{"title":"用于控制轴长缩短的创新型无线眼部调制贴片","authors":"Lin Ye, Jing Zheng","doi":"10.1002/mba2.91","DOIUrl":null,"url":null,"abstract":"<p>In a recent paper published in <i>Nature Communications</i>, Zhong et al.<span><sup>1</sup></span> described a wireless battery-free ocular modulation patch. This patch could be utilized in posterior scleral reinforcement (PSR) surgery, to correct high myopia by shortening the axial length (AXL) and reinforce the sclera to prevent myopia recurrence.</p><p>Myopia is a state of refraction in which parallel rays of light coming from infinity are brought to focus in front of the retina. The mechanism of myopia involves various signals traveling from the retina through the choroid to the sclera, eventually resulting in scleral weakening and AXL elongation. The elongation of the AXL occurs, causing light to fail to converge on the retina. This also leads to various complications arising from changes in the posterior segment structures of the eye, including posterior staphyloma and myopic maculopathy, which in turn, contributes to the continual expansion of the globe in the posterior direction.</p><p>There are many surgical options available for patients with high myopia. Myopic patients could avoid wearing glasses through corneal laser surgery and Implantable Collamer Lens surgery, which work by flattening the cornea or adding lenses to the anterior chamber to help converge light on the retina. However, these surgeries are purely optical corrections and do not address the pathological changes in the posterior segment structure in myopic eyeballs. Comparatively, traditional PSR surgery aims to strengthen the weakened posterior sclera by ocular patch. The technique was first reported by Shevelev in 1930 and was later modified by Snyder and Thompson. The primary goal of PSR surgery is to reinforce the weakened sclera, not to shorten the AXL to achieve perfect light convergence on the retina. Thus, PSR surgery is particularly essential for patients with high myopia and related complications. In light of the research background, Zhong et al. proposed the concept, that shortening AXL by a novel PSR surgery, is remarkably groundbreaking, potentially allowing for precise and personalized treatment of AXL shortening for patients with high myopia by PSR. Furthermore, traditional macular buckle is primarily used to treat macular schisis in high myopia, addressing the traction on the retina caused by posterior staphyloma in the macular area and promoting the reattachment of the macular schisis. Comparatively, this novel PSR surgery focused more specifically on the shrinkage of the sclera, further reinforcing the weakened sclera through scleral cross-linking (SCXL).</p><p>For decades, ocular patch for PSR have consisted of homologous sclera, dura mater and pericardium patches.<span><sup>2</sup></span> In recent years, nonbiological source materials have gained popularity. Researchers have proposed using various hydrogel materials were proposed for PSR, but these studies have remained limited to animal experiments.<span><sup>3, 4</sup></span> Zhong et al. developed a novel wireless battery-free ocular modulation patch, powered and controlled by an external ultrasound source. The patch consisted of piezoelectric transducers, an electrochemical micro-actuator, a drug microneedle array, μ-LEDs, a flexible circuit and biocompatible encapsulation (Figure 1). The adoption of wireless energy transmission eliminated the inaccuracies associated with traditional PSR surgery in controlling the AXL and mitigates potential hazards posed by cumbersome batteries. The novel wirelessly powering micro-actuator could trigger electrolysis process, which involved the use of microfabricated copper/gold-forked electrodes to electrolyze the aqueous solution, producing hydrogen and oxygen gas. The generation of hydrogen and oxygen gas led to mechanical deformation of the polydimethylsiloxane/polystyrene-block-polybutadiene-block-polystyrene flexible membrane. When the ocular modulation patch was placed on the rabbit eye globe, the patch applied axial pressure to the macula, thus inducing scleral shortening through mechanical action. After the micro-actuator was activated, the rabbit AXL underwent a reduction of approximately 1217 μm. In human eyes, this 1217 μm change translated to a modification of refractive power by approximately 2.5D for myopic patients. In this study, Zhong et al. solely observed the impact of the patch on axial shortening in normal rabbits. We eagerly await the assessment of the efficacy of this ocular modulation patch in addressing myopic complications like posterior staphyloma and macular schisis.</p><p>In addition, this wireless control of AXL shortening was coupled with another function: SCXL. The integration of axial shortening with SCXL theoretically stabilized the shortened AXL, prolonging the effectiveness of treatment and aiding in reducing the recurrence of high myopia. Previously, development of SCXL lagged far behind corneal cross-linking, with SCXL only being investigated in animal experiments. This was primarily due to the anatomical location of the posterior sclera, which made effective delivery of photosensitizers and illumination challenging. Most articles describe using 360-degree conjunctival peritomy and muscle traction to expose the equatorial-posterior sclera. Riboflavin is then applied to the exposed area,<span><sup>5</sup></span> with some articles mentioning the use of iontophoresis technology to enhance absorption. Since it is difficult to expose the posterior sclera, most SCXL studies targeted the equatorial region of the sclera, which was not the most weakened position of the sclera in patients with high myopia. In this study, Zhong et al. combined SXL with PSR surgery to more directly target the posterior sclera. Notably, this ocular patch marked the first instance of delivering riboflavin to the posterior sclera through a microneedle array (polyvinylpyrrolidone and riboflavin), overcoming previous challenges in drug delivery for SCXL. Riboflavin is commonly combined with blue light in SCXL to avoid the potential side effects of ultraviolet light. The blue μ-LED (443 nm) has already been applied to the wireless ocular modulation patch and could be activated using ultrasound. Furthermore, the combination of PSR and SCXL surgery within a single procedure represented an exceptionally innovative surgical concept. The emergence of this combined surgery could significantly advance the application of composite and personalized scleral reinforcement in myopia control. Measurements of rigidity of the sclera revealed that, SCXL increased the scleral Young's modulus by approximately 151.25% at Day 7 and by 387% at Day 22. Collagen fibers exhibited a more tightly arranged structure after SCXL. Analysis of porosity from H&E-stained sections showed a 58.33% decrease in porosity in the SCXL group compared to the control group. A further comparison of the therapeutic efficacy of varying intensities of light exposure and different concentrations of riboflavin delivery might be a future research direction. As Zhang et al. noted, the study had limitations due to its small sample size and the relatively short 22-day postsurgery observation period. Potential postoperative complications, such as ocular hypertension, conjunctival tissue edema, and vitreous hemorrhage, should be considered in the future. Furthermore, it would be interesting to consider the changes in choroidal thickness and blood flow postsurgery, as choroidal blood flow is found to be closely related to the development of high myopia.</p><p>In summary, Zhong et al. proposed a scleral reinforcement patch for treating high myopia, which combined the functions of axial shortening and SCXL in a wireless battery-free manner. While there were already various methods for treating myopia, achieving a balance between efficacy and safety is often crucial. This article primarily introduced an innovative concept for treating high myopia, but many issues remained unresolved. Further research is needed for long-term monitoring of axial shortening efficacy and safety. The size of rabbit eyes differs from human eyes, so it is uncertain whether the wireless ocular patch needs to be redesigned for human use. Additionally, we anticipate seeing the effectiveness of this new patch applied to myopic sclera, considering the significant differences between myopic sclera and normal sclera.</p><p><b>Lin Ye</b>: Conceptualization; investigation; visualization; writing—original draft. <b>Jing Zheng</b>: Conceptualization; project administration; supervision; visualization; writing—review & editing. All authors have read and approved the final manuscript.</p><p>The authors declare no conflict of interest.</p><p>Not applicable.</p>","PeriodicalId":100901,"journal":{"name":"MedComm – Biomaterials and Applications","volume":"3 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mba2.91","citationCount":"0","resultStr":"{\"title\":\"Innovative wireless ocular modulation patch for controlled axial length shortening\",\"authors\":\"Lin Ye, Jing Zheng\",\"doi\":\"10.1002/mba2.91\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In a recent paper published in <i>Nature Communications</i>, Zhong et al.<span><sup>1</sup></span> described a wireless battery-free ocular modulation patch. This patch could be utilized in posterior scleral reinforcement (PSR) surgery, to correct high myopia by shortening the axial length (AXL) and reinforce the sclera to prevent myopia recurrence.</p><p>Myopia is a state of refraction in which parallel rays of light coming from infinity are brought to focus in front of the retina. The mechanism of myopia involves various signals traveling from the retina through the choroid to the sclera, eventually resulting in scleral weakening and AXL elongation. The elongation of the AXL occurs, causing light to fail to converge on the retina. This also leads to various complications arising from changes in the posterior segment structures of the eye, including posterior staphyloma and myopic maculopathy, which in turn, contributes to the continual expansion of the globe in the posterior direction.</p><p>There are many surgical options available for patients with high myopia. Myopic patients could avoid wearing glasses through corneal laser surgery and Implantable Collamer Lens surgery, which work by flattening the cornea or adding lenses to the anterior chamber to help converge light on the retina. However, these surgeries are purely optical corrections and do not address the pathological changes in the posterior segment structure in myopic eyeballs. Comparatively, traditional PSR surgery aims to strengthen the weakened posterior sclera by ocular patch. The technique was first reported by Shevelev in 1930 and was later modified by Snyder and Thompson. The primary goal of PSR surgery is to reinforce the weakened sclera, not to shorten the AXL to achieve perfect light convergence on the retina. Thus, PSR surgery is particularly essential for patients with high myopia and related complications. In light of the research background, Zhong et al. proposed the concept, that shortening AXL by a novel PSR surgery, is remarkably groundbreaking, potentially allowing for precise and personalized treatment of AXL shortening for patients with high myopia by PSR. Furthermore, traditional macular buckle is primarily used to treat macular schisis in high myopia, addressing the traction on the retina caused by posterior staphyloma in the macular area and promoting the reattachment of the macular schisis. Comparatively, this novel PSR surgery focused more specifically on the shrinkage of the sclera, further reinforcing the weakened sclera through scleral cross-linking (SCXL).</p><p>For decades, ocular patch for PSR have consisted of homologous sclera, dura mater and pericardium patches.<span><sup>2</sup></span> In recent years, nonbiological source materials have gained popularity. Researchers have proposed using various hydrogel materials were proposed for PSR, but these studies have remained limited to animal experiments.<span><sup>3, 4</sup></span> Zhong et al. developed a novel wireless battery-free ocular modulation patch, powered and controlled by an external ultrasound source. The patch consisted of piezoelectric transducers, an electrochemical micro-actuator, a drug microneedle array, μ-LEDs, a flexible circuit and biocompatible encapsulation (Figure 1). The adoption of wireless energy transmission eliminated the inaccuracies associated with traditional PSR surgery in controlling the AXL and mitigates potential hazards posed by cumbersome batteries. The novel wirelessly powering micro-actuator could trigger electrolysis process, which involved the use of microfabricated copper/gold-forked electrodes to electrolyze the aqueous solution, producing hydrogen and oxygen gas. The generation of hydrogen and oxygen gas led to mechanical deformation of the polydimethylsiloxane/polystyrene-block-polybutadiene-block-polystyrene flexible membrane. When the ocular modulation patch was placed on the rabbit eye globe, the patch applied axial pressure to the macula, thus inducing scleral shortening through mechanical action. After the micro-actuator was activated, the rabbit AXL underwent a reduction of approximately 1217 μm. In human eyes, this 1217 μm change translated to a modification of refractive power by approximately 2.5D for myopic patients. In this study, Zhong et al. solely observed the impact of the patch on axial shortening in normal rabbits. We eagerly await the assessment of the efficacy of this ocular modulation patch in addressing myopic complications like posterior staphyloma and macular schisis.</p><p>In addition, this wireless control of AXL shortening was coupled with another function: SCXL. The integration of axial shortening with SCXL theoretically stabilized the shortened AXL, prolonging the effectiveness of treatment and aiding in reducing the recurrence of high myopia. Previously, development of SCXL lagged far behind corneal cross-linking, with SCXL only being investigated in animal experiments. This was primarily due to the anatomical location of the posterior sclera, which made effective delivery of photosensitizers and illumination challenging. Most articles describe using 360-degree conjunctival peritomy and muscle traction to expose the equatorial-posterior sclera. Riboflavin is then applied to the exposed area,<span><sup>5</sup></span> with some articles mentioning the use of iontophoresis technology to enhance absorption. Since it is difficult to expose the posterior sclera, most SCXL studies targeted the equatorial region of the sclera, which was not the most weakened position of the sclera in patients with high myopia. In this study, Zhong et al. combined SXL with PSR surgery to more directly target the posterior sclera. Notably, this ocular patch marked the first instance of delivering riboflavin to the posterior sclera through a microneedle array (polyvinylpyrrolidone and riboflavin), overcoming previous challenges in drug delivery for SCXL. Riboflavin is commonly combined with blue light in SCXL to avoid the potential side effects of ultraviolet light. The blue μ-LED (443 nm) has already been applied to the wireless ocular modulation patch and could be activated using ultrasound. Furthermore, the combination of PSR and SCXL surgery within a single procedure represented an exceptionally innovative surgical concept. The emergence of this combined surgery could significantly advance the application of composite and personalized scleral reinforcement in myopia control. Measurements of rigidity of the sclera revealed that, SCXL increased the scleral Young's modulus by approximately 151.25% at Day 7 and by 387% at Day 22. Collagen fibers exhibited a more tightly arranged structure after SCXL. Analysis of porosity from H&E-stained sections showed a 58.33% decrease in porosity in the SCXL group compared to the control group. A further comparison of the therapeutic efficacy of varying intensities of light exposure and different concentrations of riboflavin delivery might be a future research direction. As Zhang et al. noted, the study had limitations due to its small sample size and the relatively short 22-day postsurgery observation period. Potential postoperative complications, such as ocular hypertension, conjunctival tissue edema, and vitreous hemorrhage, should be considered in the future. Furthermore, it would be interesting to consider the changes in choroidal thickness and blood flow postsurgery, as choroidal blood flow is found to be closely related to the development of high myopia.</p><p>In summary, Zhong et al. proposed a scleral reinforcement patch for treating high myopia, which combined the functions of axial shortening and SCXL in a wireless battery-free manner. While there were already various methods for treating myopia, achieving a balance between efficacy and safety is often crucial. This article primarily introduced an innovative concept for treating high myopia, but many issues remained unresolved. Further research is needed for long-term monitoring of axial shortening efficacy and safety. The size of rabbit eyes differs from human eyes, so it is uncertain whether the wireless ocular patch needs to be redesigned for human use. Additionally, we anticipate seeing the effectiveness of this new patch applied to myopic sclera, considering the significant differences between myopic sclera and normal sclera.</p><p><b>Lin Ye</b>: Conceptualization; investigation; visualization; writing—original draft. <b>Jing Zheng</b>: Conceptualization; project administration; supervision; visualization; writing—review & editing. All authors have read and approved the final manuscript.</p><p>The authors declare no conflict of interest.</p><p>Not applicable.</p>\",\"PeriodicalId\":100901,\"journal\":{\"name\":\"MedComm – Biomaterials and Applications\",\"volume\":\"3 3\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mba2.91\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"MedComm – Biomaterials and Applications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/mba2.91\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"MedComm – Biomaterials and Applications","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/mba2.91","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
在最近发表于《自然-通讯》(Nature Communications)的一篇论文中,Zhong 等人1 描述了一种无需电池的无线眼部调制贴片。近视是一种屈光状态,即来自无限远处的平行光线在视网膜前聚焦。近视的发生机制包括各种信号从视网膜通过脉络膜传到巩膜,最终导致巩膜变薄和 AXL 拉长。AXL 的拉长导致光线无法汇聚到视网膜上。这也会导致眼球后段结构发生变化,引起各种并发症,包括后葡萄肿和近视性黄斑病变,进而导致眼球向后方持续扩张。近视患者可以通过角膜激光手术和植入式角膜塑形镜手术来避免戴眼镜,这些手术通过压平角膜或在前房添加镜片来帮助光线汇聚到视网膜上。然而,这些手术只是单纯的光学矫正,并不能解决近视眼后节结构的病理变化。相比之下,传统的 PSR 手术旨在通过眼球修补术来加固薄弱的后巩膜。该技术由 Shevelev 于 1930 年首次报道,后经 Snyder 和 Thompson 改良。PSR 手术的主要目的是加固薄弱的巩膜,而不是缩短 AXL 以实现视网膜上完美的光线会聚。因此,PSR 手术对高度近视及相关并发症患者尤为重要。鉴于上述研究背景,钟南山等人提出了一个概念,即通过一种新型的 PSR 手术缩短 AXL 具有显著的开创性,有可能通过 PSR 为高度近视患者提供精确和个性化的 AXL 缩短治疗。此外,传统的黄斑扣带术主要用于治疗高度近视的黄斑裂孔,解决黄斑区后葡萄膜瘤对视网膜的牵引,促进黄斑裂孔的重新附着。几十年来,用于 PSR 的眼部补片一直由同种巩膜、硬脑膜和心包补片组成。研究人员提出了使用各种水凝胶材料进行 PSR 的建议,但这些研究仍局限于动物实验。该贴片由压电传感器、电化学微执行器、药物微针阵列、μ-LED、柔性电路和生物兼容封装组成(图 1)。采用无线能量传输消除了传统 PSR 手术在控制 AXL 方面的不准确性,并减轻了笨重电池带来的潜在危害。这种新型无线供电微型执行器可触发电解过程,利用微加工铜/金叉电极电解水溶液,产生氢气和氧气。氢气和氧气的产生导致聚二甲基硅氧烷/聚苯乙烯-块状-聚丁二烯-块状-聚苯乙烯柔性膜发生机械变形。当眼球调制贴片贴在兔眼球上时,贴片对黄斑施加轴向压力,从而通过机械作用诱导巩膜缩短。微型致动器启动后,兔子的 AXL 缩短了约 1217 μm。在人眼中,这 1217 μm 的变化意味着近视患者的屈光力降低了约 2.5D。在这项研究中,Zhong 等人只观察了眼罩对正常兔子轴向缩短的影响。我们热切期待着对这种眼部调节贴片在解决近视并发症(如后葡萄膜瘤和黄斑裂孔)方面的功效进行评估:SCXL。将轴向缩短与 SCXL 结合在一起,理论上可以稳定缩短的 AXL,延长治疗效果,并有助于减少高度近视的复发。在此之前,SCXL 的发展远远落后于角膜交联术,SCXL 仅在动物实验中进行研究。
Innovative wireless ocular modulation patch for controlled axial length shortening
In a recent paper published in Nature Communications, Zhong et al.1 described a wireless battery-free ocular modulation patch. This patch could be utilized in posterior scleral reinforcement (PSR) surgery, to correct high myopia by shortening the axial length (AXL) and reinforce the sclera to prevent myopia recurrence.
Myopia is a state of refraction in which parallel rays of light coming from infinity are brought to focus in front of the retina. The mechanism of myopia involves various signals traveling from the retina through the choroid to the sclera, eventually resulting in scleral weakening and AXL elongation. The elongation of the AXL occurs, causing light to fail to converge on the retina. This also leads to various complications arising from changes in the posterior segment structures of the eye, including posterior staphyloma and myopic maculopathy, which in turn, contributes to the continual expansion of the globe in the posterior direction.
There are many surgical options available for patients with high myopia. Myopic patients could avoid wearing glasses through corneal laser surgery and Implantable Collamer Lens surgery, which work by flattening the cornea or adding lenses to the anterior chamber to help converge light on the retina. However, these surgeries are purely optical corrections and do not address the pathological changes in the posterior segment structure in myopic eyeballs. Comparatively, traditional PSR surgery aims to strengthen the weakened posterior sclera by ocular patch. The technique was first reported by Shevelev in 1930 and was later modified by Snyder and Thompson. The primary goal of PSR surgery is to reinforce the weakened sclera, not to shorten the AXL to achieve perfect light convergence on the retina. Thus, PSR surgery is particularly essential for patients with high myopia and related complications. In light of the research background, Zhong et al. proposed the concept, that shortening AXL by a novel PSR surgery, is remarkably groundbreaking, potentially allowing for precise and personalized treatment of AXL shortening for patients with high myopia by PSR. Furthermore, traditional macular buckle is primarily used to treat macular schisis in high myopia, addressing the traction on the retina caused by posterior staphyloma in the macular area and promoting the reattachment of the macular schisis. Comparatively, this novel PSR surgery focused more specifically on the shrinkage of the sclera, further reinforcing the weakened sclera through scleral cross-linking (SCXL).
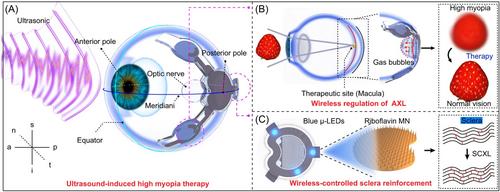
For decades, ocular patch for PSR have consisted of homologous sclera, dura mater and pericardium patches.2 In recent years, nonbiological source materials have gained popularity. Researchers have proposed using various hydrogel materials were proposed for PSR, but these studies have remained limited to animal experiments.3, 4 Zhong et al. developed a novel wireless battery-free ocular modulation patch, powered and controlled by an external ultrasound source. The patch consisted of piezoelectric transducers, an electrochemical micro-actuator, a drug microneedle array, μ-LEDs, a flexible circuit and biocompatible encapsulation (Figure 1). The adoption of wireless energy transmission eliminated the inaccuracies associated with traditional PSR surgery in controlling the AXL and mitigates potential hazards posed by cumbersome batteries. The novel wirelessly powering micro-actuator could trigger electrolysis process, which involved the use of microfabricated copper/gold-forked electrodes to electrolyze the aqueous solution, producing hydrogen and oxygen gas. The generation of hydrogen and oxygen gas led to mechanical deformation of the polydimethylsiloxane/polystyrene-block-polybutadiene-block-polystyrene flexible membrane. When the ocular modulation patch was placed on the rabbit eye globe, the patch applied axial pressure to the macula, thus inducing scleral shortening through mechanical action. After the micro-actuator was activated, the rabbit AXL underwent a reduction of approximately 1217 μm. In human eyes, this 1217 μm change translated to a modification of refractive power by approximately 2.5D for myopic patients. In this study, Zhong et al. solely observed the impact of the patch on axial shortening in normal rabbits. We eagerly await the assessment of the efficacy of this ocular modulation patch in addressing myopic complications like posterior staphyloma and macular schisis.
In addition, this wireless control of AXL shortening was coupled with another function: SCXL. The integration of axial shortening with SCXL theoretically stabilized the shortened AXL, prolonging the effectiveness of treatment and aiding in reducing the recurrence of high myopia. Previously, development of SCXL lagged far behind corneal cross-linking, with SCXL only being investigated in animal experiments. This was primarily due to the anatomical location of the posterior sclera, which made effective delivery of photosensitizers and illumination challenging. Most articles describe using 360-degree conjunctival peritomy and muscle traction to expose the equatorial-posterior sclera. Riboflavin is then applied to the exposed area,5 with some articles mentioning the use of iontophoresis technology to enhance absorption. Since it is difficult to expose the posterior sclera, most SCXL studies targeted the equatorial region of the sclera, which was not the most weakened position of the sclera in patients with high myopia. In this study, Zhong et al. combined SXL with PSR surgery to more directly target the posterior sclera. Notably, this ocular patch marked the first instance of delivering riboflavin to the posterior sclera through a microneedle array (polyvinylpyrrolidone and riboflavin), overcoming previous challenges in drug delivery for SCXL. Riboflavin is commonly combined with blue light in SCXL to avoid the potential side effects of ultraviolet light. The blue μ-LED (443 nm) has already been applied to the wireless ocular modulation patch and could be activated using ultrasound. Furthermore, the combination of PSR and SCXL surgery within a single procedure represented an exceptionally innovative surgical concept. The emergence of this combined surgery could significantly advance the application of composite and personalized scleral reinforcement in myopia control. Measurements of rigidity of the sclera revealed that, SCXL increased the scleral Young's modulus by approximately 151.25% at Day 7 and by 387% at Day 22. Collagen fibers exhibited a more tightly arranged structure after SCXL. Analysis of porosity from H&E-stained sections showed a 58.33% decrease in porosity in the SCXL group compared to the control group. A further comparison of the therapeutic efficacy of varying intensities of light exposure and different concentrations of riboflavin delivery might be a future research direction. As Zhang et al. noted, the study had limitations due to its small sample size and the relatively short 22-day postsurgery observation period. Potential postoperative complications, such as ocular hypertension, conjunctival tissue edema, and vitreous hemorrhage, should be considered in the future. Furthermore, it would be interesting to consider the changes in choroidal thickness and blood flow postsurgery, as choroidal blood flow is found to be closely related to the development of high myopia.
In summary, Zhong et al. proposed a scleral reinforcement patch for treating high myopia, which combined the functions of axial shortening and SCXL in a wireless battery-free manner. While there were already various methods for treating myopia, achieving a balance between efficacy and safety is often crucial. This article primarily introduced an innovative concept for treating high myopia, but many issues remained unresolved. Further research is needed for long-term monitoring of axial shortening efficacy and safety. The size of rabbit eyes differs from human eyes, so it is uncertain whether the wireless ocular patch needs to be redesigned for human use. Additionally, we anticipate seeing the effectiveness of this new patch applied to myopic sclera, considering the significant differences between myopic sclera and normal sclera.
Lin Ye: Conceptualization; investigation; visualization; writing—original draft. Jing Zheng: Conceptualization; project administration; supervision; visualization; writing—review & editing. All authors have read and approved the final manuscript.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


