Anandi Lobo, Katrina Collins, Seema Kaushal, Andres M Acosta, Mahmut Akgul, Amit K Adhya, Hikmat A Al-Ahmadie, Khaleel I Al-Obaidy, Ali Amin, Mahul B Amin, Manju Aron, Bonnie L Balzer, Rupanita Biswal, Subashish Mohanty, Lisa Browning, Indranil Chakrabarti, Luca Cima, Alessia Cimadamore, Sangeeta Desai, Jasreman Dhillon, Akansha Deshwal, Guillermo G Diego, Preeti Diwaker, Laurence A Galea, Cristina Magi-Galluzzi, Giovanna A Giannico, Nilesh S Gupta, Aiman Haider, Michelle S Hirsch, Kenneth A Iczkowski, Samriti Arora, Ekta Jain, Deepika Jain, Shilpy Jha, Shivani Kandukuri, Chia-Sui Kao, Sunny, Oleksandr N Kryvenko, Ramani M Kumar, Niraj Kumari, Lakshmi P Kunju, Levente Kuthi, João Lobo, Jose I Lopez, Daniel J Luthringer, Fiona Maclean, Claudia Manini, Rahul Mannan, María G Martos, Rohit Mehra, Santosh Menon, Pritinanda Mishra, Holger Moch, Rodolfo Montironi, Manas R Baisakh, George J Netto, Lovelesh K Nigam, Adeboye O Osunkoya, Francesca Pagliuca, Gladell P Paner, Angel Panizo, Anil V Parwani, Maria M Picken, Susan Prendeville, Christopher G Przybycin, Suvendu Purkait, Francisco J Queipo, B Vishal Rao, Priya Rao, Victor E Reuter, Sankalp Sancheti, Ankur R Sangoi, Rohan Sardana, Swati Satturwar, Rajal B Shah, Shivani Sharma, Mallika Dixit, Monica Verma, Deepika Sirohi, Steven C Smith, Shailesh Soni, Sandhya Sundaram, Meenakshi Swain, Maria Tretiakova, Kiril Trpkov, Gorka MuñizUnamunzaga, Ming Zhou, Sean R Williamson, Antonio Lopez-Beltran, Liang Cheng, Sambit K Mohanty
{"title":"尿路上皮癌(UC)常规组织学和亚型组织学分子异质性的进展、识别和解释:泌尿科病理学家调查和文献综述。","authors":"Anandi Lobo, Katrina Collins, Seema Kaushal, Andres M Acosta, Mahmut Akgul, Amit K Adhya, Hikmat A Al-Ahmadie, Khaleel I Al-Obaidy, Ali Amin, Mahul B Amin, Manju Aron, Bonnie L Balzer, Rupanita Biswal, Subashish Mohanty, Lisa Browning, Indranil Chakrabarti, Luca Cima, Alessia Cimadamore, Sangeeta Desai, Jasreman Dhillon, Akansha Deshwal, Guillermo G Diego, Preeti Diwaker, Laurence A Galea, Cristina Magi-Galluzzi, Giovanna A Giannico, Nilesh S Gupta, Aiman Haider, Michelle S Hirsch, Kenneth A Iczkowski, Samriti Arora, Ekta Jain, Deepika Jain, Shilpy Jha, Shivani Kandukuri, Chia-Sui Kao, Sunny, Oleksandr N Kryvenko, Ramani M Kumar, Niraj Kumari, Lakshmi P Kunju, Levente Kuthi, João Lobo, Jose I Lopez, Daniel J Luthringer, Fiona Maclean, Claudia Manini, Rahul Mannan, María G Martos, Rohit Mehra, Santosh Menon, Pritinanda Mishra, Holger Moch, Rodolfo Montironi, Manas R Baisakh, George J Netto, Lovelesh K Nigam, Adeboye O Osunkoya, Francesca Pagliuca, Gladell P Paner, Angel Panizo, Anil V Parwani, Maria M Picken, Susan Prendeville, Christopher G Przybycin, Suvendu Purkait, Francisco J Queipo, B Vishal Rao, Priya Rao, Victor E Reuter, Sankalp Sancheti, Ankur R Sangoi, Rohan Sardana, Swati Satturwar, Rajal B Shah, Shivani Sharma, Mallika Dixit, Monica Verma, Deepika Sirohi, Steven C Smith, Shailesh Soni, Sandhya Sundaram, Meenakshi Swain, Maria Tretiakova, Kiril Trpkov, Gorka MuñizUnamunzaga, Ming Zhou, Sean R Williamson, Antonio Lopez-Beltran, Liang Cheng, Sambit K Mohanty","doi":"10.1111/his.15287","DOIUrl":null,"url":null,"abstract":"<div>\n \n <section>\n \n <h3> Aims</h3>\n \n <p>Urothelial carcinoma (UC) demonstrates significant molecular and histologic heterogeneity. The WHO 2022 classification has hinted at adding molecular signatures to the morphologic diagnosis. As morphology and associated molecular repertoire may potentially translate to choices of and response to therapy and relapse rate, broader acceptability of recognizing these key features among uropathologists is needed. This prompted an international survey to ascertain the practice patterns in classical/subtype UC among uropathologists across the globe.</p>\n </section>\n \n <section>\n \n <h3> Methods and Results</h3>\n \n <p>A survey instrument was shared among 98 uropathologists using SurveyMonkey software. Anonymized respondent data were analysed. The response rate was 85%. A majority were in concordance with the profiles of luminal (93%) and basal (82%) types. Opinion on the <i>FGFR3</i> testing platform was variable. While 95% concurred that <i>TERT</i> promoter mutation is the key driver in UC, 72% had the opinion that <i>APOBEC</i> mutagenesis is the main signature in muscle invasive bladder cancer (MIBC). Uropathologists have divergent opinions on MIBC and <i>ERCC2</i> mutations. Among the participants, 94% would quantify aggressive micropapillary and sarcomatoid histology, while 88% would reevaluate another transurethral resection of the bladder tumour specimen in nonmuscle invasive tumour with micropapillary, small cell, or sarcomatoid histology. A leading number agreed to specific molecular signatures of micropapillary (93%), plasmacytoid (97%), and small cell (86%) subtypes. Ninety-six percent of participants agreed that a small-cell component portends a more aggressive course and should be treated with neoadjuvant chemotherapy and 63% would perform <i>HER2/neu</i> testing only on oncologist's request in advanced tumours. Ninety percent agreed that microsatellite instability testing, although not a standard protocol, should be considered in young patients with upper tract UC. Eighty-six percent agreed that UC with high tumour mutational burden would be a better candidate for immunotherapy.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In the era of precision medicine, enhanced understanding of molecular heterogeneity of UC will contribute to better therapeutic options, novel biomarker discovery, innovative management protocols, and outcomes. Our survey provides a broad perspective of pathologists' perceptions and experience regarding incorporation of histomolecular approaches to “personalize” therapy. Due to variable clinical adoption, there is a need for additional data using uniform study criteria. This will drive generation of best practice guidelines in this area for widespread and consistent clinical utility.</p>\n </section>\n </div>","PeriodicalId":13219,"journal":{"name":"Histopathology","volume":"85 5","pages":"748-759"},"PeriodicalIF":3.9000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Advances, recognition, and interpretation of molecular heterogeneity among conventional and subtype histology of urothelial carcinoma (UC): a survey among urologic pathologists and comprehensive review of the literature\",\"authors\":\"Anandi Lobo, Katrina Collins, Seema Kaushal, Andres M Acosta, Mahmut Akgul, Amit K Adhya, Hikmat A Al-Ahmadie, Khaleel I Al-Obaidy, Ali Amin, Mahul B Amin, Manju Aron, Bonnie L Balzer, Rupanita Biswal, Subashish Mohanty, Lisa Browning, Indranil Chakrabarti, Luca Cima, Alessia Cimadamore, Sangeeta Desai, Jasreman Dhillon, Akansha Deshwal, Guillermo G Diego, Preeti Diwaker, Laurence A Galea, Cristina Magi-Galluzzi, Giovanna A Giannico, Nilesh S Gupta, Aiman Haider, Michelle S Hirsch, Kenneth A Iczkowski, Samriti Arora, Ekta Jain, Deepika Jain, Shilpy Jha, Shivani Kandukuri, Chia-Sui Kao, Sunny, Oleksandr N Kryvenko, Ramani M Kumar, Niraj Kumari, Lakshmi P Kunju, Levente Kuthi, João Lobo, Jose I Lopez, Daniel J Luthringer, Fiona Maclean, Claudia Manini, Rahul Mannan, María G Martos, Rohit Mehra, Santosh Menon, Pritinanda Mishra, Holger Moch, Rodolfo Montironi, Manas R Baisakh, George J Netto, Lovelesh K Nigam, Adeboye O Osunkoya, Francesca Pagliuca, Gladell P Paner, Angel Panizo, Anil V Parwani, Maria M Picken, Susan Prendeville, Christopher G Przybycin, Suvendu Purkait, Francisco J Queipo, B Vishal Rao, Priya Rao, Victor E Reuter, Sankalp Sancheti, Ankur R Sangoi, Rohan Sardana, Swati Satturwar, Rajal B Shah, Shivani Sharma, Mallika Dixit, Monica Verma, Deepika Sirohi, Steven C Smith, Shailesh Soni, Sandhya Sundaram, Meenakshi Swain, Maria Tretiakova, Kiril Trpkov, Gorka MuñizUnamunzaga, Ming Zhou, Sean R Williamson, Antonio Lopez-Beltran, Liang Cheng, Sambit K Mohanty\",\"doi\":\"10.1111/his.15287\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Urothelial carcinoma (UC) demonstrates significant molecular and histologic heterogeneity. The WHO 2022 classification has hinted at adding molecular signatures to the morphologic diagnosis. As morphology and associated molecular repertoire may potentially translate to choices of and response to therapy and relapse rate, broader acceptability of recognizing these key features among uropathologists is needed. This prompted an international survey to ascertain the practice patterns in classical/subtype UC among uropathologists across the globe.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and Results</h3>\\n \\n <p>A survey instrument was shared among 98 uropathologists using SurveyMonkey software. Anonymized respondent data were analysed. The response rate was 85%. A majority were in concordance with the profiles of luminal (93%) and basal (82%) types. Opinion on the <i>FGFR3</i> testing platform was variable. While 95% concurred that <i>TERT</i> promoter mutation is the key driver in UC, 72% had the opinion that <i>APOBEC</i> mutagenesis is the main signature in muscle invasive bladder cancer (MIBC). Uropathologists have divergent opinions on MIBC and <i>ERCC2</i> mutations. Among the participants, 94% would quantify aggressive micropapillary and sarcomatoid histology, while 88% would reevaluate another transurethral resection of the bladder tumour specimen in nonmuscle invasive tumour with micropapillary, small cell, or sarcomatoid histology. A leading number agreed to specific molecular signatures of micropapillary (93%), plasmacytoid (97%), and small cell (86%) subtypes. Ninety-six percent of participants agreed that a small-cell component portends a more aggressive course and should be treated with neoadjuvant chemotherapy and 63% would perform <i>HER2/neu</i> testing only on oncologist's request in advanced tumours. Ninety percent agreed that microsatellite instability testing, although not a standard protocol, should be considered in young patients with upper tract UC. Eighty-six percent agreed that UC with high tumour mutational burden would be a better candidate for immunotherapy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In the era of precision medicine, enhanced understanding of molecular heterogeneity of UC will contribute to better therapeutic options, novel biomarker discovery, innovative management protocols, and outcomes. Our survey provides a broad perspective of pathologists' perceptions and experience regarding incorporation of histomolecular approaches to “personalize” therapy. Due to variable clinical adoption, there is a need for additional data using uniform study criteria. This will drive generation of best practice guidelines in this area for widespread and consistent clinical utility.</p>\\n </section>\\n </div>\",\"PeriodicalId\":13219,\"journal\":{\"name\":\"Histopathology\",\"volume\":\"85 5\",\"pages\":\"748-759\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2024-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Histopathology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/his.15287\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CELL BIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Histopathology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/his.15287","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CELL BIOLOGY","Score":null,"Total":0}
Advances, recognition, and interpretation of molecular heterogeneity among conventional and subtype histology of urothelial carcinoma (UC): a survey among urologic pathologists and comprehensive review of the literature
Aims
Urothelial carcinoma (UC) demonstrates significant molecular and histologic heterogeneity. The WHO 2022 classification has hinted at adding molecular signatures to the morphologic diagnosis. As morphology and associated molecular repertoire may potentially translate to choices of and response to therapy and relapse rate, broader acceptability of recognizing these key features among uropathologists is needed. This prompted an international survey to ascertain the practice patterns in classical/subtype UC among uropathologists across the globe.
Methods and Results
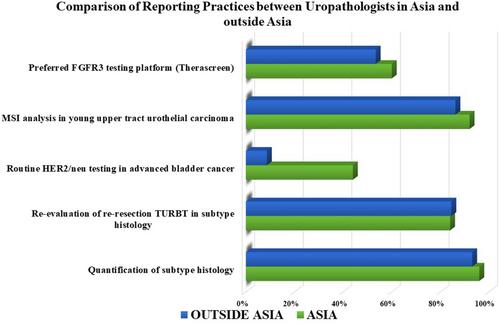
A survey instrument was shared among 98 uropathologists using SurveyMonkey software. Anonymized respondent data were analysed. The response rate was 85%. A majority were in concordance with the profiles of luminal (93%) and basal (82%) types. Opinion on the FGFR3 testing platform was variable. While 95% concurred that TERT promoter mutation is the key driver in UC, 72% had the opinion that APOBEC mutagenesis is the main signature in muscle invasive bladder cancer (MIBC). Uropathologists have divergent opinions on MIBC and ERCC2 mutations. Among the participants, 94% would quantify aggressive micropapillary and sarcomatoid histology, while 88% would reevaluate another transurethral resection of the bladder tumour specimen in nonmuscle invasive tumour with micropapillary, small cell, or sarcomatoid histology. A leading number agreed to specific molecular signatures of micropapillary (93%), plasmacytoid (97%), and small cell (86%) subtypes. Ninety-six percent of participants agreed that a small-cell component portends a more aggressive course and should be treated with neoadjuvant chemotherapy and 63% would perform HER2/neu testing only on oncologist's request in advanced tumours. Ninety percent agreed that microsatellite instability testing, although not a standard protocol, should be considered in young patients with upper tract UC. Eighty-six percent agreed that UC with high tumour mutational burden would be a better candidate for immunotherapy.
Conclusion
In the era of precision medicine, enhanced understanding of molecular heterogeneity of UC will contribute to better therapeutic options, novel biomarker discovery, innovative management protocols, and outcomes. Our survey provides a broad perspective of pathologists' perceptions and experience regarding incorporation of histomolecular approaches to “personalize” therapy. Due to variable clinical adoption, there is a need for additional data using uniform study criteria. This will drive generation of best practice guidelines in this area for widespread and consistent clinical utility.
期刊介绍:
Histopathology is an international journal intended to be of practical value to surgical and diagnostic histopathologists, and to investigators of human disease who employ histopathological methods. Our primary purpose is to publish advances in pathology, in particular those applicable to clinical practice and contributing to the better understanding of human disease.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


