Theresia Knoche, Charlotte Pietrock, Konrad Neumann, Mirjam Rossel-Zemkouo, Leon Alexander Danyel
{"title":"经眶B型超声波评估特发性颅内高压患者球后扁平:一项试验研究。","authors":"Theresia Knoche, Charlotte Pietrock, Konrad Neumann, Mirjam Rossel-Zemkouo, Leon Alexander Danyel","doi":"10.1186/s13089-024-00388-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Posterior globe flattening (PGF) is a specific neuroimaging sign in patients with idiopathic intracranial hypertension (IIH), but its detection is based on subjective qualitative neuroradiological assessment. This study sought to evaluate the utility of transorbital ultrasound to detect and quantify PGF in IIH patients using the Posterior Globe Angle (PGA).</p><p><strong>Methods: </strong>Consecutive IIH patients and healthy controls were enrolled in a prospective case-control study. Transorbital ultrasound was performed to assess the presence of PGF. For quantification of PGF, an angular measurement (PGA) was performed with the vertex centering the optic nerve at a predefined distance from the lamina cribrosa and angle legs tangentially aligned to the borders of the vitreous body. PGA measurements were compared between IIH patients and healthy controls. Additionally, the diagnostic accuracy of PGA measurements in detecting PGF was evaluated using ROC analysis.</p><p><strong>Results: </strong>Thirty-one IIH patients (37.3 ± 12.3 years, 29 female) and 28 controls (33.3 ± 11.8 years, 21 female) were compared. PGF was present in 39% of IIH patients and absent in the control group. PGA<sub>3mm</sub> measurements significantly differed between IIH and controls (116.5° ± 5.5 vs. 111.7° ± 2.9; p < 0.001). A PGA<sub>3mm</sub> cutoff of ≥ 118.5° distinguished IIH patients from controls with 100% specificity, while retaining a sensitivity of 37.5%.</p><p><strong>Conclusions: </strong>Transorbital ultrasound may be applied to detect and quantify PGF in IIH patients. Prospective, multicenter studies with extended cohorts and blinded design are needed to validate these preliminary findings and confirm the diagnostic utility of transorbital ultrasound for the assessment of PGF in IIH.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"16 1","pages":"39"},"PeriodicalIF":2.9000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11333676/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transorbital B-mode ultrasound for the assessment of posterior globe flattening in idiopathic intracranial hypertension: a pilot study.\",\"authors\":\"Theresia Knoche, Charlotte Pietrock, Konrad Neumann, Mirjam Rossel-Zemkouo, Leon Alexander Danyel\",\"doi\":\"10.1186/s13089-024-00388-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Posterior globe flattening (PGF) is a specific neuroimaging sign in patients with idiopathic intracranial hypertension (IIH), but its detection is based on subjective qualitative neuroradiological assessment. This study sought to evaluate the utility of transorbital ultrasound to detect and quantify PGF in IIH patients using the Posterior Globe Angle (PGA).</p><p><strong>Methods: </strong>Consecutive IIH patients and healthy controls were enrolled in a prospective case-control study. Transorbital ultrasound was performed to assess the presence of PGF. For quantification of PGF, an angular measurement (PGA) was performed with the vertex centering the optic nerve at a predefined distance from the lamina cribrosa and angle legs tangentially aligned to the borders of the vitreous body. PGA measurements were compared between IIH patients and healthy controls. Additionally, the diagnostic accuracy of PGA measurements in detecting PGF was evaluated using ROC analysis.</p><p><strong>Results: </strong>Thirty-one IIH patients (37.3 ± 12.3 years, 29 female) and 28 controls (33.3 ± 11.8 years, 21 female) were compared. PGF was present in 39% of IIH patients and absent in the control group. PGA<sub>3mm</sub> measurements significantly differed between IIH and controls (116.5° ± 5.5 vs. 111.7° ± 2.9; p < 0.001). A PGA<sub>3mm</sub> cutoff of ≥ 118.5° distinguished IIH patients from controls with 100% specificity, while retaining a sensitivity of 37.5%.</p><p><strong>Conclusions: </strong>Transorbital ultrasound may be applied to detect and quantify PGF in IIH patients. Prospective, multicenter studies with extended cohorts and blinded design are needed to validate these preliminary findings and confirm the diagnostic utility of transorbital ultrasound for the assessment of PGF in IIH.</p>\",\"PeriodicalId\":36911,\"journal\":{\"name\":\"Ultrasound Journal\",\"volume\":\"16 1\",\"pages\":\"39\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11333676/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-024-00388-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-024-00388-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Transorbital B-mode ultrasound for the assessment of posterior globe flattening in idiopathic intracranial hypertension: a pilot study.
Background: Posterior globe flattening (PGF) is a specific neuroimaging sign in patients with idiopathic intracranial hypertension (IIH), but its detection is based on subjective qualitative neuroradiological assessment. This study sought to evaluate the utility of transorbital ultrasound to detect and quantify PGF in IIH patients using the Posterior Globe Angle (PGA).
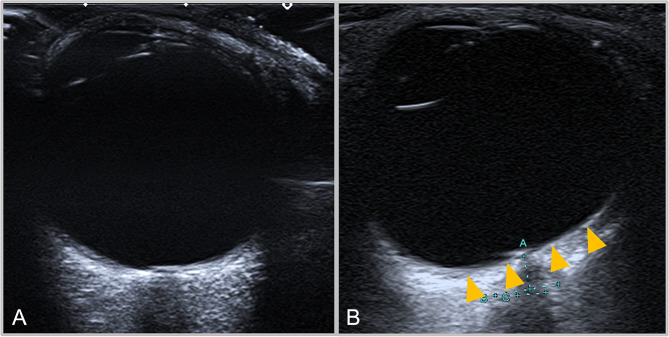
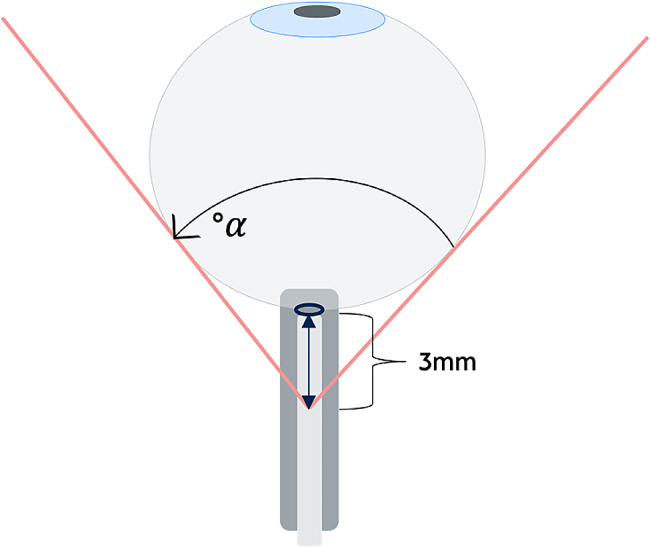
Methods: Consecutive IIH patients and healthy controls were enrolled in a prospective case-control study. Transorbital ultrasound was performed to assess the presence of PGF. For quantification of PGF, an angular measurement (PGA) was performed with the vertex centering the optic nerve at a predefined distance from the lamina cribrosa and angle legs tangentially aligned to the borders of the vitreous body. PGA measurements were compared between IIH patients and healthy controls. Additionally, the diagnostic accuracy of PGA measurements in detecting PGF was evaluated using ROC analysis.
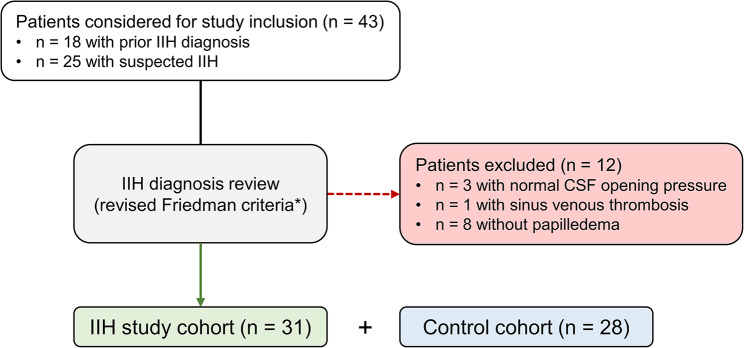
Results: Thirty-one IIH patients (37.3 ± 12.3 years, 29 female) and 28 controls (33.3 ± 11.8 years, 21 female) were compared. PGF was present in 39% of IIH patients and absent in the control group. PGA3mm measurements significantly differed between IIH and controls (116.5° ± 5.5 vs. 111.7° ± 2.9; p < 0.001). A PGA3mm cutoff of ≥ 118.5° distinguished IIH patients from controls with 100% specificity, while retaining a sensitivity of 37.5%.
Conclusions: Transorbital ultrasound may be applied to detect and quantify PGF in IIH patients. Prospective, multicenter studies with extended cohorts and blinded design are needed to validate these preliminary findings and confirm the diagnostic utility of transorbital ultrasound for the assessment of PGF in IIH.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


