Rezan Koçak Ulucaköy, Hakan Babaoğlu, Esra Kayacan Erdoğan, Kevser Orhan, Ebru Atalar, Serdar Can Güven, Hatice Ecem Konak, Bahar Özdemir Ulusoy, Pınar Akyüz Dağlı, Özlem Karakaş, Hakan Apaydın, Mehmet Akif Eksin, Bünyamin Polat, Serdar Esmer, İsmail Dogan, Yüksel Maraş, Ahmet Omma, Orhan Küçükşahin, Şükran Erten, Berkan Armağan
{"title":"炎症性风湿病的共病特征:分析视角","authors":"Rezan Koçak Ulucaköy, Hakan Babaoğlu, Esra Kayacan Erdoğan, Kevser Orhan, Ebru Atalar, Serdar Can Güven, Hatice Ecem Konak, Bahar Özdemir Ulusoy, Pınar Akyüz Dağlı, Özlem Karakaş, Hakan Apaydın, Mehmet Akif Eksin, Bünyamin Polat, Serdar Esmer, İsmail Dogan, Yüksel Maraş, Ahmet Omma, Orhan Küçükşahin, Şükran Erten, Berkan Armağan","doi":"10.1155/2024/3244597","DOIUrl":null,"url":null,"abstract":"<div>\n <p><i>Background</i>. Inflammatory rheumatic diseases (IRDs) are often associated with multiple comorbidities. Managing comorbidities now seen as important as management of primary IRDs. The aim of this study was to analyse the profiles and prevalence of comorbidities in patients with IRDs and also to highlight the critical need for comprehensive and routine screening for comorbidities. <i>Methods</i>. This study was a retrospective single-center study conducted between 2019 and 2023. IRDs were classified according to the following categories: rheumatoid arthritis, spondyloarthritis, connective tissue diseases, autoinflammatory diseases, Behçet’s disease, large vessel vasculitis (LVV), small vessel vasculitis (SVV), and crystal deposition diseases (CDD). The demographic characteristics and comorbidities (including hypertension, diabetes mellitus, hyperlipidemia, obesity, coronary artery disease, arrhythmia, heart failure, chronic kidney disease, asthma, osteoporosis, thyroid diseases, demyelinating diseases, depression, and malignancies) were obtained from the electronic patient files. <i>Results</i>. The study included 10 417 patients with IRDs (mean age 50.9 ± 14.5 years; 66.8% female). The five most prevalent comorbidities were hypertension (34.8%), obesity (29.1%), diabetes mellitus (14.1%), hyperlipidemia (12.1%), and osteoporosis (9.2%). The Poisson regression analysis demonstrated a significant association between the total number of comorbidities and CDD, LVV, and SVV. The most prevalent comorbidities were cardiovascular risk factors. Furthermore, the prevalence of osteoporosis was high in LVV, and the prevalence of chronic kidney disease and asthma was high in SVV. <i>Conclusion</i>. Our study not only presents observational data but also highlights the critical need for comprehensive and routine screening for comorbidities in patients with rheumatic diseases. We found that CDD followed by LVV and SVV were identified as the rheumatic conditions most associated with comorbidities, and these diseases are most commonly accompanied by cardiovascular risk factors. Additionally, our findings suggest that patients with rheumatological conditions may be underscreened, leading to potential underdiagnosis of comorbidities such as hyperlipidemia, osteoporosis, and possibly malignancies.</p>\n </div>","PeriodicalId":13782,"journal":{"name":"International Journal of Clinical Practice","volume":"2024 1","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2024-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/3244597","citationCount":"0","resultStr":"{\"title\":\"Comorbidity Profiles in Inflammatory Rheumatic Diseases: An Analytical Perspective\",\"authors\":\"Rezan Koçak Ulucaköy, Hakan Babaoğlu, Esra Kayacan Erdoğan, Kevser Orhan, Ebru Atalar, Serdar Can Güven, Hatice Ecem Konak, Bahar Özdemir Ulusoy, Pınar Akyüz Dağlı, Özlem Karakaş, Hakan Apaydın, Mehmet Akif Eksin, Bünyamin Polat, Serdar Esmer, İsmail Dogan, Yüksel Maraş, Ahmet Omma, Orhan Küçükşahin, Şükran Erten, Berkan Armağan\",\"doi\":\"10.1155/2024/3244597\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n <p><i>Background</i>. Inflammatory rheumatic diseases (IRDs) are often associated with multiple comorbidities. Managing comorbidities now seen as important as management of primary IRDs. The aim of this study was to analyse the profiles and prevalence of comorbidities in patients with IRDs and also to highlight the critical need for comprehensive and routine screening for comorbidities. <i>Methods</i>. This study was a retrospective single-center study conducted between 2019 and 2023. IRDs were classified according to the following categories: rheumatoid arthritis, spondyloarthritis, connective tissue diseases, autoinflammatory diseases, Behçet’s disease, large vessel vasculitis (LVV), small vessel vasculitis (SVV), and crystal deposition diseases (CDD). The demographic characteristics and comorbidities (including hypertension, diabetes mellitus, hyperlipidemia, obesity, coronary artery disease, arrhythmia, heart failure, chronic kidney disease, asthma, osteoporosis, thyroid diseases, demyelinating diseases, depression, and malignancies) were obtained from the electronic patient files. <i>Results</i>. The study included 10 417 patients with IRDs (mean age 50.9 ± 14.5 years; 66.8% female). The five most prevalent comorbidities were hypertension (34.8%), obesity (29.1%), diabetes mellitus (14.1%), hyperlipidemia (12.1%), and osteoporosis (9.2%). The Poisson regression analysis demonstrated a significant association between the total number of comorbidities and CDD, LVV, and SVV. The most prevalent comorbidities were cardiovascular risk factors. Furthermore, the prevalence of osteoporosis was high in LVV, and the prevalence of chronic kidney disease and asthma was high in SVV. <i>Conclusion</i>. Our study not only presents observational data but also highlights the critical need for comprehensive and routine screening for comorbidities in patients with rheumatic diseases. We found that CDD followed by LVV and SVV were identified as the rheumatic conditions most associated with comorbidities, and these diseases are most commonly accompanied by cardiovascular risk factors. Additionally, our findings suggest that patients with rheumatological conditions may be underscreened, leading to potential underdiagnosis of comorbidities such as hyperlipidemia, osteoporosis, and possibly malignancies.</p>\\n </div>\",\"PeriodicalId\":13782,\"journal\":{\"name\":\"International Journal of Clinical Practice\",\"volume\":\"2024 1\",\"pages\":\"\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/3244597\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Clinical Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1155/2024/3244597\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/3244597","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Comorbidity Profiles in Inflammatory Rheumatic Diseases: An Analytical Perspective
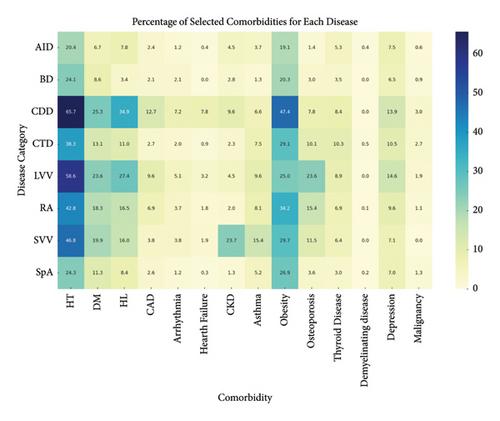
Background. Inflammatory rheumatic diseases (IRDs) are often associated with multiple comorbidities. Managing comorbidities now seen as important as management of primary IRDs. The aim of this study was to analyse the profiles and prevalence of comorbidities in patients with IRDs and also to highlight the critical need for comprehensive and routine screening for comorbidities. Methods. This study was a retrospective single-center study conducted between 2019 and 2023. IRDs were classified according to the following categories: rheumatoid arthritis, spondyloarthritis, connective tissue diseases, autoinflammatory diseases, Behçet’s disease, large vessel vasculitis (LVV), small vessel vasculitis (SVV), and crystal deposition diseases (CDD). The demographic characteristics and comorbidities (including hypertension, diabetes mellitus, hyperlipidemia, obesity, coronary artery disease, arrhythmia, heart failure, chronic kidney disease, asthma, osteoporosis, thyroid diseases, demyelinating diseases, depression, and malignancies) were obtained from the electronic patient files. Results. The study included 10 417 patients with IRDs (mean age 50.9 ± 14.5 years; 66.8% female). The five most prevalent comorbidities were hypertension (34.8%), obesity (29.1%), diabetes mellitus (14.1%), hyperlipidemia (12.1%), and osteoporosis (9.2%). The Poisson regression analysis demonstrated a significant association between the total number of comorbidities and CDD, LVV, and SVV. The most prevalent comorbidities were cardiovascular risk factors. Furthermore, the prevalence of osteoporosis was high in LVV, and the prevalence of chronic kidney disease and asthma was high in SVV. Conclusion. Our study not only presents observational data but also highlights the critical need for comprehensive and routine screening for comorbidities in patients with rheumatic diseases. We found that CDD followed by LVV and SVV were identified as the rheumatic conditions most associated with comorbidities, and these diseases are most commonly accompanied by cardiovascular risk factors. Additionally, our findings suggest that patients with rheumatological conditions may be underscreened, leading to potential underdiagnosis of comorbidities such as hyperlipidemia, osteoporosis, and possibly malignancies.
期刊介绍:
IJCP is a general medical journal. IJCP gives special priority to work that has international appeal.
IJCP publishes:
Editorials. IJCP Editorials are commissioned. [Peer reviewed at the editor''s discretion]
Perspectives. Most IJCP Perspectives are commissioned. Example. [Peer reviewed at the editor''s discretion]
Study design and interpretation. Example. [Always peer reviewed]
Original data from clinical investigations. In particular: Primary research papers from RCTs, observational studies, epidemiological studies; pre-specified sub-analyses; pooled analyses. [Always peer reviewed]
Meta-analyses. [Always peer reviewed]
Systematic reviews. From October 2009, special priority will be given to systematic reviews. [Always peer reviewed]
Non-systematic/narrative reviews. From October 2009, reviews that are not systematic will be considered only if they include a discrete Methods section that must explicitly describe the authors'' approach. Special priority will, however, be given to systematic reviews. [Always peer reviewed]
''How to…'' papers. Example. [Always peer reviewed]
Consensus statements. [Always peer reviewed] Short reports. [Always peer reviewed]
Letters. [Peer reviewed at the editor''s discretion]
International scope
IJCP publishes work from investigators globally. Around 30% of IJCP articles list an author from the UK. Around 30% of IJCP articles list an author from the USA or Canada. Around 45% of IJCP articles list an author from a European country that is not the UK. Around 15% of articles published in IJCP list an author from a country in the Asia-Pacific region.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


