Wei Guo, Jing Tian, Yajing Wang, Yajing Zhang, Jingjing Yan, Yutao Du, Yanbo Zhang, Qinghua Han
{"title":"预测射血分数轻度降低型心力衰竭患者死亡风险的网络动态提名图。","authors":"Wei Guo, Jing Tian, Yajing Wang, Yajing Zhang, Jingjing Yan, Yutao Du, Yanbo Zhang, Qinghua Han","doi":"10.2147/RMHP.S474862","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to develop an integrative dynamic nomogram, including N-terminal pro-B type natural peptide (NT-proBNP) and estimated glomerular filtration rate (eGFR), for predicting the risk of all-cause mortality in HFmrEF patients.</p><p><strong>Patients and methods: </strong>790 HFmrEF patients were prospectively enrolled in the development cohort for the model. The least absolute shrinkage and selection operator (LASSO) regression and Random Survival Forest (RSF) were employed to select predictors for all-cause mortality. Develop a nomogram based on the Cox proportional hazard model for predicting long-term mortality (1-, 3-, and 5-year) in HFmrEF. Internal validation was conducted using Bootstrap, and the final model was validated in an external cohort of 338 consecutive adult patients. Discrimination and predictive performance were evaluated by calculating the time-dependent concordance index (C-index), area under the ROC curve (AUC), and calibration curve, with clinical value assessed via decision curve analysis (DCA). Integrated discrimination improvement (IDI) and net reclassification improvement (NRI) were used to assess the contributions of NT-proBNP and eGFR to the nomogram. Finally, develop a dynamic nomogram using the \"Dynnom\" package.</p><p><strong>Results: </strong>The optimal independent predictors for all-cause mortality (<i>APSELNH: A: angiotensin-converting enzyme inhibitors/angiotensin receptor blockers/angiotensin receptor-neprilysin inhibitor (ACEI/ARB/ARNI), P: percutaneous coronary intervention/coronary artery bypass graft (PCI/CABG), S: stroke, E: eGFR, L: lg of NT-proBNP</i>, <i>N: NYHA, H: healthcare</i>) were incorporated into the dynamic nomogram. The C-index in the development cohort and validation cohort were 0.858 and 0.826, respectively, with AUCs exceeding 0.8, indicating good discrimination and predictive ability. DCA curves and calibration curves demonstrated clinical applicability and good consistency of the nomogram. NT-proBNP and eGFR provided significant net benefits to the nomogram.</p><p><strong>Conclusion: </strong>In this study, the dynamic APSELNH nomogram developed serves as an accessible, functional, and effective clinical decision support calculator, offering accurate prognostic assessment for patients with HFmrEF.</p>","PeriodicalId":56009,"journal":{"name":"Risk Management and Healthcare Policy","volume":"17 ","pages":"1959-1972"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11330247/pdf/","citationCount":"0","resultStr":"{\"title\":\"Web-Based Dynamic Nomogram for Predicting Risk of Mortality in Heart Failure with Mildly Reduced Ejection Fraction.\",\"authors\":\"Wei Guo, Jing Tian, Yajing Wang, Yajing Zhang, Jingjing Yan, Yutao Du, Yanbo Zhang, Qinghua Han\",\"doi\":\"10.2147/RMHP.S474862\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study aimed to develop an integrative dynamic nomogram, including N-terminal pro-B type natural peptide (NT-proBNP) and estimated glomerular filtration rate (eGFR), for predicting the risk of all-cause mortality in HFmrEF patients.</p><p><strong>Patients and methods: </strong>790 HFmrEF patients were prospectively enrolled in the development cohort for the model. The least absolute shrinkage and selection operator (LASSO) regression and Random Survival Forest (RSF) were employed to select predictors for all-cause mortality. Develop a nomogram based on the Cox proportional hazard model for predicting long-term mortality (1-, 3-, and 5-year) in HFmrEF. Internal validation was conducted using Bootstrap, and the final model was validated in an external cohort of 338 consecutive adult patients. Discrimination and predictive performance were evaluated by calculating the time-dependent concordance index (C-index), area under the ROC curve (AUC), and calibration curve, with clinical value assessed via decision curve analysis (DCA). Integrated discrimination improvement (IDI) and net reclassification improvement (NRI) were used to assess the contributions of NT-proBNP and eGFR to the nomogram. Finally, develop a dynamic nomogram using the \\\"Dynnom\\\" package.</p><p><strong>Results: </strong>The optimal independent predictors for all-cause mortality (<i>APSELNH: A: angiotensin-converting enzyme inhibitors/angiotensin receptor blockers/angiotensin receptor-neprilysin inhibitor (ACEI/ARB/ARNI), P: percutaneous coronary intervention/coronary artery bypass graft (PCI/CABG), S: stroke, E: eGFR, L: lg of NT-proBNP</i>, <i>N: NYHA, H: healthcare</i>) were incorporated into the dynamic nomogram. The C-index in the development cohort and validation cohort were 0.858 and 0.826, respectively, with AUCs exceeding 0.8, indicating good discrimination and predictive ability. DCA curves and calibration curves demonstrated clinical applicability and good consistency of the nomogram. NT-proBNP and eGFR provided significant net benefits to the nomogram.</p><p><strong>Conclusion: </strong>In this study, the dynamic APSELNH nomogram developed serves as an accessible, functional, and effective clinical decision support calculator, offering accurate prognostic assessment for patients with HFmrEF.</p>\",\"PeriodicalId\":56009,\"journal\":{\"name\":\"Risk Management and Healthcare Policy\",\"volume\":\"17 \",\"pages\":\"1959-1972\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-08-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11330247/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Risk Management and Healthcare Policy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/RMHP.S474862\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Risk Management and Healthcare Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/RMHP.S474862","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Web-Based Dynamic Nomogram for Predicting Risk of Mortality in Heart Failure with Mildly Reduced Ejection Fraction.
Purpose: This study aimed to develop an integrative dynamic nomogram, including N-terminal pro-B type natural peptide (NT-proBNP) and estimated glomerular filtration rate (eGFR), for predicting the risk of all-cause mortality in HFmrEF patients.
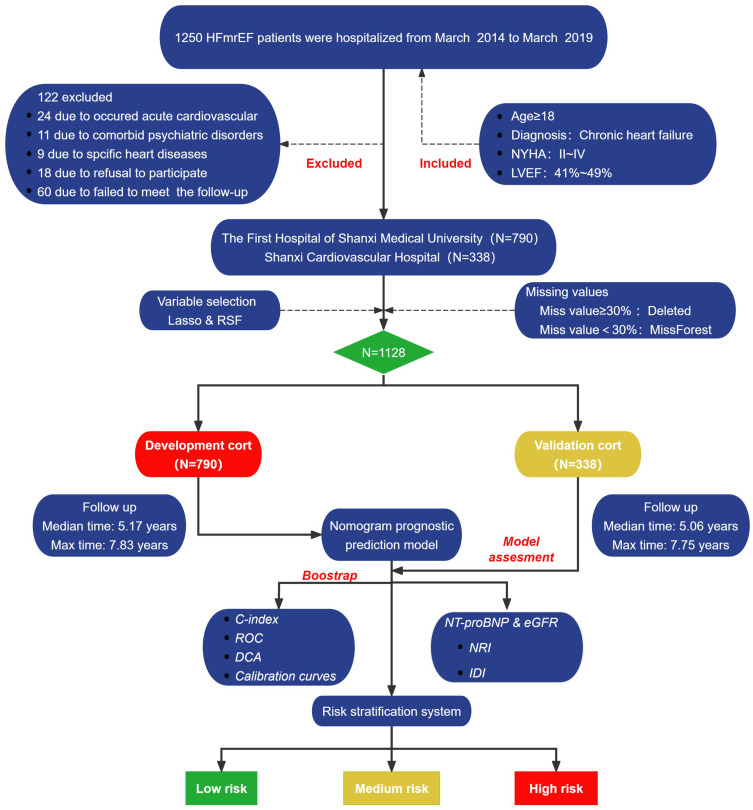
Patients and methods: 790 HFmrEF patients were prospectively enrolled in the development cohort for the model. The least absolute shrinkage and selection operator (LASSO) regression and Random Survival Forest (RSF) were employed to select predictors for all-cause mortality. Develop a nomogram based on the Cox proportional hazard model for predicting long-term mortality (1-, 3-, and 5-year) in HFmrEF. Internal validation was conducted using Bootstrap, and the final model was validated in an external cohort of 338 consecutive adult patients. Discrimination and predictive performance were evaluated by calculating the time-dependent concordance index (C-index), area under the ROC curve (AUC), and calibration curve, with clinical value assessed via decision curve analysis (DCA). Integrated discrimination improvement (IDI) and net reclassification improvement (NRI) were used to assess the contributions of NT-proBNP and eGFR to the nomogram. Finally, develop a dynamic nomogram using the "Dynnom" package.
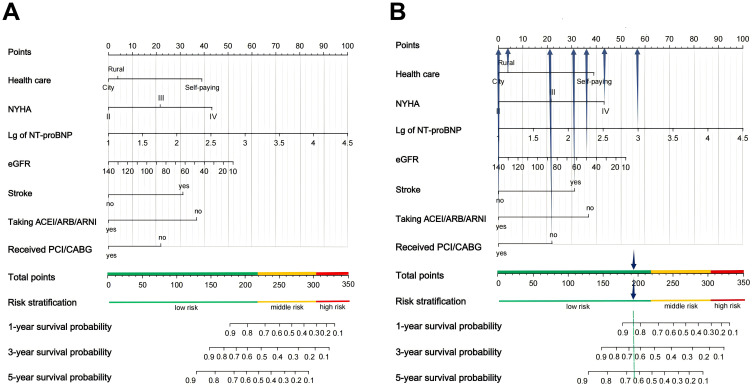
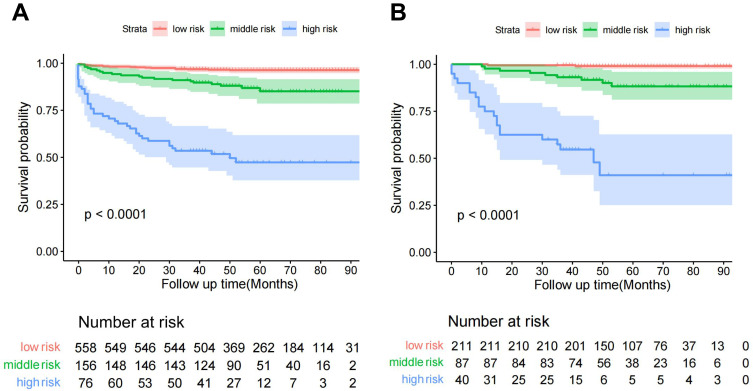
Results: The optimal independent predictors for all-cause mortality (APSELNH: A: angiotensin-converting enzyme inhibitors/angiotensin receptor blockers/angiotensin receptor-neprilysin inhibitor (ACEI/ARB/ARNI), P: percutaneous coronary intervention/coronary artery bypass graft (PCI/CABG), S: stroke, E: eGFR, L: lg of NT-proBNP, N: NYHA, H: healthcare) were incorporated into the dynamic nomogram. The C-index in the development cohort and validation cohort were 0.858 and 0.826, respectively, with AUCs exceeding 0.8, indicating good discrimination and predictive ability. DCA curves and calibration curves demonstrated clinical applicability and good consistency of the nomogram. NT-proBNP and eGFR provided significant net benefits to the nomogram.
Conclusion: In this study, the dynamic APSELNH nomogram developed serves as an accessible, functional, and effective clinical decision support calculator, offering accurate prognostic assessment for patients with HFmrEF.
期刊介绍:
Risk Management and Healthcare Policy is an international, peer-reviewed, open access journal focusing on all aspects of public health, policy and preventative measures to promote good health and improve morbidity and mortality in the population. Specific topics covered in the journal include:
Public and community health
Policy and law
Preventative and predictive healthcare
Risk and hazard management
Epidemiology, detection and screening
Lifestyle and diet modification
Vaccination and disease transmission/modification programs
Health and safety and occupational health
Healthcare services provision
Health literacy and education
Advertising and promotion of health issues
Health economic evaluations and resource management
Risk Management and Healthcare Policy focuses on human interventional and observational research. The journal welcomes submitted papers covering original research, clinical and epidemiological studies, reviews and evaluations, guidelines, expert opinion and commentary, and extended reports. Case reports will only be considered if they make a valuable and original contribution to the literature. The journal does not accept study protocols, animal-based or cell line-based studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


