Kadie-Ann Sterling, Mary Joan MacLeod, Mark Barber, Melanie Turner
{"title":"男性和女性缺血性和出血性中风后的急性期护理、二级预防和预后:一项数据链接研究。","authors":"Kadie-Ann Sterling, Mary Joan MacLeod, Mark Barber, Melanie Turner","doi":"10.1159/000540371","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>There is evidence that sex differences exist in stroke presentation, risk factors, severity, treatment, and outcomes. To further understand this, we explored how sex differences influence acute stroke management, secondary prevention prescribing, and mortality outcomes in a well-characterised cohort of first-ever stroke patients in Scotland.</p><p><strong>Methods: </strong>This is a retrospective, population-based, data-linkage study of stroke admissions to acute care hospitals in Scotland between January 1, 2011, and December 31, 2018. Data sources included the Scottish Stroke Care Audit (SSCA), the Prescribing Information System (PIS), the Scottish Morbidity Record 01 (SMR01), and the National Records of Scotland (NRS) death records. Multivariable logistic regression was used to explore the association between patient sex, acute stroke care, and secondary prevention prescribing, while Cox proportional hazards models were used to explore the association between patient sex and all-cause mortality up to 1 year after index event.</p><p><strong>Results: </strong>This study included 5,901 patients with a first-ever intracerebral haemorrhage (ICH) and 47,087 patients with a first-ever acute ischaemic stroke (AIS). After an ICH, women had significantly lower odds of receiving all components of the stroke care bundle (adjusted odds ratio [aOR], 0.78; 95% confidence interval [CI], 0.69-0.87) and were less likely to be prescribed antihypertensives within 90 days after discharge to the usual place of residence (aOR, 0.78; 95% CI, 0.63-0.97). There was no sex difference in stroke care bundle achievement for those admitted with AIS; however, women had significantly lower odds of receiving antihypertensives, lipid-lowering drugs, or oral anticoagulants after discharge. The risk of all-cause mortality was lower in women at 1 year after both ICH (adjusted hazard ratio [aHR], 0.90; 95% CI, 0.83-0.98) and AIS (aHR, 0.91; 95% CI, 0.87-0.95) after adjusting for potential confounders.</p><p><strong>Conclusion: </strong>The sex differences in stroke treatment and outcomes may be partly explained by the older age of women at the time of stroke, which influences stroke presentation, severity, and prognosis. However, following adjustment, women had a reduced risk of all-cause mortality after both ICH and AIS.</p>","PeriodicalId":9683,"journal":{"name":"Cerebrovascular Diseases","volume":" ","pages":"371-378"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136599/pdf/","citationCount":"0","resultStr":"{\"title\":\"Acute Care, Secondary Prevention, and Outcomes after Ischaemic and Haemorrhagic Stroke in Men and Women: A Data-Linkage Study.\",\"authors\":\"Kadie-Ann Sterling, Mary Joan MacLeod, Mark Barber, Melanie Turner\",\"doi\":\"10.1159/000540371\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>There is evidence that sex differences exist in stroke presentation, risk factors, severity, treatment, and outcomes. To further understand this, we explored how sex differences influence acute stroke management, secondary prevention prescribing, and mortality outcomes in a well-characterised cohort of first-ever stroke patients in Scotland.</p><p><strong>Methods: </strong>This is a retrospective, population-based, data-linkage study of stroke admissions to acute care hospitals in Scotland between January 1, 2011, and December 31, 2018. Data sources included the Scottish Stroke Care Audit (SSCA), the Prescribing Information System (PIS), the Scottish Morbidity Record 01 (SMR01), and the National Records of Scotland (NRS) death records. Multivariable logistic regression was used to explore the association between patient sex, acute stroke care, and secondary prevention prescribing, while Cox proportional hazards models were used to explore the association between patient sex and all-cause mortality up to 1 year after index event.</p><p><strong>Results: </strong>This study included 5,901 patients with a first-ever intracerebral haemorrhage (ICH) and 47,087 patients with a first-ever acute ischaemic stroke (AIS). After an ICH, women had significantly lower odds of receiving all components of the stroke care bundle (adjusted odds ratio [aOR], 0.78; 95% confidence interval [CI], 0.69-0.87) and were less likely to be prescribed antihypertensives within 90 days after discharge to the usual place of residence (aOR, 0.78; 95% CI, 0.63-0.97). There was no sex difference in stroke care bundle achievement for those admitted with AIS; however, women had significantly lower odds of receiving antihypertensives, lipid-lowering drugs, or oral anticoagulants after discharge. The risk of all-cause mortality was lower in women at 1 year after both ICH (adjusted hazard ratio [aHR], 0.90; 95% CI, 0.83-0.98) and AIS (aHR, 0.91; 95% CI, 0.87-0.95) after adjusting for potential confounders.</p><p><strong>Conclusion: </strong>The sex differences in stroke treatment and outcomes may be partly explained by the older age of women at the time of stroke, which influences stroke presentation, severity, and prognosis. However, following adjustment, women had a reduced risk of all-cause mortality after both ICH and AIS.</p>\",\"PeriodicalId\":9683,\"journal\":{\"name\":\"Cerebrovascular Diseases\",\"volume\":\" \",\"pages\":\"371-378\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136599/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebrovascular Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000540371\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000540371","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/17 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Acute Care, Secondary Prevention, and Outcomes after Ischaemic and Haemorrhagic Stroke in Men and Women: A Data-Linkage Study.
Introduction: There is evidence that sex differences exist in stroke presentation, risk factors, severity, treatment, and outcomes. To further understand this, we explored how sex differences influence acute stroke management, secondary prevention prescribing, and mortality outcomes in a well-characterised cohort of first-ever stroke patients in Scotland.
Methods: This is a retrospective, population-based, data-linkage study of stroke admissions to acute care hospitals in Scotland between January 1, 2011, and December 31, 2018. Data sources included the Scottish Stroke Care Audit (SSCA), the Prescribing Information System (PIS), the Scottish Morbidity Record 01 (SMR01), and the National Records of Scotland (NRS) death records. Multivariable logistic regression was used to explore the association between patient sex, acute stroke care, and secondary prevention prescribing, while Cox proportional hazards models were used to explore the association between patient sex and all-cause mortality up to 1 year after index event.
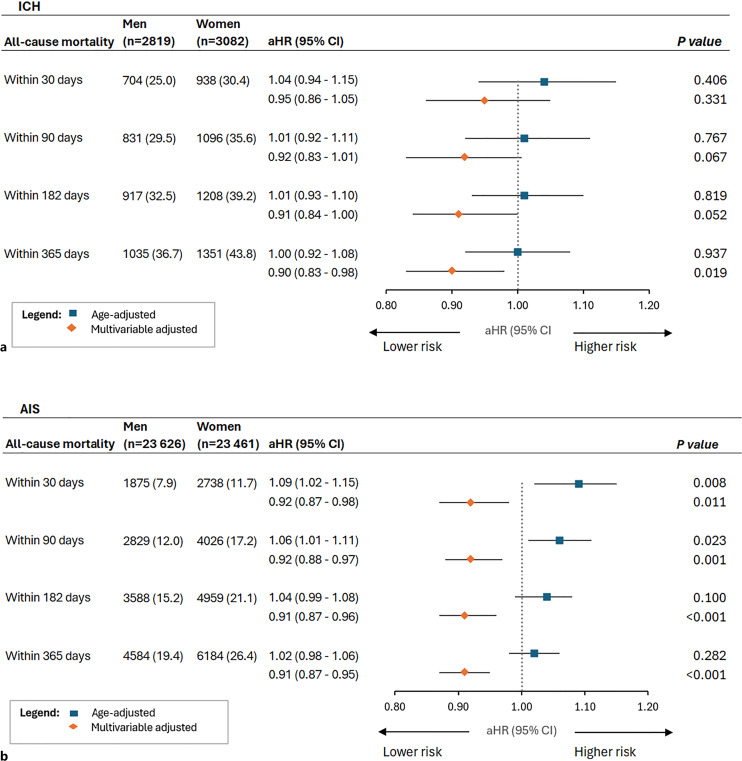
Results: This study included 5,901 patients with a first-ever intracerebral haemorrhage (ICH) and 47,087 patients with a first-ever acute ischaemic stroke (AIS). After an ICH, women had significantly lower odds of receiving all components of the stroke care bundle (adjusted odds ratio [aOR], 0.78; 95% confidence interval [CI], 0.69-0.87) and were less likely to be prescribed antihypertensives within 90 days after discharge to the usual place of residence (aOR, 0.78; 95% CI, 0.63-0.97). There was no sex difference in stroke care bundle achievement for those admitted with AIS; however, women had significantly lower odds of receiving antihypertensives, lipid-lowering drugs, or oral anticoagulants after discharge. The risk of all-cause mortality was lower in women at 1 year after both ICH (adjusted hazard ratio [aHR], 0.90; 95% CI, 0.83-0.98) and AIS (aHR, 0.91; 95% CI, 0.87-0.95) after adjusting for potential confounders.
Conclusion: The sex differences in stroke treatment and outcomes may be partly explained by the older age of women at the time of stroke, which influences stroke presentation, severity, and prognosis. However, following adjustment, women had a reduced risk of all-cause mortality after both ICH and AIS.
期刊介绍:
A rapidly-growing field, stroke and cerebrovascular research is unique in that it involves a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. ''Cerebrovascular Diseases'' is an international forum which meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues, dealing with all aspects of stroke and cerebrovascular diseases. It contains original contributions, reviews of selected topics and clinical investigative studies, recent meeting reports and work-in-progress as well as discussions on controversial issues. All aspects related to clinical advances are considered, while purely experimental work appears if directly relevant to clinical issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


