Mathijs Willemsen, Pieter Smeets, Aniek de Coninck
{"title":"异基因造血细胞移植治疗 T 细胞急性淋巴细胞白血病后的孤立性周围神经系统复发。","authors":"Mathijs Willemsen, Pieter Smeets, Aniek de Coninck","doi":"10.1002/ajh.27441","DOIUrl":null,"url":null,"abstract":"<p>A 23-year-old man was admitted with left peripheral facial nerve palsy and right C7 radiculopathy. Ten weeks prior, he had received an allogeneic hematopoietic stem cell transplant (allo-HSCT) for presumed peripheral nervous system (PNS) and cerebrospinal fluid (CSF) flow cytometry-confirmed central nervous system (CNS) relapse of T-cell acute lymphoblastic leukemia (T-ALL). CNS MRI showed bilateral peripheral facial nerve enhancement without evidence of leptomeningeal or spinal disease (Figure 1A). CSF flow cytometry, viral PCRs, and bacterial cultures were unrevealing on multiple occasions. MRI of the brachial plexus showed diffuse nerve root thickening and edema with pathological enhancement, more pronounced on the right side (Figure 1B,C). Nerve conduction studies showed no evidence of demyelination. A total body PET/CT scan showed bilateral FDG accumulation in the brachial plexus, more pronounced on the right side (Figure 1D). Complete blood count was within normal limits with full donor chimerism. Bone marrow biopsy and flow cytometry excluded medullary relapse. Meanwhile, the patient experienced progressive pain, weakness, and muscle atrophy of the right arm requiring high-dose opioids and also developed right peripheral facial nerve palsy and similar symptomology of the left arm. High-dose intravenous immunoglobulins were ineffective. In an attempt to obtain a definitive diagnosis, the patient underwent surgical brachial plexus C7 biopsy. Hematoxylin and eosin staining showed effacement of normal nerve architecture with diffuse infiltration of blast-like cells (Figure 1E,F). S100 immunohistochemistry revealed sparse preexisting nerve fibers (Figure 1G). Blast-like cells were strongly positive for CD3 (Figure 1H) and TdT (Figure 1I), as well as CD10 and weakly positive for CD4 and CD8. MPO, PAX5 and CD30 were negative. A diagnosis of PNS relapse in the brachial plexus, and potentially facial nerves, was made. Without remaining curative treatment options, the patient received radiotherapy, resulting in substantial pain relief, and dexamethasone and was discharged home with palliative care.</p><p>The infiltration of peripheral nerves by leukemic blasts, termed neuroleukemiosis, is a rare neurological manifestation of leukemia with unknown incidence and no established diagnostic or therapeutic guidelines.<span><sup>1, 2</sup></span> Biopsy-confirmed cases of neuroleukemiosis in T-ALL are only sparsely reported in the literature.<span><sup>3-7</sup></span></p><p>The patient did not have CNS involvement at diagnosis but experienced a combined PNS and CNS relapse after intensive chemotherapy warranting allo-HSCT. Interestingly, relapse post-allo-HSCT was isolated to the PNS with similar symptomology as the pre-allo-HSCT relapse, suggesting that reinduction chemotherapy, myeloablative conditioning, and graft-versus-leukemia effect were more effective in eradicating CNS than PNS disease. Leukemic blasts can persists in the PNS for many years as exemplified by a case of acute monoblastic leukemia with isolated median nerve relapse after 12 years of remission.<span><sup>8</sup></span> Isolated PNS relapse often precedes systemic relapse.<span><sup>1</sup></span></p><p>Neuroleukemiosis is a rare clinical entity that should be included in the differential diagnosis of unexplained neurological deficits in patients with acute leukemia, even during remission. Isolated extramedullary relapse of the PNS is extremely rare and the PNS might serve as an sanctuary site for leukemic blasts and facilitate systemic relapse.<span><sup>1, 2</sup></span></p><p>The authors have declared that no conflicts of interest exist.</p><p>The patient provided written informed consent for use of medical information and images in this case report. The signed informed consent form is available upon request.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"99 10","pages":"2023-2025"},"PeriodicalIF":10.1000,"publicationDate":"2024-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27441","citationCount":"0","resultStr":"{\"title\":\"Isolated peripheral nervous system relapse after allogeneic hematopoietic cell transplantation for T-cell acute lymphoblastic leukemia\",\"authors\":\"Mathijs Willemsen, Pieter Smeets, Aniek de Coninck\",\"doi\":\"10.1002/ajh.27441\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 23-year-old man was admitted with left peripheral facial nerve palsy and right C7 radiculopathy. Ten weeks prior, he had received an allogeneic hematopoietic stem cell transplant (allo-HSCT) for presumed peripheral nervous system (PNS) and cerebrospinal fluid (CSF) flow cytometry-confirmed central nervous system (CNS) relapse of T-cell acute lymphoblastic leukemia (T-ALL). CNS MRI showed bilateral peripheral facial nerve enhancement without evidence of leptomeningeal or spinal disease (Figure 1A). CSF flow cytometry, viral PCRs, and bacterial cultures were unrevealing on multiple occasions. MRI of the brachial plexus showed diffuse nerve root thickening and edema with pathological enhancement, more pronounced on the right side (Figure 1B,C). Nerve conduction studies showed no evidence of demyelination. A total body PET/CT scan showed bilateral FDG accumulation in the brachial plexus, more pronounced on the right side (Figure 1D). Complete blood count was within normal limits with full donor chimerism. Bone marrow biopsy and flow cytometry excluded medullary relapse. Meanwhile, the patient experienced progressive pain, weakness, and muscle atrophy of the right arm requiring high-dose opioids and also developed right peripheral facial nerve palsy and similar symptomology of the left arm. High-dose intravenous immunoglobulins were ineffective. In an attempt to obtain a definitive diagnosis, the patient underwent surgical brachial plexus C7 biopsy. Hematoxylin and eosin staining showed effacement of normal nerve architecture with diffuse infiltration of blast-like cells (Figure 1E,F). S100 immunohistochemistry revealed sparse preexisting nerve fibers (Figure 1G). Blast-like cells were strongly positive for CD3 (Figure 1H) and TdT (Figure 1I), as well as CD10 and weakly positive for CD4 and CD8. MPO, PAX5 and CD30 were negative. A diagnosis of PNS relapse in the brachial plexus, and potentially facial nerves, was made. Without remaining curative treatment options, the patient received radiotherapy, resulting in substantial pain relief, and dexamethasone and was discharged home with palliative care.</p><p>The infiltration of peripheral nerves by leukemic blasts, termed neuroleukemiosis, is a rare neurological manifestation of leukemia with unknown incidence and no established diagnostic or therapeutic guidelines.<span><sup>1, 2</sup></span> Biopsy-confirmed cases of neuroleukemiosis in T-ALL are only sparsely reported in the literature.<span><sup>3-7</sup></span></p><p>The patient did not have CNS involvement at diagnosis but experienced a combined PNS and CNS relapse after intensive chemotherapy warranting allo-HSCT. Interestingly, relapse post-allo-HSCT was isolated to the PNS with similar symptomology as the pre-allo-HSCT relapse, suggesting that reinduction chemotherapy, myeloablative conditioning, and graft-versus-leukemia effect were more effective in eradicating CNS than PNS disease. Leukemic blasts can persists in the PNS for many years as exemplified by a case of acute monoblastic leukemia with isolated median nerve relapse after 12 years of remission.<span><sup>8</sup></span> Isolated PNS relapse often precedes systemic relapse.<span><sup>1</sup></span></p><p>Neuroleukemiosis is a rare clinical entity that should be included in the differential diagnosis of unexplained neurological deficits in patients with acute leukemia, even during remission. Isolated extramedullary relapse of the PNS is extremely rare and the PNS might serve as an sanctuary site for leukemic blasts and facilitate systemic relapse.<span><sup>1, 2</sup></span></p><p>The authors have declared that no conflicts of interest exist.</p><p>The patient provided written informed consent for use of medical information and images in this case report. The signed informed consent form is available upon request.</p>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"99 10\",\"pages\":\"2023-2025\"},\"PeriodicalIF\":10.1000,\"publicationDate\":\"2024-07-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27441\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27441\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27441","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Isolated peripheral nervous system relapse after allogeneic hematopoietic cell transplantation for T-cell acute lymphoblastic leukemia
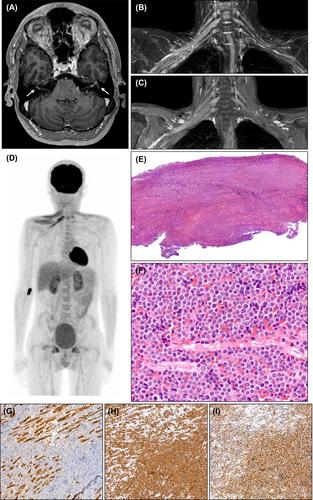
A 23-year-old man was admitted with left peripheral facial nerve palsy and right C7 radiculopathy. Ten weeks prior, he had received an allogeneic hematopoietic stem cell transplant (allo-HSCT) for presumed peripheral nervous system (PNS) and cerebrospinal fluid (CSF) flow cytometry-confirmed central nervous system (CNS) relapse of T-cell acute lymphoblastic leukemia (T-ALL). CNS MRI showed bilateral peripheral facial nerve enhancement without evidence of leptomeningeal or spinal disease (Figure 1A). CSF flow cytometry, viral PCRs, and bacterial cultures were unrevealing on multiple occasions. MRI of the brachial plexus showed diffuse nerve root thickening and edema with pathological enhancement, more pronounced on the right side (Figure 1B,C). Nerve conduction studies showed no evidence of demyelination. A total body PET/CT scan showed bilateral FDG accumulation in the brachial plexus, more pronounced on the right side (Figure 1D). Complete blood count was within normal limits with full donor chimerism. Bone marrow biopsy and flow cytometry excluded medullary relapse. Meanwhile, the patient experienced progressive pain, weakness, and muscle atrophy of the right arm requiring high-dose opioids and also developed right peripheral facial nerve palsy and similar symptomology of the left arm. High-dose intravenous immunoglobulins were ineffective. In an attempt to obtain a definitive diagnosis, the patient underwent surgical brachial plexus C7 biopsy. Hematoxylin and eosin staining showed effacement of normal nerve architecture with diffuse infiltration of blast-like cells (Figure 1E,F). S100 immunohistochemistry revealed sparse preexisting nerve fibers (Figure 1G). Blast-like cells were strongly positive for CD3 (Figure 1H) and TdT (Figure 1I), as well as CD10 and weakly positive for CD4 and CD8. MPO, PAX5 and CD30 were negative. A diagnosis of PNS relapse in the brachial plexus, and potentially facial nerves, was made. Without remaining curative treatment options, the patient received radiotherapy, resulting in substantial pain relief, and dexamethasone and was discharged home with palliative care.
The infiltration of peripheral nerves by leukemic blasts, termed neuroleukemiosis, is a rare neurological manifestation of leukemia with unknown incidence and no established diagnostic or therapeutic guidelines.1, 2 Biopsy-confirmed cases of neuroleukemiosis in T-ALL are only sparsely reported in the literature.3-7
The patient did not have CNS involvement at diagnosis but experienced a combined PNS and CNS relapse after intensive chemotherapy warranting allo-HSCT. Interestingly, relapse post-allo-HSCT was isolated to the PNS with similar symptomology as the pre-allo-HSCT relapse, suggesting that reinduction chemotherapy, myeloablative conditioning, and graft-versus-leukemia effect were more effective in eradicating CNS than PNS disease. Leukemic blasts can persists in the PNS for many years as exemplified by a case of acute monoblastic leukemia with isolated median nerve relapse after 12 years of remission.8 Isolated PNS relapse often precedes systemic relapse.1
Neuroleukemiosis is a rare clinical entity that should be included in the differential diagnosis of unexplained neurological deficits in patients with acute leukemia, even during remission. Isolated extramedullary relapse of the PNS is extremely rare and the PNS might serve as an sanctuary site for leukemic blasts and facilitate systemic relapse.1, 2
The authors have declared that no conflicts of interest exist.
The patient provided written informed consent for use of medical information and images in this case report. The signed informed consent form is available upon request.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


