Morgan E. Cooley MD, Rose A. Maxwell PhD, MBA, Rebecca Miller BS, Samantha L. Wiegand MD, David S. Mckenna MD
{"title":"第三孕期超声波诊断妊娠年龄偏大与剖宫产风险。","authors":"Morgan E. Cooley MD, Rose A. Maxwell PhD, MBA, Rebecca Miller BS, Samantha L. Wiegand MD, David S. Mckenna MD","doi":"10.1002/jum.16539","DOIUrl":null,"url":null,"abstract":"<div>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>Determine if knowledge of a third-trimester ultrasound diagnosis of large for gestational age (LGA) independently increases the risk of cesarean delivery (CD).</p>\n </section>\n \n <section>\n \n <h3> Study Design</h3>\n \n <p>Historical cohort comparing CD rate among patients diagnosed with an LGA fetus on a clinically indicated ultrasound from January 2017 to July 2021 with those without an LGA diagnosis at 34 weeks or later. LGA was defined as an ultrasound-estimated fetal weight greater than or equal to the 90th percentile for the gestational age. Univariate analysis was performed to identify significant confounding variables and was utilized as covariates for binary regression with CD rate as the primary outcome, and adjusted odds ratios (AOR) with 95% confidence intervals (CI) were calculated. Nulliparous term singleton vertex (NTSV) and multiparous CD rates were also compared.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>There were 447 patients diagnosed with an LGA fetus and 1971 patients without an LGA diagnosis on third-trimester ultrasound. The positive predictive value of LGA diagnosis was 50.1% and the false positive rate was 10.6%. Patients with a diagnosis of LGA had higher AOR of CD (OR 2.11, 95% CI 1.56-2.83), and higher AOR of NTSV CD (OR 1.88, 95% CI 1.14-3.13) compared with those without an LGA diagnosis. There was no difference in the rates of non-medically indicated CD, multiparous primary CD, and attempted and successful TOLAC.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Our results suggest third-trimester ultrasound diagnosis of LGA independently increases odds of CD, specifically among nulliparous patients, and the potential bias may be one factor contributing to excessive CDs and NTSV CDs.</p>\n </section>\n </div>","PeriodicalId":17563,"journal":{"name":"Journal of Ultrasound in Medicine","volume":"43 11","pages":"2109-2117"},"PeriodicalIF":2.1000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jum.16539","citationCount":"0","resultStr":"{\"title\":\"Third-Trimester Ultrasound Diagnosis of Large for Gestational Age and Risk of Cesarean Delivery\",\"authors\":\"Morgan E. Cooley MD, Rose A. Maxwell PhD, MBA, Rebecca Miller BS, Samantha L. Wiegand MD, David S. Mckenna MD\",\"doi\":\"10.1002/jum.16539\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>Determine if knowledge of a third-trimester ultrasound diagnosis of large for gestational age (LGA) independently increases the risk of cesarean delivery (CD).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Study Design</h3>\\n \\n <p>Historical cohort comparing CD rate among patients diagnosed with an LGA fetus on a clinically indicated ultrasound from January 2017 to July 2021 with those without an LGA diagnosis at 34 weeks or later. LGA was defined as an ultrasound-estimated fetal weight greater than or equal to the 90th percentile for the gestational age. Univariate analysis was performed to identify significant confounding variables and was utilized as covariates for binary regression with CD rate as the primary outcome, and adjusted odds ratios (AOR) with 95% confidence intervals (CI) were calculated. Nulliparous term singleton vertex (NTSV) and multiparous CD rates were also compared.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>There were 447 patients diagnosed with an LGA fetus and 1971 patients without an LGA diagnosis on third-trimester ultrasound. The positive predictive value of LGA diagnosis was 50.1% and the false positive rate was 10.6%. Patients with a diagnosis of LGA had higher AOR of CD (OR 2.11, 95% CI 1.56-2.83), and higher AOR of NTSV CD (OR 1.88, 95% CI 1.14-3.13) compared with those without an LGA diagnosis. There was no difference in the rates of non-medically indicated CD, multiparous primary CD, and attempted and successful TOLAC.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Our results suggest third-trimester ultrasound diagnosis of LGA independently increases odds of CD, specifically among nulliparous patients, and the potential bias may be one factor contributing to excessive CDs and NTSV CDs.</p>\\n </section>\\n </div>\",\"PeriodicalId\":17563,\"journal\":{\"name\":\"Journal of Ultrasound in Medicine\",\"volume\":\"43 11\",\"pages\":\"2109-2117\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jum.16539\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Ultrasound in Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jum.16539\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ACOUSTICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Ultrasound in Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jum.16539","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ACOUSTICS","Score":null,"Total":0}
引用次数: 0
摘要
研究目的:了解第三孕期超声诊断胎龄过大(LGA)是否会增加剖宫产风险:确定知道第三孕期超声诊断为巨大胎儿(LGA)是否会独立增加剖宫产(CD)风险:历史队列:比较2017年1月至2021年7月期间经临床指征超声诊断为LGA胎儿的患者与34周或之后未确诊LGA胎儿的患者的剖宫产率。LGA的定义是超声估计的胎儿体重大于或等于胎龄的第90百分位数。进行单变量分析以确定重要的混杂变量,并将其作为以CD率为主要结果的二元回归的协变量,计算出调整后的几率比(AOR)及95%置信区间(CI)。此外,还比较了无子宫期单胎顶点(NTSV)和多胎CD率:结果:经第三孕期超声检查确诊为 LGA 胎儿的患者有 447 例,未确诊为 LGA 胎儿的患者有 1971 例。LGA诊断的阳性预测值为50.1%,假阳性率为10.6%。与未确诊 LGA 的患者相比,确诊 LGA 的患者 CD 的 AOR 较高(OR 2.11,95% CI 1.56-2.83),NTSV CD 的 AOR 较高(OR 1.88,95% CI 1.14-3.13)。非医学指征的 CD、多胎原发性 CD 以及尝试和成功 TOLAC 的比率没有差异:我们的研究结果表明,第三孕期超声诊断 LGA 会独立增加 CD 的几率,特别是在无子宫患者中,潜在的偏差可能是导致过多 CD 和 NTSV CD 的一个因素。
Third-Trimester Ultrasound Diagnosis of Large for Gestational Age and Risk of Cesarean Delivery
Objective
Determine if knowledge of a third-trimester ultrasound diagnosis of large for gestational age (LGA) independently increases the risk of cesarean delivery (CD).
Study Design
Historical cohort comparing CD rate among patients diagnosed with an LGA fetus on a clinically indicated ultrasound from January 2017 to July 2021 with those without an LGA diagnosis at 34 weeks or later. LGA was defined as an ultrasound-estimated fetal weight greater than or equal to the 90th percentile for the gestational age. Univariate analysis was performed to identify significant confounding variables and was utilized as covariates for binary regression with CD rate as the primary outcome, and adjusted odds ratios (AOR) with 95% confidence intervals (CI) were calculated. Nulliparous term singleton vertex (NTSV) and multiparous CD rates were also compared.
Results
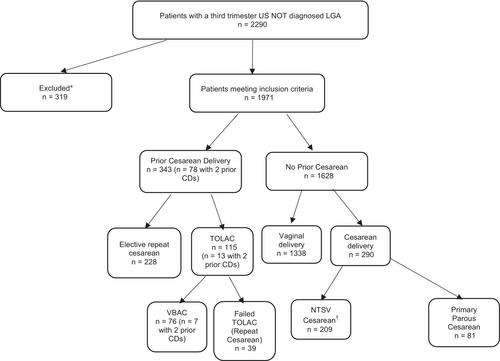
There were 447 patients diagnosed with an LGA fetus and 1971 patients without an LGA diagnosis on third-trimester ultrasound. The positive predictive value of LGA diagnosis was 50.1% and the false positive rate was 10.6%. Patients with a diagnosis of LGA had higher AOR of CD (OR 2.11, 95% CI 1.56-2.83), and higher AOR of NTSV CD (OR 1.88, 95% CI 1.14-3.13) compared with those without an LGA diagnosis. There was no difference in the rates of non-medically indicated CD, multiparous primary CD, and attempted and successful TOLAC.
Conclusion
Our results suggest third-trimester ultrasound diagnosis of LGA independently increases odds of CD, specifically among nulliparous patients, and the potential bias may be one factor contributing to excessive CDs and NTSV CDs.
期刊介绍:
The Journal of Ultrasound in Medicine (JUM) is dedicated to the rapid, accurate publication of original articles dealing with all aspects of medical ultrasound, particularly its direct application to patient care but also relevant basic science, advances in instrumentation, and biological effects. The journal is an official publication of the American Institute of Ultrasound in Medicine and publishes articles in a variety of categories, including Original Research papers, Review Articles, Pictorial Essays, Technical Innovations, Case Series, Letters to the Editor, and more, from an international bevy of countries in a continual effort to showcase and promote advances in the ultrasound community.
Represented through these efforts are a wide variety of disciplines of ultrasound, including, but not limited to:
-Basic Science-
Breast Ultrasound-
Contrast-Enhanced Ultrasound-
Dermatology-
Echocardiography-
Elastography-
Emergency Medicine-
Fetal Echocardiography-
Gastrointestinal Ultrasound-
General and Abdominal Ultrasound-
Genitourinary Ultrasound-
Gynecologic Ultrasound-
Head and Neck Ultrasound-
High Frequency Clinical and Preclinical Imaging-
Interventional-Intraoperative Ultrasound-
Musculoskeletal Ultrasound-
Neurosonology-
Obstetric Ultrasound-
Ophthalmologic Ultrasound-
Pediatric Ultrasound-
Point-of-Care Ultrasound-
Public Policy-
Superficial Structures-
Therapeutic Ultrasound-
Ultrasound Education-
Ultrasound in Global Health-
Urologic Ultrasound-
Vascular Ultrasound

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


