Lucy Collins, Eleanor Angley, Joel Smith, Fergus Cameron, Phoebe Stewart
{"title":"警惕虚假 HbA1c:罕见的 alpha1-globin 基因突变。","authors":"Lucy Collins, Eleanor Angley, Joel Smith, Fergus Cameron, Phoebe Stewart","doi":"10.1111/jpc.16649","DOIUrl":null,"url":null,"abstract":"<p>An 11-year-old girl was investigated for impaired glucose tolerance. Her medical history included transient congenital hypothyroidism. Her family medical history was notable for type 2 diabetes mellitus affecting her mother, maternal grandmother, maternal uncle and paternal grandfather. She denied history of polyuria, polydipsia, weight loss and exogenous glucocorticoid administration. On examination, her weight was 72.3 kg (99.5 percentile, <i>Z</i> = 2.59), height 160.5 cm (98.9 percentile, <i>Z</i> = 2.30) and body mass index 28.1 kg/m<sup>2</sup> (98.0 percentile, <i>Z</i> = 2.06). Acanthosis nigricans was noted circumferentially around her neck. There was no clinical stigmata of endogenous hypercortisolism. Initial biochemistry (Table 1) demonstrated elevated glycosylated haemoglobin (HbA1c) at 14.9%. Antibodies associated with type 1 diabetes mellitus were negative. Full blood count, thyroid function, renal function and haematinics were unremarkable. C-peptide was elevated. Liver function, urinary albumin/creatinine ratio and lipid profile were unremarkable.</p><p>Repeat HbA1c (14.5%, Biorad D10 Ion exchange chromatography, Fig. 1) was elevated. A presumed diagnosis of type 2 diabetes was made. Metformin extended release and 18 units of basal insulin were commenced, in addition to life-style and dietary intervention. Blood glucose monitoring reflected excellent glycaemic control, with blood sugar levels between 4.7 and 6.3 mmol/L. Basal insulin was rapidly reduced, and eventually ceased after 4 weeks due to stable blood glucose levels. A spurious HbA1c result was suspected.</p><p>Fructosamine was low at 231 μmol/L (250–380) and oral glucose tolerance test (OGTT) was normal; fasting glucose 4.5 mmol/L (<6.1 mmol), 60-min glucose 5.0 mmol/L (<7.8 mmol/L) and 120-min glucose 4.6 mmol/L (<7.8 mmol/L). A Freestyle Libre 2 Continuous Glucose Monitoring System displayed 99% of blood glucose readings in range (3.9–10.0 mmol/L). HbA1c was repeated on an alternative assay. HbA1c was normal at 5.4% (Trinity Biotech Boronate Affinity Chromatography). Metformin was ceased, and the diagnosis of type 2 diabetes was revised.</p><p>An underlying haemoglobinopathy was hypothesised to cause the discrepancy in HbA1c and OGTT results. A haemoglobinopathy screen detected an abnormal haemoglobin variant in zone 11 of 10.6%, suggestive of an uncommon alpha variant (Fig. 2). Genetic testing was undertaken. DNA sequencing found her to be compound heterozygous for the common single gene deletion (−alpha 3.7) alpha thalassaemia mutation and the HbA1:c382A>G (Hb Shantou) variant in the alpha1-globin gene. The HbA1:c382A>G (Hb Shantou) genetic variant is responsible for the haemoglobin variant.</p><p>Cascade testing in her family is underway.</p><p>The incidence of paediatric type 2 diabetes has increased, especially in high-risk ethnic groups (Indigenous Australians, Pacific Islanders and Maori people).<span><sup>1</sup></span> Close monitoring and intensive management of paediatric type 2 diabetes is crucial; glycaemic control typically deteriorates quickly, and complications occur earlier than in adults. Diagnosis is based on fasting glucose, or 2-h glucose concentration during an OGTT or HbA1c. In the absence of symptoms, testing should be confirmed with a repeat test on a different day.<span><sup>2</sup></span></p><p>HbA1c holds a central role in the diagnosis and management of diabetes mellitus. The rate of A1c formation is proportional to the concentration of glucose within the erythrocyte during its life-span, typically 120 days. It is important to be alert to clinical scenarios and interfering factors that may yield false results.<span><sup>3</sup></span> Falsely elevated HbA1c can be seen in any condition that prolongs the life of the erythrocyte or is associated with reduced red cell turnover, such as iron/B12/folate deficiency anaemia and asplenia. Severe hypertriglyceridaemia, hyperbilirubinaemia and uraemia may also falsely elevate HbA1c.<span><sup>3</sup></span> Falsely low HbA1c results can be seen in acute and chronic bone loss, haemolytic anaemia and splenomegaly. In addition, haemoglobin variants can lead to falsely elevated or lowered HbA1c. If the amino acid substitution causes a change in the net charge (as with HbS, C, D and E), ion-exchange high-performance liquid chromatography (HPLC) or electrophoresis may be affected. If a substitution occurs at a glycation site, the rate of glycation may be affected. If the variant causes a reduced erythrocyte life-span, the HbA1c would be falsely lowered, irrespective of method used.<span><sup>4</sup></span> The presence of a haemoglobin variant should be suspected in patients with incongruent glucose monitoring and HbA1c results, markedly elevated HbA1c results>15% and significantly different HbA1c results compared to a previous value.<span><sup>3</sup></span></p><p>Reports of Hb Shantou (HbA1:c382A>G) are limited.<span><sup>5</sup></span> Hb Shantou reflects a nucleotide mutation at position c.382 A>G on the α1-globin gene. A single published report describes a case of a falsely high HbA1c value in a pregnant woman of Chinese ethnicity due to this novel α1-globin gene mutation.<span><sup>5</sup></span></p><p>Fructosamine measurement, glycated albumin and continuous glucose monitoring may provide alternatives to HbA1c. Fructosamine, the product formed by a nonenzymatic reaction of glucose and serum proteins, reflects a shorter period of glycaemic control (typically 2–3 weeks) compared to HbA1c as the half-life of albumin is approximately 20 days.<span><sup>3</sup></span> The accuracy of fructosamine measurement is limited in situations of hypoproteinaemia/hypoalbuminaemia, such as nephrotic syndrome and chronic liver disease. In addition, boronate affinity HPLC, subsequently utilised in our case, is not typically affected by haemoglobin variant interference<span><sup>6</sup></span> and may provide a more accurate representation of glycaemic control.</p><p>In conclusion, as rates of type 2 diabetes increase in our paediatric population, clinicians should be alert to the limitations and inaccuracies of diagnostic and monitoring tests, most notably HbA1c. Haemoglobin variants may falsely elevate or lower HbA1c, and alternative diagnostic methods are required to improve accuracy.</p>","PeriodicalId":16648,"journal":{"name":"Journal of paediatrics and child health","volume":"60 10","pages":"610-612"},"PeriodicalIF":1.4000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16649","citationCount":"0","resultStr":"{\"title\":\"Be alert to a spurious HbA1c: A rare alpha1-globin gene mutation\",\"authors\":\"Lucy Collins, Eleanor Angley, Joel Smith, Fergus Cameron, Phoebe Stewart\",\"doi\":\"10.1111/jpc.16649\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>An 11-year-old girl was investigated for impaired glucose tolerance. Her medical history included transient congenital hypothyroidism. Her family medical history was notable for type 2 diabetes mellitus affecting her mother, maternal grandmother, maternal uncle and paternal grandfather. She denied history of polyuria, polydipsia, weight loss and exogenous glucocorticoid administration. On examination, her weight was 72.3 kg (99.5 percentile, <i>Z</i> = 2.59), height 160.5 cm (98.9 percentile, <i>Z</i> = 2.30) and body mass index 28.1 kg/m<sup>2</sup> (98.0 percentile, <i>Z</i> = 2.06). Acanthosis nigricans was noted circumferentially around her neck. There was no clinical stigmata of endogenous hypercortisolism. Initial biochemistry (Table 1) demonstrated elevated glycosylated haemoglobin (HbA1c) at 14.9%. Antibodies associated with type 1 diabetes mellitus were negative. Full blood count, thyroid function, renal function and haematinics were unremarkable. C-peptide was elevated. Liver function, urinary albumin/creatinine ratio and lipid profile were unremarkable.</p><p>Repeat HbA1c (14.5%, Biorad D10 Ion exchange chromatography, Fig. 1) was elevated. A presumed diagnosis of type 2 diabetes was made. Metformin extended release and 18 units of basal insulin were commenced, in addition to life-style and dietary intervention. Blood glucose monitoring reflected excellent glycaemic control, with blood sugar levels between 4.7 and 6.3 mmol/L. Basal insulin was rapidly reduced, and eventually ceased after 4 weeks due to stable blood glucose levels. A spurious HbA1c result was suspected.</p><p>Fructosamine was low at 231 μmol/L (250–380) and oral glucose tolerance test (OGTT) was normal; fasting glucose 4.5 mmol/L (<6.1 mmol), 60-min glucose 5.0 mmol/L (<7.8 mmol/L) and 120-min glucose 4.6 mmol/L (<7.8 mmol/L). A Freestyle Libre 2 Continuous Glucose Monitoring System displayed 99% of blood glucose readings in range (3.9–10.0 mmol/L). HbA1c was repeated on an alternative assay. HbA1c was normal at 5.4% (Trinity Biotech Boronate Affinity Chromatography). Metformin was ceased, and the diagnosis of type 2 diabetes was revised.</p><p>An underlying haemoglobinopathy was hypothesised to cause the discrepancy in HbA1c and OGTT results. A haemoglobinopathy screen detected an abnormal haemoglobin variant in zone 11 of 10.6%, suggestive of an uncommon alpha variant (Fig. 2). Genetic testing was undertaken. DNA sequencing found her to be compound heterozygous for the common single gene deletion (−alpha 3.7) alpha thalassaemia mutation and the HbA1:c382A>G (Hb Shantou) variant in the alpha1-globin gene. The HbA1:c382A>G (Hb Shantou) genetic variant is responsible for the haemoglobin variant.</p><p>Cascade testing in her family is underway.</p><p>The incidence of paediatric type 2 diabetes has increased, especially in high-risk ethnic groups (Indigenous Australians, Pacific Islanders and Maori people).<span><sup>1</sup></span> Close monitoring and intensive management of paediatric type 2 diabetes is crucial; glycaemic control typically deteriorates quickly, and complications occur earlier than in adults. Diagnosis is based on fasting glucose, or 2-h glucose concentration during an OGTT or HbA1c. In the absence of symptoms, testing should be confirmed with a repeat test on a different day.<span><sup>2</sup></span></p><p>HbA1c holds a central role in the diagnosis and management of diabetes mellitus. The rate of A1c formation is proportional to the concentration of glucose within the erythrocyte during its life-span, typically 120 days. It is important to be alert to clinical scenarios and interfering factors that may yield false results.<span><sup>3</sup></span> Falsely elevated HbA1c can be seen in any condition that prolongs the life of the erythrocyte or is associated with reduced red cell turnover, such as iron/B12/folate deficiency anaemia and asplenia. Severe hypertriglyceridaemia, hyperbilirubinaemia and uraemia may also falsely elevate HbA1c.<span><sup>3</sup></span> Falsely low HbA1c results can be seen in acute and chronic bone loss, haemolytic anaemia and splenomegaly. In addition, haemoglobin variants can lead to falsely elevated or lowered HbA1c. If the amino acid substitution causes a change in the net charge (as with HbS, C, D and E), ion-exchange high-performance liquid chromatography (HPLC) or electrophoresis may be affected. If a substitution occurs at a glycation site, the rate of glycation may be affected. If the variant causes a reduced erythrocyte life-span, the HbA1c would be falsely lowered, irrespective of method used.<span><sup>4</sup></span> The presence of a haemoglobin variant should be suspected in patients with incongruent glucose monitoring and HbA1c results, markedly elevated HbA1c results>15% and significantly different HbA1c results compared to a previous value.<span><sup>3</sup></span></p><p>Reports of Hb Shantou (HbA1:c382A>G) are limited.<span><sup>5</sup></span> Hb Shantou reflects a nucleotide mutation at position c.382 A>G on the α1-globin gene. A single published report describes a case of a falsely high HbA1c value in a pregnant woman of Chinese ethnicity due to this novel α1-globin gene mutation.<span><sup>5</sup></span></p><p>Fructosamine measurement, glycated albumin and continuous glucose monitoring may provide alternatives to HbA1c. Fructosamine, the product formed by a nonenzymatic reaction of glucose and serum proteins, reflects a shorter period of glycaemic control (typically 2–3 weeks) compared to HbA1c as the half-life of albumin is approximately 20 days.<span><sup>3</sup></span> The accuracy of fructosamine measurement is limited in situations of hypoproteinaemia/hypoalbuminaemia, such as nephrotic syndrome and chronic liver disease. In addition, boronate affinity HPLC, subsequently utilised in our case, is not typically affected by haemoglobin variant interference<span><sup>6</sup></span> and may provide a more accurate representation of glycaemic control.</p><p>In conclusion, as rates of type 2 diabetes increase in our paediatric population, clinicians should be alert to the limitations and inaccuracies of diagnostic and monitoring tests, most notably HbA1c. Haemoglobin variants may falsely elevate or lower HbA1c, and alternative diagnostic methods are required to improve accuracy.</p>\",\"PeriodicalId\":16648,\"journal\":{\"name\":\"Journal of paediatrics and child health\",\"volume\":\"60 10\",\"pages\":\"610-612\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16649\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of paediatrics and child health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16649\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of paediatrics and child health","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16649","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Be alert to a spurious HbA1c: A rare alpha1-globin gene mutation
An 11-year-old girl was investigated for impaired glucose tolerance. Her medical history included transient congenital hypothyroidism. Her family medical history was notable for type 2 diabetes mellitus affecting her mother, maternal grandmother, maternal uncle and paternal grandfather. She denied history of polyuria, polydipsia, weight loss and exogenous glucocorticoid administration. On examination, her weight was 72.3 kg (99.5 percentile, Z = 2.59), height 160.5 cm (98.9 percentile, Z = 2.30) and body mass index 28.1 kg/m2 (98.0 percentile, Z = 2.06). Acanthosis nigricans was noted circumferentially around her neck. There was no clinical stigmata of endogenous hypercortisolism. Initial biochemistry (Table 1) demonstrated elevated glycosylated haemoglobin (HbA1c) at 14.9%. Antibodies associated with type 1 diabetes mellitus were negative. Full blood count, thyroid function, renal function and haematinics were unremarkable. C-peptide was elevated. Liver function, urinary albumin/creatinine ratio and lipid profile were unremarkable.
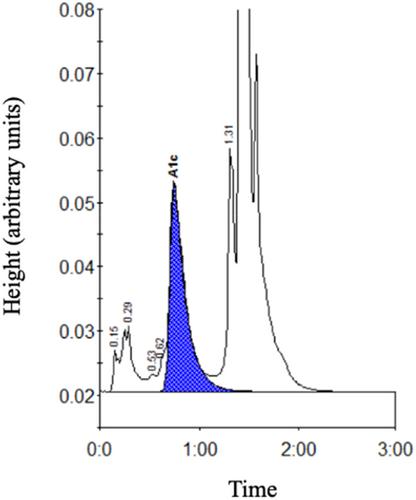
Repeat HbA1c (14.5%, Biorad D10 Ion exchange chromatography, Fig. 1) was elevated. A presumed diagnosis of type 2 diabetes was made. Metformin extended release and 18 units of basal insulin were commenced, in addition to life-style and dietary intervention. Blood glucose monitoring reflected excellent glycaemic control, with blood sugar levels between 4.7 and 6.3 mmol/L. Basal insulin was rapidly reduced, and eventually ceased after 4 weeks due to stable blood glucose levels. A spurious HbA1c result was suspected.
Fructosamine was low at 231 μmol/L (250–380) and oral glucose tolerance test (OGTT) was normal; fasting glucose 4.5 mmol/L (<6.1 mmol), 60-min glucose 5.0 mmol/L (<7.8 mmol/L) and 120-min glucose 4.6 mmol/L (<7.8 mmol/L). A Freestyle Libre 2 Continuous Glucose Monitoring System displayed 99% of blood glucose readings in range (3.9–10.0 mmol/L). HbA1c was repeated on an alternative assay. HbA1c was normal at 5.4% (Trinity Biotech Boronate Affinity Chromatography). Metformin was ceased, and the diagnosis of type 2 diabetes was revised.
An underlying haemoglobinopathy was hypothesised to cause the discrepancy in HbA1c and OGTT results. A haemoglobinopathy screen detected an abnormal haemoglobin variant in zone 11 of 10.6%, suggestive of an uncommon alpha variant (Fig. 2). Genetic testing was undertaken. DNA sequencing found her to be compound heterozygous for the common single gene deletion (−alpha 3.7) alpha thalassaemia mutation and the HbA1:c382A>G (Hb Shantou) variant in the alpha1-globin gene. The HbA1:c382A>G (Hb Shantou) genetic variant is responsible for the haemoglobin variant.
Cascade testing in her family is underway.
The incidence of paediatric type 2 diabetes has increased, especially in high-risk ethnic groups (Indigenous Australians, Pacific Islanders and Maori people).1 Close monitoring and intensive management of paediatric type 2 diabetes is crucial; glycaemic control typically deteriorates quickly, and complications occur earlier than in adults. Diagnosis is based on fasting glucose, or 2-h glucose concentration during an OGTT or HbA1c. In the absence of symptoms, testing should be confirmed with a repeat test on a different day.2
HbA1c holds a central role in the diagnosis and management of diabetes mellitus. The rate of A1c formation is proportional to the concentration of glucose within the erythrocyte during its life-span, typically 120 days. It is important to be alert to clinical scenarios and interfering factors that may yield false results.3 Falsely elevated HbA1c can be seen in any condition that prolongs the life of the erythrocyte or is associated with reduced red cell turnover, such as iron/B12/folate deficiency anaemia and asplenia. Severe hypertriglyceridaemia, hyperbilirubinaemia and uraemia may also falsely elevate HbA1c.3 Falsely low HbA1c results can be seen in acute and chronic bone loss, haemolytic anaemia and splenomegaly. In addition, haemoglobin variants can lead to falsely elevated or lowered HbA1c. If the amino acid substitution causes a change in the net charge (as with HbS, C, D and E), ion-exchange high-performance liquid chromatography (HPLC) or electrophoresis may be affected. If a substitution occurs at a glycation site, the rate of glycation may be affected. If the variant causes a reduced erythrocyte life-span, the HbA1c would be falsely lowered, irrespective of method used.4 The presence of a haemoglobin variant should be suspected in patients with incongruent glucose monitoring and HbA1c results, markedly elevated HbA1c results>15% and significantly different HbA1c results compared to a previous value.3
Reports of Hb Shantou (HbA1:c382A>G) are limited.5 Hb Shantou reflects a nucleotide mutation at position c.382 A>G on the α1-globin gene. A single published report describes a case of a falsely high HbA1c value in a pregnant woman of Chinese ethnicity due to this novel α1-globin gene mutation.5
Fructosamine measurement, glycated albumin and continuous glucose monitoring may provide alternatives to HbA1c. Fructosamine, the product formed by a nonenzymatic reaction of glucose and serum proteins, reflects a shorter period of glycaemic control (typically 2–3 weeks) compared to HbA1c as the half-life of albumin is approximately 20 days.3 The accuracy of fructosamine measurement is limited in situations of hypoproteinaemia/hypoalbuminaemia, such as nephrotic syndrome and chronic liver disease. In addition, boronate affinity HPLC, subsequently utilised in our case, is not typically affected by haemoglobin variant interference6 and may provide a more accurate representation of glycaemic control.
In conclusion, as rates of type 2 diabetes increase in our paediatric population, clinicians should be alert to the limitations and inaccuracies of diagnostic and monitoring tests, most notably HbA1c. Haemoglobin variants may falsely elevate or lower HbA1c, and alternative diagnostic methods are required to improve accuracy.
期刊介绍:
The Journal of Paediatrics and Child Health publishes original research articles of scientific excellence in paediatrics and child health. Research Articles, Case Reports and Letters to the Editor are published, together with invited Reviews, Annotations, Editorial Comments and manuscripts of educational interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



