Lyu Lyu, Cui Xv, Juan Xu, Zhenzhen Liu, Yanru He, Wenjing Zhu, Lin Lin, Qiang Yang, Yun Wei, Jinda Wang, Taoke Huang, Benchuan Hao, Hongbin Liu
{"title":"生长分化因子-15可预测冠心病患者的全因死亡和主要不良心血管事件:一项前瞻性队列研究。","authors":"Lyu Lyu, Cui Xv, Juan Xu, Zhenzhen Liu, Yanru He, Wenjing Zhu, Lin Lin, Qiang Yang, Yun Wei, Jinda Wang, Taoke Huang, Benchuan Hao, Hongbin Liu","doi":"10.1007/s11239-024-03019-5","DOIUrl":null,"url":null,"abstract":"<p><p>The prognostic value of growth differentiation factor-15 (GDF-15) in predicting long-term adverse outcomes in coronary heart disease (CHD) patients remains limited. Our study examines the association between GDF-15 and adverse outcomes over an extended period in CHD patients and firstly assesses the incremental prognostic effect of incorporating GDF-15 into the Framingham risk score (FRS)-based model. This single-center prospective cohort study included 3,321 patients with CHD categorized into 2,479 acute coronary syndrome (ACS) (74.6%) and 842 non-ACS (25.4%) groups. The median age was 61.0 years (range: 53.0-70.0), and 917 (27.6%) were females. Mortality and major adverse cardiovascular events (MACEs) included cardiovascular mortality, myocardial infarction (MI), stroke, and heart failure (HF) (inclusive of HF episodes requiring outpatient treatment and/or hospital admission). Cox regression models assessed the associations between GDF-15 and the incidence of all-cause mortality and MACEs. Patients were stratified into three groups based on GDF-15 levels: the first tertile group (< 1,370 ng/L), the second tertile group (1,370-2,556 ng/L), and the third tertile group (> 2,556 ng/L). The C-index, integrated discrimination improvement (IDI), net reclassification improvement (NRI), and decision curve analysis (DCA) were used to assess incremental value. Over a median 9.4-year follow-up, 759 patients (22.9%) died, and 1,291 (38.9%) experienced MACEs. The multivariate Cox model indicated that GDF-15 was significantly associated with all-cause mortality (per ln unit increase, HR = 1.49, 95% CI: 1.36-1.64) and MACEs (per ln unit increase, HR = 1.29, 95% CI: 1.20-1.38). These associations persisted when GDF-15 was analyzed as an ordinal variable (p for trend < 0.05). Subgroup analysis of ACS and non-ACS for the components of MACEs separately showed a significant association between GDF-15 and both cardiovascular mortality and HF, but no association was observed between GDF-15 and MI /stroke in both ACS and non-ACS patients. The addition of GDF-15 to the FRS-based model enhanced the discrimination for both all-cause mortality (∆ C-index = 0.009, 95% CI: 0.005-0.014; IDI = 0.030, 95% CI: 0.015-0.047; continuous NRI = 0.631, 95% CI: 0.569-0.652) and MACEs (∆ C-index = 0.009, 95% CI: 0.006-0.012; IDI = 0.026, 95% CI: 0.009-0.042; continuous NRI = 0.593, 95% CI: 0.478-0.682). DCA suggested that incorporating GDF-15 into the FRS-based model demonstrated higher net benefits compared to FRS-based models alone (All-cause mortality: FRS-based model: area under the curve of DCA (AUDC) = 0.0903, FRS-based model + GDF-15: AUDC = 0.0908; MACEs: FRS-based model: AUDC = 0.1806, FRS-based model + GDF-15: AUDC = 0.1833). GDF-15 significantly associates with the long-term prognosis of all-cause mortality and MACEs in CHD patients and significantly improves the prognostic accuracy of the FRS-based model for both outcomes.</p>","PeriodicalId":17546,"journal":{"name":"Journal of Thrombosis and Thrombolysis","volume":" ","pages":"1109-1121"},"PeriodicalIF":2.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Growth differentiation factor-15 predicts all-cause death and major adverse cardiovascular events in patients with coronary heart disease: a prospective cohort study.\",\"authors\":\"Lyu Lyu, Cui Xv, Juan Xu, Zhenzhen Liu, Yanru He, Wenjing Zhu, Lin Lin, Qiang Yang, Yun Wei, Jinda Wang, Taoke Huang, Benchuan Hao, Hongbin Liu\",\"doi\":\"10.1007/s11239-024-03019-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The prognostic value of growth differentiation factor-15 (GDF-15) in predicting long-term adverse outcomes in coronary heart disease (CHD) patients remains limited. Our study examines the association between GDF-15 and adverse outcomes over an extended period in CHD patients and firstly assesses the incremental prognostic effect of incorporating GDF-15 into the Framingham risk score (FRS)-based model. This single-center prospective cohort study included 3,321 patients with CHD categorized into 2,479 acute coronary syndrome (ACS) (74.6%) and 842 non-ACS (25.4%) groups. The median age was 61.0 years (range: 53.0-70.0), and 917 (27.6%) were females. Mortality and major adverse cardiovascular events (MACEs) included cardiovascular mortality, myocardial infarction (MI), stroke, and heart failure (HF) (inclusive of HF episodes requiring outpatient treatment and/or hospital admission). Cox regression models assessed the associations between GDF-15 and the incidence of all-cause mortality and MACEs. Patients were stratified into three groups based on GDF-15 levels: the first tertile group (< 1,370 ng/L), the second tertile group (1,370-2,556 ng/L), and the third tertile group (> 2,556 ng/L). The C-index, integrated discrimination improvement (IDI), net reclassification improvement (NRI), and decision curve analysis (DCA) were used to assess incremental value. Over a median 9.4-year follow-up, 759 patients (22.9%) died, and 1,291 (38.9%) experienced MACEs. The multivariate Cox model indicated that GDF-15 was significantly associated with all-cause mortality (per ln unit increase, HR = 1.49, 95% CI: 1.36-1.64) and MACEs (per ln unit increase, HR = 1.29, 95% CI: 1.20-1.38). These associations persisted when GDF-15 was analyzed as an ordinal variable (p for trend < 0.05). Subgroup analysis of ACS and non-ACS for the components of MACEs separately showed a significant association between GDF-15 and both cardiovascular mortality and HF, but no association was observed between GDF-15 and MI /stroke in both ACS and non-ACS patients. The addition of GDF-15 to the FRS-based model enhanced the discrimination for both all-cause mortality (∆ C-index = 0.009, 95% CI: 0.005-0.014; IDI = 0.030, 95% CI: 0.015-0.047; continuous NRI = 0.631, 95% CI: 0.569-0.652) and MACEs (∆ C-index = 0.009, 95% CI: 0.006-0.012; IDI = 0.026, 95% CI: 0.009-0.042; continuous NRI = 0.593, 95% CI: 0.478-0.682). DCA suggested that incorporating GDF-15 into the FRS-based model demonstrated higher net benefits compared to FRS-based models alone (All-cause mortality: FRS-based model: area under the curve of DCA (AUDC) = 0.0903, FRS-based model + GDF-15: AUDC = 0.0908; MACEs: FRS-based model: AUDC = 0.1806, FRS-based model + GDF-15: AUDC = 0.1833). GDF-15 significantly associates with the long-term prognosis of all-cause mortality and MACEs in CHD patients and significantly improves the prognostic accuracy of the FRS-based model for both outcomes.</p>\",\"PeriodicalId\":17546,\"journal\":{\"name\":\"Journal of Thrombosis and Thrombolysis\",\"volume\":\" \",\"pages\":\"1109-1121\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Thrombosis and Thrombolysis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11239-024-03019-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thrombosis and Thrombolysis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11239-024-03019-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Growth differentiation factor-15 predicts all-cause death and major adverse cardiovascular events in patients with coronary heart disease: a prospective cohort study.
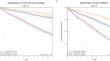
The prognostic value of growth differentiation factor-15 (GDF-15) in predicting long-term adverse outcomes in coronary heart disease (CHD) patients remains limited. Our study examines the association between GDF-15 and adverse outcomes over an extended period in CHD patients and firstly assesses the incremental prognostic effect of incorporating GDF-15 into the Framingham risk score (FRS)-based model. This single-center prospective cohort study included 3,321 patients with CHD categorized into 2,479 acute coronary syndrome (ACS) (74.6%) and 842 non-ACS (25.4%) groups. The median age was 61.0 years (range: 53.0-70.0), and 917 (27.6%) were females. Mortality and major adverse cardiovascular events (MACEs) included cardiovascular mortality, myocardial infarction (MI), stroke, and heart failure (HF) (inclusive of HF episodes requiring outpatient treatment and/or hospital admission). Cox regression models assessed the associations between GDF-15 and the incidence of all-cause mortality and MACEs. Patients were stratified into three groups based on GDF-15 levels: the first tertile group (< 1,370 ng/L), the second tertile group (1,370-2,556 ng/L), and the third tertile group (> 2,556 ng/L). The C-index, integrated discrimination improvement (IDI), net reclassification improvement (NRI), and decision curve analysis (DCA) were used to assess incremental value. Over a median 9.4-year follow-up, 759 patients (22.9%) died, and 1,291 (38.9%) experienced MACEs. The multivariate Cox model indicated that GDF-15 was significantly associated with all-cause mortality (per ln unit increase, HR = 1.49, 95% CI: 1.36-1.64) and MACEs (per ln unit increase, HR = 1.29, 95% CI: 1.20-1.38). These associations persisted when GDF-15 was analyzed as an ordinal variable (p for trend < 0.05). Subgroup analysis of ACS and non-ACS for the components of MACEs separately showed a significant association between GDF-15 and both cardiovascular mortality and HF, but no association was observed between GDF-15 and MI /stroke in both ACS and non-ACS patients. The addition of GDF-15 to the FRS-based model enhanced the discrimination for both all-cause mortality (∆ C-index = 0.009, 95% CI: 0.005-0.014; IDI = 0.030, 95% CI: 0.015-0.047; continuous NRI = 0.631, 95% CI: 0.569-0.652) and MACEs (∆ C-index = 0.009, 95% CI: 0.006-0.012; IDI = 0.026, 95% CI: 0.009-0.042; continuous NRI = 0.593, 95% CI: 0.478-0.682). DCA suggested that incorporating GDF-15 into the FRS-based model demonstrated higher net benefits compared to FRS-based models alone (All-cause mortality: FRS-based model: area under the curve of DCA (AUDC) = 0.0903, FRS-based model + GDF-15: AUDC = 0.0908; MACEs: FRS-based model: AUDC = 0.1806, FRS-based model + GDF-15: AUDC = 0.1833). GDF-15 significantly associates with the long-term prognosis of all-cause mortality and MACEs in CHD patients and significantly improves the prognostic accuracy of the FRS-based model for both outcomes.
期刊介绍:
The Journal of Thrombosis and Thrombolysis is a long-awaited resource for contemporary cardiologists, hematologists, vascular medicine specialists and clinician-scientists actively involved in treatment decisions and clinical investigation of thrombotic disorders involving the cardiovascular and cerebrovascular systems. The principal focus of the Journal centers on the pathobiology of thrombosis and vascular disorders and the use of anticoagulants, platelet antagonists, cell-based therapies and interventions in scientific investigation, clinical-translational research and patient care.
The Journal will publish original work which emphasizes the interface between fundamental scientific principles and clinical investigation, stimulating an interdisciplinary and scholarly dialogue in thrombosis and vascular science. Published works will also define platforms for translational research, drug development, clinical trials and patient-directed applications. The Journal of Thrombosis and Thrombolysis'' integrated format will expand the reader''s knowledge base and provide important insights for both the investigation and direct clinical application of the most rapidly growing fields in medicine-thrombosis and vascular science.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


