Emily L. Podany, Shaun Bulsara, Katherine Sanchez, Kristen Otte, Matthew J. Ellis, Maryam Kinik
{"title":"综合癌症中心不同患者参与乳腺癌临床试验的情况","authors":"Emily L. Podany, Shaun Bulsara, Katherine Sanchez, Kristen Otte, Matthew J. Ellis, Maryam Kinik","doi":"10.1038/s41523-024-00672-0","DOIUrl":null,"url":null,"abstract":"<p>This study was designed to determine the enrollment patterns in breast cancer clinical trials (CCTs) of patients with diverse backgrounds in an equal access setting and to evaluate the factors contributing to low rates of clinical trial accrual in patients of low socioeconomic status (SES). We performed a retrospective review of a prospectively maintained database of new patients seen at the Dan L. Duncan Comprehensive Cancer Center dating from 5/2015 to 9/2021, which included 3043 patients screened for breast CCTs. We compared the rate of CCT availability, eligibility, and enrollment between two patient populations: Smith Clinic, where most patients are of low SES and uninsured, and Baylor St. Luke’s Medical Center (BSLMC) with mostly predominantly insured, higher income patients. We performed logistic regression to evaluate whether differences in age, clinic, race, trial type, and primary language may be underlying the differences in CCT enrollment. More patients were eligible for CCTs at Smith Clinic (53.7% vs 44.7%, <i>p</i> < 0.001). However, Smith Clinic patients were more likely to decline CCT enrollment compared to BSLMC (61.3% declined vs 39.4%, <i>p</i> < 0.001). On multivariate analysis, Black patients had a significantly higher rate of CCT refusal overall (OR = 0.26, 95% CI 0.12–0.56, <i>p</i> < 0.001) and BSLMC only (OR = 0.20, 95% CI 0.060–0.60, <i>p</i> = 0.006). Our data shows that it is likely an oversimplification to assume that equal access will lead to the elimination of CCT disparities. Efforts to diversify CCTs must include consideration of structural and institutional inequities as well as social needs.</p>","PeriodicalId":19247,"journal":{"name":"NPJ Breast Cancer","volume":"43 1","pages":""},"PeriodicalIF":6.5000,"publicationDate":"2024-08-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Breast cancer clinical trial participation among diverse patients at a comprehensive cancer center\",\"authors\":\"Emily L. Podany, Shaun Bulsara, Katherine Sanchez, Kristen Otte, Matthew J. Ellis, Maryam Kinik\",\"doi\":\"10.1038/s41523-024-00672-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>This study was designed to determine the enrollment patterns in breast cancer clinical trials (CCTs) of patients with diverse backgrounds in an equal access setting and to evaluate the factors contributing to low rates of clinical trial accrual in patients of low socioeconomic status (SES). We performed a retrospective review of a prospectively maintained database of new patients seen at the Dan L. Duncan Comprehensive Cancer Center dating from 5/2015 to 9/2021, which included 3043 patients screened for breast CCTs. We compared the rate of CCT availability, eligibility, and enrollment between two patient populations: Smith Clinic, where most patients are of low SES and uninsured, and Baylor St. Luke’s Medical Center (BSLMC) with mostly predominantly insured, higher income patients. We performed logistic regression to evaluate whether differences in age, clinic, race, trial type, and primary language may be underlying the differences in CCT enrollment. More patients were eligible for CCTs at Smith Clinic (53.7% vs 44.7%, <i>p</i> < 0.001). However, Smith Clinic patients were more likely to decline CCT enrollment compared to BSLMC (61.3% declined vs 39.4%, <i>p</i> < 0.001). On multivariate analysis, Black patients had a significantly higher rate of CCT refusal overall (OR = 0.26, 95% CI 0.12–0.56, <i>p</i> < 0.001) and BSLMC only (OR = 0.20, 95% CI 0.060–0.60, <i>p</i> = 0.006). Our data shows that it is likely an oversimplification to assume that equal access will lead to the elimination of CCT disparities. Efforts to diversify CCTs must include consideration of structural and institutional inequities as well as social needs.</p>\",\"PeriodicalId\":19247,\"journal\":{\"name\":\"NPJ Breast Cancer\",\"volume\":\"43 1\",\"pages\":\"\"},\"PeriodicalIF\":6.5000,\"publicationDate\":\"2024-08-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NPJ Breast Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41523-024-00672-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NPJ Breast Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41523-024-00672-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
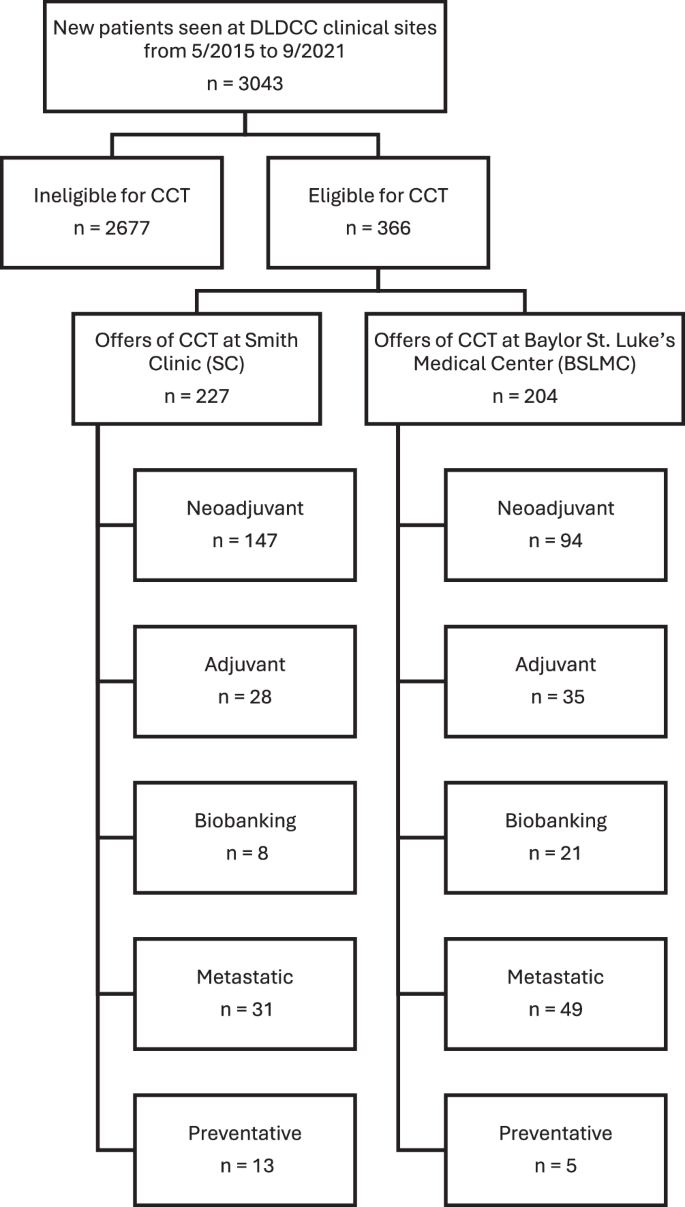
本研究旨在确定在平等就医环境下不同背景的患者参加乳腺癌临床试验(CCT)的模式,并评估导致社会经济地位(SES)低下的患者参加临床试验率低的因素。我们对丹-邓肯综合癌症中心(Dan L. Duncan Comprehensive Cancer Center)自 2015 年 5 月至 2021 年 9 月期间新就诊患者的前瞻性数据库进行了回顾性审查,其中包括 3043 名接受乳腺 CCT 筛选的患者。我们比较了两个患者群体的 CCT 可用性、资格和注册率:Smith Clinic)和 Baylor St. Luke's Medical Center(BSLMC),前者的大多数患者都是社会经济地位较低且没有保险的,而后者的大多数患者都是有保险且收入较高的。我们进行了逻辑回归,以评估年龄、诊所、种族、试验类型和主要语言的差异是否可能是导致 CCT 入选率差异的根本原因。更多患者符合史密斯诊所的 CCT 条件(53.7% 对 44.7%,P < 0.001)。然而,与 BSLMC 相比,史密斯诊所的患者更有可能拒绝加入 CCT(61.3% 拒绝 vs 39.4%,p < 0.001)。在多变量分析中,黑人患者的总体 CCT 拒绝率明显更高(OR = 0.26,95% CI 0.12-0.56,p <0.001),仅 BSLMC(OR = 0.20,95% CI 0.060-0.60,p = 0.006)。我们的数据表明,假设平等的机会将导致 CCT 差距的消除,很可能是过于简单化了。使 CCT 多元化的努力必须包括对结构性和制度性不平等以及社会需求的考虑。
Breast cancer clinical trial participation among diverse patients at a comprehensive cancer center
This study was designed to determine the enrollment patterns in breast cancer clinical trials (CCTs) of patients with diverse backgrounds in an equal access setting and to evaluate the factors contributing to low rates of clinical trial accrual in patients of low socioeconomic status (SES). We performed a retrospective review of a prospectively maintained database of new patients seen at the Dan L. Duncan Comprehensive Cancer Center dating from 5/2015 to 9/2021, which included 3043 patients screened for breast CCTs. We compared the rate of CCT availability, eligibility, and enrollment between two patient populations: Smith Clinic, where most patients are of low SES and uninsured, and Baylor St. Luke’s Medical Center (BSLMC) with mostly predominantly insured, higher income patients. We performed logistic regression to evaluate whether differences in age, clinic, race, trial type, and primary language may be underlying the differences in CCT enrollment. More patients were eligible for CCTs at Smith Clinic (53.7% vs 44.7%, p < 0.001). However, Smith Clinic patients were more likely to decline CCT enrollment compared to BSLMC (61.3% declined vs 39.4%, p < 0.001). On multivariate analysis, Black patients had a significantly higher rate of CCT refusal overall (OR = 0.26, 95% CI 0.12–0.56, p < 0.001) and BSLMC only (OR = 0.20, 95% CI 0.060–0.60, p = 0.006). Our data shows that it is likely an oversimplification to assume that equal access will lead to the elimination of CCT disparities. Efforts to diversify CCTs must include consideration of structural and institutional inequities as well as social needs.
期刊介绍:
npj Breast Cancer publishes original research articles, reviews, brief correspondence, meeting reports, editorial summaries and hypothesis generating observations which could be unexplained or preliminary findings from experiments, novel ideas, or the framing of new questions that need to be solved. Featured topics of the journal include imaging, immunotherapy, molecular classification of disease, mechanism-based therapies largely targeting signal transduction pathways, carcinogenesis including hereditary susceptibility and molecular epidemiology, survivorship issues including long-term toxicities of treatment and secondary neoplasm occurrence, the biophysics of cancer, mechanisms of metastasis and their perturbation, and studies of the tumor microenvironment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


