Elahe Yaghmaei, Ahmad Najafi, Reza Daneshvar Kakhki
{"title":"一名未确诊的 HIV 阳性患者因水痘-带状疱疹病毒感染引发的纵向广泛横贯性脊髓炎","authors":"Elahe Yaghmaei, Ahmad Najafi, Reza Daneshvar Kakhki","doi":"10.1155/2024/9027198","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Longitudinal extensive transverse myelitis (LETM) has four main causes: inflammatory, malnutrition, vascular, and infectious causes. Among the commonly described viral causes leading to LETM are the <i>Herpesviridae</i> family, HIV, and HTLV-1. <i>Case Presentation</i>. A 43-year-old man presented with asymmetric weakness of the lower limbs (the left side was weaker), urinary retention, and flank pain. The symptoms began five days after shingle eruption and progressed over twelve days. He was diagnosed with longitudinal extensive transvers myelitis extending from T4 to T6, which corresponded to the same dermatome involved in shingles. The PCR result of cerebrospinal fluid was positive for varicella-zoster virus with a viral load of 500 copies/ml. Additionally, the initial HIV enzyme-linked immunosorbent assay (ELISA) test was positive, and his CD4 count was 72 cells/mm<sup>3</sup>. Other lab results were normal. Based on the appearance of LETM in the thoracic MRI at T4-T6, VZV myelitis was diagnosed, and treatment was initiated with acyclovir (30 mg/kg divided daily for twenty-one days), methylprednisolone (1 g/day for three days), prophylactic antibiotics (trimethoprim/sulfamethoxazole, rifampin, and isoniazid), and antiretroviral therapy (dolutegravir and Truvada). After 2-month follow-up, he was nearly free of symptoms.</p><p><strong>Conclusion: </strong>Infection is one of the critical causes of transverse myelitis. When a patient presents with skin shingles along with myelopathy, varicella-zoster myelitis should be considered, and the patient should be evaluated in terms of immune system dysfunction. Treatment with acyclovir has been shown to be effective in reducing clinical symptoms in such cases.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2024 ","pages":"9027198"},"PeriodicalIF":0.9000,"publicationDate":"2024-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11272404/pdf/","citationCount":"0","resultStr":"{\"title\":\"Longitudinal Extensive Transverse Myelitis due to Varicella-Zoster Virus Infection in an Undiagnosed HIV-Positive Patient.\",\"authors\":\"Elahe Yaghmaei, Ahmad Najafi, Reza Daneshvar Kakhki\",\"doi\":\"10.1155/2024/9027198\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Longitudinal extensive transverse myelitis (LETM) has four main causes: inflammatory, malnutrition, vascular, and infectious causes. Among the commonly described viral causes leading to LETM are the <i>Herpesviridae</i> family, HIV, and HTLV-1. <i>Case Presentation</i>. A 43-year-old man presented with asymmetric weakness of the lower limbs (the left side was weaker), urinary retention, and flank pain. The symptoms began five days after shingle eruption and progressed over twelve days. He was diagnosed with longitudinal extensive transvers myelitis extending from T4 to T6, which corresponded to the same dermatome involved in shingles. The PCR result of cerebrospinal fluid was positive for varicella-zoster virus with a viral load of 500 copies/ml. Additionally, the initial HIV enzyme-linked immunosorbent assay (ELISA) test was positive, and his CD4 count was 72 cells/mm<sup>3</sup>. Other lab results were normal. Based on the appearance of LETM in the thoracic MRI at T4-T6, VZV myelitis was diagnosed, and treatment was initiated with acyclovir (30 mg/kg divided daily for twenty-one days), methylprednisolone (1 g/day for three days), prophylactic antibiotics (trimethoprim/sulfamethoxazole, rifampin, and isoniazid), and antiretroviral therapy (dolutegravir and Truvada). After 2-month follow-up, he was nearly free of symptoms.</p><p><strong>Conclusion: </strong>Infection is one of the critical causes of transverse myelitis. When a patient presents with skin shingles along with myelopathy, varicella-zoster myelitis should be considered, and the patient should be evaluated in terms of immune system dysfunction. Treatment with acyclovir has been shown to be effective in reducing clinical symptoms in such cases.</p>\",\"PeriodicalId\":9615,\"journal\":{\"name\":\"Case Reports in Neurological Medicine\",\"volume\":\"2024 \",\"pages\":\"9027198\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11272404/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Neurological Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/9027198\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/9027198","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Longitudinal Extensive Transverse Myelitis due to Varicella-Zoster Virus Infection in an Undiagnosed HIV-Positive Patient.
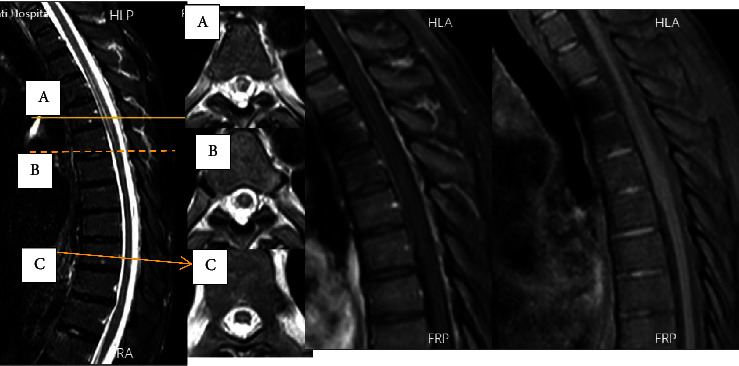
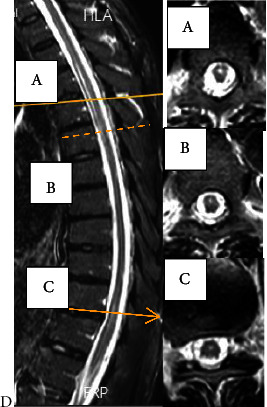
Introduction: Longitudinal extensive transverse myelitis (LETM) has four main causes: inflammatory, malnutrition, vascular, and infectious causes. Among the commonly described viral causes leading to LETM are the Herpesviridae family, HIV, and HTLV-1. Case Presentation. A 43-year-old man presented with asymmetric weakness of the lower limbs (the left side was weaker), urinary retention, and flank pain. The symptoms began five days after shingle eruption and progressed over twelve days. He was diagnosed with longitudinal extensive transvers myelitis extending from T4 to T6, which corresponded to the same dermatome involved in shingles. The PCR result of cerebrospinal fluid was positive for varicella-zoster virus with a viral load of 500 copies/ml. Additionally, the initial HIV enzyme-linked immunosorbent assay (ELISA) test was positive, and his CD4 count was 72 cells/mm3. Other lab results were normal. Based on the appearance of LETM in the thoracic MRI at T4-T6, VZV myelitis was diagnosed, and treatment was initiated with acyclovir (30 mg/kg divided daily for twenty-one days), methylprednisolone (1 g/day for three days), prophylactic antibiotics (trimethoprim/sulfamethoxazole, rifampin, and isoniazid), and antiretroviral therapy (dolutegravir and Truvada). After 2-month follow-up, he was nearly free of symptoms.
Conclusion: Infection is one of the critical causes of transverse myelitis. When a patient presents with skin shingles along with myelopathy, varicella-zoster myelitis should be considered, and the patient should be evaluated in terms of immune system dysfunction. Treatment with acyclovir has been shown to be effective in reducing clinical symptoms in such cases.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


