{"title":"孤立性输卵管扭转:青春期急性盆腔疼痛的罕见病因。","authors":"Khaoula Magdoud, Hiba Mkadmi, Fatma Moussa, Zeineb Ghali, Sana Menjli, Abir Karoui","doi":"10.1111/jpc.16629","DOIUrl":null,"url":null,"abstract":"<p>Isolated fallopian tube torsion is a rare surgical emergency in adolescent girls, with an estimated incidence of one in 1 500 000 cases.<span><sup>1</sup></span> The clinical representation is not specific, leading to challenging and delayed diagnosis, often made intraoperatively. Conservative surgical management is uncommon in these young patients due to late diagnosis.<span><sup>1</sup></span> This work aims to recall the main characteristics of isolated fallopian tube torsion through a clinical case that successfully underwent conservative treatment.</p><p>We report the case of isolated fallopian tube torsion in a 14-year-old girl who consulted the hospital's emergency department due to sudden pain in the right iliac fossa. The pain has been ongoing for 8 h without radiation to other parts of the body and associated with an episode of vomiting without transit disorder or urinary functional signs. A similar episode that resolved spontaneously 3 months ago was reported. This patient has no medical or surgical history. No abdominal or pelvic trauma was reported. She was a virgin. Menarche occurred at the age of 12 years with irregular cycles. She was on the 25th day of her menstrual cycle.</p><p>On physical examination, the patient was apyretic and haemodynamically stable. Urine Multistix analysis was negative. Abdominal examination revealed a right iliac fossa defence, without palpable mass or abdominal contracture. The lumbar fossa was not tender. The digital rectal examination did not trigger pain. The gynaecological examination was not performed.</p><p>Suprapubic pelvic ultrasound, conducted with a full bladder, showed a normal uterus, and left ovary. The assessment of the right adnexa revealed a unilocular rounded anechoic mass with a regular and thin wall, without vegetation, non-vascularised by colour Doppler, measuring 50 mm in diameter.</p><p>No inflammatory syndrome in biology was found. Serum β-human chorionic gonadotropin (HCG) level was negative.</p><p>The diagnosis of right adnexal torsion was evoked. The patient underwent an emergency laparoscopy.</p><p>On examination, the uterus and left adnexa were normal in appearance. There was a bluish, 5-cm rounded, juxta-uterine mass with fringes, suggesting an isolated torsion of the right fallopian tube, coiling around the utero-ovarian ligament four times in clockwise direction, with ipsilateral unaffected right ovary. No cysts, especially in the mesosalpinx, were found. The appendix was normal (Fig. 1).</p><p>The right fallopian tube was then untwisted. A progressive recoloration was noted after about 10 min of observation and uncoiled tubal recovery was satisfactory (Fig. 2). The right fallopian tube appeared to be abnormally elongated. Conservative treatment with saline solution cleansing and post-operative antibiotic coverage was conducted.</p><p>The post-operative follow-up was uneventful. The patient was fully and clearly informed of her condition. A detailed medical report was delivered.</p><p>The clinical presentation of isolated fallopian tube torsion is misleading, and often misdiagnosed as adnexal torsion.<span><sup>2</sup></span> However, semiology is crucial for the diagnostic orientation towards isolated tubal torsion. The pain usually occurs acutely and is frequently accompanied by one or more episodes of nausea and vomiting.<span><sup>3</sup></span></p><p>It seems that isolated tubal torsion is more common in younger women, especially adolescent girls, compared to adnexal torsion.<span><sup>4</sup></span></p><p>Isolated torsion of the tube does not have pathognomonic symptoms. Acute pelvic pain appears to be the most common clinical presentation.<span><sup>5</sup></span></p><p>Besides, spontaneously resolved ipsilateral iliac fossa pain episode may evoke a previous sub-torsion.</p><p>There are two possible courses of evolution for the pain episode. The first one is subacute type, in which there are some deferred symptoms and thereby delay in the intervention. The other one is acute type, in which there is severe abdominal pain, indicating the need for an emergency surgery.</p><p>Multiple and repeated abdominal palpation to assess the abdominal defence are essential, reflecting the degree of the tube's ischemia, adversely affecting its viability prognosis.</p><p>However, a pelvic mass might be discerned on palpation as well as through pelvic examination.<span><sup>1</sup></span></p><p>In a woman of childbearing age, ectopic pregnancy is systematically considered and typically ruled out using β-HCG assay and pelvic ultrasound.</p><p>The diagnosis of isolated fallopian tube torsion in a young girl is challenging. In this context, it is commonly primordial to rule out acute appendicitis, which is more frequent and consistently considered in the presence of right iliac fossa pain among this population.</p><p>Abdominal, and specifically transvaginal, ultrasound is the gold standard for exploring acute pelvic pain in adolescent girls. It implies locating the ovaries and then looking for a mass, which is most often located between the ovary and the uterine horn. It may sometimes be found in Douglas' cul-de-sac. Initially, the mass is homogeneous and progressively becomes heterogeneous at a more advanced stage, reflecting the presence of areas of haemorrhagic necrosis.<span><sup>6</sup></span> The walls may have thickened due to epithelial oedema.</p><p>In addition, computed tomography and magnetic resonance imaging have not shown their superiority over ultrasound in diagnosis terms.<span><sup>6</sup></span></p><p>Isolated tubal torsion more frequently occurs on the right side. Indeed, the torsion mechanism on the left side is thought to be limited by the presence of the sigmoid colon.<span><sup>7</sup></span></p><p>The underlying mechanisms of isolated fallopian tube torsion are not yet fully understood and seem to be the result of a combination of an anatomical triggering factor and a hemodynamic factor that sustains this process.<span><sup>8</sup></span></p><p>Then there are the hemodynamic factors as follows: The mesosalpinx veins are longer and more flexible than the arteries. When a twist occurs, these veins become congested, facilitating further spiralisation.</p><p>Besides, other aetiologies have been reported in the literature such as tubal hyperperistalsis, tubal sterilisation (especially according to the Pomeroy technique) or abdominal trauma.</p><p>In adolescents, the main risk factors for this condition are mainly congenital hydrosalpinx and sports that involve sudden movements.<span><sup>3</sup></span></p><p>In our observation, the aetiology was most likely excessive length of the mesosalpinx.</p><p>Finally, the treatment of isolated tubal torsion is laparoscopic surgery. It involves untwisting the fallopian tube and assessing its revascularisation after potential warming with saline solution. If revascularisation does not occur, a salpingectomy will be performed.<span><sup>4</sup></span></p><p>Salpingectomy, given the delayed diagnosis, was the most reported treatment in the literature.</p><p>The preservation of the fallopian tube could be discussed even in the case of a persistent necrotic and haemorrhagic appearance.<span><sup>4</sup></span></p><p>The approach to the contralateral adnexa is controversial as bilateral involvement is considered to be rare. In any case, regular monitoring and informing the patient are required.</p><p>Isolated tubal torsion is a rare surgical emergency in adolescent girls. It is underestimated due to the misleading clinical presentation and the non-specificity of imaging tests. The diagnosis should be systematically considered in cases of pelvic pain, as it can impact the fertility prognosis of these young patients. Improving the knowledge and awareness of gynaecologists about this condition can improve the management of these adolescent girls.</p><p>Ethical approval is considered unnecessary by the ethics committee of the hospital centre, because this is a unique case encountered during practice and which does not involve any experimentation on humans or animals.</p><p>We had written consent from parents for the publication of the article and images.</p>","PeriodicalId":16648,"journal":{"name":"Journal of paediatrics and child health","volume":"60 10","pages":"601-603"},"PeriodicalIF":1.6000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16629","citationCount":"0","resultStr":"{\"title\":\"Isolated fallopian tube torsion: A rare cause of acute pelvic pain in adolescence\",\"authors\":\"Khaoula Magdoud, Hiba Mkadmi, Fatma Moussa, Zeineb Ghali, Sana Menjli, Abir Karoui\",\"doi\":\"10.1111/jpc.16629\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Isolated fallopian tube torsion is a rare surgical emergency in adolescent girls, with an estimated incidence of one in 1 500 000 cases.<span><sup>1</sup></span> The clinical representation is not specific, leading to challenging and delayed diagnosis, often made intraoperatively. Conservative surgical management is uncommon in these young patients due to late diagnosis.<span><sup>1</sup></span> This work aims to recall the main characteristics of isolated fallopian tube torsion through a clinical case that successfully underwent conservative treatment.</p><p>We report the case of isolated fallopian tube torsion in a 14-year-old girl who consulted the hospital's emergency department due to sudden pain in the right iliac fossa. The pain has been ongoing for 8 h without radiation to other parts of the body and associated with an episode of vomiting without transit disorder or urinary functional signs. A similar episode that resolved spontaneously 3 months ago was reported. This patient has no medical or surgical history. No abdominal or pelvic trauma was reported. She was a virgin. Menarche occurred at the age of 12 years with irregular cycles. She was on the 25th day of her menstrual cycle.</p><p>On physical examination, the patient was apyretic and haemodynamically stable. Urine Multistix analysis was negative. Abdominal examination revealed a right iliac fossa defence, without palpable mass or abdominal contracture. The lumbar fossa was not tender. The digital rectal examination did not trigger pain. The gynaecological examination was not performed.</p><p>Suprapubic pelvic ultrasound, conducted with a full bladder, showed a normal uterus, and left ovary. The assessment of the right adnexa revealed a unilocular rounded anechoic mass with a regular and thin wall, without vegetation, non-vascularised by colour Doppler, measuring 50 mm in diameter.</p><p>No inflammatory syndrome in biology was found. Serum β-human chorionic gonadotropin (HCG) level was negative.</p><p>The diagnosis of right adnexal torsion was evoked. The patient underwent an emergency laparoscopy.</p><p>On examination, the uterus and left adnexa were normal in appearance. There was a bluish, 5-cm rounded, juxta-uterine mass with fringes, suggesting an isolated torsion of the right fallopian tube, coiling around the utero-ovarian ligament four times in clockwise direction, with ipsilateral unaffected right ovary. No cysts, especially in the mesosalpinx, were found. The appendix was normal (Fig. 1).</p><p>The right fallopian tube was then untwisted. A progressive recoloration was noted after about 10 min of observation and uncoiled tubal recovery was satisfactory (Fig. 2). The right fallopian tube appeared to be abnormally elongated. Conservative treatment with saline solution cleansing and post-operative antibiotic coverage was conducted.</p><p>The post-operative follow-up was uneventful. The patient was fully and clearly informed of her condition. A detailed medical report was delivered.</p><p>The clinical presentation of isolated fallopian tube torsion is misleading, and often misdiagnosed as adnexal torsion.<span><sup>2</sup></span> However, semiology is crucial for the diagnostic orientation towards isolated tubal torsion. The pain usually occurs acutely and is frequently accompanied by one or more episodes of nausea and vomiting.<span><sup>3</sup></span></p><p>It seems that isolated tubal torsion is more common in younger women, especially adolescent girls, compared to adnexal torsion.<span><sup>4</sup></span></p><p>Isolated torsion of the tube does not have pathognomonic symptoms. Acute pelvic pain appears to be the most common clinical presentation.<span><sup>5</sup></span></p><p>Besides, spontaneously resolved ipsilateral iliac fossa pain episode may evoke a previous sub-torsion.</p><p>There are two possible courses of evolution for the pain episode. The first one is subacute type, in which there are some deferred symptoms and thereby delay in the intervention. The other one is acute type, in which there is severe abdominal pain, indicating the need for an emergency surgery.</p><p>Multiple and repeated abdominal palpation to assess the abdominal defence are essential, reflecting the degree of the tube's ischemia, adversely affecting its viability prognosis.</p><p>However, a pelvic mass might be discerned on palpation as well as through pelvic examination.<span><sup>1</sup></span></p><p>In a woman of childbearing age, ectopic pregnancy is systematically considered and typically ruled out using β-HCG assay and pelvic ultrasound.</p><p>The diagnosis of isolated fallopian tube torsion in a young girl is challenging. In this context, it is commonly primordial to rule out acute appendicitis, which is more frequent and consistently considered in the presence of right iliac fossa pain among this population.</p><p>Abdominal, and specifically transvaginal, ultrasound is the gold standard for exploring acute pelvic pain in adolescent girls. It implies locating the ovaries and then looking for a mass, which is most often located between the ovary and the uterine horn. It may sometimes be found in Douglas' cul-de-sac. Initially, the mass is homogeneous and progressively becomes heterogeneous at a more advanced stage, reflecting the presence of areas of haemorrhagic necrosis.<span><sup>6</sup></span> The walls may have thickened due to epithelial oedema.</p><p>In addition, computed tomography and magnetic resonance imaging have not shown their superiority over ultrasound in diagnosis terms.<span><sup>6</sup></span></p><p>Isolated tubal torsion more frequently occurs on the right side. Indeed, the torsion mechanism on the left side is thought to be limited by the presence of the sigmoid colon.<span><sup>7</sup></span></p><p>The underlying mechanisms of isolated fallopian tube torsion are not yet fully understood and seem to be the result of a combination of an anatomical triggering factor and a hemodynamic factor that sustains this process.<span><sup>8</sup></span></p><p>Then there are the hemodynamic factors as follows: The mesosalpinx veins are longer and more flexible than the arteries. When a twist occurs, these veins become congested, facilitating further spiralisation.</p><p>Besides, other aetiologies have been reported in the literature such as tubal hyperperistalsis, tubal sterilisation (especially according to the Pomeroy technique) or abdominal trauma.</p><p>In adolescents, the main risk factors for this condition are mainly congenital hydrosalpinx and sports that involve sudden movements.<span><sup>3</sup></span></p><p>In our observation, the aetiology was most likely excessive length of the mesosalpinx.</p><p>Finally, the treatment of isolated tubal torsion is laparoscopic surgery. It involves untwisting the fallopian tube and assessing its revascularisation after potential warming with saline solution. If revascularisation does not occur, a salpingectomy will be performed.<span><sup>4</sup></span></p><p>Salpingectomy, given the delayed diagnosis, was the most reported treatment in the literature.</p><p>The preservation of the fallopian tube could be discussed even in the case of a persistent necrotic and haemorrhagic appearance.<span><sup>4</sup></span></p><p>The approach to the contralateral adnexa is controversial as bilateral involvement is considered to be rare. In any case, regular monitoring and informing the patient are required.</p><p>Isolated tubal torsion is a rare surgical emergency in adolescent girls. It is underestimated due to the misleading clinical presentation and the non-specificity of imaging tests. The diagnosis should be systematically considered in cases of pelvic pain, as it can impact the fertility prognosis of these young patients. Improving the knowledge and awareness of gynaecologists about this condition can improve the management of these adolescent girls.</p><p>Ethical approval is considered unnecessary by the ethics committee of the hospital centre, because this is a unique case encountered during practice and which does not involve any experimentation on humans or animals.</p><p>We had written consent from parents for the publication of the article and images.</p>\",\"PeriodicalId\":16648,\"journal\":{\"name\":\"Journal of paediatrics and child health\",\"volume\":\"60 10\",\"pages\":\"601-603\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16629\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of paediatrics and child health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16629\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of paediatrics and child health","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16629","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Isolated fallopian tube torsion: A rare cause of acute pelvic pain in adolescence
Isolated fallopian tube torsion is a rare surgical emergency in adolescent girls, with an estimated incidence of one in 1 500 000 cases.1 The clinical representation is not specific, leading to challenging and delayed diagnosis, often made intraoperatively. Conservative surgical management is uncommon in these young patients due to late diagnosis.1 This work aims to recall the main characteristics of isolated fallopian tube torsion through a clinical case that successfully underwent conservative treatment.
We report the case of isolated fallopian tube torsion in a 14-year-old girl who consulted the hospital's emergency department due to sudden pain in the right iliac fossa. The pain has been ongoing for 8 h without radiation to other parts of the body and associated with an episode of vomiting without transit disorder or urinary functional signs. A similar episode that resolved spontaneously 3 months ago was reported. This patient has no medical or surgical history. No abdominal or pelvic trauma was reported. She was a virgin. Menarche occurred at the age of 12 years with irregular cycles. She was on the 25th day of her menstrual cycle.
On physical examination, the patient was apyretic and haemodynamically stable. Urine Multistix analysis was negative. Abdominal examination revealed a right iliac fossa defence, without palpable mass or abdominal contracture. The lumbar fossa was not tender. The digital rectal examination did not trigger pain. The gynaecological examination was not performed.
Suprapubic pelvic ultrasound, conducted with a full bladder, showed a normal uterus, and left ovary. The assessment of the right adnexa revealed a unilocular rounded anechoic mass with a regular and thin wall, without vegetation, non-vascularised by colour Doppler, measuring 50 mm in diameter.
No inflammatory syndrome in biology was found. Serum β-human chorionic gonadotropin (HCG) level was negative.
The diagnosis of right adnexal torsion was evoked. The patient underwent an emergency laparoscopy.
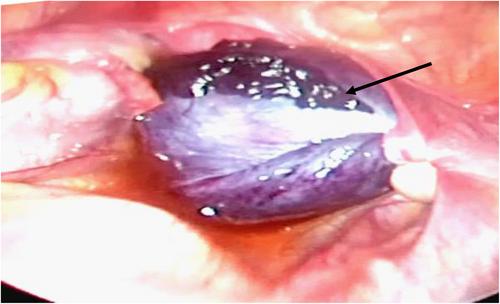
On examination, the uterus and left adnexa were normal in appearance. There was a bluish, 5-cm rounded, juxta-uterine mass with fringes, suggesting an isolated torsion of the right fallopian tube, coiling around the utero-ovarian ligament four times in clockwise direction, with ipsilateral unaffected right ovary. No cysts, especially in the mesosalpinx, were found. The appendix was normal (Fig. 1).
The right fallopian tube was then untwisted. A progressive recoloration was noted after about 10 min of observation and uncoiled tubal recovery was satisfactory (Fig. 2). The right fallopian tube appeared to be abnormally elongated. Conservative treatment with saline solution cleansing and post-operative antibiotic coverage was conducted.
The post-operative follow-up was uneventful. The patient was fully and clearly informed of her condition. A detailed medical report was delivered.
The clinical presentation of isolated fallopian tube torsion is misleading, and often misdiagnosed as adnexal torsion.2 However, semiology is crucial for the diagnostic orientation towards isolated tubal torsion. The pain usually occurs acutely and is frequently accompanied by one or more episodes of nausea and vomiting.3
It seems that isolated tubal torsion is more common in younger women, especially adolescent girls, compared to adnexal torsion.4
Isolated torsion of the tube does not have pathognomonic symptoms. Acute pelvic pain appears to be the most common clinical presentation.5
Besides, spontaneously resolved ipsilateral iliac fossa pain episode may evoke a previous sub-torsion.
There are two possible courses of evolution for the pain episode. The first one is subacute type, in which there are some deferred symptoms and thereby delay in the intervention. The other one is acute type, in which there is severe abdominal pain, indicating the need for an emergency surgery.
Multiple and repeated abdominal palpation to assess the abdominal defence are essential, reflecting the degree of the tube's ischemia, adversely affecting its viability prognosis.
However, a pelvic mass might be discerned on palpation as well as through pelvic examination.1
In a woman of childbearing age, ectopic pregnancy is systematically considered and typically ruled out using β-HCG assay and pelvic ultrasound.
The diagnosis of isolated fallopian tube torsion in a young girl is challenging. In this context, it is commonly primordial to rule out acute appendicitis, which is more frequent and consistently considered in the presence of right iliac fossa pain among this population.
Abdominal, and specifically transvaginal, ultrasound is the gold standard for exploring acute pelvic pain in adolescent girls. It implies locating the ovaries and then looking for a mass, which is most often located between the ovary and the uterine horn. It may sometimes be found in Douglas' cul-de-sac. Initially, the mass is homogeneous and progressively becomes heterogeneous at a more advanced stage, reflecting the presence of areas of haemorrhagic necrosis.6 The walls may have thickened due to epithelial oedema.
In addition, computed tomography and magnetic resonance imaging have not shown their superiority over ultrasound in diagnosis terms.6
Isolated tubal torsion more frequently occurs on the right side. Indeed, the torsion mechanism on the left side is thought to be limited by the presence of the sigmoid colon.7
The underlying mechanisms of isolated fallopian tube torsion are not yet fully understood and seem to be the result of a combination of an anatomical triggering factor and a hemodynamic factor that sustains this process.8
Then there are the hemodynamic factors as follows: The mesosalpinx veins are longer and more flexible than the arteries. When a twist occurs, these veins become congested, facilitating further spiralisation.
Besides, other aetiologies have been reported in the literature such as tubal hyperperistalsis, tubal sterilisation (especially according to the Pomeroy technique) or abdominal trauma.
In adolescents, the main risk factors for this condition are mainly congenital hydrosalpinx and sports that involve sudden movements.3
In our observation, the aetiology was most likely excessive length of the mesosalpinx.
Finally, the treatment of isolated tubal torsion is laparoscopic surgery. It involves untwisting the fallopian tube and assessing its revascularisation after potential warming with saline solution. If revascularisation does not occur, a salpingectomy will be performed.4
Salpingectomy, given the delayed diagnosis, was the most reported treatment in the literature.
The preservation of the fallopian tube could be discussed even in the case of a persistent necrotic and haemorrhagic appearance.4
The approach to the contralateral adnexa is controversial as bilateral involvement is considered to be rare. In any case, regular monitoring and informing the patient are required.
Isolated tubal torsion is a rare surgical emergency in adolescent girls. It is underestimated due to the misleading clinical presentation and the non-specificity of imaging tests. The diagnosis should be systematically considered in cases of pelvic pain, as it can impact the fertility prognosis of these young patients. Improving the knowledge and awareness of gynaecologists about this condition can improve the management of these adolescent girls.
Ethical approval is considered unnecessary by the ethics committee of the hospital centre, because this is a unique case encountered during practice and which does not involve any experimentation on humans or animals.
We had written consent from parents for the publication of the article and images.
期刊介绍:
The Journal of Paediatrics and Child Health publishes original research articles of scientific excellence in paediatrics and child health. Research Articles, Case Reports and Letters to the Editor are published, together with invited Reviews, Annotations, Editorial Comments and manuscripts of educational interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


