三级医疗机构肝脏风险评分的诊断和预后性能
IF 9.5
1区 医学
Q1 GASTROENTEROLOGY & HEPATOLOGY
引用次数: 0
摘要
背景& 目的肝脏风险评分已被提出作为一种基于血液的工具,用于估算肝脏硬度测量值(LSM),从而对没有已知慢性肝病(CLD)的患者发生代偿性晚期慢性肝病(cACLD,LSM≥10 kPa)和肝脏相关事件的风险进行分层。方法回顾性纳入转诊到两个肝病门诊的患者(队列 I,n = 5,897;队列 II,n = 1,558)。评估了肝脏风险评分与 LSM 的校准/一致性,并将 cACLD 的诊断准确性与纤维化-4(FIB-4)/天门冬氨酸氨基转移酶与血小板比值指数(APRI)进行了比较。结果在队列 I/II 中,平均年龄为 48.3/51.8 岁,44.2%/44.7% 为女性,主要病因为病毒性肝炎(51.中位 LSM 为 6.9 (IQR 5.1-10.9)/5.8 (IQR 4.5-8.8) kPa,1,690 (28.7%)/322 (20.7%) 名患者患有 cACLD。尽管存在中等程度的相关性(Pearson's r = 0.325/0.422),但肝脏风险评分系统性地低估了 LSM(低 2.93/1.80 分/kPa),且一致性范围较宽,尤其是在较高值时。肝脏风险评分对 cACLD 的诊断准确性(接收器操作者特征曲线下面积 [AUROC] 0.757/0.790)与 FIB-4(AUROC 0.769/0.813)和 APRI(AUROC 0.747/0.765)相当。建议的 10 分临界值的准确率为 74.2%/81.2%,特异性高(91.9%/93.4%),但阴性预测值低(76.6%/84.5%,Cohen's κ = 0.260/0.327)。肝脏风险评分在预测 1-5 年内肝功能失代偿方面显示出合理的准确性(AUROC 0.778-0.832)。但是,它不如 LSM(AUROC 0.847-0.901,p <0.001)和 FIB-4(AUROC 0.898-0.913,p <0.001)。结论在三级医疗机构中,LiverRisk 评分并不能改善 cACLD 的诊断或肝功能失代偿的预测。影响和意义LiverRisk 评分已被提出作为一种无创工具,用于评估肝脏僵硬度测量,从而评估代偿性晚期慢性肝病和肝脏相关事件的风险。随着实验室报告自动实施的讨论,出现了其在普通人群机会性筛查之外的适用性问题。在两个大型肝病门诊转诊患者队列中,LiverRisk评分不能准确预测肝硬变,不能提高cACLD的识别率,与FIB-4相比,对肝功能失代偿的预测性较低。尽管肝脏风险评分在初级医疗机构筛查无已知肝病患者方面迈出了一大步,但我们的研究结果表明,肝脏风险评分并不能改善初级医疗机构以外的患者管理,即在检测前 cACLD 可能性较高的人群中。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Diagnostic and prognostic performance of the LiverRisk score in tertiary care
Background & Aims
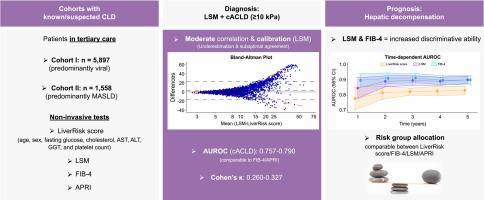
The LiverRisk score has been proposed as a blood-based tool to estimate liver stiffness measurement (LSM), thereby stratifying the risk of compensated advanced chronic liver disease (cACLD, LSM ≥10 kPa) and liver-related events in patients without known chronic liver disease (CLD). We aimed to evaluate its diagnostic/prognostic performance in tertiary care.
Methods
Patients referred to two hepatology outpatient clinics (cohort I, n = 5,897; cohort II, n = 1,558) were retrospectively included. Calibration/agreement of the LiverRisk score with LSM was assessed, and diagnostic accuracy for cACLD was compared with that of fibrosis-4 (FIB-4)/aspartate aminotransferase-to-platelet ratio index (APRI). The prediction of hepatic decompensation and utility of proposed cut-offs were evaluated.
Results
In cohort I/II, mean age was 48.3/51.8 years, 44.2%/44.7% were female, predominant etiologies were viral hepatitis (51.8%)/metabolic dysfunction-associated steatotic liver disease (63.7%), median LSM was 6.9 (IQR 5.1–10.9)/5.8 (IQR 4.5–8.8) kPa, and 1,690 (28.7%)/322 (20.7%) patients had cACLD.
Despite a moderate correlation (Pearson’s r = 0.325/0.422), the LiverRisk score systematically underestimated LSM (2.93/1.80 points/kPa lower), and range of agreement was wide, especially at higher values.
The diagnostic accuracy of the LiverRisk score for cACLD (area under the receiver operator characteristics curve [AUROC] 0.757/0.790) was comparable to that of FIB-4 (AUROC 0.769/0.813) and APRI (AUROC 0.747/0.765). The proposed cut-off of 10 points yielded an accuracy of 74.2%/81.2%, high specificity (91.9%/93.4%), but low negative predictive value (76.6%/84.5%, Cohen’s κ = 0.260/0.327).
In cohort I, 208 (3.5%) patients developed hepatic decompensation (median follow-up 4.7 years). The LiverRisk score showed a reasonable accuracy for predicting hepatic decompensation within 1–5 years (AUROC 0.778–0.832). However, it was inferior to LSM (AUROC 0.847–0.901, p <0.001) and FIB-4 (AUROC 0.898–0.913, p <0.001). Similar to the strata of other non-invasive tests, the proposed LiverRisk groups had distinct risks of hepatic decompensation.
Conclusions
The LiverRisk score did not improve the diagnosis of cACLD or prediction of hepatic decompensation in the tertiary care setting.
Impact and implications
The LiverRisk score has been proposed as a non-invasive tool to estimate liver stiffness measurement and thus the risk of compensated advanced chronic liver disease and liver-related events. As automatic implementation into lab reports is being discussed, the question of its applicability outside of opportunistic screening in the general population arises. In two large cohorts of patients referred to hepatology outpatient clinics, the LiverRisk score did not accurately predict liver stiffness, did not improve cACLD identification, and had a lower predictive performance for hepatic decompensation as compared with FIB-4. Although it represents a major step forward for screening patients without known liver disease in primary care, our findings indicate that the LiverRisk score does not improve patient management outside the primary care setting, that is, in cohorts with a higher pre-test probability of cACLD.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊
JHEP Reports
GASTROENTEROLOGY & HEPATOLOGY-
CiteScore
12.40
自引率
2.40%
发文量
161
审稿时长
36 days
期刊介绍:
JHEP Reports is an open access journal that is affiliated with the European Association for the Study of the Liver (EASL). It serves as a companion journal to the highly respected Journal of Hepatology.
The primary objective of JHEP Reports is to publish original papers and reviews that contribute to the advancement of knowledge in the field of liver diseases. The journal covers a wide range of topics, including basic, translational, and clinical research. It also focuses on global issues in hepatology, with particular emphasis on areas such as clinical trials, novel diagnostics, precision medicine and therapeutics, cancer research, cellular and molecular studies, artificial intelligence, microbiome research, epidemiology, and cutting-edge technologies.
In summary, JHEP Reports is dedicated to promoting scientific discoveries and innovations in liver diseases through the publication of high-quality research papers and reviews covering various aspects of hepatology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


