Jia Wang, Xiang Li, Jiahui Jiang, Ze Luo, Xilun Tan, Ruhua Ren, Tsutomu Fujita, Yoshifumi Kashima, Tetsuaki Li Tanimura, Ming Wang, Chenhao Zhang
{"title":"右心室-肺动脉耦合与射血分数保留型心力衰竭的预后","authors":"Jia Wang, Xiang Li, Jiahui Jiang, Ze Luo, Xilun Tan, Ruhua Ren, Tsutomu Fujita, Yoshifumi Kashima, Tetsuaki Li Tanimura, Ming Wang, Chenhao Zhang","doi":"10.1002/clc.24308","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Right ventricular–pulmonary artery coupling (RVPAC) refers to the relationship between right ventricular systolic force and afterload. The ratio of echocardiograph-derived tricuspid annular plane systolic excursion (TAPSE) to pulmonary artery systolic pressure (PASP) has been proposed as a noninvasive measurement of RVPAC and reported as an independent prognostic parameter of heart failure. However, it has not been adequately in detail evaluated in heart failure with preserved ejection fraction (HFpEF). We hypothesized that RVPAC may be used and proposed as an expression of key risk factors in patients with HFpEF.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We retrospectively analyzed TAPSE/PASP of 648 HFpEF patients hospitalized in Chongqing Hospital of Traditional Chinese Medicine from January 1, 2016 to January 1, 2017. All eligible patients were followed up for 5 years. The correlation between TAPSE/SPAP index and clinical indicators and outcomes was evaluated.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The final analysis included 414 patients. Nonsurvivors had significantly lower TAPSE, TAPSE/PASP and higher PASP compared with survivors (<i>p</i> < 0.0001). ROC curve analysis showed that the optimal cutoff of TAPSE, PASP, and RVPAC to predict all-cause death were 16.5 mm, 37.5 mmHg, and 0.45 mm/mmHg, respectively. In multivariate Cox regression analyses adjusted for gender showed a significant, independent association of the RVPAC with the composite endpoint of all-cause death or HF-related recurrent hospitalization (HR: 0.006; 95% CI 0.001–0.057, <i>p</i> < 0.001).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>RVPAC, defined by the ratio of TAPSE to PASP, is the expression of a key risk factor in HFpEF patients, which is independently associated with the composite endpoint of all-cause death or HF-related recurrent hospitalization.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 7","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24308","citationCount":"0","resultStr":"{\"title\":\"Right Ventricular–Pulmonary Arterial Coupling and Outcome in Heart Failure With Preserved Ejection Fraction\",\"authors\":\"Jia Wang, Xiang Li, Jiahui Jiang, Ze Luo, Xilun Tan, Ruhua Ren, Tsutomu Fujita, Yoshifumi Kashima, Tetsuaki Li Tanimura, Ming Wang, Chenhao Zhang\",\"doi\":\"10.1002/clc.24308\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Right ventricular–pulmonary artery coupling (RVPAC) refers to the relationship between right ventricular systolic force and afterload. The ratio of echocardiograph-derived tricuspid annular plane systolic excursion (TAPSE) to pulmonary artery systolic pressure (PASP) has been proposed as a noninvasive measurement of RVPAC and reported as an independent prognostic parameter of heart failure. However, it has not been adequately in detail evaluated in heart failure with preserved ejection fraction (HFpEF). We hypothesized that RVPAC may be used and proposed as an expression of key risk factors in patients with HFpEF.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We retrospectively analyzed TAPSE/PASP of 648 HFpEF patients hospitalized in Chongqing Hospital of Traditional Chinese Medicine from January 1, 2016 to January 1, 2017. All eligible patients were followed up for 5 years. The correlation between TAPSE/SPAP index and clinical indicators and outcomes was evaluated.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The final analysis included 414 patients. Nonsurvivors had significantly lower TAPSE, TAPSE/PASP and higher PASP compared with survivors (<i>p</i> < 0.0001). ROC curve analysis showed that the optimal cutoff of TAPSE, PASP, and RVPAC to predict all-cause death were 16.5 mm, 37.5 mmHg, and 0.45 mm/mmHg, respectively. In multivariate Cox regression analyses adjusted for gender showed a significant, independent association of the RVPAC with the composite endpoint of all-cause death or HF-related recurrent hospitalization (HR: 0.006; 95% CI 0.001–0.057, <i>p</i> < 0.001).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>RVPAC, defined by the ratio of TAPSE to PASP, is the expression of a key risk factor in HFpEF patients, which is independently associated with the composite endpoint of all-cause death or HF-related recurrent hospitalization.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"47 7\",\"pages\":\"\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-07-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24308\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.24308\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24308","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Right Ventricular–Pulmonary Arterial Coupling and Outcome in Heart Failure With Preserved Ejection Fraction
Background
Right ventricular–pulmonary artery coupling (RVPAC) refers to the relationship between right ventricular systolic force and afterload. The ratio of echocardiograph-derived tricuspid annular plane systolic excursion (TAPSE) to pulmonary artery systolic pressure (PASP) has been proposed as a noninvasive measurement of RVPAC and reported as an independent prognostic parameter of heart failure. However, it has not been adequately in detail evaluated in heart failure with preserved ejection fraction (HFpEF). We hypothesized that RVPAC may be used and proposed as an expression of key risk factors in patients with HFpEF.
Methods
We retrospectively analyzed TAPSE/PASP of 648 HFpEF patients hospitalized in Chongqing Hospital of Traditional Chinese Medicine from January 1, 2016 to January 1, 2017. All eligible patients were followed up for 5 years. The correlation between TAPSE/SPAP index and clinical indicators and outcomes was evaluated.
Results
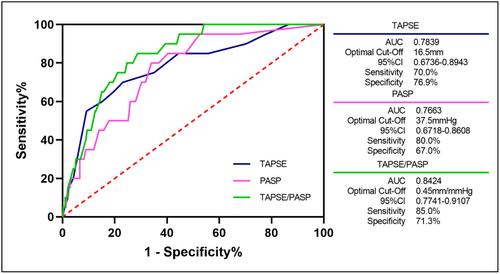
The final analysis included 414 patients. Nonsurvivors had significantly lower TAPSE, TAPSE/PASP and higher PASP compared with survivors (p < 0.0001). ROC curve analysis showed that the optimal cutoff of TAPSE, PASP, and RVPAC to predict all-cause death were 16.5 mm, 37.5 mmHg, and 0.45 mm/mmHg, respectively. In multivariate Cox regression analyses adjusted for gender showed a significant, independent association of the RVPAC with the composite endpoint of all-cause death or HF-related recurrent hospitalization (HR: 0.006; 95% CI 0.001–0.057, p < 0.001).
Conclusions
RVPAC, defined by the ratio of TAPSE to PASP, is the expression of a key risk factor in HFpEF patients, which is independently associated with the composite endpoint of all-cause death or HF-related recurrent hospitalization.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


