Sriram Deivasigamani, Eric S Adams, Shannon Stock, Srinath Kotamarti, Denis Séguier, Tarek Taha, Lauren E Howard, Alireza Aminsharifi, Ghalib Jibara, Christopher L Amling, William J Aronson, Matthew R Cooperberg, Christopher J Kane, Martha K Terris, Zachary Klaassen, Lourdes Guerrios-Rivera, Stephen J Freedland, Thomas J Polascik
{"title":"根据根治性前列腺切除术的组织病理学,选择黑人男性作为中危前列腺癌前列腺半消融术的潜在候选者--一项多中心 SEARCH 队列研究。","authors":"Sriram Deivasigamani, Eric S Adams, Shannon Stock, Srinath Kotamarti, Denis Séguier, Tarek Taha, Lauren E Howard, Alireza Aminsharifi, Ghalib Jibara, Christopher L Amling, William J Aronson, Matthew R Cooperberg, Christopher J Kane, Martha K Terris, Zachary Klaassen, Lourdes Guerrios-Rivera, Stephen J Freedland, Thomas J Polascik","doi":"10.1038/s41391-024-00880-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance and objective: </strong>Partial gland ablation (PGA) is increasingly popular as a treatment for men with intermediate-risk prostate cancer (IR-PCa) to preserve functional outcomes while controlling their cancer. We aimed to determine the impact of race and clinical characteristics on the risk of upstaging (≥pT2c) and having adverse pathological outcomes including seminal vesicle invasion (SVI), extra prostatic extension (EPE) and lymph node invasion (LNI) at radical prostatectomy (RP) among men with IR disease eligible for PGA with hemi-ablation (HA).</p><p><strong>Design: </strong>Retrospective analysis.</p><p><strong>Setting: </strong>Multicenter.</p><p><strong>Participants and measures: </strong>We studied patients diagnosed with unilateral IR-PCa treated with RP between 1988 and 2020 at 9 different Veterans Affairs hospitals within the SEARCH cohort. We analyzed differences in clinicopathological characteristics and outcome variables (odds of ≥pT2c and SVI, EPE and LNI) by race using multivariable logistic regression after adjusting for covariates.</p><p><strong>Results: </strong>Among 3127 patients, 33% were African American (AA) men with unilateral IR-PCa undergoing RP. Compared to non-AA men, AA individuals were younger (61 vs. 65 years, p < 0.001), presented with a higher prostate specific antigen (PSA) category (≥10 ng/ml; 34 vs. 26%, p < 0.001), and had a lower clinical stage (p < 0.001). Among the 2,798 (89.5%) with ≥pT2c stage, AA men exhibited higher ≥ pT2c rates (93 vs. 89%, p < 0.001), primarily due to increased pT2c staging (64 vs. 57%), where upstaging beyond pT2 was lower than non-AA men (29 vs. 32%). On multivariable analysis, AA men were found to have higher odds of ≥pT2c (odds ratio [OR]: 1.39 CI, 1.02-1.88, p = 0.04), lower odds of EPE (OR: 0.73 CI, 0.58-0.91, p < 0.01) and no statistically significant associations with LNI (OR: 0.79 CI, 0.42-1.46, p = 0.45) and SVI (OR: 1 CI, 0.74-1.35, p = 0.99) compared to non-AA men. On multivariable analysis, clinical features associated with higher odds of ≥pT2c were pre-operative PSA ≥ 15 (OR = 2.07, P = 0.01) and higher number of positive cores (HPC) on biopsy (OR = 1.36, P < 0.001). Similarly, PSA ≥ 15, Gleason grade ≥3 and HPC on biopsy were associated with higher odds of SVI, EPE and LNI, respectively.</p><p><strong>Conclusions: </strong>In men with IR-PCa undergoing RP, AA men demonstrated an overall higher likelihood of ≥pT2c with lower upstaging beyond pT2, lower likelihood of EPE and no significant difference in likelihood of SVI and LNI compared to non-AA men. These findings support select AA men to be potential candidates for PGA, such as HA. Clinical factors are predictive of higher pathological stage and adverse pathological outcomes at RP and could be considered when selecting candidates for PGA.</p>","PeriodicalId":20727,"journal":{"name":"Prostate Cancer and Prostatic Diseases","volume":" ","pages":""},"PeriodicalIF":5.1000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Select black men are potential candidates for prostate hemi-ablation based on radical prostatectomy histopathology for intermediate-risk prostate cancer-a multicenter SEARCH cohort study.\",\"authors\":\"Sriram Deivasigamani, Eric S Adams, Shannon Stock, Srinath Kotamarti, Denis Séguier, Tarek Taha, Lauren E Howard, Alireza Aminsharifi, Ghalib Jibara, Christopher L Amling, William J Aronson, Matthew R Cooperberg, Christopher J Kane, Martha K Terris, Zachary Klaassen, Lourdes Guerrios-Rivera, Stephen J Freedland, Thomas J Polascik\",\"doi\":\"10.1038/s41391-024-00880-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance and objective: </strong>Partial gland ablation (PGA) is increasingly popular as a treatment for men with intermediate-risk prostate cancer (IR-PCa) to preserve functional outcomes while controlling their cancer. We aimed to determine the impact of race and clinical characteristics on the risk of upstaging (≥pT2c) and having adverse pathological outcomes including seminal vesicle invasion (SVI), extra prostatic extension (EPE) and lymph node invasion (LNI) at radical prostatectomy (RP) among men with IR disease eligible for PGA with hemi-ablation (HA).</p><p><strong>Design: </strong>Retrospective analysis.</p><p><strong>Setting: </strong>Multicenter.</p><p><strong>Participants and measures: </strong>We studied patients diagnosed with unilateral IR-PCa treated with RP between 1988 and 2020 at 9 different Veterans Affairs hospitals within the SEARCH cohort. We analyzed differences in clinicopathological characteristics and outcome variables (odds of ≥pT2c and SVI, EPE and LNI) by race using multivariable logistic regression after adjusting for covariates.</p><p><strong>Results: </strong>Among 3127 patients, 33% were African American (AA) men with unilateral IR-PCa undergoing RP. Compared to non-AA men, AA individuals were younger (61 vs. 65 years, p < 0.001), presented with a higher prostate specific antigen (PSA) category (≥10 ng/ml; 34 vs. 26%, p < 0.001), and had a lower clinical stage (p < 0.001). Among the 2,798 (89.5%) with ≥pT2c stage, AA men exhibited higher ≥ pT2c rates (93 vs. 89%, p < 0.001), primarily due to increased pT2c staging (64 vs. 57%), where upstaging beyond pT2 was lower than non-AA men (29 vs. 32%). On multivariable analysis, AA men were found to have higher odds of ≥pT2c (odds ratio [OR]: 1.39 CI, 1.02-1.88, p = 0.04), lower odds of EPE (OR: 0.73 CI, 0.58-0.91, p < 0.01) and no statistically significant associations with LNI (OR: 0.79 CI, 0.42-1.46, p = 0.45) and SVI (OR: 1 CI, 0.74-1.35, p = 0.99) compared to non-AA men. On multivariable analysis, clinical features associated with higher odds of ≥pT2c were pre-operative PSA ≥ 15 (OR = 2.07, P = 0.01) and higher number of positive cores (HPC) on biopsy (OR = 1.36, P < 0.001). Similarly, PSA ≥ 15, Gleason grade ≥3 and HPC on biopsy were associated with higher odds of SVI, EPE and LNI, respectively.</p><p><strong>Conclusions: </strong>In men with IR-PCa undergoing RP, AA men demonstrated an overall higher likelihood of ≥pT2c with lower upstaging beyond pT2, lower likelihood of EPE and no significant difference in likelihood of SVI and LNI compared to non-AA men. These findings support select AA men to be potential candidates for PGA, such as HA. Clinical factors are predictive of higher pathological stage and adverse pathological outcomes at RP and could be considered when selecting candidates for PGA.</p>\",\"PeriodicalId\":20727,\"journal\":{\"name\":\"Prostate Cancer and Prostatic Diseases\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":5.1000,\"publicationDate\":\"2024-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Prostate Cancer and Prostatic Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41391-024-00880-6\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prostate Cancer and Prostatic Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41391-024-00880-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
重要性和目的:部分腺体消融术(PGA)作为中危前列腺癌(IR-PCa)男性患者的一种治疗方法越来越受欢迎,它可以在控制癌症的同时保留功能性结果。我们的目的是确定种族和临床特征对符合半消融(HA)PGA治疗条件的中危前列腺癌患者的分期上移(≥pT2c)风险和不良病理结果(包括精囊侵犯(SVI)、前列腺外扩展(EPE)和淋巴结侵犯(LNI))的影响:设计:回顾性分析:多中心:我们研究了1988年至2020年间在SEARCH队列中9家不同的退伍军人事务医院接受RP治疗的单侧IR-PCa患者。在调整协变量后,我们使用多变量逻辑回归分析了不同种族在临床病理特征和结局变量(≥pT2c 和 SVI、EPE 和 LNI 的几率)方面的差异:在3127名患者中,33%为接受RP手术的单侧IR-PCa非裔美国人(AA)男性。与非非裔美国人男性相比,非裔美国人更年轻(61 岁对 65 岁,P 结论:非裔美国人的年龄更小:在接受 RP 的 IR-PCa 男性患者中,与非 AA 男性患者相比,AA 男性患者≥pT2c 的可能性总体较高,pT2 以上分期较低,EPE 的可能性较低,SVI 和 LNI 的可能性无显著差异。这些发现支持选择 AA 男性作为 PGA(如 HA)的潜在候选者。临床因素可预测较高的病理分期和 RP 时的不良病理结果,因此在选择 PGA 候选者时可加以考虑。
Select black men are potential candidates for prostate hemi-ablation based on radical prostatectomy histopathology for intermediate-risk prostate cancer-a multicenter SEARCH cohort study.
Importance and objective: Partial gland ablation (PGA) is increasingly popular as a treatment for men with intermediate-risk prostate cancer (IR-PCa) to preserve functional outcomes while controlling their cancer. We aimed to determine the impact of race and clinical characteristics on the risk of upstaging (≥pT2c) and having adverse pathological outcomes including seminal vesicle invasion (SVI), extra prostatic extension (EPE) and lymph node invasion (LNI) at radical prostatectomy (RP) among men with IR disease eligible for PGA with hemi-ablation (HA).
Design: Retrospective analysis.
Setting: Multicenter.
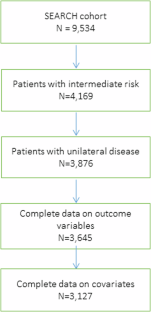
Participants and measures: We studied patients diagnosed with unilateral IR-PCa treated with RP between 1988 and 2020 at 9 different Veterans Affairs hospitals within the SEARCH cohort. We analyzed differences in clinicopathological characteristics and outcome variables (odds of ≥pT2c and SVI, EPE and LNI) by race using multivariable logistic regression after adjusting for covariates.
Results: Among 3127 patients, 33% were African American (AA) men with unilateral IR-PCa undergoing RP. Compared to non-AA men, AA individuals were younger (61 vs. 65 years, p < 0.001), presented with a higher prostate specific antigen (PSA) category (≥10 ng/ml; 34 vs. 26%, p < 0.001), and had a lower clinical stage (p < 0.001). Among the 2,798 (89.5%) with ≥pT2c stage, AA men exhibited higher ≥ pT2c rates (93 vs. 89%, p < 0.001), primarily due to increased pT2c staging (64 vs. 57%), where upstaging beyond pT2 was lower than non-AA men (29 vs. 32%). On multivariable analysis, AA men were found to have higher odds of ≥pT2c (odds ratio [OR]: 1.39 CI, 1.02-1.88, p = 0.04), lower odds of EPE (OR: 0.73 CI, 0.58-0.91, p < 0.01) and no statistically significant associations with LNI (OR: 0.79 CI, 0.42-1.46, p = 0.45) and SVI (OR: 1 CI, 0.74-1.35, p = 0.99) compared to non-AA men. On multivariable analysis, clinical features associated with higher odds of ≥pT2c were pre-operative PSA ≥ 15 (OR = 2.07, P = 0.01) and higher number of positive cores (HPC) on biopsy (OR = 1.36, P < 0.001). Similarly, PSA ≥ 15, Gleason grade ≥3 and HPC on biopsy were associated with higher odds of SVI, EPE and LNI, respectively.
Conclusions: In men with IR-PCa undergoing RP, AA men demonstrated an overall higher likelihood of ≥pT2c with lower upstaging beyond pT2, lower likelihood of EPE and no significant difference in likelihood of SVI and LNI compared to non-AA men. These findings support select AA men to be potential candidates for PGA, such as HA. Clinical factors are predictive of higher pathological stage and adverse pathological outcomes at RP and could be considered when selecting candidates for PGA.
期刊介绍:
Prostate Cancer and Prostatic Diseases covers all aspects of prostatic diseases, in particular prostate cancer, the subject of intensive basic and clinical research world-wide. The journal also reports on exciting new developments being made in diagnosis, surgery, radiotherapy, drug discovery and medical management.
Prostate Cancer and Prostatic Diseases is of interest to surgeons, oncologists and clinicians treating patients and to those involved in research into diseases of the prostate. The journal covers the three main areas - prostate cancer, male LUTS and prostatitis.
Prostate Cancer and Prostatic Diseases publishes original research articles, reviews, topical comment and critical appraisals of scientific meetings and the latest books. The journal also contains a calendar of forthcoming scientific meetings. The Editors and a distinguished Editorial Board ensure that submitted articles receive fast and efficient attention and are refereed to the highest possible scientific standard. A fast track system is available for topical articles of particular significance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


