Heather I Greenwood, Cristian K Maldonado Rodas, Rita I Freimanis, Alexa C Glencer, Phoebe N Miller, Rita A Mukhtar, Case Brabham, Christina Yau, Jennifer M Rosenbluth, Gillian L Hirst, Michael J Campbell, Alexander Borowsky, Nola Hylton, Laura J Esserman, Amrita Basu
{"title":"磁共振成像对患有导管原位癌的妇女进行积极监控的启示。","authors":"Heather I Greenwood, Cristian K Maldonado Rodas, Rita I Freimanis, Alexa C Glencer, Phoebe N Miller, Rita A Mukhtar, Case Brabham, Christina Yau, Jennifer M Rosenbluth, Gillian L Hirst, Michael J Campbell, Alexander Borowsky, Nola Hylton, Laura J Esserman, Amrita Basu","doi":"10.1038/s41523-024-00677-9","DOIUrl":null,"url":null,"abstract":"<p><p>New approaches are needed to determine which ductal carcinoma in situ (DCIS) is at high risk for progression to invasive ductal carcinoma (IDC). We retrospectively studied DCIS patients who declined surgery (2002-2019), and received endocrine therapy (ET) and breast MRI. Baseline MRI and changes at 3 months and 6 months were analyzed by recursive partitioning to stratify IDC risk. Sixty-two patients (63 DCIS; 1 bilateral) with a mean follow-up of 8.5 years were included. Fifty-one percent remained on active surveillance (AS) without evidence of IDC, with a mean duration of 7.6 years. A decision tree based on MRI features of lesion distinctness and background parenchymal enhancement (BPE) at baseline and change after 3 months of ET stratified patients into low, intermediate, and high risk for progression to IDC. MRI imaging features in patients treated with ET and undergoing AS, may help determine which DCIS lesions are at low versus high risk for IDC.</p>","PeriodicalId":19247,"journal":{"name":"NPJ Breast Cancer","volume":"10 1","pages":"71"},"PeriodicalIF":6.5000,"publicationDate":"2024-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11298531/pdf/","citationCount":"0","resultStr":"{\"title\":\"Magnetic resonance imaging insights from active surveillance of women with ductal carcinoma in situ.\",\"authors\":\"Heather I Greenwood, Cristian K Maldonado Rodas, Rita I Freimanis, Alexa C Glencer, Phoebe N Miller, Rita A Mukhtar, Case Brabham, Christina Yau, Jennifer M Rosenbluth, Gillian L Hirst, Michael J Campbell, Alexander Borowsky, Nola Hylton, Laura J Esserman, Amrita Basu\",\"doi\":\"10.1038/s41523-024-00677-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>New approaches are needed to determine which ductal carcinoma in situ (DCIS) is at high risk for progression to invasive ductal carcinoma (IDC). We retrospectively studied DCIS patients who declined surgery (2002-2019), and received endocrine therapy (ET) and breast MRI. Baseline MRI and changes at 3 months and 6 months were analyzed by recursive partitioning to stratify IDC risk. Sixty-two patients (63 DCIS; 1 bilateral) with a mean follow-up of 8.5 years were included. Fifty-one percent remained on active surveillance (AS) without evidence of IDC, with a mean duration of 7.6 years. A decision tree based on MRI features of lesion distinctness and background parenchymal enhancement (BPE) at baseline and change after 3 months of ET stratified patients into low, intermediate, and high risk for progression to IDC. MRI imaging features in patients treated with ET and undergoing AS, may help determine which DCIS lesions are at low versus high risk for IDC.</p>\",\"PeriodicalId\":19247,\"journal\":{\"name\":\"NPJ Breast Cancer\",\"volume\":\"10 1\",\"pages\":\"71\"},\"PeriodicalIF\":6.5000,\"publicationDate\":\"2024-08-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11298531/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NPJ Breast Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41523-024-00677-9\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NPJ Breast Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41523-024-00677-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Magnetic resonance imaging insights from active surveillance of women with ductal carcinoma in situ.
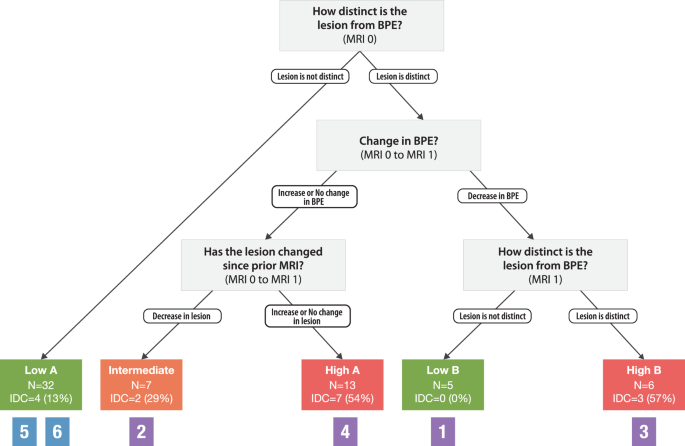
New approaches are needed to determine which ductal carcinoma in situ (DCIS) is at high risk for progression to invasive ductal carcinoma (IDC). We retrospectively studied DCIS patients who declined surgery (2002-2019), and received endocrine therapy (ET) and breast MRI. Baseline MRI and changes at 3 months and 6 months were analyzed by recursive partitioning to stratify IDC risk. Sixty-two patients (63 DCIS; 1 bilateral) with a mean follow-up of 8.5 years were included. Fifty-one percent remained on active surveillance (AS) without evidence of IDC, with a mean duration of 7.6 years. A decision tree based on MRI features of lesion distinctness and background parenchymal enhancement (BPE) at baseline and change after 3 months of ET stratified patients into low, intermediate, and high risk for progression to IDC. MRI imaging features in patients treated with ET and undergoing AS, may help determine which DCIS lesions are at low versus high risk for IDC.
期刊介绍:
npj Breast Cancer publishes original research articles, reviews, brief correspondence, meeting reports, editorial summaries and hypothesis generating observations which could be unexplained or preliminary findings from experiments, novel ideas, or the framing of new questions that need to be solved. Featured topics of the journal include imaging, immunotherapy, molecular classification of disease, mechanism-based therapies largely targeting signal transduction pathways, carcinogenesis including hereditary susceptibility and molecular epidemiology, survivorship issues including long-term toxicities of treatment and secondary neoplasm occurrence, the biophysics of cancer, mechanisms of metastasis and their perturbation, and studies of the tumor microenvironment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


