{"title":"原发性胆道弥漫大 B 细胞淋巴瘤的独特内镜特征:病例报告与文献综述(附视频)。","authors":"Tomoya Nakamura, Yoshiharu Masaki, Naohiro Kameyama, Yujiro Kawakami, Keisuke Ishigami, Yumemi Takada, Shuji Satoh, Taro Sugawara, Shintaro Sugita, Hiroshi Nakase","doi":"10.1002/deo2.414","DOIUrl":null,"url":null,"abstract":"<p>A 67-year-old man visited our hospital complaining of dark-colored urine and upper abdominal pain. Magnetic resonance cholangiopancreatography showed stricture of the distal bile duct, and contrast-enhanced computed tomography showed irregular thickening of the distal bile duct wall. However, no enlarged lymph nodes, pancreatic tumors, or other neoplastic lesions were apparent around the bile duct. Endoscopic ultrasonography and intraductal ultrasonography showed irregular thickening of the inner hypoechoic layer without the disappearance of the innermost thin hyperechoic layer. On the basis of these findings, we considered that the bile duct lesion was of non-epithelial origin. Thus, we repeatedly performed bile duct biopsies from the same site under fluoroscopy to obtain a sample of the submucosal tissue. The pathological diagnosis was diffuse large B-cell lymphoma, and the patient received systemic chemotherapy (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). After six courses of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone, positron emission tomography-computed tomography showed the disappearance of 18-fluorodeoxyglucose uptake in the bile duct and endoscopic retrograde cholangiography showed improvement of the bile duct stricture. Endoscopic findings and repeated biopsies were useful in making the diagnosis of primary biliary diffuse large B-cell lymphoma.</p>","PeriodicalId":93973,"journal":{"name":"DEN open","volume":"5 1","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2024-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11284119/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unique endoscopic features of primary biliary diffuse large B-cell lymphoma: A case report with literature review (with video)\",\"authors\":\"Tomoya Nakamura, Yoshiharu Masaki, Naohiro Kameyama, Yujiro Kawakami, Keisuke Ishigami, Yumemi Takada, Shuji Satoh, Taro Sugawara, Shintaro Sugita, Hiroshi Nakase\",\"doi\":\"10.1002/deo2.414\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 67-year-old man visited our hospital complaining of dark-colored urine and upper abdominal pain. Magnetic resonance cholangiopancreatography showed stricture of the distal bile duct, and contrast-enhanced computed tomography showed irregular thickening of the distal bile duct wall. However, no enlarged lymph nodes, pancreatic tumors, or other neoplastic lesions were apparent around the bile duct. Endoscopic ultrasonography and intraductal ultrasonography showed irregular thickening of the inner hypoechoic layer without the disappearance of the innermost thin hyperechoic layer. On the basis of these findings, we considered that the bile duct lesion was of non-epithelial origin. Thus, we repeatedly performed bile duct biopsies from the same site under fluoroscopy to obtain a sample of the submucosal tissue. The pathological diagnosis was diffuse large B-cell lymphoma, and the patient received systemic chemotherapy (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). After six courses of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone, positron emission tomography-computed tomography showed the disappearance of 18-fluorodeoxyglucose uptake in the bile duct and endoscopic retrograde cholangiography showed improvement of the bile duct stricture. Endoscopic findings and repeated biopsies were useful in making the diagnosis of primary biliary diffuse large B-cell lymphoma.</p>\",\"PeriodicalId\":93973,\"journal\":{\"name\":\"DEN open\",\"volume\":\"5 1\",\"pages\":\"\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11284119/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"DEN open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/deo2.414\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"DEN open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/deo2.414","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
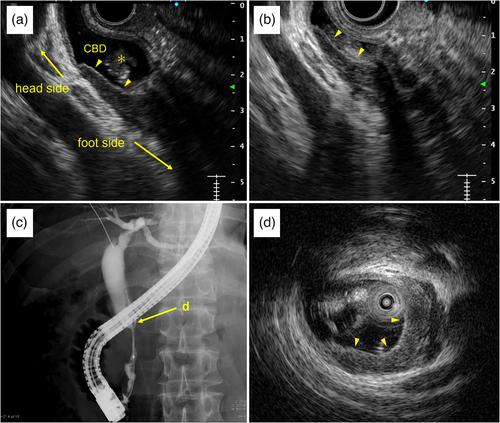
一名 67 岁的男子因深色尿液和上腹部疼痛到我院就诊。磁共振胰胆管造影显示远端胆管狭窄,对比增强计算机断层扫描显示远端胆管壁不规则增厚。但是,胆管周围没有明显的肿大淋巴结、胰腺肿瘤或其他肿瘤病变。内镜超声波检查和导管内超声波检查显示内侧低回声层不规则增厚,但最内侧的薄高回声层没有消失。根据这些结果,我们认为胆管病变是非上皮源性的。因此,我们在透视下反复从同一部位进行胆管活检,以获取黏膜下组织样本。病理诊断为弥漫大 B 细胞淋巴瘤,患者接受了全身化疗(利妥昔单抗、环磷酰胺、多柔比星、长春新碱和泼尼松)。经过六个疗程的利妥昔单抗、环磷酰胺、多柔比星、长春新碱和泼尼松治疗后,正电子发射计算机断层扫描显示胆管中的 18-氟脱氧葡萄糖摄取消失,内镜逆行胆管造影显示胆管狭窄有所改善。内镜检查结果和反复活检有助于诊断原发性胆道弥漫大B细胞淋巴瘤。
Unique endoscopic features of primary biliary diffuse large B-cell lymphoma: A case report with literature review (with video)
A 67-year-old man visited our hospital complaining of dark-colored urine and upper abdominal pain. Magnetic resonance cholangiopancreatography showed stricture of the distal bile duct, and contrast-enhanced computed tomography showed irregular thickening of the distal bile duct wall. However, no enlarged lymph nodes, pancreatic tumors, or other neoplastic lesions were apparent around the bile duct. Endoscopic ultrasonography and intraductal ultrasonography showed irregular thickening of the inner hypoechoic layer without the disappearance of the innermost thin hyperechoic layer. On the basis of these findings, we considered that the bile duct lesion was of non-epithelial origin. Thus, we repeatedly performed bile duct biopsies from the same site under fluoroscopy to obtain a sample of the submucosal tissue. The pathological diagnosis was diffuse large B-cell lymphoma, and the patient received systemic chemotherapy (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). After six courses of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone, positron emission tomography-computed tomography showed the disappearance of 18-fluorodeoxyglucose uptake in the bile duct and endoscopic retrograde cholangiography showed improvement of the bile duct stricture. Endoscopic findings and repeated biopsies were useful in making the diagnosis of primary biliary diffuse large B-cell lymphoma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


