Thi Thu Ngan Dinh, Barbara de Graaff, Julie A. Campbell, Matthew D. Jose, John Burgess, Timothy Saunder, Alex Kitsos, Andrew J. Palmer
{"title":"妊娠期糖尿病的医疗成本:澳大利亚塔斯马尼亚州疾病成本研究。","authors":"Thi Thu Ngan Dinh, Barbara de Graaff, Julie A. Campbell, Matthew D. Jose, John Burgess, Timothy Saunder, Alex Kitsos, Andrew J. Palmer","doi":"10.1111/dme.15417","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>To estimate the direct costs during the prenatal, delivery and postpartum periods in mothers with diabetes in pregnancy, compared to those without.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study used a population-based dataset from 2004 to 2017, including 57,090 people with diabetes and 114,179 people without diabetes in Tasmania, Australia. Based on diagnostic codes, delivery episodes with gestational diabetes mellitus (GDM) were identified and matched with delivery episodes without diabetes in pregnancy. A group of delivery episodes with pre-existing diabetes was identified for comparison. Hospitalisation, emergency department and pathology costs of these groups were calculated and adjusted to 2020–2021 Australian dollars.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>There were 2774 delivery episodes with GDM, 2774 delivery episodes without diabetes and 237 delivery episodes with pre-existing diabetes identified. Across the 24-month period, the pre-existing diabetes group required the highest costs, totalling $23,536/person. This was followed by the GDM ($13,210/person), and the no diabetes group ($11,167/person). The incremental costs of GDM over the no diabetes group were $890 (95% CI 635; 1160) in the year preceding delivery; $812 (616; 1031) within the delivery period and $341 (110; 582) in the year following delivery (<i>p</i> < 0.05). Within the year preceding delivery, the incremental costs in the prenatal period were $803 (579; 1058) (<i>p</i> < 0.05). Within the year following delivery, the incremental costs in the postpartum period were $137 (55; 238) (<i>p</i> < 0.05).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Our results emphasised the importance of proper management of diabetes in pregnancy in the prenatal and postpartum periods and highlighted the significance of screening and preventative strategies for diabetes in pregnancy.</p>\n </section>\n </div>","PeriodicalId":11251,"journal":{"name":"Diabetic Medicine","volume":"41 10","pages":""},"PeriodicalIF":3.2000,"publicationDate":"2024-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dme.15417","citationCount":"0","resultStr":"{\"title\":\"Healthcare costs attributable to diabetes in pregnancy: A cost of illness study in Tasmania, Australia\",\"authors\":\"Thi Thu Ngan Dinh, Barbara de Graaff, Julie A. Campbell, Matthew D. Jose, John Burgess, Timothy Saunder, Alex Kitsos, Andrew J. Palmer\",\"doi\":\"10.1111/dme.15417\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>To estimate the direct costs during the prenatal, delivery and postpartum periods in mothers with diabetes in pregnancy, compared to those without.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This study used a population-based dataset from 2004 to 2017, including 57,090 people with diabetes and 114,179 people without diabetes in Tasmania, Australia. Based on diagnostic codes, delivery episodes with gestational diabetes mellitus (GDM) were identified and matched with delivery episodes without diabetes in pregnancy. A group of delivery episodes with pre-existing diabetes was identified for comparison. Hospitalisation, emergency department and pathology costs of these groups were calculated and adjusted to 2020–2021 Australian dollars.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>There were 2774 delivery episodes with GDM, 2774 delivery episodes without diabetes and 237 delivery episodes with pre-existing diabetes identified. Across the 24-month period, the pre-existing diabetes group required the highest costs, totalling $23,536/person. This was followed by the GDM ($13,210/person), and the no diabetes group ($11,167/person). The incremental costs of GDM over the no diabetes group were $890 (95% CI 635; 1160) in the year preceding delivery; $812 (616; 1031) within the delivery period and $341 (110; 582) in the year following delivery (<i>p</i> < 0.05). Within the year preceding delivery, the incremental costs in the prenatal period were $803 (579; 1058) (<i>p</i> < 0.05). Within the year following delivery, the incremental costs in the postpartum period were $137 (55; 238) (<i>p</i> < 0.05).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Our results emphasised the importance of proper management of diabetes in pregnancy in the prenatal and postpartum periods and highlighted the significance of screening and preventative strategies for diabetes in pregnancy.</p>\\n </section>\\n </div>\",\"PeriodicalId\":11251,\"journal\":{\"name\":\"Diabetic Medicine\",\"volume\":\"41 10\",\"pages\":\"\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dme.15417\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetic Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/dme.15417\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetic Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/dme.15417","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Healthcare costs attributable to diabetes in pregnancy: A cost of illness study in Tasmania, Australia
Aims
To estimate the direct costs during the prenatal, delivery and postpartum periods in mothers with diabetes in pregnancy, compared to those without.
Methods
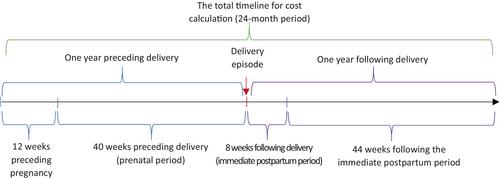
This study used a population-based dataset from 2004 to 2017, including 57,090 people with diabetes and 114,179 people without diabetes in Tasmania, Australia. Based on diagnostic codes, delivery episodes with gestational diabetes mellitus (GDM) were identified and matched with delivery episodes without diabetes in pregnancy. A group of delivery episodes with pre-existing diabetes was identified for comparison. Hospitalisation, emergency department and pathology costs of these groups were calculated and adjusted to 2020–2021 Australian dollars.
Results
There were 2774 delivery episodes with GDM, 2774 delivery episodes without diabetes and 237 delivery episodes with pre-existing diabetes identified. Across the 24-month period, the pre-existing diabetes group required the highest costs, totalling $23,536/person. This was followed by the GDM ($13,210/person), and the no diabetes group ($11,167/person). The incremental costs of GDM over the no diabetes group were $890 (95% CI 635; 1160) in the year preceding delivery; $812 (616; 1031) within the delivery period and $341 (110; 582) in the year following delivery (p < 0.05). Within the year preceding delivery, the incremental costs in the prenatal period were $803 (579; 1058) (p < 0.05). Within the year following delivery, the incremental costs in the postpartum period were $137 (55; 238) (p < 0.05).
Conclusions
Our results emphasised the importance of proper management of diabetes in pregnancy in the prenatal and postpartum periods and highlighted the significance of screening and preventative strategies for diabetes in pregnancy.
期刊介绍:
Diabetic Medicine, the official journal of Diabetes UK, is published monthly simultaneously, in print and online editions.
The journal publishes a range of key information on all clinical aspects of diabetes mellitus, ranging from human genetic studies through clinical physiology and trials to diabetes epidemiology. We do not publish original animal or cell culture studies unless they are part of a study of clinical diabetes involving humans. Categories of publication include research articles, reviews, editorials, commentaries, and correspondence. All material is peer-reviewed.
We aim to disseminate knowledge about diabetes research with the goal of improving the management of people with diabetes. The journal therefore seeks to provide a forum for the exchange of ideas between clinicians and researchers worldwide. Topics covered are of importance to all healthcare professionals working with people with diabetes, whether in primary care or specialist services.
Surplus generated from the sale of Diabetic Medicine is used by Diabetes UK to know diabetes better and fight diabetes more effectively on behalf of all people affected by and at risk of diabetes as well as their families and carers.”

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


