Jawad Turfa, Ali Hijazi, Yasser Fadlallah, Melhem El-Harati, Hani Dimassi, Marwan El Najjar
{"title":"创伤性脑损伤开颅手术后 30 天死亡率和发病率的预测因素:ACS NSQIP 数据库分析。","authors":"Jawad Turfa, Ali Hijazi, Yasser Fadlallah, Melhem El-Harati, Hani Dimassi, Marwan El Najjar","doi":"10.1089/neur.2024.0039","DOIUrl":null,"url":null,"abstract":"<p><p>Traumatic brain injury (TBI) is the leading cause of death among trauma patients. Identifying preoperative factors that predict postoperative outcomes in such patients can guide surgical decision-making. The aim of this study was to develop a predictive model using preoperative variables that predicts 30-day mortality and morbidity in patients undergoing neurosurgery following TBI. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database was queried between 2005 and 2017 for patients aged 18 years or older who underwent TBI-specific surgery. The primary outcome was 30-day mortality, and the secondary outcome was a composite morbidity score. Significant variables on univariate analysis with Chi-squared test were used to compute multivariable logistic regression models for both outcomes, and Hosmer-Lemeshow test was used. A total of 1634 patients met the inclusion criteria. Most patients were elderly aged >60 years (74.48%), male (63.59%), of White race (73.62%), and non-Hispanic ethnicity (82.44%). The overall 30-day mortality rate was 20.3%. Using multivariate logistic regression, 11 preoperative variables were significantly associated with 30-day mortality, including (aOR, 95% CI) age 70-79 years (3.38, 2.03-5.62) and age >80 years (7.70, 4.74-12.51), ventilator dependency (6.04, 4.21-8.67), receiving dialysis (4.97, 2.43-10.18), disseminated cancer (4.42, 1.50-13.0), and coma >24 hours (3.30, 1.40-7.80), among others. Similarly, 12 preoperative variables were found to be significantly associated with 30-day morbidity, including acute renal failure (7.10, 1.91-26.32), return to OR (3.82, 2.77-5.27), sepsis (3.27, 1.11-9.66), prior operation within 30 days (2.55, 1.06-4.95), and insulin-dependent diabetes (1.60, 1.06-2.40), among others. After constructing receiver operating characteristic curve, the model for mortality had an area under the curve (AUC) of 0.843, whereas composite morbidity had an AUC of 0.716. This model can aid in clinical decision-making for triaging patients based on prognosis in cases of mass casualty events.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"5 1","pages":"660-670"},"PeriodicalIF":1.8000,"publicationDate":"2024-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11271074/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictors of 30-Day Mortality and Morbidity Following Craniotomy for Traumatic Brain Injury: An ACS NSQIP Database Analysis.\",\"authors\":\"Jawad Turfa, Ali Hijazi, Yasser Fadlallah, Melhem El-Harati, Hani Dimassi, Marwan El Najjar\",\"doi\":\"10.1089/neur.2024.0039\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Traumatic brain injury (TBI) is the leading cause of death among trauma patients. Identifying preoperative factors that predict postoperative outcomes in such patients can guide surgical decision-making. The aim of this study was to develop a predictive model using preoperative variables that predicts 30-day mortality and morbidity in patients undergoing neurosurgery following TBI. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database was queried between 2005 and 2017 for patients aged 18 years or older who underwent TBI-specific surgery. The primary outcome was 30-day mortality, and the secondary outcome was a composite morbidity score. Significant variables on univariate analysis with Chi-squared test were used to compute multivariable logistic regression models for both outcomes, and Hosmer-Lemeshow test was used. A total of 1634 patients met the inclusion criteria. Most patients were elderly aged >60 years (74.48%), male (63.59%), of White race (73.62%), and non-Hispanic ethnicity (82.44%). The overall 30-day mortality rate was 20.3%. Using multivariate logistic regression, 11 preoperative variables were significantly associated with 30-day mortality, including (aOR, 95% CI) age 70-79 years (3.38, 2.03-5.62) and age >80 years (7.70, 4.74-12.51), ventilator dependency (6.04, 4.21-8.67), receiving dialysis (4.97, 2.43-10.18), disseminated cancer (4.42, 1.50-13.0), and coma >24 hours (3.30, 1.40-7.80), among others. Similarly, 12 preoperative variables were found to be significantly associated with 30-day morbidity, including acute renal failure (7.10, 1.91-26.32), return to OR (3.82, 2.77-5.27), sepsis (3.27, 1.11-9.66), prior operation within 30 days (2.55, 1.06-4.95), and insulin-dependent diabetes (1.60, 1.06-2.40), among others. After constructing receiver operating characteristic curve, the model for mortality had an area under the curve (AUC) of 0.843, whereas composite morbidity had an AUC of 0.716. This model can aid in clinical decision-making for triaging patients based on prognosis in cases of mass casualty events.</p>\",\"PeriodicalId\":74300,\"journal\":{\"name\":\"Neurotrauma reports\",\"volume\":\"5 1\",\"pages\":\"660-670\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-07-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11271074/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurotrauma reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/neur.2024.0039\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2024.0039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Predictors of 30-Day Mortality and Morbidity Following Craniotomy for Traumatic Brain Injury: An ACS NSQIP Database Analysis.
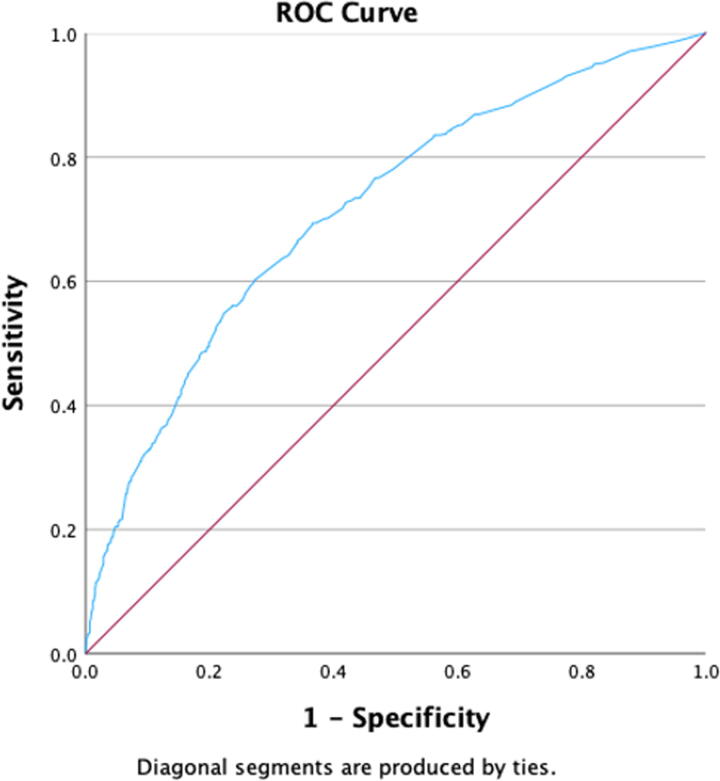
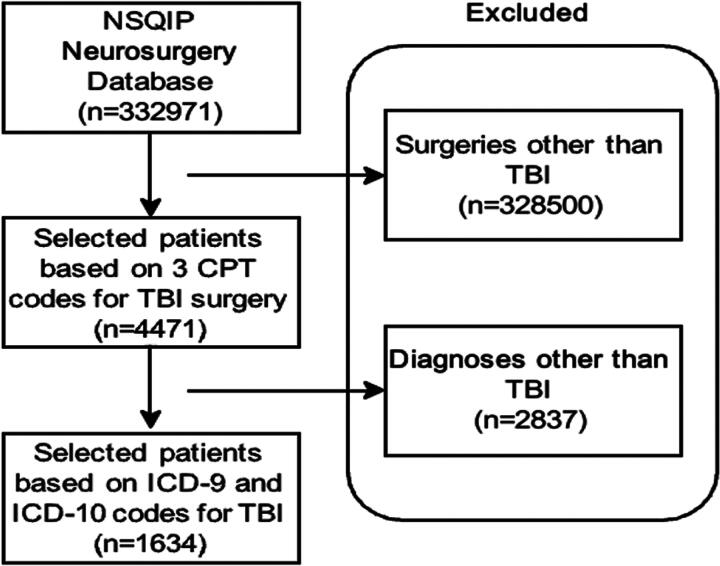
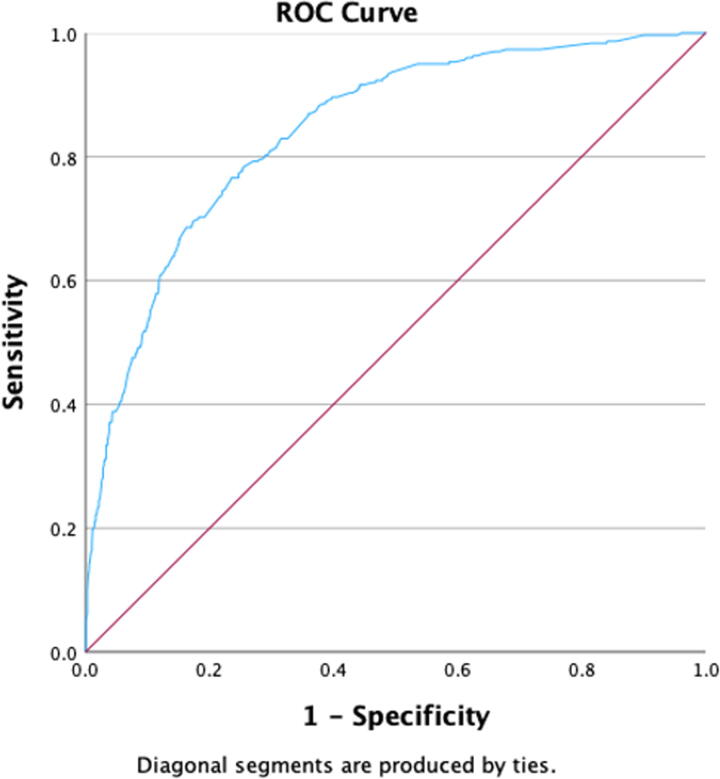
Traumatic brain injury (TBI) is the leading cause of death among trauma patients. Identifying preoperative factors that predict postoperative outcomes in such patients can guide surgical decision-making. The aim of this study was to develop a predictive model using preoperative variables that predicts 30-day mortality and morbidity in patients undergoing neurosurgery following TBI. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database was queried between 2005 and 2017 for patients aged 18 years or older who underwent TBI-specific surgery. The primary outcome was 30-day mortality, and the secondary outcome was a composite morbidity score. Significant variables on univariate analysis with Chi-squared test were used to compute multivariable logistic regression models for both outcomes, and Hosmer-Lemeshow test was used. A total of 1634 patients met the inclusion criteria. Most patients were elderly aged >60 years (74.48%), male (63.59%), of White race (73.62%), and non-Hispanic ethnicity (82.44%). The overall 30-day mortality rate was 20.3%. Using multivariate logistic regression, 11 preoperative variables were significantly associated with 30-day mortality, including (aOR, 95% CI) age 70-79 years (3.38, 2.03-5.62) and age >80 years (7.70, 4.74-12.51), ventilator dependency (6.04, 4.21-8.67), receiving dialysis (4.97, 2.43-10.18), disseminated cancer (4.42, 1.50-13.0), and coma >24 hours (3.30, 1.40-7.80), among others. Similarly, 12 preoperative variables were found to be significantly associated with 30-day morbidity, including acute renal failure (7.10, 1.91-26.32), return to OR (3.82, 2.77-5.27), sepsis (3.27, 1.11-9.66), prior operation within 30 days (2.55, 1.06-4.95), and insulin-dependent diabetes (1.60, 1.06-2.40), among others. After constructing receiver operating characteristic curve, the model for mortality had an area under the curve (AUC) of 0.843, whereas composite morbidity had an AUC of 0.716. This model can aid in clinical decision-making for triaging patients based on prognosis in cases of mass casualty events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


