core Collection 中检索了相关文献,进行了贝叶斯网络荟萃分析。研究纳入了比较以下治疗方式的随机临床试验(RCT)和回顾性研究(RS):新辅助化放疗(nCRT)、新辅助化疗(nCT)、新辅助放疗(nR)、新辅助免疫化疗(nICT)和单纯手术(SA)。此外,还按放射剂量、检查淋巴结(ELN)、重建途径、吻合部位和手术方法进行了分组分析:本研究共纳入 62 项研究,12746 名患者,其中 17 项为研究性临床试验。在两项 RCT 中,AL 的五种治疗方式之间没有观察到明显的统计学差异(nCRT-nICT:风险比 1.51,95% 置信区间 0.52-4.4;nCT-nICT:1.71,0.56-5.08;nICT-nR:0.79,0.12-8.02;nICT-SA:0.59,0.2-1.84)和 RS(nCRT-nICT:风险比 1.53,95% 置信区间 0.84-2.84;nCT-nICT:1.56,0.87-2.88;nICT-SA:0.6,0.31-1.12;nICT-nR:1.08,0.09-36.02)。亚组分析显示,除了nCRT与nCT(0.21,0.05-0.73)对放射剂量≥41.4 Gy的AL的影响外,其他五种治疗方式的AL没有明显差异:结论:新辅助治疗不会明显增加食管切除术后 AL 的发生率。结论:新辅助治疗不会明显增加食管切除术后 AL 的发生率,中等剂量的照射与 AL 风险升高无关。临床医生在开具新辅助治疗处方时可以不必过于担心。
Does neoadjuvant therapy contribute to increased risk in anastomotic leakage of esophageal cancer? A network meta-analysis
Aim
Conflicting results have been reported about the impact of neoadjuvant therapy on anastomotic leakage (AL) after esophagectomy. We aimed to unravel the potential effect of neoadjuvant therapy on AL after esophagectomy through a network meta-analysis.
Methods
A Bayesian network meta-analysis was performed by retrieving relevant literature from PubMed, EMbase, The Cochrane Library and Web of Science Core Collection. Randomized clinical trials (RCTs) and retrospective studies (RS) comparing the following treatment modalities were included: neoadjuvant chemoradiation (nCRT), neoadjuvant chemotherapy (nCT), neoadjuvant radiotherapy (nR), neoadjuvant immunochemotherapy (nICT), and surgery alone (SA). Subgroup analyses by radiation dose, examined lymph nodes (ELN), route of reconstruction, site of anastomosis, and surgical approach were also conducted.
Results
A total of 62 studies with 12,746 patients were included for the present study, among which 17 were RCTs. There were no significantly statistical differences observed among the five treatment modalities in AL for both RCTs (nCRT-nICT: risk ratio 1.51, 95% confidence interval 0.52–4.4; nCT-nICT: 1.71, 0.56–5.08; nICT-nR: 0.79, 0.12–8.02; nICT-SA: 0.59, 0.2–1.84) and RS (nCRT-nICT: odds ratio 1.53, 95% confidence interval 0.84–2.84; nCT-nICT: 1.56, 0.87–2.88; nICT-SA: 0.6, 0.31–1.12; nICT-nR: 1.08, 0.09–36.02). Subgroup analysis revealed that no significant difference in AL was observed among the five treatment modalities except for the impact of nCRT versus nCT (0.21, 0.05–0.73) on AL with a radiation dose ≥41.4 Gy.
Conclusions
Neoadjuvant therapy do not significantly increase the incidence of AL after esophagectomy. Administration of irradiation with a moderate dose is not associated with elevated risk in AL. Clinicians can be less apprehensive about prescribing nCRT.
期刊介绍:
The Journal of Evidence-Based Medicine (EMB) is an esteemed international healthcare and medical decision-making journal, dedicated to publishing groundbreaking research outcomes in evidence-based decision-making, research, practice, and education. Serving as the official English-language journal of the Cochrane China Centre and West China Hospital of Sichuan University, we eagerly welcome editorials, commentaries, and systematic reviews encompassing various topics such as clinical trials, policy, drug and patient safety, education, and knowledge translation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


