Justin J Song, Nicholas J Jackson, Helen Shang, Henry M Honda, Kristin Boulier
{"title":"评估肝硬化患者心房颤动抗凝治疗的安全性:真实世界结果研究","authors":"Justin J Song, Nicholas J Jackson, Helen Shang, Henry M Honda, Kristin Boulier","doi":"10.1177/10742484241256271","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>In patients with atrial fibrillation (AF) and stroke risk factors, randomized trials have demonstrated that anticoagulation decreases the risk of ischemic stroke. However, all trials to date have excluded patients with significant liver disease, leaving guidelines to extrapolate recommendations. We aim to evaluate the impact of anticoagulation on safety events in patients with AF and cirrhosis.</p><p><strong>Methods and results: </strong>In this retrospective cohort study, we obtained de-identified health record data to extract anticoagulation strategy, comorbidities, prescriptions, lab values, and procedures for a cohort of patients with cirrhosis who develop AF. After selecting a propensity matched population to match patients with various anticoagulation strategies, we tracked data on outcomes for death, transfusion requirements, hospital and ICU admissions. After propensity score weighting and multivariable adjustment, anticoagulation strategy was associated with increased hospital admission count (OR = 1.74 per admission, <i>P</i> < .001), binary risk of hospital admission (OR = 1.54, <i>P</i> = .010) and risk of ICU admission (OR = 1.41, <i>P</i> = .047). We detected no significant differences in mortality, transfusion of blood products, or average length of stay. Direct oral anticoagulant (DOAC) prescriptions were associated with increased binary risk of hospital admission compared to warfarin prescriptions. In a third comparison, DOAC strategy alone was associated with increased hospital admission count (OR = 1.41 per admission, <i>P</i> < .001) and binary risk of hospital admission (OR = 1.52, <i>P</i> = .038) compared to no anticoagulation strategy.</p><p><strong>Conclusion: </strong>Anticoagulation strategy in patients with cirrhosis and AF was associated with increased rate of hospital admission and ICU admission but not associated with increased risk of mortality or transfusion requirement.</p>","PeriodicalId":15281,"journal":{"name":"Journal of Cardiovascular Pharmacology and Therapeutics","volume":"29 ","pages":"10742484241256271"},"PeriodicalIF":2.8000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11981305/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessing Safety of Anticoagulation for Atrial Fibrillation in Patients with Cirrhosis: A Real-World Outcomes Study.\",\"authors\":\"Justin J Song, Nicholas J Jackson, Helen Shang, Henry M Honda, Kristin Boulier\",\"doi\":\"10.1177/10742484241256271\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>In patients with atrial fibrillation (AF) and stroke risk factors, randomized trials have demonstrated that anticoagulation decreases the risk of ischemic stroke. However, all trials to date have excluded patients with significant liver disease, leaving guidelines to extrapolate recommendations. We aim to evaluate the impact of anticoagulation on safety events in patients with AF and cirrhosis.</p><p><strong>Methods and results: </strong>In this retrospective cohort study, we obtained de-identified health record data to extract anticoagulation strategy, comorbidities, prescriptions, lab values, and procedures for a cohort of patients with cirrhosis who develop AF. After selecting a propensity matched population to match patients with various anticoagulation strategies, we tracked data on outcomes for death, transfusion requirements, hospital and ICU admissions. After propensity score weighting and multivariable adjustment, anticoagulation strategy was associated with increased hospital admission count (OR = 1.74 per admission, <i>P</i> < .001), binary risk of hospital admission (OR = 1.54, <i>P</i> = .010) and risk of ICU admission (OR = 1.41, <i>P</i> = .047). We detected no significant differences in mortality, transfusion of blood products, or average length of stay. Direct oral anticoagulant (DOAC) prescriptions were associated with increased binary risk of hospital admission compared to warfarin prescriptions. In a third comparison, DOAC strategy alone was associated with increased hospital admission count (OR = 1.41 per admission, <i>P</i> < .001) and binary risk of hospital admission (OR = 1.52, <i>P</i> = .038) compared to no anticoagulation strategy.</p><p><strong>Conclusion: </strong>Anticoagulation strategy in patients with cirrhosis and AF was associated with increased rate of hospital admission and ICU admission but not associated with increased risk of mortality or transfusion requirement.</p>\",\"PeriodicalId\":15281,\"journal\":{\"name\":\"Journal of Cardiovascular Pharmacology and Therapeutics\",\"volume\":\"29 \",\"pages\":\"10742484241256271\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11981305/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Pharmacology and Therapeutics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/10742484241256271\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Pharmacology and Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10742484241256271","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Assessing Safety of Anticoagulation for Atrial Fibrillation in Patients with Cirrhosis: A Real-World Outcomes Study.
Aims: In patients with atrial fibrillation (AF) and stroke risk factors, randomized trials have demonstrated that anticoagulation decreases the risk of ischemic stroke. However, all trials to date have excluded patients with significant liver disease, leaving guidelines to extrapolate recommendations. We aim to evaluate the impact of anticoagulation on safety events in patients with AF and cirrhosis.
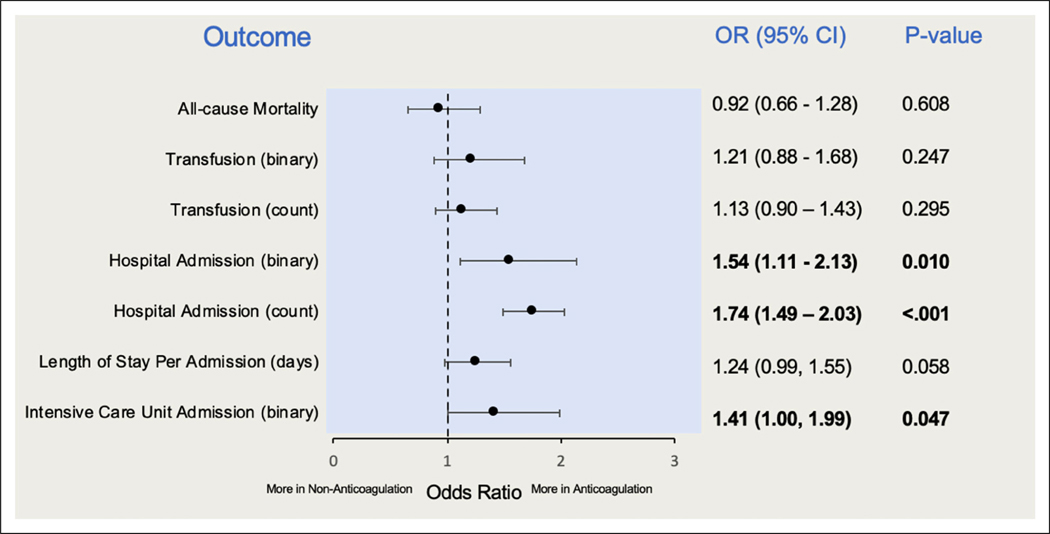
Methods and results: In this retrospective cohort study, we obtained de-identified health record data to extract anticoagulation strategy, comorbidities, prescriptions, lab values, and procedures for a cohort of patients with cirrhosis who develop AF. After selecting a propensity matched population to match patients with various anticoagulation strategies, we tracked data on outcomes for death, transfusion requirements, hospital and ICU admissions. After propensity score weighting and multivariable adjustment, anticoagulation strategy was associated with increased hospital admission count (OR = 1.74 per admission, P < .001), binary risk of hospital admission (OR = 1.54, P = .010) and risk of ICU admission (OR = 1.41, P = .047). We detected no significant differences in mortality, transfusion of blood products, or average length of stay. Direct oral anticoagulant (DOAC) prescriptions were associated with increased binary risk of hospital admission compared to warfarin prescriptions. In a third comparison, DOAC strategy alone was associated with increased hospital admission count (OR = 1.41 per admission, P < .001) and binary risk of hospital admission (OR = 1.52, P = .038) compared to no anticoagulation strategy.
Conclusion: Anticoagulation strategy in patients with cirrhosis and AF was associated with increased rate of hospital admission and ICU admission but not associated with increased risk of mortality or transfusion requirement.
期刊介绍:
Journal of Cardiovascular Pharmacology and Therapeutics (JCPT) is a peer-reviewed journal that publishes original basic human studies, animal studies, and bench research with potential clinical application to cardiovascular pharmacology and therapeutics. Experimental studies focus on translational research. This journal is a member of the Committee on Publication Ethics (COPE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


