Daniel J. Hammersley, Srinjay Mukhopadhyay, Xiuyu Chen, Richard E. Jones, Aaraby Ragavan, Saad Javed, Husein Rajabali, Emmanuel Androulakis, Lara Curran, Lukas Mach, Zohya Khalique, Resham Baruah, Kaushik Guha, John Gregson, Shihua Zhao, Antonio De Marvao, Upasana Tayal, Amrit S. Lota, James S. Ware, Dudley J. Pennell, Sanjay K. Prasad, Brian P. Halliday
{"title":"利用多参数心血管磁共振精确预测扩张型心肌病和射血分数轻度降低患者的心衰事件。","authors":"Daniel J. Hammersley, Srinjay Mukhopadhyay, Xiuyu Chen, Richard E. Jones, Aaraby Ragavan, Saad Javed, Husein Rajabali, Emmanuel Androulakis, Lara Curran, Lukas Mach, Zohya Khalique, Resham Baruah, Kaushik Guha, John Gregson, Shihua Zhao, Antonio De Marvao, Upasana Tayal, Amrit S. Lota, James S. Ware, Dudley J. Pennell, Sanjay K. Prasad, Brian P. Halliday","doi":"10.1002/ejhf.3425","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>To assess whether left ventricular (LV) global longitudinal strain (GLS), derived from cardiovascular magnetic resonance (CMR), is associated with (i) progressive heart failure (HF), and (ii) sudden cardiac death (SCD) in patients with dilated cardiomyopathy with mildly reduced ejection fraction (DCMmrEF).</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>We conducted a prospective observational cohort study of patients with DCM and LV ejection fraction (LVEF) ≥40% assessed by CMR, including feature-tracking to assess LV GLS and late gadolinium enhancement (LGE). Long-term adjudicated follow-up included (i) HF hospitalization, LV assist device implantation or HF death, and (ii) SCD or aborted SCD (aSCD). Of 355 patients with DCMmrEF (median age 54 years [interquartile range 43–64], 216 men [60.8%], median LVEF 49% [46–54]) followed up for a median 7.8 years (5.2–9.4), 32 patients (9%) experienced HF events and 19 (5%) died suddenly or experienced aSCD. LV GLS was associated with HF events in a multivariable model when considered as either a continuous (per % hazard ratio [HR] 1.10, 95% confidence interval [CI] 1.00–1.21, <i>p</i> = 0.045) or dichotomized variable (LV GLS > −15.4%: HR 2.70, 95% CI 1.30–5.94, <i>p</i> = 0.008). LGE presence was\n not associated with HF events (HR 1.49, 95% CI 0.73–3.01, <i>p</i> = 0.270). Conversely, LV GLS was not associated with SCD/aSCD (per % HR 1.07, 95% CI 0.95–1.22, <i>p</i> = 0.257), whereas LGE presence was (HR 3.58, 95% CI 1.39–9.23, <i>p</i> = 0.008). LVEF was neither associated with HF events nor SCD/aSCD.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Multi-parametric CMR has utility for precision prognostic stratification of patients with DCMmrEF. LV GLS stratifies risk of progressive HF, while LGE stratifies SCD risk.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"26 12","pages":"2553-2562"},"PeriodicalIF":10.8000,"publicationDate":"2024-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7616534/pdf/","citationCount":"0","resultStr":"{\"title\":\"Precision prediction of heart failure events in patients with dilated cardiomyopathy and mildly reduced ejection fraction using multi-parametric cardiovascular magnetic resonance\",\"authors\":\"Daniel J. Hammersley, Srinjay Mukhopadhyay, Xiuyu Chen, Richard E. Jones, Aaraby Ragavan, Saad Javed, Husein Rajabali, Emmanuel Androulakis, Lara Curran, Lukas Mach, Zohya Khalique, Resham Baruah, Kaushik Guha, John Gregson, Shihua Zhao, Antonio De Marvao, Upasana Tayal, Amrit S. Lota, James S. Ware, Dudley J. Pennell, Sanjay K. Prasad, Brian P. Halliday\",\"doi\":\"10.1002/ejhf.3425\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>To assess whether left ventricular (LV) global longitudinal strain (GLS), derived from cardiovascular magnetic resonance (CMR), is associated with (i) progressive heart failure (HF), and (ii) sudden cardiac death (SCD) in patients with dilated cardiomyopathy with mildly reduced ejection fraction (DCMmrEF).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>We conducted a prospective observational cohort study of patients with DCM and LV ejection fraction (LVEF) ≥40% assessed by CMR, including feature-tracking to assess LV GLS and late gadolinium enhancement (LGE). Long-term adjudicated follow-up included (i) HF hospitalization, LV assist device implantation or HF death, and (ii) SCD or aborted SCD (aSCD). Of 355 patients with DCMmrEF (median age 54 years [interquartile range 43–64], 216 men [60.8%], median LVEF 49% [46–54]) followed up for a median 7.8 years (5.2–9.4), 32 patients (9%) experienced HF events and 19 (5%) died suddenly or experienced aSCD. LV GLS was associated with HF events in a multivariable model when considered as either a continuous (per % hazard ratio [HR] 1.10, 95% confidence interval [CI] 1.00–1.21, <i>p</i> = 0.045) or dichotomized variable (LV GLS > −15.4%: HR 2.70, 95% CI 1.30–5.94, <i>p</i> = 0.008). LGE presence was\\n not associated with HF events (HR 1.49, 95% CI 0.73–3.01, <i>p</i> = 0.270). Conversely, LV GLS was not associated with SCD/aSCD (per % HR 1.07, 95% CI 0.95–1.22, <i>p</i> = 0.257), whereas LGE presence was (HR 3.58, 95% CI 1.39–9.23, <i>p</i> = 0.008). LVEF was neither associated with HF events nor SCD/aSCD.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Multi-parametric CMR has utility for precision prognostic stratification of patients with DCMmrEF. LV GLS stratifies risk of progressive HF, while LGE stratifies SCD risk.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"26 12\",\"pages\":\"2553-2562\"},\"PeriodicalIF\":10.8000,\"publicationDate\":\"2024-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7616534/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3425\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3425","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Precision prediction of heart failure events in patients with dilated cardiomyopathy and mildly reduced ejection fraction using multi-parametric cardiovascular magnetic resonance
Aims
To assess whether left ventricular (LV) global longitudinal strain (GLS), derived from cardiovascular magnetic resonance (CMR), is associated with (i) progressive heart failure (HF), and (ii) sudden cardiac death (SCD) in patients with dilated cardiomyopathy with mildly reduced ejection fraction (DCMmrEF).
Methods and results
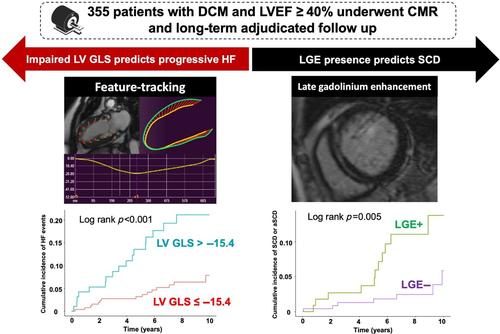
We conducted a prospective observational cohort study of patients with DCM and LV ejection fraction (LVEF) ≥40% assessed by CMR, including feature-tracking to assess LV GLS and late gadolinium enhancement (LGE). Long-term adjudicated follow-up included (i) HF hospitalization, LV assist device implantation or HF death, and (ii) SCD or aborted SCD (aSCD). Of 355 patients with DCMmrEF (median age 54 years [interquartile range 43–64], 216 men [60.8%], median LVEF 49% [46–54]) followed up for a median 7.8 years (5.2–9.4), 32 patients (9%) experienced HF events and 19 (5%) died suddenly or experienced aSCD. LV GLS was associated with HF events in a multivariable model when considered as either a continuous (per % hazard ratio [HR] 1.10, 95% confidence interval [CI] 1.00–1.21, p = 0.045) or dichotomized variable (LV GLS > −15.4%: HR 2.70, 95% CI 1.30–5.94, p = 0.008). LGE presence was
not associated with HF events (HR 1.49, 95% CI 0.73–3.01, p = 0.270). Conversely, LV GLS was not associated with SCD/aSCD (per % HR 1.07, 95% CI 0.95–1.22, p = 0.257), whereas LGE presence was (HR 3.58, 95% CI 1.39–9.23, p = 0.008). LVEF was neither associated with HF events nor SCD/aSCD.
Conclusion
Multi-parametric CMR has utility for precision prognostic stratification of patients with DCMmrEF. LV GLS stratifies risk of progressive HF, while LGE stratifies SCD risk.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


