{"title":"院外心脏骤停患者的预后取决于院前高级气道管理的时机:一项回顾性观察研究。","authors":"Sang-Hun Lee, Hyun Wook Ryoo","doi":"10.12701/jyms.2024.00332","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with out-of-hospital cardiac arrest (OHCA), guidelines recommend advanced airway (AA) management at the advanced cardiovascular life support stage; however, the ideal timing remains controversial. Therefore, we evaluated the prognosis according to the timing of AA in patients with OHCA.</p><p><strong>Methods: </strong>We conducted a retrospective observational study of patients with OHCA at six major hospitals in Daegu Metropolitan City, South Korea, from August 2019 to June 2022. We compared groups with early and late AA and evaluated prognosis, including recovery of spontaneous circulation (ROSC), survival to discharge, and neurological evaluation, according to AA timing.</p><p><strong>Results: </strong>Of 2,087 patients with OHCA, 945 underwent early AA management and 1,142 underwent late AA management. The timing of AA management did not influence ROSC in the emergency department (5-6 minutes: adjusted odds ratio [aOR], 0.97; p=0.914; 7-9 minutes: aOR, 1.37; p=0.223; ≥10 minutes: aOR, 1.32; p=0.345). The timing of AA management also did not influence survival to discharge (5-6 minutes: aOR, 0.79; p=0.680; 7-9 minutes: aOR, 1.04; p=0.944; ≥10 minutes: aOR, 1.86; p=0.320) or good neurological outcomes (5-6 minutes: aOR, 1.72; p=0.512; 7-9 minutes: aOR, 0.48; p=0.471; ≥10 minutes: aOR, 0.96; p=0.892).</p><p><strong>Conclusion: </strong>AA timing in patients with OHCA was not associated with ROSC, survival to hospital discharge, or neurological outcomes.</p>","PeriodicalId":74020,"journal":{"name":"Journal of Yeungnam medical science","volume":" ","pages":"288-295"},"PeriodicalIF":1.4000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11534406/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes in patients with out-of-hospital cardiac arrest according to prehospital advanced airway management timing: a retrospective observational study.\",\"authors\":\"Sang-Hun Lee, Hyun Wook Ryoo\",\"doi\":\"10.12701/jyms.2024.00332\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In patients with out-of-hospital cardiac arrest (OHCA), guidelines recommend advanced airway (AA) management at the advanced cardiovascular life support stage; however, the ideal timing remains controversial. Therefore, we evaluated the prognosis according to the timing of AA in patients with OHCA.</p><p><strong>Methods: </strong>We conducted a retrospective observational study of patients with OHCA at six major hospitals in Daegu Metropolitan City, South Korea, from August 2019 to June 2022. We compared groups with early and late AA and evaluated prognosis, including recovery of spontaneous circulation (ROSC), survival to discharge, and neurological evaluation, according to AA timing.</p><p><strong>Results: </strong>Of 2,087 patients with OHCA, 945 underwent early AA management and 1,142 underwent late AA management. The timing of AA management did not influence ROSC in the emergency department (5-6 minutes: adjusted odds ratio [aOR], 0.97; p=0.914; 7-9 minutes: aOR, 1.37; p=0.223; ≥10 minutes: aOR, 1.32; p=0.345). The timing of AA management also did not influence survival to discharge (5-6 minutes: aOR, 0.79; p=0.680; 7-9 minutes: aOR, 1.04; p=0.944; ≥10 minutes: aOR, 1.86; p=0.320) or good neurological outcomes (5-6 minutes: aOR, 1.72; p=0.512; 7-9 minutes: aOR, 0.48; p=0.471; ≥10 minutes: aOR, 0.96; p=0.892).</p><p><strong>Conclusion: </strong>AA timing in patients with OHCA was not associated with ROSC, survival to hospital discharge, or neurological outcomes.</p>\",\"PeriodicalId\":74020,\"journal\":{\"name\":\"Journal of Yeungnam medical science\",\"volume\":\" \",\"pages\":\"288-295\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11534406/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Yeungnam medical science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12701/jyms.2024.00332\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Yeungnam medical science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12701/jyms.2024.00332","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:对于院外心脏骤停(OHCA)患者,指南建议在高级心血管生命支持阶段进行高级气道(AA)管理;然而,理想的时机仍存在争议。因此,我们根据 OHCA 患者实施 AA 的时机对其预后进行了评估:我们在 2019 年 8 月至 2022 年 6 月期间对韩国大邱广域市六家主要医院的 OHCA 患者进行了一项回顾性观察研究。我们比较了早期和晚期AA组,并根据AA时间评估了预后,包括自主循环恢复(ROSC)、出院存活率和神经系统评估:在2087名OHCA患者中,945人接受了早期AA治疗,1142人接受了晚期AA治疗。AA管理的时间并不影响急诊科的ROSC(5-6分钟:调整比值比[aOR],0.97;p=0.914;7-9分钟:aOR,1.37;p=0.223;≥10分钟:aOR,1.32;p=0.345)。AA管理的时间也不影响出院后的存活率(5-6分钟:aOR,0.79;p=0.680;7-9分钟:aOR,1.04;p=0.944;≥10分钟:aOR,1.86;p=0.320)或良好的神经功能预后(5-6分钟:aOR,1.72;p=0.512;7-9分钟:aOR,0.48;p=0.471;≥10分钟:aOR,0.96;p=0.892):结论:OHCA 患者的 AA 时间与 ROSC、出院存活率或神经系统预后无关。
Outcomes in patients with out-of-hospital cardiac arrest according to prehospital advanced airway management timing: a retrospective observational study.
Background: In patients with out-of-hospital cardiac arrest (OHCA), guidelines recommend advanced airway (AA) management at the advanced cardiovascular life support stage; however, the ideal timing remains controversial. Therefore, we evaluated the prognosis according to the timing of AA in patients with OHCA.
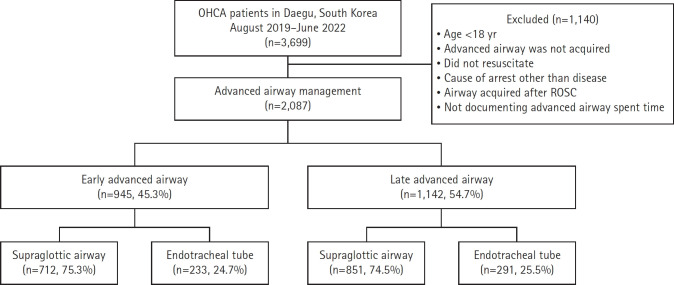
Methods: We conducted a retrospective observational study of patients with OHCA at six major hospitals in Daegu Metropolitan City, South Korea, from August 2019 to June 2022. We compared groups with early and late AA and evaluated prognosis, including recovery of spontaneous circulation (ROSC), survival to discharge, and neurological evaluation, according to AA timing.
Results: Of 2,087 patients with OHCA, 945 underwent early AA management and 1,142 underwent late AA management. The timing of AA management did not influence ROSC in the emergency department (5-6 minutes: adjusted odds ratio [aOR], 0.97; p=0.914; 7-9 minutes: aOR, 1.37; p=0.223; ≥10 minutes: aOR, 1.32; p=0.345). The timing of AA management also did not influence survival to discharge (5-6 minutes: aOR, 0.79; p=0.680; 7-9 minutes: aOR, 1.04; p=0.944; ≥10 minutes: aOR, 1.86; p=0.320) or good neurological outcomes (5-6 minutes: aOR, 1.72; p=0.512; 7-9 minutes: aOR, 0.48; p=0.471; ≥10 minutes: aOR, 0.96; p=0.892).
Conclusion: AA timing in patients with OHCA was not associated with ROSC, survival to hospital discharge, or neurological outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


