Muhammad Aetesam-ur-Rahman MBBS, Tian X. Zhao PhD, Kitty Paques BSc, Joana Oliveira BSc, Yi-Da Chiu PhD, Melissa Duckworth BSc, Bharat Khialani MPH, Stephen Kyranis MClinEpi, Martin R. Bennett PhD, Nick E. J. West MD, Stephen P. Hoole MD
{"title":"经皮血运重建中的微循环保护评估:支架植入技术与设备比较。","authors":"Muhammad Aetesam-ur-Rahman MBBS, Tian X. Zhao PhD, Kitty Paques BSc, Joana Oliveira BSc, Yi-Da Chiu PhD, Melissa Duckworth BSc, Bharat Khialani MPH, Stephen Kyranis MClinEpi, Martin R. Bennett PhD, Nick E. J. West MD, Stephen P. Hoole MD","doi":"10.1002/ccd.31155","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Coronary microvascular dysfunction (CMD) after percutaneous coronary intervention (PCI) is prognostically important and may also be a cause of persistent angina. The stent balloon inflation technique or material properties may influence the degree of CMD post-PCI.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Thirty-six patients with stable angina attending for elective PCI were randomized to either slow drug eluting stent (DES) implantation technique (DES slow group): +2 atm. every 5 s., maintained for a further 30 s or a standard stent implantation technique (DES std group): rapid inflation and deflation. PressureWire X with thermodilution at rest and hyperemia and optical coherence tomography (OCT) were performed pre- and post-PCI. Combined primary endpoints were changes in index of microvascular resistance (delta IMR) and coronary flow reserve (delta CFR) following PCI. The secondary endpoints included differences in cardiac troponin I (delta cTnI) at 6 h post-PCI, Seattle angina questionnaire (SAQ) at 1, 3, 6, and 12 months and OCT measures of stent results immediately post-PCI and at 3 months.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Both groups were well matched, with similar baseline characteristics and OCT-defined plaque characteristics. Delta IMR was significantly better in the DES slow PCI arm with a median difference of −4.14 (95% CI -10.49, −0.39, <i>p</i> = <i>0.04</i>). Delta CFR was also numerically higher with a median difference of 0.47 (95% CI −0.52, 1.31, <i>p</i> = 0.46). This did not translate to improved delta median cTnI (1.5 (34.8) vs. 0 (27.5) ng/L, <i>p</i> = 0.75) or median SAQ score at 3 months, (85 (20) vs. 95 (17.5), <i>p</i> = 0.47).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Slow stent implantation is associated with less CMD after elective PCI in patients with stable angina.</p>\n </section>\n </div>","PeriodicalId":9650,"journal":{"name":"Catheterization and Cardiovascular Interventions","volume":"104 3","pages":"462-471"},"PeriodicalIF":2.1000,"publicationDate":"2024-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccd.31155","citationCount":"0","resultStr":"{\"title\":\"Evaluation of microcirculatory protection in percutaneous revascularisation: A stent implantation technique and device comparison\",\"authors\":\"Muhammad Aetesam-ur-Rahman MBBS, Tian X. Zhao PhD, Kitty Paques BSc, Joana Oliveira BSc, Yi-Da Chiu PhD, Melissa Duckworth BSc, Bharat Khialani MPH, Stephen Kyranis MClinEpi, Martin R. Bennett PhD, Nick E. J. West MD, Stephen P. Hoole MD\",\"doi\":\"10.1002/ccd.31155\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Coronary microvascular dysfunction (CMD) after percutaneous coronary intervention (PCI) is prognostically important and may also be a cause of persistent angina. The stent balloon inflation technique or material properties may influence the degree of CMD post-PCI.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Thirty-six patients with stable angina attending for elective PCI were randomized to either slow drug eluting stent (DES) implantation technique (DES slow group): +2 atm. every 5 s., maintained for a further 30 s or a standard stent implantation technique (DES std group): rapid inflation and deflation. PressureWire X with thermodilution at rest and hyperemia and optical coherence tomography (OCT) were performed pre- and post-PCI. Combined primary endpoints were changes in index of microvascular resistance (delta IMR) and coronary flow reserve (delta CFR) following PCI. The secondary endpoints included differences in cardiac troponin I (delta cTnI) at 6 h post-PCI, Seattle angina questionnaire (SAQ) at 1, 3, 6, and 12 months and OCT measures of stent results immediately post-PCI and at 3 months.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Both groups were well matched, with similar baseline characteristics and OCT-defined plaque characteristics. Delta IMR was significantly better in the DES slow PCI arm with a median difference of −4.14 (95% CI -10.49, −0.39, <i>p</i> = <i>0.04</i>). Delta CFR was also numerically higher with a median difference of 0.47 (95% CI −0.52, 1.31, <i>p</i> = 0.46). This did not translate to improved delta median cTnI (1.5 (34.8) vs. 0 (27.5) ng/L, <i>p</i> = 0.75) or median SAQ score at 3 months, (85 (20) vs. 95 (17.5), <i>p</i> = 0.47).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Slow stent implantation is associated with less CMD after elective PCI in patients with stable angina.</p>\\n </section>\\n </div>\",\"PeriodicalId\":9650,\"journal\":{\"name\":\"Catheterization and Cardiovascular Interventions\",\"volume\":\"104 3\",\"pages\":\"462-471\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccd.31155\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Catheterization and Cardiovascular Interventions\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ccd.31155\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Catheterization and Cardiovascular Interventions","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ccd.31155","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:经皮冠状动脉介入治疗(PCI)后冠状动脉微血管功能障碍(CMD)对预后非常重要,也可能是导致持续心绞痛的原因之一。支架球囊充气技术或材料特性可能会影响经皮冠状动脉介入术后冠状动脉微血管功能障碍的程度:方法:36 名稳定型心绞痛患者接受择期 PCI,随机分为药物洗脱支架 (DES) 慢速植入技术组(DES 慢速组)和药物洗脱支架 (DES) 加压技术组(DES 加压组):+或标准支架植入技术(DES std 组):快速充气和放气。在PCI前和PCI后进行了带有静息和充血时热稀释功能的压力线X和光学相干断层扫描(OCT)。综合主要终点是PCI后微血管阻力指数(delta IMR)和冠状动脉血流储备(delta CFR)的变化。次要终点包括PCI术后6小时的心肌肌钙蛋白I(delta cTnI)、1、3、6和12个月的西雅图心绞痛问卷(SAQ)以及PCI术后即刻和3个月时支架效果的OCT测量结果:结果:两组患者匹配度良好,基线特征和 OCT 定义的斑块特征相似。DES慢速PCI组的Delta IMR明显更好,中位差值为-4.14(95% CI -10.49,-0.39,p = 0.04)。Delta CFR 在数值上也更高,中位差值为 0.47 (95% CI -0.52, 1.31, p = 0.46)。这并没有转化为 cTnI 中位数 Delta 值的改善(1.5 (34.8) vs. 0 (27.5) ng/L,p = 0.75),也没有转化为 3 个月时 SAQ 中位数得分的改善(85 (20) vs. 95 (17.5),p = 0.47):结论:对于稳定型心绞痛患者,缓慢植入支架与择期 PCI 后较少的 CMD 有关。
Evaluation of microcirculatory protection in percutaneous revascularisation: A stent implantation technique and device comparison
Background
Coronary microvascular dysfunction (CMD) after percutaneous coronary intervention (PCI) is prognostically important and may also be a cause of persistent angina. The stent balloon inflation technique or material properties may influence the degree of CMD post-PCI.
Methods
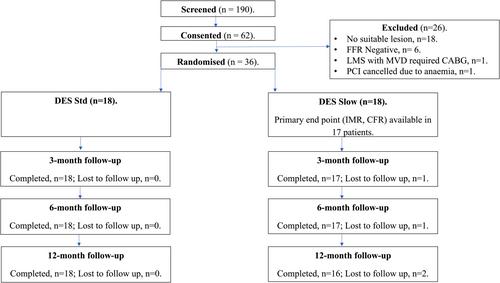
Thirty-six patients with stable angina attending for elective PCI were randomized to either slow drug eluting stent (DES) implantation technique (DES slow group): +2 atm. every 5 s., maintained for a further 30 s or a standard stent implantation technique (DES std group): rapid inflation and deflation. PressureWire X with thermodilution at rest and hyperemia and optical coherence tomography (OCT) were performed pre- and post-PCI. Combined primary endpoints were changes in index of microvascular resistance (delta IMR) and coronary flow reserve (delta CFR) following PCI. The secondary endpoints included differences in cardiac troponin I (delta cTnI) at 6 h post-PCI, Seattle angina questionnaire (SAQ) at 1, 3, 6, and 12 months and OCT measures of stent results immediately post-PCI and at 3 months.
Results
Both groups were well matched, with similar baseline characteristics and OCT-defined plaque characteristics. Delta IMR was significantly better in the DES slow PCI arm with a median difference of −4.14 (95% CI -10.49, −0.39, p = 0.04). Delta CFR was also numerically higher with a median difference of 0.47 (95% CI −0.52, 1.31, p = 0.46). This did not translate to improved delta median cTnI (1.5 (34.8) vs. 0 (27.5) ng/L, p = 0.75) or median SAQ score at 3 months, (85 (20) vs. 95 (17.5), p = 0.47).
Conclusion
Slow stent implantation is associated with less CMD after elective PCI in patients with stable angina.
期刊介绍:
Catheterization and Cardiovascular Interventions is an international journal covering the broad field of cardiovascular diseases. Subject material includes basic and clinical information that is derived from or related to invasive and interventional coronary or peripheral vascular techniques. The journal focuses on material that will be of immediate practical value to physicians providing patient care in the clinical laboratory setting. To accomplish this, the journal publishes Preliminary Reports and Work In Progress articles that complement the traditional Original Studies, Case Reports, and Comprehensive Reviews. Perspective and insight concerning controversial subjects and evolving technologies are provided regularly through Editorial Commentaries furnished by members of the Editorial Board and other experts. Articles are subject to double-blind peer review and complete editorial evaluation prior to any decision regarding acceptability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


