Michael Eiswerth, Prateek Mathur, Hani Rashed, Frank Greenway, Eric Ravussin, William Johnson, Pichamol Jirapinyo, Christopher C Thompson, Farid Kehdy, Shabnam Sarker, Le Yu Naing, Michael W Daniels, Thomas Abell
{"title":"自律神经和肠道特征分析有助于预测对多种肥胖症疗法的反应。","authors":"Michael Eiswerth, Prateek Mathur, Hani Rashed, Frank Greenway, Eric Ravussin, William Johnson, Pichamol Jirapinyo, Christopher C Thompson, Farid Kehdy, Shabnam Sarker, Le Yu Naing, Michael W Daniels, Thomas Abell","doi":"10.1007/s11695-024-07360-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Changes in autonomic (ANS) and enteric nervous systems (ENS) may be involved in pathogenesis of obesity. We hypothesized that baseline autonomic and enteric parameters may predict outcomes of diverse obesity therapies.</p><p><strong>Material and methods: </strong>We studied ANS and ENS physiology in 37 patients (8 male, 29 female, age 45 years, weight 129.7 kg) at 4 centers in patients undergoing medical (9: low-calorie diet) versus invasive (22: 16 sleeve, 6 bypass) and semi-invasive (6: 2 band, 2 high energy stimulation, 2 aspiration) weight loss therapies. Weight loss was reported as percent weight loss from baseline to latest values at 1 year and in some up to 5 years; classified as < or > /= 20% for each group. ANS testing included sympathetic adrenergic function by measuring reflex vasoconstriction and postural adjustment ratio. ENS was measured non-invasively using cutaneous low-resolution electrogastrogram.</p><p><strong>Results: </strong>Percent weight loss was greater with the invasive (28.5%) than semi-invasive (9.1%) or non-invasive low-calorie diet (4.4%) (p < .001). Percent weight loss at 1 year (and up to 5 years) corresponded to the adrenergic measure of postural adjustment ratio (r = .42, p = .012), total pulse amplitude at rest (r = .56, p < .001), and electrogastrogram standing-to-rest difference (r = .33, p = .056).</p><p><strong>Conclusion: </strong>Baseline autonomic and enteric function measures correspond to percentage with loss in this pilot study using diverse weight loss methods. Autonomic and enteric profiling has potential clinical use for evaluation and treatment of obesity but needed larger controlled trials.</p>","PeriodicalId":19460,"journal":{"name":"Obesity Surgery","volume":" ","pages":"3147-3160"},"PeriodicalIF":2.9000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Autonomic and Enteric Profiling May Help Predict Response to Diverse Obesity Therapies.\",\"authors\":\"Michael Eiswerth, Prateek Mathur, Hani Rashed, Frank Greenway, Eric Ravussin, William Johnson, Pichamol Jirapinyo, Christopher C Thompson, Farid Kehdy, Shabnam Sarker, Le Yu Naing, Michael W Daniels, Thomas Abell\",\"doi\":\"10.1007/s11695-024-07360-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Changes in autonomic (ANS) and enteric nervous systems (ENS) may be involved in pathogenesis of obesity. We hypothesized that baseline autonomic and enteric parameters may predict outcomes of diverse obesity therapies.</p><p><strong>Material and methods: </strong>We studied ANS and ENS physiology in 37 patients (8 male, 29 female, age 45 years, weight 129.7 kg) at 4 centers in patients undergoing medical (9: low-calorie diet) versus invasive (22: 16 sleeve, 6 bypass) and semi-invasive (6: 2 band, 2 high energy stimulation, 2 aspiration) weight loss therapies. Weight loss was reported as percent weight loss from baseline to latest values at 1 year and in some up to 5 years; classified as < or > /= 20% for each group. ANS testing included sympathetic adrenergic function by measuring reflex vasoconstriction and postural adjustment ratio. ENS was measured non-invasively using cutaneous low-resolution electrogastrogram.</p><p><strong>Results: </strong>Percent weight loss was greater with the invasive (28.5%) than semi-invasive (9.1%) or non-invasive low-calorie diet (4.4%) (p < .001). Percent weight loss at 1 year (and up to 5 years) corresponded to the adrenergic measure of postural adjustment ratio (r = .42, p = .012), total pulse amplitude at rest (r = .56, p < .001), and electrogastrogram standing-to-rest difference (r = .33, p = .056).</p><p><strong>Conclusion: </strong>Baseline autonomic and enteric function measures correspond to percentage with loss in this pilot study using diverse weight loss methods. Autonomic and enteric profiling has potential clinical use for evaluation and treatment of obesity but needed larger controlled trials.</p>\",\"PeriodicalId\":19460,\"journal\":{\"name\":\"Obesity Surgery\",\"volume\":\" \",\"pages\":\"3147-3160\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Obesity Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11695-024-07360-9\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11695-024-07360-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/24 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
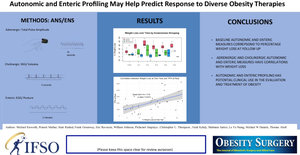
Autonomic and Enteric Profiling May Help Predict Response to Diverse Obesity Therapies.
Purpose: Changes in autonomic (ANS) and enteric nervous systems (ENS) may be involved in pathogenesis of obesity. We hypothesized that baseline autonomic and enteric parameters may predict outcomes of diverse obesity therapies.
Material and methods: We studied ANS and ENS physiology in 37 patients (8 male, 29 female, age 45 years, weight 129.7 kg) at 4 centers in patients undergoing medical (9: low-calorie diet) versus invasive (22: 16 sleeve, 6 bypass) and semi-invasive (6: 2 band, 2 high energy stimulation, 2 aspiration) weight loss therapies. Weight loss was reported as percent weight loss from baseline to latest values at 1 year and in some up to 5 years; classified as < or > /= 20% for each group. ANS testing included sympathetic adrenergic function by measuring reflex vasoconstriction and postural adjustment ratio. ENS was measured non-invasively using cutaneous low-resolution electrogastrogram.
Results: Percent weight loss was greater with the invasive (28.5%) than semi-invasive (9.1%) or non-invasive low-calorie diet (4.4%) (p < .001). Percent weight loss at 1 year (and up to 5 years) corresponded to the adrenergic measure of postural adjustment ratio (r = .42, p = .012), total pulse amplitude at rest (r = .56, p < .001), and electrogastrogram standing-to-rest difference (r = .33, p = .056).
Conclusion: Baseline autonomic and enteric function measures correspond to percentage with loss in this pilot study using diverse weight loss methods. Autonomic and enteric profiling has potential clinical use for evaluation and treatment of obesity but needed larger controlled trials.
期刊介绍:
Obesity Surgery is the official journal of the International Federation for the Surgery of Obesity and metabolic disorders (IFSO). A journal for bariatric/metabolic surgeons, Obesity Surgery provides an international, interdisciplinary forum for communicating the latest research, surgical and laparoscopic techniques, for treatment of massive obesity and metabolic disorders. Topics covered include original research, clinical reports, current status, guidelines, historical notes, invited commentaries, letters to the editor, medicolegal issues, meeting abstracts, modern surgery/technical innovations, new concepts, reviews, scholarly presentations and opinions.
Obesity Surgery benefits surgeons performing obesity/metabolic surgery, general surgeons and surgical residents, endoscopists, anesthetists, support staff, nurses, dietitians, psychiatrists, psychologists, plastic surgeons, internists including endocrinologists and diabetologists, nutritional scientists, and those dealing with eating disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


