Anne K Ellis, Victoria Cook, Paul K Keith, Sean R Mace, William Moote, Andrew O'Keefe, Jaclyn Quirt, Lana Rosenfield, Peter Small, Wade Watson
{"title":"加拿大过敏性鼻炎重点实践参数。","authors":"Anne K Ellis, Victoria Cook, Paul K Keith, Sean R Mace, William Moote, Andrew O'Keefe, Jaclyn Quirt, Lana Rosenfield, Peter Small, Wade Watson","doi":"10.1186/s13223-024-00899-3","DOIUrl":null,"url":null,"abstract":"<p><p>Allergic rhinitis (AR) is a prevalent disease in Canada that affects both children and adults. Several guidelines for the management of AR have been published by professional allergy societies worldwide. However, there are regional differences in the clinical management of AR, and regulatory approval of some AR pharmacotherapies varies among countries. Thus, six research questions specific to the treatment of AR in Canada were identified for this focused practice parameter. Reviews of the literature published since 2016 were conducted to obtain evidence-based support for the responses of the Work Group to each research question. In response to research question 1 \"In patients with symptoms indicative of AR, is serum-specific IgE sufficient to identify candidates for immunotherapy or is a skin prick test mandatory?\" the Work Group concluded that either sIgE testing or skin prick test are acceptable for diagnosing AR and guiding immunotherapy. In response to research question 2 \"When taking into account the preferences of the patient and the prescriber (stakeholder engagement) should second-generation oral antihistamine (OAH) or intranasal corticosteroid (INCS) be first line?\" the Work Group concluded that existing guidelines generally agree on the use of INCS as a first-line therapy used for AR, however, patient and provider preferences and considerations can easily shift the first choice to a second-generation OAH. In response to research question 3 \"Is a combination intranasal antihistamine (INAH)/INCS formulation superior to INCS plus OAH? Do they become equivalent after prolonged use?\" the Work Group concluded that that the combination INAH/INCS is superior to an INCS plus OAH. However, there was insufficient evidence to answer the second question. In response to research question 4 \"Do leukotriene receptor antagonists (LTRA) have a greater benefit than OAH in AR for some symptoms to justify a therapeutic trial in those who cannot tolerate INCS?\" the Work Group concluded that LTRAs have inferior, or at best equivalent, daytime or overall symptom control compared with OAH, but LTRAs may improve nighttime symptom control and provide benefits in patients with AR and concomitant asthma. In response to research question 5 \"Should sublingual immunotherapy (SLIT) tablets be considered first-line immunotherapeutic options over subcutaneous immunotherapy (SCIT) based on the evidence of efficacy?\" the Work Group concluded that the choice of SLIT or SCIT cannot be made on efficacy alone, and differences in other factors outweigh any differences in efficacy. In response to research question 6 \"Based on efficacy data, should ALL patients seen by an allergist be offered SLIT or SCIT as a treatment option?\" the Work Group concluded that the efficacy data suggests that SLIT or SCIT should be used broadly in patients with AR, but other clinical concerns also need to be taken into consideration.</p>","PeriodicalId":51302,"journal":{"name":"Allergy Asthma and Clinical Immunology","volume":"20 1","pages":"45"},"PeriodicalIF":2.4000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11311964/pdf/","citationCount":"0","resultStr":"{\"title\":\"Focused allergic rhinitis practice parameter for Canada.\",\"authors\":\"Anne K Ellis, Victoria Cook, Paul K Keith, Sean R Mace, William Moote, Andrew O'Keefe, Jaclyn Quirt, Lana Rosenfield, Peter Small, Wade Watson\",\"doi\":\"10.1186/s13223-024-00899-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Allergic rhinitis (AR) is a prevalent disease in Canada that affects both children and adults. Several guidelines for the management of AR have been published by professional allergy societies worldwide. However, there are regional differences in the clinical management of AR, and regulatory approval of some AR pharmacotherapies varies among countries. Thus, six research questions specific to the treatment of AR in Canada were identified for this focused practice parameter. Reviews of the literature published since 2016 were conducted to obtain evidence-based support for the responses of the Work Group to each research question. In response to research question 1 \\\"In patients with symptoms indicative of AR, is serum-specific IgE sufficient to identify candidates for immunotherapy or is a skin prick test mandatory?\\\" the Work Group concluded that either sIgE testing or skin prick test are acceptable for diagnosing AR and guiding immunotherapy. In response to research question 2 \\\"When taking into account the preferences of the patient and the prescriber (stakeholder engagement) should second-generation oral antihistamine (OAH) or intranasal corticosteroid (INCS) be first line?\\\" the Work Group concluded that existing guidelines generally agree on the use of INCS as a first-line therapy used for AR, however, patient and provider preferences and considerations can easily shift the first choice to a second-generation OAH. In response to research question 3 \\\"Is a combination intranasal antihistamine (INAH)/INCS formulation superior to INCS plus OAH? Do they become equivalent after prolonged use?\\\" the Work Group concluded that that the combination INAH/INCS is superior to an INCS plus OAH. However, there was insufficient evidence to answer the second question. In response to research question 4 \\\"Do leukotriene receptor antagonists (LTRA) have a greater benefit than OAH in AR for some symptoms to justify a therapeutic trial in those who cannot tolerate INCS?\\\" the Work Group concluded that LTRAs have inferior, or at best equivalent, daytime or overall symptom control compared with OAH, but LTRAs may improve nighttime symptom control and provide benefits in patients with AR and concomitant asthma. In response to research question 5 \\\"Should sublingual immunotherapy (SLIT) tablets be considered first-line immunotherapeutic options over subcutaneous immunotherapy (SCIT) based on the evidence of efficacy?\\\" the Work Group concluded that the choice of SLIT or SCIT cannot be made on efficacy alone, and differences in other factors outweigh any differences in efficacy. In response to research question 6 \\\"Based on efficacy data, should ALL patients seen by an allergist be offered SLIT or SCIT as a treatment option?\\\" the Work Group concluded that the efficacy data suggests that SLIT or SCIT should be used broadly in patients with AR, but other clinical concerns also need to be taken into consideration.</p>\",\"PeriodicalId\":51302,\"journal\":{\"name\":\"Allergy Asthma and Clinical Immunology\",\"volume\":\"20 1\",\"pages\":\"45\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11311964/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Allergy Asthma and Clinical Immunology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13223-024-00899-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy Asthma and Clinical Immunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13223-024-00899-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
摘要
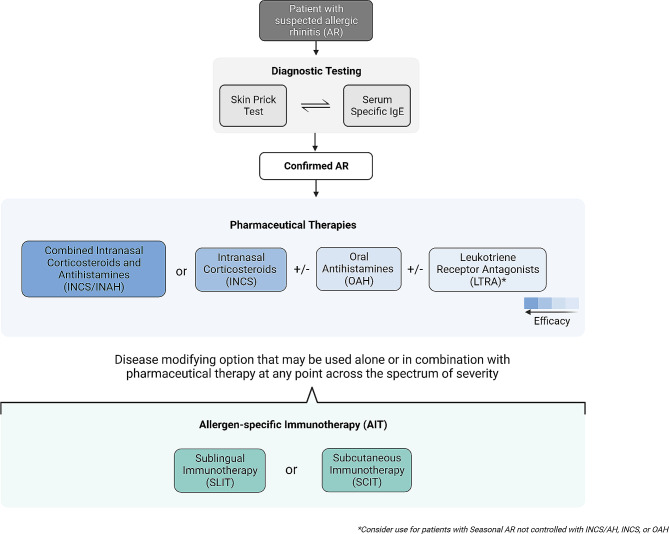
过敏性鼻炎(AR)是加拿大的一种流行病,对儿童和成年人都有影响。世界各地的专业过敏学会已发布了多份过敏性鼻炎治疗指南。然而,AR 的临床管理存在地区差异,而且各国对某些 AR 药物疗法的监管审批也不尽相同。因此,本重点实践参数确定了针对加拿大 AR 治疗的六个研究问题。我们对 2016 年以来发表的文献进行了回顾,以便为工作组对每个研究问题的答复获取循证支持。在回答研究问题 1 "对于有 AR 症状指征的患者,血清特异性 IgE 是否足以确定免疫疗法的候选者,还是必须进行皮肤点刺试验?"时,工作组得出结论认为,血清特异性 IgE 检测或皮肤点刺试验均可用于诊断 AR 和指导免疫疗法。针对研究问题 2 "考虑到患者和开处方者(利益相关者参与)的偏好,第一线疗法应该是第二代口服抗组胺药(OAH)还是鼻内皮质激素(INCS)?"工作组得出结论,现有指南普遍认为 INCS 是 AR 的第一线疗法,但患者和提供者的偏好和考虑因素很容易将第一选择转移到第二代 OAH。针对研究问题 3 "鼻内抗组胺剂 (INAH)/INCS 组合配方是否优于 INCS 加 OAH?长期使用后两者是否具有同等疗效?"工作组得出结论认为,INAH/INCS 复方制剂优于 INCS 加 OAH。但是,没有足够的证据来回答第二个问题。针对研究问题 4 "白三烯受体拮抗剂(LTRA)对 AR 的某些症状是否比 OAH 更有益,从而有理由对那些不能耐受 INCS 的患者进行治疗试验?"工作小组得出结论,与 OAH 相比,LTRA 的日间或总体症状控制效果较差,或最多与 OAH 相当,但 LTRA 可改善夜间症状控制,并为 AR 和合并哮喘的患者带来益处。在回答研究问题 5 "根据疗效证据,舌下免疫疗法(SLIT)片剂是否应被视为优于皮下免疫疗法(SCIT)的一线免疫疗法选择?"时,工作组得出结论认为,不能仅根据疗效来选择舌下免疫疗法或皮下免疫疗法,其他因素的差异大于疗效上的差异。针对研究问题 6 "根据疗效数据,过敏专科医生接诊的所有患者是否都应选择 SLIT 或 SCIT 作为治疗方案?",工作小组得出结论:疗效数据表明,SLIT 或 SCIT 应广泛用于 AR 患者,但也需要考虑其他临床问题。
Focused allergic rhinitis practice parameter for Canada.
Allergic rhinitis (AR) is a prevalent disease in Canada that affects both children and adults. Several guidelines for the management of AR have been published by professional allergy societies worldwide. However, there are regional differences in the clinical management of AR, and regulatory approval of some AR pharmacotherapies varies among countries. Thus, six research questions specific to the treatment of AR in Canada were identified for this focused practice parameter. Reviews of the literature published since 2016 were conducted to obtain evidence-based support for the responses of the Work Group to each research question. In response to research question 1 "In patients with symptoms indicative of AR, is serum-specific IgE sufficient to identify candidates for immunotherapy or is a skin prick test mandatory?" the Work Group concluded that either sIgE testing or skin prick test are acceptable for diagnosing AR and guiding immunotherapy. In response to research question 2 "When taking into account the preferences of the patient and the prescriber (stakeholder engagement) should second-generation oral antihistamine (OAH) or intranasal corticosteroid (INCS) be first line?" the Work Group concluded that existing guidelines generally agree on the use of INCS as a first-line therapy used for AR, however, patient and provider preferences and considerations can easily shift the first choice to a second-generation OAH. In response to research question 3 "Is a combination intranasal antihistamine (INAH)/INCS formulation superior to INCS plus OAH? Do they become equivalent after prolonged use?" the Work Group concluded that that the combination INAH/INCS is superior to an INCS plus OAH. However, there was insufficient evidence to answer the second question. In response to research question 4 "Do leukotriene receptor antagonists (LTRA) have a greater benefit than OAH in AR for some symptoms to justify a therapeutic trial in those who cannot tolerate INCS?" the Work Group concluded that LTRAs have inferior, or at best equivalent, daytime or overall symptom control compared with OAH, but LTRAs may improve nighttime symptom control and provide benefits in patients with AR and concomitant asthma. In response to research question 5 "Should sublingual immunotherapy (SLIT) tablets be considered first-line immunotherapeutic options over subcutaneous immunotherapy (SCIT) based on the evidence of efficacy?" the Work Group concluded that the choice of SLIT or SCIT cannot be made on efficacy alone, and differences in other factors outweigh any differences in efficacy. In response to research question 6 "Based on efficacy data, should ALL patients seen by an allergist be offered SLIT or SCIT as a treatment option?" the Work Group concluded that the efficacy data suggests that SLIT or SCIT should be used broadly in patients with AR, but other clinical concerns also need to be taken into consideration.
期刊介绍:
Allergy, Asthma & Clinical Immunology (AACI), the official journal of the Canadian Society of Allergy and Clinical Immunology (CSACI), is an open access journal that encompasses all aspects of diagnosis, epidemiology, prevention and treatment of allergic and immunologic disease.
By offering a high-visibility forum for new insights and discussions, AACI provides a platform for the dissemination of allergy and clinical immunology research and reviews amongst allergists, pulmonologists, immunologists and other physicians, healthcare workers, medical students and the public worldwide.
AACI reports on basic research and clinically applied studies in the following areas and other related topics: asthma and occupational lung disease, rhinoconjunctivitis and rhinosinusitis, drug hypersensitivity, allergic skin diseases, urticaria and angioedema, venom hypersensitivity, anaphylaxis and food allergy, immunotherapy, immune modulators and biologics, immune deficiency and autoimmunity, T cell and B cell functions, regulatory T cells, natural killer cells, mast cell and eosinophil functions, complement abnormalities.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


