André Costa Pinho, Alexandra Luís Manco, Marco Silva, Hugo Santos Sousa, Fernando Resende, John Preto, Eduardo Lima da Costa
{"title":"胃内球囊作为体重指数(BMI)≥ 50 kg/m2 患者进行代谢减重手术前的第一步:球囊术后的结果与手术后的总体结果相关吗?","authors":"André Costa Pinho, Alexandra Luís Manco, Marco Silva, Hugo Santos Sousa, Fernando Resende, John Preto, Eduardo Lima da Costa","doi":"10.1007/s11695-024-07418-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients with body mass index (BMI) ≥ 50 kg/m<sup>2</sup>, classified with obesity class IV/V, require complex treatments. Intragastric balloon (IGB) is a possible treatment before metabolic bariatric surgery (MBS) that may reduce peri-operative complications. This study evaluates IGB outcomes and complications before MBS in patients with Obesity IV/V, and subsequent MBS results, regarding weight loss and comorbidity resolution.</p><p><strong>Methods: </strong>Retrospective cohort study of all patients with BMI above 50 kg/m<sup>2</sup> submitted to IGB before MBS between 2009 and 2023 in a high-volume center. Variables analyzed included weight loss after IGB and MBS, IGB complications, and comorbidity resolution. Suboptimal clinical responses were defined as %TWL < 5% for IGB, %TWL < 20% for MBS, and %TWL < 25% or BMI ≥ 35 kg/m<sup>2</sup> for IGB + MBS.</p><p><strong>Results: </strong>Seventy-four patients (mean BMI 58.8 ± 8 kg/m<sup>2</sup>) were included. After IGB, the mean %TWL was 14.2 ± 8.5%, with a 21.6% complication rate, predominantly nausea and vomiting, and one death. Suboptimal clinical response of IGB affected 13.5% of patients, and 5.4% required early removal. Two years after MBS, the mean %TWL was 38.2 ± 11.6%, mainly due to MBS, yet approximately one-third of %TWL was attributed to IGB. No correlation was found between IGB and MBS outcomes. At 2-year follow-up, 45.1% patients had %TWL ≥ 25 and BMI < 35 kg/m<sup>2</sup>.</p><p><strong>Conclusion: </strong>The IGB is a treatment option before MBS in patients with Obesity Class IV/V, with acceptable weight loss outcomes but not infrequent complications. A multidisciplinary approach is mandatory, and all treatments must be considered in this difficult subset of patients.</p>","PeriodicalId":19460,"journal":{"name":"Obesity Surgery","volume":null,"pages":null},"PeriodicalIF":2.9000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11349788/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intragastric Balloon as a First Step Before Metabolic Bariatric Surgery in Patients with BMI ≥ 50 kg/m<sup>2</sup>: are the Results After Balloon Related to Global Outcomes After Surgery?\",\"authors\":\"André Costa Pinho, Alexandra Luís Manco, Marco Silva, Hugo Santos Sousa, Fernando Resende, John Preto, Eduardo Lima da Costa\",\"doi\":\"10.1007/s11695-024-07418-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Patients with body mass index (BMI) ≥ 50 kg/m<sup>2</sup>, classified with obesity class IV/V, require complex treatments. Intragastric balloon (IGB) is a possible treatment before metabolic bariatric surgery (MBS) that may reduce peri-operative complications. This study evaluates IGB outcomes and complications before MBS in patients with Obesity IV/V, and subsequent MBS results, regarding weight loss and comorbidity resolution.</p><p><strong>Methods: </strong>Retrospective cohort study of all patients with BMI above 50 kg/m<sup>2</sup> submitted to IGB before MBS between 2009 and 2023 in a high-volume center. Variables analyzed included weight loss after IGB and MBS, IGB complications, and comorbidity resolution. Suboptimal clinical responses were defined as %TWL < 5% for IGB, %TWL < 20% for MBS, and %TWL < 25% or BMI ≥ 35 kg/m<sup>2</sup> for IGB + MBS.</p><p><strong>Results: </strong>Seventy-four patients (mean BMI 58.8 ± 8 kg/m<sup>2</sup>) were included. After IGB, the mean %TWL was 14.2 ± 8.5%, with a 21.6% complication rate, predominantly nausea and vomiting, and one death. Suboptimal clinical response of IGB affected 13.5% of patients, and 5.4% required early removal. Two years after MBS, the mean %TWL was 38.2 ± 11.6%, mainly due to MBS, yet approximately one-third of %TWL was attributed to IGB. No correlation was found between IGB and MBS outcomes. At 2-year follow-up, 45.1% patients had %TWL ≥ 25 and BMI < 35 kg/m<sup>2</sup>.</p><p><strong>Conclusion: </strong>The IGB is a treatment option before MBS in patients with Obesity Class IV/V, with acceptable weight loss outcomes but not infrequent complications. A multidisciplinary approach is mandatory, and all treatments must be considered in this difficult subset of patients.</p>\",\"PeriodicalId\":19460,\"journal\":{\"name\":\"Obesity Surgery\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11349788/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Obesity Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11695-024-07418-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11695-024-07418-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
Intragastric Balloon as a First Step Before Metabolic Bariatric Surgery in Patients with BMI ≥ 50 kg/m2: are the Results After Balloon Related to Global Outcomes After Surgery?
Introduction: Patients with body mass index (BMI) ≥ 50 kg/m2, classified with obesity class IV/V, require complex treatments. Intragastric balloon (IGB) is a possible treatment before metabolic bariatric surgery (MBS) that may reduce peri-operative complications. This study evaluates IGB outcomes and complications before MBS in patients with Obesity IV/V, and subsequent MBS results, regarding weight loss and comorbidity resolution.
Methods: Retrospective cohort study of all patients with BMI above 50 kg/m2 submitted to IGB before MBS between 2009 and 2023 in a high-volume center. Variables analyzed included weight loss after IGB and MBS, IGB complications, and comorbidity resolution. Suboptimal clinical responses were defined as %TWL < 5% for IGB, %TWL < 20% for MBS, and %TWL < 25% or BMI ≥ 35 kg/m2 for IGB + MBS.
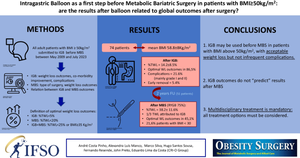
Results: Seventy-four patients (mean BMI 58.8 ± 8 kg/m2) were included. After IGB, the mean %TWL was 14.2 ± 8.5%, with a 21.6% complication rate, predominantly nausea and vomiting, and one death. Suboptimal clinical response of IGB affected 13.5% of patients, and 5.4% required early removal. Two years after MBS, the mean %TWL was 38.2 ± 11.6%, mainly due to MBS, yet approximately one-third of %TWL was attributed to IGB. No correlation was found between IGB and MBS outcomes. At 2-year follow-up, 45.1% patients had %TWL ≥ 25 and BMI < 35 kg/m2.
Conclusion: The IGB is a treatment option before MBS in patients with Obesity Class IV/V, with acceptable weight loss outcomes but not infrequent complications. A multidisciplinary approach is mandatory, and all treatments must be considered in this difficult subset of patients.
期刊介绍:
Obesity Surgery is the official journal of the International Federation for the Surgery of Obesity and metabolic disorders (IFSO). A journal for bariatric/metabolic surgeons, Obesity Surgery provides an international, interdisciplinary forum for communicating the latest research, surgical and laparoscopic techniques, for treatment of massive obesity and metabolic disorders. Topics covered include original research, clinical reports, current status, guidelines, historical notes, invited commentaries, letters to the editor, medicolegal issues, meeting abstracts, modern surgery/technical innovations, new concepts, reviews, scholarly presentations and opinions.
Obesity Surgery benefits surgeons performing obesity/metabolic surgery, general surgeons and surgical residents, endoscopists, anesthetists, support staff, nurses, dietitians, psychiatrists, psychologists, plastic surgeons, internists including endocrinologists and diabetologists, nutritional scientists, and those dealing with eating disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


