耐药性高血压:诊断、评估和治疗--泰国高血压学会临床共识声明。
IF 4.3
2区 医学
Q1 PERIPHERAL VASCULAR DISEASE
引用次数: 0
摘要
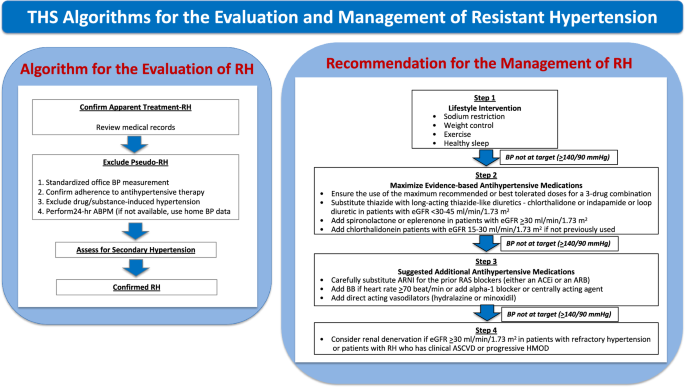
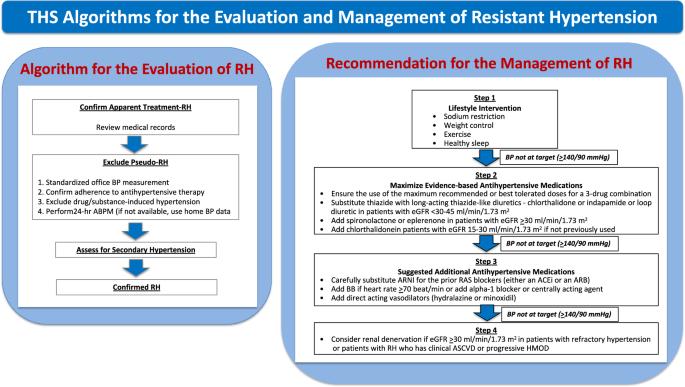
难治性高血压(RH)包括在接受≥3种降压药物治疗的同时血压(BP)仍未得到控制,或在接受≥4种降压药物治疗的同时血压得到控制的高血压患者。RH 的确切患病率很难量化。但据合理估计,真正的 RH 约占高血压人群的 5%。与一般高血压患者相比,RH 患者的心血管风险更高。要排除假性血压阻力,必须进行标准化的诊室血压测量、确认是否遵医嘱、寻找药物或物质引起的血压升高,并进行动态或家庭血压监测。应根据临床数据进行适当的进一步检查,以排除继发性高血压的可能原因。高血压的治疗包括加强生活方式干预和调整降压药物方案。改变生活方式的基本要素包括限制钠盐摄入、控制体重、规律运动和健康睡眠。建议根据现有证据逐步调整降压药物。介绍了根据患者的肾功能选择合适的利尿剂。萨库比特利/缬沙坦可谨慎替代之前的肾素-血管紧张素系统阻滞剂,尤其是射血分数保留的心力衰竭患者。如果血压仍无法控制,则应考虑采用肾神经支配等设备治疗。由于基于设备的治疗是一种侵入性且成本高昂的治疗方法,因此只有在仔细、适当地选择病例后才能使用。在实际操作中,RH 的治疗应根据每位患者的特点进行个体化。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Resistant hypertension: diagnosis, evaluation, and treatment a clinical consensus statement from the Thai hypertension society
Resistant hypertension (RH) includes hypertensive patients with uncontrolled blood pressure (BP) while receiving ≥3 BP-lowering medications or with controlled BP while receiving ≥4 BP-lowering medications. The exact prevalence of RH is challenging to quantify. However, a reasonable estimate of true RH is around 5% of the hypertensive population. Patients with RH have higher cardiovascular risk as compared with hypertensive patients in general. Standardized office BP measurement, confirmation of medical adherence, search for drug- or substance-induced BP elevation, and ambulatory or home BP monitoring are mandatory to exclude pseudoresistance. Appropriate further investigations, guided by clinical data, should be pursued to exclude possible secondary causes of hypertension. The management of RH includes the intensification of lifestyle interventions and the modification of antihypertensive drug regimens. The essential aspects of lifestyle modification include sodium restriction, body weight control, regular exercise, and healthy sleep. Step-by-step adjustment of the BP-lowering drugs based on the available evidence is proposed. The suitable choice of diuretics according to patients’ renal function is presented. Sacubitril/valsartan can be carefully substituted for the prior renin-angiotensin system blockers, especially in those with heart failure with preserved ejection fraction. If BP remains uncontrolled, device therapy such as renal nerve denervation should be considered. Since device-based treatment is an invasive and costly procedure, it should be used only after careful and appropriate case selection. In real-world practice, the management of RH should be individualized depending on each patient’s characteristics.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Hypertension Research
医学-外周血管病
CiteScore
7.40
自引率
16.70%
发文量
249
审稿时长
3-8 weeks
期刊介绍:
Hypertension Research is the official publication of the Japanese Society of Hypertension. The journal publishes papers reporting original clinical and experimental research that contribute to the advancement of knowledge in the field of hypertension and related cardiovascular diseases. The journal publishes Review Articles, Articles, Correspondence and Comments.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


